
Abstract
China’s rapid population aging and eroded family support capacity have heightened demand for sustainable eldercare solutions. To improve the capacity and quality of socialized eldercare services, China has initiated the community- and home-based elderly care services (CHECS) pilot program in 203 regions. This study explores its impact on older adults’ care patterns, aiming to address the need for effective eldercare approaches amid demographic and social changes. This study followed a quasi-experimental design and derived longitudinal data from the China Health and Retirement Longitudinal Study (CHARLS) for 2011 to 2020. We employed a staggered difference-in-differences (DID) approach to evaluate the effects of the CHECS pilot on older adults’ eldercare patterns across 5 key dimensions: living arrangements, care arrangements, economic sources, consumption expenditures, and spiritual comfort. The CHECS pilot significantly influences older adults’ care patterns across multiple dimensions. It increases the likelihood of hiring social personnel for care, reduces financial dependence on children, enhances financial self-sufficiency, and raises medical consumption expenditures. However, it decreases contact frequency with non-cohabiting children and does not affect living arrangements. These findings remain consistent across various tests. Notably, heterogeneous analysis shows stronger effects in regions with higher pension burdens and among vulnerable groups. Furthermore, CHECS also promotes greater use of community healthcare/eldercare services and shifts older adults’ perspectives on eldercare responsibilities. The implementation of the CHECS pilot significantly reshapes eldercare patterns in China across various dimensions, including care arrangements, economic resources, consumption expenditures, and spiritual comfort. CHECS demonstrates a viable, community-centered solution to aging and declining family support, offering an adaptable model for countries with similar eldercare pressures.
Keywords
Introduction
Given the rapid global population aging, the burden of eldercare has become an increasingly important policy concern. By the end of 2023, the proportion of the population aged 60 and above in China reached 21.1%, with those aged 65 and above accounting for 15.4% (National Bureau of Statistics). According to the “China Home-based Eldercare Industry Development White Paper (2021-2022; https://m.thepaper.cn/baijiahao_16915696),” approximately 90% of the elderly population opt for home-based eldercare, resulting in substantial pressure on family caregivers. However, the role of family-based care has gradually weakened, due to factors such as declining fertility levels, changes in lifestyle, family miniaturization (According to the seventh census, the average household size in China is 2.62.), increased population mobility, and higher rates of female labor force participation.1,2 As a result, the demand for elderly care services has grown substantially. According to the Research Report on Urban Home-Based Elderly Care Services in China (2008), 25.22% of elderly individuals require domestic services, 18.40% require nursing care, 18.90% seek daycare at elderly daycare centers, 36.80% require health care and end-of-life comfort services, and 13.79% need mental comfort services. The challenge of leveraging community resources to meet the care needs of older adults, while allowing them to remain in familiar homes and communities, has garnered significant attention from both the government and society.
To address the dual challenges of population aging and the weakening of family-based elderly care, the Chinese government has proposed developing community- and home-based elderly care services (CHECS). CHCES refers to a service model in which the government and social forces rely on communities to provide continuous and comprehensive medical care, social support, and daily care services to individuals, thereby maintaining their independence and remaining in familiar surroundings.3,4 Specific services include onsite visits, elderly service hotline, accompaniment to medical appointments, assistance with daily shopping, legal aid, in-home housekeeping, senior dining tables, daycare centers, or nursing homes, as well as psychological counseling services. 5 Its core design prioritizes aging in place by complementing family care, while addressing gaps in informal support through standardized, accessible services. Since 2000, the Decision on Strengthening the Work on Aging has emphasized community-based solutions for elderly care. As a result, communities have increasingly played a crucial role in supporting home care, as the development of home and community care services has become a key aspect of modernizing China’s eldercare model.
In 2016, the Ministry of Civil Affairs and the Ministry of Finance launched pilot reforms for CHECS, rolling them out across China in multiple phases. These pilots were implemented in 203 regions across 31 provinces (including autonomous regions and municipalities) and the Xinjiang Production and Construction Corps. Figure 1 shows the cities in mainland China that were covered by the pilot from 2016 to 2020. A total of 5 billion RMB was allocated by the central government via the Lottery Public Welfare Fund as performance-based subsidies. This central investment demonstrated a significant leverage effect, with local fiscal contributions exceeding 18 billion RMB during the pilot phase, and social investments amounting to at least 13 billion RMB. The total investment exceeded 36 billion RMB, benefiting 150 million elderly individuals (https://www.thepaper.cn/newsDetail_forward_17531070). The CHECS pilot programs in China are organized around 7 key components, as outlined by the central government’s guidelines (These components include: (1) establishing and operating several home and community-based elderly care service institutions through mechanisms such as services purchasing, public-private partnerships, government subsidies for private institutions, and equity cooperation; (2) encouraging professional elderly care institutions to provide home and community elderly care services; (3) exploring the “Internet+” model for home and community elderly care services; (4) strengthening the construction of elderly care staff teams and improving their remuneration; (5) promoting the standardization and regulation of elderly care services; (6) advancing the integration of medical and elderly care services; and (7) constructing community elderly care service facilities through various methods to meet the care needs of elderly individuals, particularly those in rural and urban areas, such as empty-nest and left-behind elderly individuals.). Regarding the outcomes of policy implementation, China has made significant strides in developing home- and community-based elderly care services. Following the initiation of the pilot policies, the number of community elderly care institutions and available beds grew significantly. From the end of 2016 to the end of 2023, the number of community elderly care institutions increased from 34 000 to 363 000, and the number of beds grew from 1.276 to 3.058 million, reflecting growth rates of 967.6% and 139.7%, respectively (National Bureau of Statistics). These reforms, which have since been extended to all provinces, offer a wide range of services from basic healthcare and daily assistance to more comprehensive support designed to improve older adults’ overall quality of life.

CHECS pilot regions during 2016 to 2020.
While a growing literature has explored the influence of CHECS on older adults, highlighting it as an influential factor in fostering healthy aging outcomes, including physical and mental health, life satisfaction, intergenerational transfers, labor participation, and social participation,6-15 limited attention has paid to its impacts on traditional eldercare system. Given that typical services listed in the CHECS program can assist older people with daily living, provide regular physical examinations and health management, and offer more opportunities for them to demonstrate competence and maintain social networks, all of which enhance older adults’ independence and reduce the pressure on family caregivers. This raises a critical question: Can CHECS bring about lasting, meaningful changes to China’s traditional eldercare system? Therefore, based on a staggered DID approach using longitudinal data from the CHARLS from 2011 to 2020, our study examines the association between CHECS and the 5 dimensions of eldercare patterns (living arrangements, care arrangements, economic sources, consumption expenditures, and spiritual comfort) among older adults. It also tests whether these relationships vary by region and older adults’ socio-demographic characteristics and analyzes CHECS’ role in promoting the utilization of community-based healthcare and eldercare services, as well as shaping older adults’ perceptions of eldercare responsibilities.
Methods
Sample Construction
Our study utilizes a panel dataset from the CHARLS conducted in 2011, 2013, 2015, 2018, and 2020. The CHARLS is a large-scale, interdisciplinary research project, jointly managed by Wuhan University and Peking University, designed to collect high-quality microdata that comprehensively represents individuals and households aged 45 and older in China. The dataset encompasses a broad array of variables, including demographic information, family structure and financial support, health status, physical measurements, access to medical services and health insurance, employment, retirement, pensions, income, consumption, assets, and community characteristics, covering more than 150 counties and 450 communities across 28 provinces, providing a nationally representative sample. Moreover, we incorporated prefecture-level data from the China City Statistical Yearbook to enrich the analysis.
We make the following instructions on the data handling process: (1) Since CHECS in China is mainly to serve older adults, our research is on individuals aged 60 and above; (2) we excluded observations with missing values in key control variables; (3) to exclude the interference of sample outliers on the results, the upper, and lower 1% of all continuous variables were trimmed.
Variables
Measurement of the Eldercare Mode
Since the eldercare pattern comprehensively reflects the care arrangements for older adults, we categorize it into 5 aspects following Cheng et al 16 and Shao et al 17 : living arrangements, care arrangements, main economic sources, main consumption expenditures, and spiritual support. The summary description of the eldercare patterns is shown in Table 1.
(1) Living arrangements reflect the actual living arrangements of older adults, including living independently (ie, by themselves or with spouses; others = 0), living with children (others = 0), and living in the elderly care institution (others = 0).
(2) Care arrangements reflect the eldercare arrangement, encompassing daily care and care during illness. According to the source of eldercare support, the primary providers are spouses (others = 0), children (others = 0), and social personnel (others = 0).
(3) The main economic sources are the primary source of livelihood from oneself (and spouse), children, or pension (including subsidies). We assign a value of 1 to the source with the largest amount and 0 to the others.
(4) Consumption expenditures are measured by the logarithm of the family’s annual medical, fitness, and matron expenses.
(5) Spiritual comfort reflects contact with non-residing children and social activities. Contact with non-residing children is based on the frequency of contact online, ranging from 1 = almost never to 9 = almost every day. Social activities are calculated by summing the frequencies of behaviors: visiting neighbors, playing mahjong, helping neighbors, and dancing/fitness, helping neighbors, and dancing/fitness, volunteering, caring for sick non-residents, and attending training courses, each graded on a scale of 1 to 3 (1 = infrequent, 2 = weekly, 3 = daily).
Indicator Summary for the Eldercare Pattern.

Measurement of CHECS
In the staggered DID model, the independent variable is whether the individual is covered by CHECS. We treat the implementation of CHECS in various regions as quasi-natural experiments. We classify older adults from pilot cities during the pilot periods as included in the treatment group (assigned a value of 1); otherwise, they are assigned to the control group (assigned a value of 0).
As described in Section 2.1, the pilot CHECS program in China encompasses 203 regions across 31 provincial-level administrative divisions, with the remaining regions designated as non-pilot areas. In our study sample, 67 out of 113 prefectural-level cities had implemented CHECS by the time the CHARLS survey was conducted in 2020.
Control Variables
Following prior research, we incorporate several control variables into our regression model.16,17
(1) Demographic and sociological characteristics, such as gender (male = 1, female = 0), age, education level (illiterate = 1, primary school = 2, middle school = 3, high school = 4, vocational school, and above = 5), marital status (married = 1, others = 0).
(2) Economic conditions, mainly based on per capita household income (log transformation).
(3) Family and social support, including the number of surviving children, family size, and social pension insurance (participation = 1, nonparticipation = 0).
(4) Health status, measured by self-rated health. This indicator is based on the answer to the questionnaire “How do you feel about your own health status now?,” ranging from 1 = very bad to 5 = very good.
(5) Area characteristics. A potential threat here is that the pilot cities may be selected by central and local governments based on pre-determined city-level characteristics and thus may be assigned non-randomly. We address this issue by introducing area characteristics, including the logarithm of per capita GDP, the logarithm of the local general budget expenditure, and the number of hospitals (including health centers).
Descriptive Statistics
Table 2 presents the descriptive statistics of the variables of interest. Regarding living arrangements, 71.63% of elderly individuals choose to live either alone or with a spouse. Notably, the treatment group exhibits a higher proportion of individuals living alone compared to the control group. In terms of elder care providers, children play a predominant role in assisting elderly individuals. This aligns with the broader literature on family caregiving, which shows that children often assume primary responsibility for elder care. The primary economic sources of older adults are typically their children and pensions (including government subsidies). However, a notable distinction emerges between the treatment and control groups: the treatment group is less reliant on financial support from their children and exhibits greater dependence on pensions. This shift could reflect variations in policy or socioeconomic factors that affect the financial autonomy of elderly individuals in the treatment group. Additionally, the treatment group allocates a higher proportion of expenditures to medical and healthcare services compared to the control group. In terms of spiritual support, the treatment group communicates less frequently with their children but participates more actively in social activities than the control group. Approximately 25.47% of the individual observations are derived from the pilot implementation of the CHECS program. The summary statistics for the control variables align with those reported in prior studies.
Descriptive Statistics.

Empirical Strategy
This study adopts a quasi-experimental research design to evaluate the causal effects of CHECS pilot policy on older individuals’ eldercare patterns. Since the CHECS pilot policy was implemented across multiple cities in China from 2016 to 2020, this paper adopts the staggered DID estimation approach to assess the policy treatment effect on the eldercare pattern. 18 Samples falling within the coverage scope for CHECS beneficiaries are included in the “treatment group,” while the remaining samples of non-beneficiaries are categorized as the “control group.” The baseline regression model is as follows:

Where the subscript i represents individual observations, c represents cities, and t denotes time periods,
To confirm the effectiveness of the staggered DID estimation results, this paper tests the parallel trend hypothesis referring to Beck et al
18
The specific econometric model is shown in equation (2), in which k represents the years before and after the implementation of CHECS, the coefficient

In addition, considering that the non-randomness of policies may cause endogeneity issues and that there may be selection bias in whether the city is chosen as a pilot city, we also use the Bacon decomposition, 19 placebo test, the PSM-DID model, eliminate the effect of other policies, and eliminate the cities that the pilots are partitioned to further verify the applicability and effectiveness of the staggered DID model.
Statistical Analysis
Data were analyzed using Stata (version 18) software. Descriptive statistics (mean, standard deviation (SD), min, and max) were used to describe the study variables. To evaluate the impact of the CHECS pilot on eldercare patterns, a staggered DID approach was employed. The validity of the DID design depends on the parallel trend assumption. A significance level of P < .05 was adopted.
Results
Baseline Regression
Table 3 presents the estimated effects of CHECS on eldercare patterns, as analyzed using equation (1).
Impact of CHECS on Eldercare Patterns.

Note. Robust standard errors clustered at the individual level are reported in parentheses, and ***, **, and * indicate significance at the 1%, 5%, and 10% levels, respectively.
Regarding the living arrangements, results suggest that CHECS did not significantly alter the actual living arrangements of older adults. This finding indicates that while CHECS has a broad impact on other aspects of eldercare, it does not directly impact the core decision of where older individuals reside.
In terms of care arrangements, we see a significant increase in the likelihood that older adults will hire external caregivers. Specifically, the probability of hiring someone to provide care when they are sick increases by 1.26 percentage points, a change that is statistically significant at the 5% level. This suggests that CHECS facilitated greater acceptance of professional or social care services among older adults, thereby indirectly alleviating the burden of household-based caregiving, especially in households where caregiving responsibilities could be extensive and burdensome.
Concerning the main economic sources, the results reveal a notable shift in the primary economic sources of elderly individuals. There is a significant increase in the likelihood that older adults’ primary financial support comes from themselves or their spouse, accompanied by a marked decrease in their financial dependence on children. Specifically, the probability that older adults’ primary financial source comes from self or spouse increases by 0.86 percentage points and is significant at the 5% level. In contrast, the probability that older adults rely on their children for financial support decreases by 3.31 percentage points, a change that is significant at the 1% level. These findings suggest that CHECS has had a positive impact on promoting active aging, reducing older adults’ financial dependence on their children, and fostering greater financial self-sufficiency.
Regarding consumption expenditures, the results indicate that CHECS is associated with an increase in medical consumption expenditure of about 16.85%, which is statistically significant at the 5% level. This suggests that the implementation of CHECS has led to greater utilization of healthcare services by older adults, potentially improving the health outcomes of the older population. However, the lack of a significant effect of CHECS on fitness or matron expenses implies that the intervention does not substantially shift the demand for preventive health measures or lifestyle-related consumption among the general population.
Concerning spiritual comfort, the results reveal that after the implementation of CHECS, the frequency of contact between older adults and their non-cohabiting children decreased by 0.0664 points, a change that is statistically significant at the 1% level. This finding suggests that CHECS have reduced older adults’ emotional or psychological dependence on their children, potentially reflecting an increased sense of autonomy and self-reliance.
To validate the robustness of the staggered DID estimation results, we tested the parallel trend hypothesis, following the methodology outlined by Beck et al.
18
The estimated coefficients (
Robustness Check
Placebo Test
To determine the extent to which the baseline regression results are affected by unobservable omitted variables and random factors, this study randomly generates the pilot cities and time for CHECS and accordingly, constructs randomized experiments at the pilot time and city levels to re-run the regression. The process described above was reiterated 500 times to verify the validity of the placebo test, yielding estimated coefficients and their P-values for the 500 pilot policies. The findings, presented in the appendix, indicate the possibility that the baseline estimation results being driven by unobservable factors can be excluded. This outcome strengthens the validity of the study’s conclusions and reinforces the role of CHECS from a counterfactual perspective.
Testing for Estimation Bias
Considering the potential bias inherent in staggered DID estimation, we adopt the methodology proposed by Goodman-Bacon 19 to assess the extent of estimation bias. According to Goodman-Bacon, multi-period DID estimates can be categorized into 3 categories: (1) newly treated units treating previously untreated units as controls, (2) newly treated units treating units that have not yet been treated as controls, and (3) newly treated units treating units that have already been treated as controls. Notably, the third category inherently incorporates treatment effects, making it inappropriate as a control group. To address this potential issue, we perform a Bacon decomposition to detect any biases in the estimation. As detailed in the Supplemental Material, our analysis reveals that samples that have never received the treatment carry relatively larger weights compared to the control group. The fact that the time-varying treatment group assigns significant weight to the never-treated group as the control group implies that there is no substantial bias in the estimation results. This implies that the estimates produced by our model are robust, and therefore, we can conclude that the results are relatively reliable.
PSM-DID Regression
The propensity score matching (PSM) method is widely used to assess the robustness of estimation results, particularly with respect to endogeneity arising from non-random policy assignment and potential selectivity bias. To ensure that the control and treatment groups are sufficiently comparable for accurately estimating the net effect of CHECS, this study employs PSM analysis to examine the causal relationship between CHECS and the eldercare patterns of older individuals, holding other conditions constant. This study uses a nearest-neighbor 1:3 matching method to select control group samples from non-pilot cities that are closest to the pilot cities in terms of propensity scores. The estimation results, as presented in the Supplemental Material, demonstrate that the coefficients and significance levels obtained after nearest-neighbor matching are consistent with those from the baseline regression, further supporting the robustness of the baseline findings.
Removing Interference From Contemporaneous Policies
The implementation of various policies related to eldercare during the sample period may also influence the estimation results. A key policy aimed at alleviating the burden of family-based eldercare is the public long-term care insurance (LTCI) pilot program. Launched initially as a pilot in July 2012, China’s LTCI program was expanded and more widely implemented after 2016. Previous studies have highlighted the significant role of LTCI in enhancing care quality, increasing medical service utilization, promoting home-based care, and fostering intergenerational support in China.20-22 Considering this, we remove sample cities that implemented LTCI during the sample period to re-estimate the baseline regression model. As demonstrated in the Supplemental Materials, the estimated coefficients remain consistent with the baseline outcomes after excluding these subsamples, thereby reinforcing the robustness and reliability of the original findings.
Eliminating the Cities Where Pilots are Conducted by Districts
Given that the implementation of CHECS in specific districts within certain cities may introduce confounding factors and biases into the estimation, it is necessary to exclude these cities from the analysis to ensure the robustness and validity of the research findings. Thus, we exclude the samples from Shanghai, Beijing, Tianjin, and Chongqing, cities where CHECS was carried out on a district-by-district basis, from the analysis and re-estimate the results. As shown in the Supplemental Materials, the estimated coefficients for the core explanatory variables remain statistically significant even after the exclusion of these subsamples, thereby affirming the robustness of the baseline results.
Heterogeneous Analysis
CHECS is highly associated with eldercare patterns among all older adults, as demonstrated in the preceding sections. However, due to regional and individual differences, their responses to CHECS vary significantly. Therefore, this study investigated the heterogeneous treatment effects of CHECS across different groups in this subsection.
Heterogeneity by Regional Differences
On the one hand, China’s dualistic urban-rural structure has led to an unequal distribution of public resources, resulting in significant disparities in the provision of public pension services. On the other hand, differences in the degree of regional aging further contribute to the uneven allocation of pension service resources across different areas. Therefore, this section aims to analyze the heterogeneity of CHECS by examining both urban-rural disparities and regional variations in aging levels. The results in Table 4 show that CHECS has almost no effect on the living arrangements of older adults, with coefficients close to zero and highly statistically insignificant. This finding aligns with the baseline results, suggesting that the CHECS does not significantly influence the living arrangements of older adults.
Heterogeneous Analysis of Regional Differences.

Note. N represents the sample size, and ***, **, and * indicate significance at the 1%, 5%, and 10% levels, respectively.
Regarding elder care arrangements, CHECS has no significant effect on the care arrangements for seniors residing in urban areas or regions with lower levels of aging. Conversely, for seniors residing in rural areas and regions with higher levels of aging, the likelihood of receiving care from social personnel increases significantly, by 0.81 and 1.58 percentage points, respectively. The increasing reliance on social personnel for eldercare in rural and more aged regions may be indicative of gaps in informal caregiving resources, suggesting a greater role for CHECS in expanding formal care services in these areas.
Concerning the main economic sources, CHECS exerts a significant impact on the primary source of income for older adults residing in rural areas and regions with higher aging levels. Specifically, for seniors in rural areas, CHECS significantly increases their economic independence while reducing their reliance on financial support from children. For older adults in regions with higher aging levels, CHECS significantly decreases their economic dependence on children while increasing their reliance on pensions and subsidies, suggesting that CHECS has played a significant role in alleviating the financial burden on families and enhancing pension security.
For consumption expenditures, CHECS has no significant effect on fitness or matron expenses across all senior groups. However, it significantly influences medical expenses for older adults residing in rural areas and in regions with lower aging levels. Specifically, CHECS increases medical expenses by 31.01 and 34.58 percentage points for older adults residing in rural areas and in regions with lower levels of aging, respectively. The improvement in healthcare access facilitated by CHECS may be a key factor contributing to the increase in medical costs in these areas.
Concerning spiritual support, CHECS does not significantly affect the frequency of social activities for any of the subsamples. However, it has a significant impact on the frequency of contact with children among older adults residing in rural areas and regions with both higher and lower levels of aging. Specifically, for seniors in rural areas, CHECS significantly reduces the frequency of contact with their children. Similarly, among older adults in regions with varying aging levels, CHECS also reduces the frequency of contact with children.
Overall, the implementation of CHECS demonstrates substantial heterogeneity in its effects across urban and rural areas, as well as regions with varying degrees of aging. This suggests that, although CHECS has had a positive impact on the quality of life and economic well-being of elderly individuals, its policy effects vary significantly across regions and by the degree of population aging. In particular, CHECS has shown a more pronounced impact in rural areas and regions with higher aging levels.
Heterogeneity by Individual Differences
Furthermore, we discovered that the influence of CHECS may vary significantly due to individual differences. We test heterogeneity among older adults by education (higher vs lower), income (above median vs below median), number of children (single vs multiple), and age (over 80 vs under 80). Table 5 presents the results.
Heterogeneous Analysis of Individual Differences.
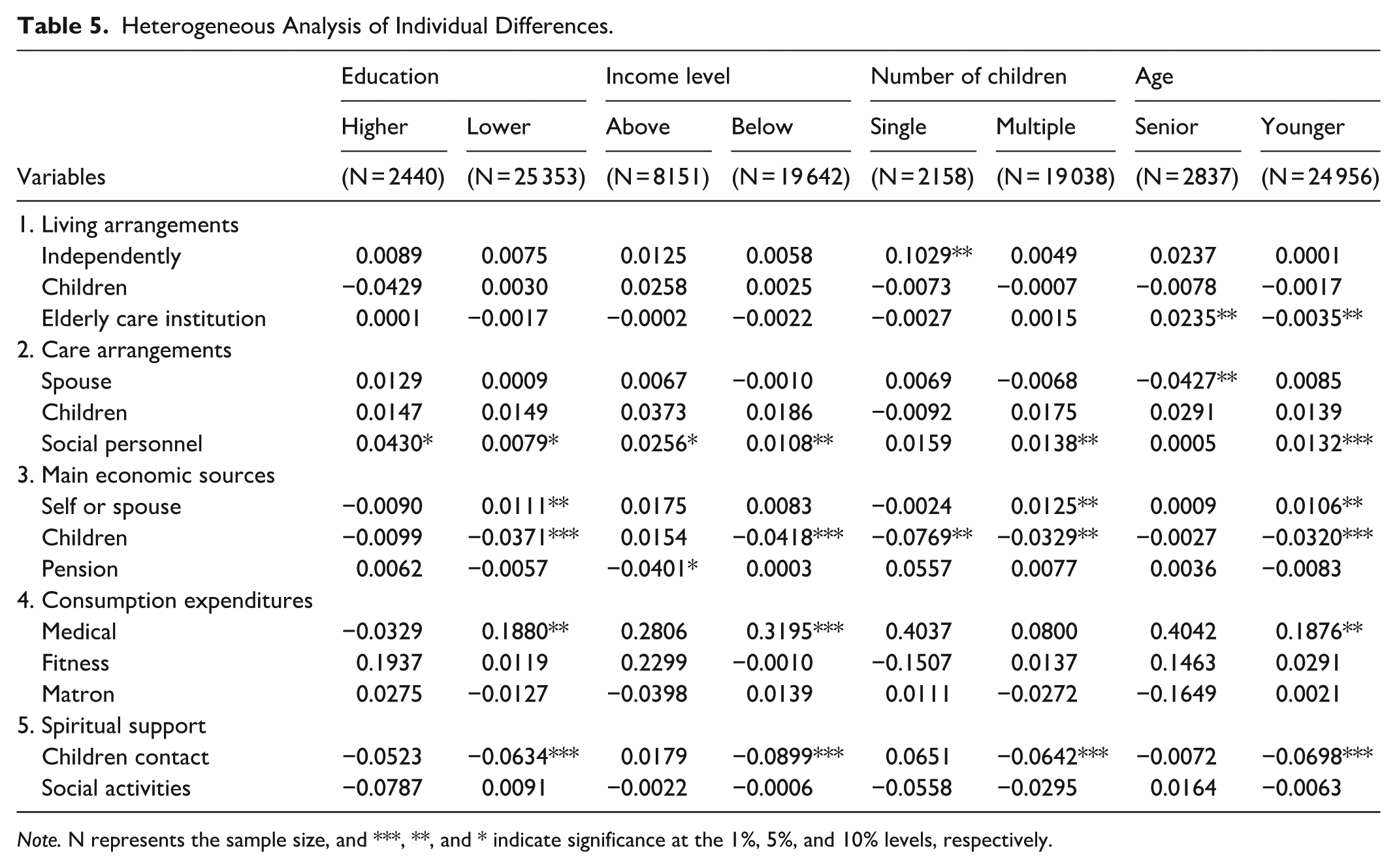
Note. N represents the sample size, and ***, **, and * indicate significance at the 1%, 5%, and 10% levels, respectively.
For living arrangements, we find that CHECS significantly influences seniors with only 1 child, aged below 80, and aged 80 and above. Correspondingly, older adults with only 1 child have a significant increase in the probability of living alone or with a spouse, thereby increasing their residential independence. For older adults aged 80 or younger, the likelihood of living in social care facilities decreases. In contrast, the possibility of living in social care facilities increases for older adults aged 80 and above.
Regarding elder care arrangements, CHECS significantly increases the possibility of receiving care from social personnel, regardless of education and income. Moreover, CHECS significantly affects care arrangements for older adults with multiple children, those aged 80 and below, and those aged 80 and above. Specifically, the possibility of receiving care from social personnel increases significantly by 1.38 and 1.32 percentage points, respectively, for older adults with multiple children and those aged 80 and below. For those aged 80 and above, the likelihood of receiving care from spouses decreases by 4.27 percentage points, suggesting that CHECS relieves spouses’ care burden in older families. However, CHECS has no significant effect on the care arrangements for seniors with only 1 child.
Concerning the main economic sources, CHECS demonstrates a noteworthy impact on the economic dynamics of elderly individuals, particularly those facing financial vulnerabilities. Specifically, the CHECS significantly reduces older adults’ dependence on financial transfers from their children, especially among those with lower educational attainment, below-median income, a single child, or multiple children, and individuals aged 80 and below. Additionally, the study reveals that CHECS improves economic independence among seniors with lower education, multiple children, and those under 80, which may be attributed to better access to public health services. The findings imply that CHECS may serve as a critical tool in alleviating the economic burden on the elderly, particularly those in lower socioeconomic strata.
For consumption expenditures, regardless of education, income, number of children, or age, CHECS has no significant effect on fitness or matron expenses, which aligns with the baseline results. Moreover, CHECS significantly influences medical expenses for older adults with lower education, below-median income, and those aged 80 and below. Specifically, CHECS increases their medical expenses by 18.80, 3.95, and 18.76 percentage points, respectively.
Concerning spiritual support, aligning with the baseline results, CHECS does not significantly affect the frequency of social activities. However, it significantly reduces the frequency of contact with their children among older adults with lower education, below-median income, multiple children, and those aged 80 and below, thereby increasing their emotional independence.
Further Analysis
To provide further evidence regarding the changes in eldercare patterns induced by CHECS, this section examines the influence of CHECS coverage on the actual utilization of relative services by older adults, as well as its impact on their perceptions of eldercare.
The analysis presented in this section utilizes a panel dataset drawn from the CLASS (The CLASS is a nationwide, continuous, and large-scale social survey project organized by Renmin University of China. It covers 462 village and neighborhood committees across 28 provinces, autonomous regions, and municipalities directly under the Central Government (excluding Hong Kong, Macao, Taiwan, Hainan, Xinjiang, and Tibet). The survey provides comprehensive data on living standards, social dynamics, and economic conditions in both rural and urban China. Data collected in 2014, 2016, 2018, and 2020 have been published, offering valuable insights into trends and changes in Chinese society over the past decade.) conducted in 2012, 2014, 2016, and 2020. This dataset is particularly well-suited for our study, as it encompasses the key variables critical to our analysis in this section (We did not utilize this dataset in our primary regression analysis for 2 main reasons. First, the CLASS does not include urban variables for the years 2014 and 2018. Although we considered matching and supplementing the data from 2016 and 2020, such an approach would result in a significant loss of samples. Second, the dataset lacks comprehensive information on eldercare. However, given that it provides valuable data on healthcare services, eldercare services, and attitudes toward eldercare, we incorporate it in this section as a supplementary resource to enrich the analysis.). The estimation methodology and control variables employed in this analysis are consistent with those used in the baseline regression model, ensuring comparability and robustness of the results.
Further Evidence of Healthcare and Eldercare Utilization
Despite the potential of CHECS to expand access to healthcare and eldercare services, significant disparities in service utilization persist. 23 Older adults often lack sufficient health knowledge or face barriers in accessing information regarding the availability, quality, and cost of community-based and home care services. This information deficit leads to low awareness and acceptance of available services, which in turn hampers actual service utilization. 24 Therefore, further empirical analysis will be conducted to evaluate the effectiveness of CHECS in promoting the use of community-based healthcare and eldercare services among the elderly population.
Regarding community-based healthcare services, respondents were asked whether they had ever received community healthcare services, including onsite nursing, onsite medical treatment, rehabilitation training, rental of rehabilitation aids, free physical examinations, electronic health records, and health workshops. Based on the responses, we construct a binary variable to measure the utilization of community-based healthcare services among older adults. Regarding community home-based elderly care services, the respondents were inquired about whether they received services such as onsite visits, elderly service hotline, accompaniment to medical appointments, assistance with daily shopping, legal aid, in-home housekeeping, senior dining tables, daycare centers, or nursing homes, as well as psychological counseling services. Based on the responses, a binary variable was created to assess the utilization of community home-based elderly care services by older adults.
Table 6 presents the results. Specifically, CHECS coverage was found to be significantly and positively correlated with the utilization of community-based healthcare and eldercare services of older adults, with increases of 6.62% and 4.81%, respectively, at the 1% significance level. The results indicate that the implementation of CHECS significantly enhanced the utilization of community-based healthcare and eldercare services among older adults. One possible explanation for this outcome is that CHECS fosters greater trust in these services among elderly individuals by establishing a comprehensive and integrated health management and care network. This network optimizes resource allocation and enhances both service coverage and quality by connecting community health service providers, primary healthcare facilities, and elderly care resources, thereby increasing seniors’ willingness to utilize and rely on community-based healthcare and eldercare services. This shift reflects the gradual transformation of the elderly population’s demands for healthcare and eldercare services, as well as their increasing acceptance and recognition of the existing service system.
Impact on Healthcare and Eldercare Services Utilization.
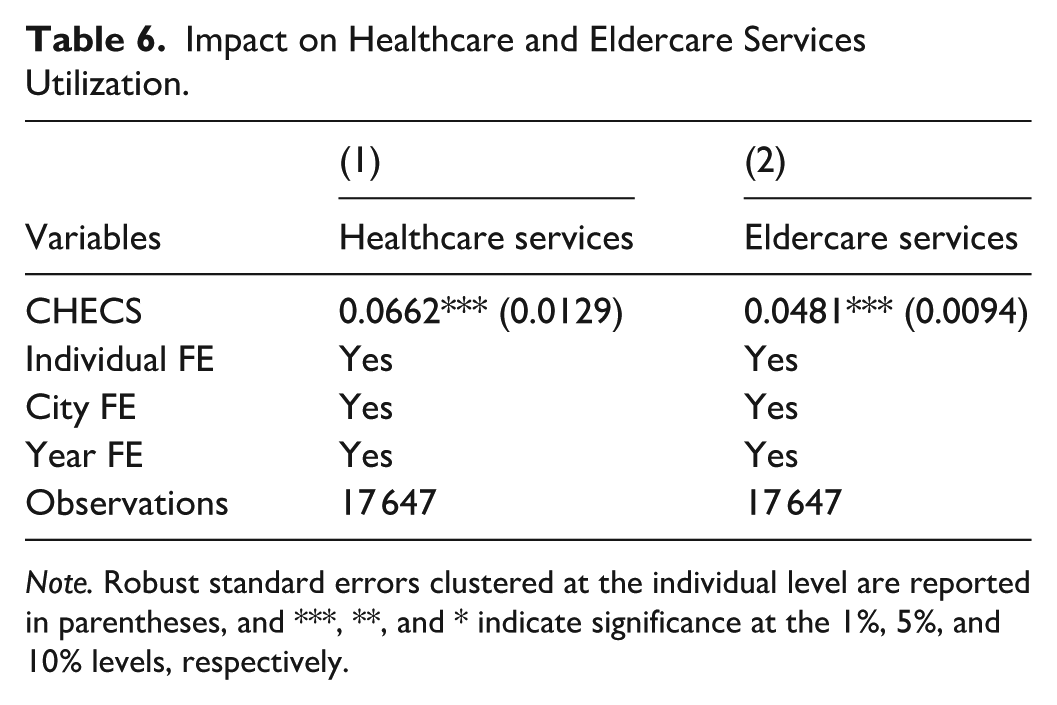
Note. Robust standard errors clustered at the individual level are reported in parentheses, and ***, **, and * indicate significance at the 1%, 5%, and 10% levels, respectively.
Impact on the Perception of Eldercare Responsibilities
The choice of the elderly care model is closely linked to prevailing perceptions of aging. Under traditional family-based caregiving norms, elderly individuals typically rely on their children or family members for care, with the belief that children have a responsibility and duty to provide both physical and emotional support to their parents. This caregiving norm is prevalent in East Asian cultures, such as China, where strong family ties and filial piety are emphasized. 25 However, with the ongoing transformations in social structures—marked by factors such as increased urbanization, migration, family downsizing, and the growing participation of women in the labor force—the traditional “family care” model faces significant challenges. As discussed in previous sections, CHECS has the potential to reshape caregiving paradigms. This raises the question: Does it also influence the long-standing traditional views on aging and caregiving?
The dependent variable in this analysis is the perception of aging, specifically individuals’ awareness and attitudes toward caregiving responsibilities. Based on the question, “Who do you believe should primarily take responsibility for the care of the elderly?,” we categorized responses into 4 groups: individual or spouse (other = 0), children (other = 0), government or society (other = 0), and shared responsibility (other = 0). The results are presented in Table 7.
Impact on the Perception of Eldercare Responsibility.

Note. Robust standard errors clustered at the individual level are reported in parentheses, and ***, **, and * indicate significance at the 1%, 5%, and 10% levels, respectively.
The results suggest that CHECS has significantly facilitated a reconfiguration of older adults’ perceptions of the responsibilities associated with elderly care, particularly in their attitudes toward government and society’s involvement in this area. As evidenced by the results in Column (3), CHECS significantly increased the proportion of older adults who believe that the responsibility for elderly care should lie with the government or society, by 2.17% at the 5% significance level. Through a government-led society-involved community care system, on the one hand, older adults demonstrate a stronger acknowledgment of the government and society’s roles in delivering public services and ensuring social welfare. Such recognition not only enhances older adults’ social trust in government institutions but also emphasizes the critical role of governmental in advancing the welfare of the aging population.
On the other hand, it effectively mitigates the effects of the traditional “eldercare isolation” phenomenon. Traditionally, caregiving for older adults has been regarded primarily as a family or personal responsibility, with elderly individuals often depending on their spouses or children for support. This family-centered approach, however, has frequently resulted in emotional isolation and a lack of social support. By promoting the integration of community and government resources, CHECS enhances social support and the availability of healthcare services for older adults, thereby reducing their reliance on family care. This, in turn, fosters a greater sense of social participation and belonging, enabling elderly individuals to access a more diversified range of care options and facilitating their integration into a broader social framework. Thus, the transformation induced by CHECS not only reconfigures the perception of caregiving responsibilities but also contributes to a more inclusive, socially connected model of elderly care. It encourages a shift away from isolation toward a model in which community and government collaboration play a central role in ensuring the well-being of older adults.
Discussion
To our best knowledge, this study is the first to explore the association between CHECS utilization and eldercare patterns among older adults in China. We found that the CHECS pilot policy significantly affects the eldercare patterns of older adults in the pilot cities. Specifically, no significant changes in living arrangements were observed. In terms of care arrangements, CHECS notably increases the likelihood that older adults will be cared for by social personnel. Regarding the main economic sources, CHECS significantly increases older adults’ financial independence, concurrently reducing their financial dependence on children. Regarding consumption expenditures, CHECS is significantly associated with an increase in medical expenditures. Concerning spiritual comfort, CHECS significantly correlates with a reduction in the frequency of contact between older adults and their non-cohabiting children. We also found that the pilot policy has a more pronounced effect in rural areas and regions with higher levels of aging. Moreover, the CHECS exhibits a more significant impact on older adults with lower educational attainment, below-median income levels, multiple children, and those under 80. Furthermore, CHECS significantly boosts community-based healthcare and eldercare utilization and alters older adults’ perceptions of eldercare responsibility.
Our results showed that CHECS failed to significantly influence older adults’ living arrangements, such as decisions to live alone, with children, or in residential care. This finding addresses a key gap in the literature, which has predominantly focused on how living arrangements influence CHECS utilization rather than the reverse. While prior research confirms that community-based programs help older adults remain at home longer and delay nursing home admission,26-29 these aging-in-place effects differ fundamentally from those of altering living arrangements. The latter involves shifts in core residential status, whereas the former merely supports older adults in maintaining their current housing situations. Our findings suggest that CHECS supports existing living arrangements rather than causing changes. The lack of impact on living arrangements further reflects the complex interplay of demographic, health, economic, and cultural factors, such as filial piety and housing stability, which often outweigh the influence of care services.30-33
Our findings showed that CHECS significantly increases the likelihood that older adults will hire external caregivers, aligning with findings from Lu and Wu, 34 who noted that CHECS enhances access to care services by reducing barriers and integrating community resources. This increased accessibility drives more older adults to hire external caregivers, addressing concerns about finding reliable care and high costs. Notably, CHECS does not significantly affect the likelihood of older adults choosing family care from spouses or children. This can be explained by 2 reasons supported by existing literature. First, formal care services can replace informal care provided outside the home, but they cannot replace the informal care provided by dependents or co-residing relatives, 35 due to the emotional value and trust associated with family care, which external services cannot replace. 36 Second, CHECS is inherently designed to supplement, rather than substitute for, family care when family support is insufficient.37-39 This targeted impact highlights CHECS’s role in optimizing, not disrupting, the existing care structure.
In terms of the main economic sources, CHECS significantly enhances older adults’ financial independence, thereby reducing their financial reliance on children. This finding is consistent with the conclusions of Lu and Wu 34 and Chen et al 40 who highlight that such programs facilitate access to supplemental income sources, enabling older individuals to achieve greater financial autonomy. Consequently, older adults are less financially dependent on their children, alleviating the economic burden on families.
Regarding consumption expenditures, CHECS is significantly associated with increased medical expenditures, consistent with Jiang et al. 41 This correlation stems from CHECS’s role in enhancing access to professional care, such as subsidized primary consultations and preventive screenings, by integrating community resources and lowering utilization barriers, thereby prompting more timely healthcare seeking in the community rather than delayed treatment. 42 This shift toward early care leads to higher utilization of community medical services, which in turn contributes to increased medical expenditures.
Concerning spiritual comfort, our findings indicate that CHECS significantly correlates with a reduction in the frequency of contact between older adults and their non-cohabiting children, aligning with Yu and Zhang’s 43 conclusion that such formal care programs exert a substitution effect on intergenerational emotional support. Specifically, CHECS provides structured emotional support (eg, community companionship, psychological counseling) through professional care services, 44 thereby reducing older adults’ reliance on children for emotional support. This helps seniors gain greater autonomy, ease the psychological burden of needing constant familial interaction, and potentially improve mental health. Notably, this shift does not conflict with filial piety’s core of respecting and comforting older adults but replaces mere high-frequency contact with quality interactions. Relieved from the pressure of perfunctory daily check-ins, children can focus on meaningful companionship, while intergenerational relations transition from one-sided elder dependency to a more balanced, respectful dynamic. Surprisingly, our results indicated that CHECS did not significantly affect the social participation of older adults, a finding that appears to be inconsistent with results from existing studies,14,45,46 which suggested that similar programs typically have a positive impact on older individuals’ social engagement. This inconsistency may arise from differences in program implementation or regional variations, as previous studies highlighted positive outcomes in social engagement through similar initiatives. It is possible that CHECS, while addressing key caregiving needs, does not sufficiently focus on promoting social interaction or community involvement. Furthermore, barriers such as mobility limitations, health issues, and social isolation may hinder older adults’ ability to participate, regardless of the caregiving support provided. Future adaptations of CHECS could benefit from integrating strategies specifically designed to improve social engagement.
Our study further reported that the pilot policy demonstrates a more pronounced effect in areas with a heavier pension burden, especially in rural areas and regions with higher level of population aging. The urban-rural differences in eldercare patterns influenced by CHECS highlight the program’s potential to bridge the gap in access to formal care between urban and rural areas. As China develops home- and community-based care systems to serve rural populations,2,45 CHECS offers a sustainable and efficient solution for elderly care in these regions. Furthermore, older adults in regions with higher levels of aging face more challenges accessing traditional care, making CHECS particularly valuable in these areas. As the aging population grows, regions with greater demographic shifts stand to gain significant advantages from policies like CHECS, which provide a sustainable, efficient solution to the growing demand for elderly care.
Our findings also highlight CHECS’s greater impact on older adults who are more vulnerable due to limited endowment resources, such as those with lower educational attainment and below-median income. These individuals often struggle to access both financial resources and quality eldercare services. 8 By providing formal caregiving and additional support, CHECS helps raise their living standards and overall well-being. The program’s ability to reach and assist vulnerable populations is crucial in mitigating inequalities in elderly care systems. Additionally, CHECS has a more substantial effect on seniors with multiple children and those under 80. Older adults with multiple children often face coordination issues in family caregiving, which can reduce the efficiency of family care. CHECS alleviates these challenges by providing standardized community-based services, thus filling care gaps. For older adults under 80, their moderate functional independence allows them to benefit more from CHECS, such as preventive screenings and social activities. In contrast, older seniors may rely more on intensive institutional care, which CHECS currently supplements to a lesser extent. This targeted effect allows for more effective resource allocation within the policy.
Further analysis underscores that CHECS significantly increases older adults’ utilization of community-based healthcare and eldercare services, while also reshaping their perception of eldercare responsibility. The program’s promotion of community-based healthcare utilization fills a research gap in understanding CHECS’s impact on healthcare use. This aligns with our findings on increased medical expenditures, as higher healthcare utilization directly explains the rise in spending. Additionally, the increase in eldercare service utilization due to CHECS aligns with conclusions from Lu and Wu 34 and Wang et al. 47 Zhang and Zhang 48 noted that existing community eldercare facilities are underutilized due to their failure to meet the expectations of older adults. CHECS pilots effectively resolve this issue by improving the accessibility and quality of eldercare services, ensuring they better align with older adults’ needs and preferences, thereby increasing service utilization.34,47 Finally, CHECS contributes to a shift in perceptions of eldercare responsibility, emphasizing shared responsibility among the government, society, and families rather than placing the burden solely on children. This shift aligns with broader societal changes in China, where the traditional view of children as primary caregivers is gradually being replaced by a more diversified approach to eldercare.25,49,50 By guiding older adults from a family-centric model to one that emphasizes social and shared eldercare responsibility, CHECS plays a pivotal role in reshaping intergenerational eldercare ethics and fostering the development of social eldercare services.
Policy Implications
Considering the findings, this paper proposes the following policy implications. First, the evidence suggests that socialized eldercare services, such as those offered through CHECS, have the potential to alleviate the financial and emotional burden on families, particularly in regions with a high pension burden and those experiencing rapid demographic aging. Policymakers should consider expanding the scope of the CHECS pilot to cover more provinces and cities, ensuring that older adults across diverse regions benefit from these services. Second, targeted policies could be developed to further support financially vulnerable groups, such as older adults with lower levels of education and income, and those without sufficient familial support. These individuals are more likely to benefit from community-based services that promote greater independence and reduce the strain on family caregivers. Finally, the growing reliance on socialized eldercare presents an opportunity for the government to invest in strengthening healthcare infrastructure and expanding the availability of community-based healthcare services, especially in rural and underserved areas. Policymakers should also consider promoting public awareness campaigns to encourage societal acceptance of government and community-based eldercare solutions.
Limitations
Despite the valuable insights this study offers, certain limitations warrant consideration. Due to data availability constraints, this study did not encompass all pilot provinces and cities participating in the CHECS program, which may limit the generalizability of the findings to other regions. Future research could address this gap by incorporating data from additional pilot areas, thus providing a more comprehensive assessment of the policy’s nationwide impact. Additionally, given the complex nature of eldercare, future research could delve deeper into the intersection of factors influencing eldercare choices, including cultural, regional, and socioeconomic factors, to further refine the policy recommendations for enhancing eldercare in China.
Conclusion
Our study provides robust evidence that the CHECS pilot significantly reshapes eldercare patterns in China. Its impacts were concentrated on care arrangements, economic resources, consumption expenditures, and spiritual comfort. Specifically, CHECS boosts reliance on social care, increases medical expenditures, and effectively decreases the economic and emotional dependence of older adults on their children. Of particular interest, the effects of CHECS are particularly pronounced in areas with higher pension burdens and among vulnerable groups. Additionally, CHECS leads to greater utilization of community-based healthcare and eldercare services and shifts older adults’ perspectives on eldercare responsibilities. CHECS effectively eases family care pressure, offering a viable solution to China’s aging challenge. For countries with similar eldercare strains, especially those with limited resources to build large-scale institutional care facilities, CHECS provides an adaptable, community-centered model to advance sustainable eldercare systems.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261434823 – Supplemental material for Impacts of Community- and Home-Based Elderly Care Services on Eldercare Patterns: A Quasi-Experimental Study in China
Supplemental material, sj-docx-1-inq-10.1177_00469580261434823 for Impacts of Community- and Home-Based Elderly Care Services on Eldercare Patterns: A Quasi-Experimental Study in China by Ling Xiao, Chuanfeng Han and Yiliyaer Mohetaer in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580261434823 – Supplemental material for Impacts of Community- and Home-Based Elderly Care Services on Eldercare Patterns: A Quasi-Experimental Study in China
Supplemental material, sj-docx-2-inq-10.1177_00469580261434823 for Impacts of Community- and Home-Based Elderly Care Services on Eldercare Patterns: A Quasi-Experimental Study in China by Ling Xiao, Chuanfeng Han and Yiliyaer Mohetaer in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors thank the CHARLS research teams for providing the data. We also appreciate the insightful comments from the editor and anonymous reviewers which greatly improved this manuscript.
Ethical Considerations
This study utilized publicly available, secondary data from the China Health and Retirement Longitudinal Study (CHARLS). Ethical approval was granted by the Institutional Review Board (IRB) at Peking University. The IRB approval number for the main household survey is IRB00001052-11015.
Consent to Participate
Not applicable.
Author Contributions
Ling Xiao: Conceptualization; Methodology; Supervision; Writing - Review & Editing.
Chuanfeng Han: Data Curation, Validation, Visualization, Funding Acquisition.
Yiliyaer Mohetaer: Conceptualization, Supervision, Writing - Review & Editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by National Natural Science Foundation of China (Grant No. 71874123, 71972127, 71974122) and National Social Science Fund Project of China (Key Program) (Grant No. 23AZD073).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this research are publicly available from their respective official websites. Derived data supporting the findings of this study are available from the corresponding author, Yiliyaer Mohetaer, upon reasonable request.
Declaration of AI Use
The authors confirm that no Artificial Intelligence (AI) tools were used in the generation or modification of the scientific data or results. AI-powered language polishing and grammar-checking tools were utilized during the preparation of this manuscript to improve readability.
Supplemental Material
Supplemental material for this article is available online.