
Abstract
The association between living arrangements and depressive symptoms has been documented in previous systematic studies but remains controversial. This study further explored the association between living arrangements and depressive symptoms. It utilized newly published data and implemented a more rational categorization of living arrangement styles based on census data. The sample for this study was drawn from the China Health and Aging Tracking Survey (CHARLS) 2020 survey data and included 6527 residents aged at least 60 years. Depressive symptoms were defined by the 10-item Center for Epidemiologic Studies Depression Scale. Multivariate logistic regression was employed to evaluate the association between living arrangements and depressive symptoms. Additionally, gender differences in this association were analyzed, and 4 distinct living arrangement patterns were compared. Compared with living alone, living with spouse or living with children and spouse was associated with lower odds of experiencing depressive symptoms (OR = 0.281 95% CI 0.134-0.588 and 0.381 95% CI 0.177-0.819). The spouse, not the child, influences depressive symptoms in older adults. There was no significant association between women’s living arrangements and depressive symptoms. The associations of the variables with depressive symptoms within the 4 living arrangement styles were generally the same as the associations of the variables with depressive symptoms within the total sample, but there were differences between the associations of the individual variables and depressive symptoms. Older adults who live alone or live with children without a spouse are more likely to experience depressive symptoms. More attention should be given to older adults who live with children without a spouse.
Highlights
It is the spouse, not the children, that influences depressive symptoms in older adults.
Older adults who live alone or live with children without a spouse are more likely to experience depressive symptoms.
More attention should be given to older adults who live with children without a spouse.
Introduction
Depression stands as one of the most widespread psychiatric disorders among middle-aged and elderly populations worldwide. 1 According to the World Health Organization, approximately 280 million people globally are affected by depression. 2 Additionally, the global median prevalence of depression in older adults is estimated to be around 10.3%. 1 As the second leading cause of disability, depression typically impairs quality of life, increases suicide risk and decreases life expectancy.3,4 Consequently, identifying the factors linked to depressive symptoms is of utmost importance. This enables the implementation of targeted interventions to enhance the mental health of older adults.
Depression is associated with numerous potential risk factors. In recent years, living arrangements have emerged as a focal point of scientific inquiry,5,6 particularly amid the rapid demographic shifts sweeping across many nations. Declining marriage and birth rates have significantly reshaped the living patterns of older adults, 7 and this trend is particularly pronounced in China. Here, the traditional family structure is undergoing profound transformation due to the growing elderly population, the long-standing one-child policy, and the accelerating pace of urbanization. Data from the seventh national census reveals that in 2021, China’s average household size fell below 3 persons for the first time. 8
The profound changes in demographic transition have directly reshaped the social significance and practical impacts of living arrangements. Traditionally, “living with children” was not only the primary means for the elderly to obtain economic support and daily care, but also bore the intergenerational emotional bonds and social identity under the “filial piety” culture. 9 Nowadays, however, the declining birth rate and the shrinking of family size have weakened the foundation of “multigenerational cohabitation.” Meanwhile, factors such as the gradual improvement of the social security system and the enhanced sense of independence among the elderly have led to a gradual decrease in the proportion of the elderly living with their children, while the proportion of elderly couple households has been on the rise. 10 The spatial and geographical separation between the elderly and their children has reduced the possibility of children providing support, and also affected the elderly’s sense of happiness. Therefore, against the backdrop of China’s unique demographic transition, it is of great significance to re-examine the relationship between living arrangements and depressive symptoms in the elderly.
Previous studies have examined the associations between living arrangements and mental health.11,12 However, there is no academic consensus on the relationship between living arrangements and depression. As a prevalent living arrangement, cohabitation with children has garnered substantial research attention. Emerging studies suggest that this living pattern may mitigate depressive symptoms in older adults, primarily by facilitating access to support from adult children.13,14 However, other studies have shown that living with children is harmful to the mental health of older adults because of family conflict.15-17
Many more studies have compared the effects of different living arrangement styles on depression, and the findings vary just as much. Studies, Singapore, Finland, and Egypt have shown similar results, indicating that older adults living alone are more likely to report depressive symptoms than those living with children and spouses.17,18 However, studies from the United States and India reported exactly the opposite results.19,20
Social and cultural differences are important factors contributing to the variation in study results, but we found that the results varied widely even for studies conducted in the same country. A study in China revealed that the prevalence of depressive symptoms was lower in older adults living with children and spouse than in those living with spouse. 14 However, another study in China showed that older adults living with children and spouses were more likely to have depressive symptoms than those living with spouses only. 21
Building on prior research, we refined living arrangement categories using 2020 census data and analyzed the latest CHARLS 2020 data to explore links between living arrangements and depression in older adults.
Method
The study followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines, 22 as details in Appendix, Supplemental Table S1.
Sample
This study is based on data from the China Health and Aging Longitudinal Study (CHARLS), a nationally representative survey of the population aged 45 years or older living in China that includes an assessment of the social, economic, and health status of community residents. 23
Using 2020 data that initially included 19 331 respondents, we derived our analytic sample by selecting individuals aged 60 and older who were capable of communicating with interviewers and excluding those with missing data, resulting in a final sample of 6527 participants.
Measures
We utilized the 10-item short form of the Center for Epidemiologic Studies Depression Scale (CES-D-10) to assess depressive symptoms in the CHARLS study. 24 Each item was rated on a 4-point scale (1 = rarely or never to 4 = most or all of the time), and a total score ranging from 10 to 40 was calculated by summing all items, with higher scores indicating more severe depressive symptoms. The short form of the CES-D has excellent psychometric properties among older Chinese adults. 25
Independent Variables
Living Arrangements
Data from the 2020 census revealed that Chinese older adults’ living arrangements consisted of 4 main types of living arrangements: 43.7% lived with spouse; 23.1% lived with children and spouse; 16.6% lived with children without a spouse; and another 12% lived alone. 26 Considering that institutions and other living arrangements account for a relatively small proportion of the total sample, comparing them as a living arrangement type with others may affect result accuracy. Therefore, this paper selected 4 main living arrangement types as independent variables: living with children and spouses, living with spouse, living with children without a spouse, and living alone. In this study, living alone was used as the reference item.
Individual-Level Covariates
Depressive symptoms in older adults are influenced by many factors. The control variables in this study were categorized into 3 main groups: demographic and family characteristics, respondents’ health status, and daily activities.
The demographic and household characteristics of the participants included age, sex, marital status, place of residence, and education level. We categorized patients into 3 groups according to age (60-69, 70-79, and 80 years and above). 27
Marital status was categorized into 2 groups (married and other), place of residence was categorized into 2 groups (urban and rural), and education level was categorized into 3 groups (elementary school and below, middle school, and high school and above).
Health behaviors included 3 variables: alcohol consumption, self-rated health, and degree of difficulty dressing. We categorized alcohol consumption into 2 groups (drinking and nondrinking). Self-reported health was categorized into 5 levels (very good, good, fair, poor and very poor). Difficulty in dressing was categorized into 4 levels (no difficulty, difficulty but able to complete, difficulty needing help and unable to complete).
Daily activities consisted of 3 variables: leisure activities, work situation and internet use. Leisure activities were categorized into 2 groups (participating in leisure activities and not participating in leisure activities), work situation was categorized into 2 groups (working and not working), and internet use status was categorized into 2 groups (using the internet and not using the internet).
Statistical Methods
We used RStudio to analyze the data and multivariate logistic regression analysis to explore the associations between living arrangements and depressive symptoms. Prior to data analysis, the multicollinearity of variables was assessed via the variance inflation factor (VIF), which was <10, indicating that there was no multicollinearity in this study. 28 The confidence level was 95%. Statistical significance was set at P < .05.
Results
The descriptive characteristics of the study population are shown in Table 1.
Characteristics of the Study Population.

Table 2 shows the results of the multivariate logistic regression analysis between living arrangements and depressive symptoms. We found statistically significant differences in depressive symptoms across living arrangements. Model 1 revealed a lower likelihood of depressive symptoms when living with spouse or living with children and spouse than when living alone. There was no difference in the likelihood of depression between the group living alone and the group living with children without a spouse.
Logistic Regression Analysis of the Relationship Between Living Arrangements and Depressive Symptoms.
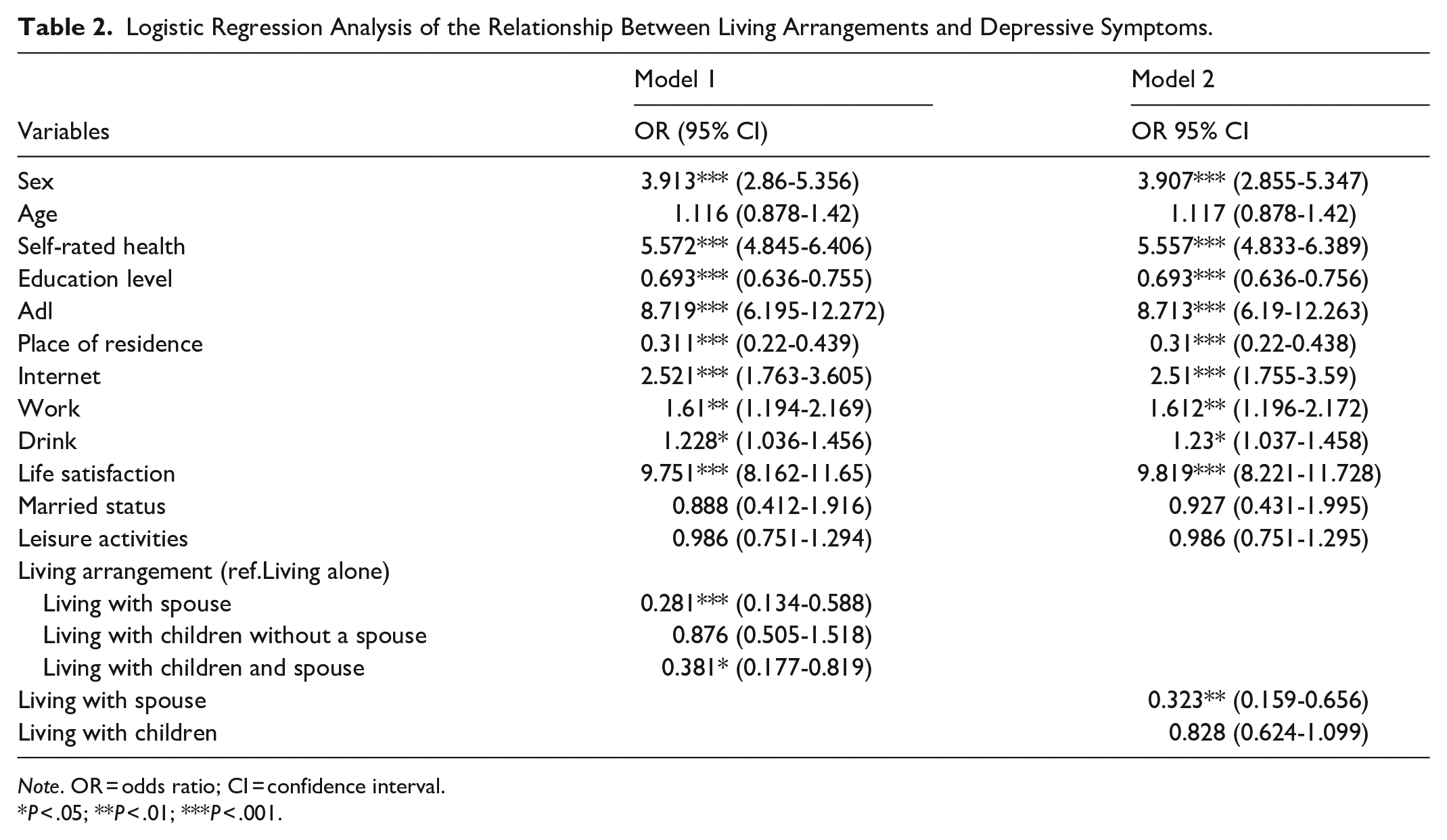
Note. OR = odds ratio; CI = confidence interval.
P < .05; **P < .01; ***P < .001.
Model 2 revealed that living with spouse was significantly associated with lower depressive symptoms and that living with children was not significantly associated with depressive symptoms.
Additionally, we found significant (P < .05) differences across gender, education, physical condition, residence, internet use, work, alcohol consumption, life satisfaction and depressive symptoms.
Table 3 reveals a gender-stratified analysis of the association between living arrangements and depressive symptoms, with men living with a spouse and men living with children and spouse having a lower risk of developing depressive symptoms than men living alone. However, there was no significant association between living arrangements and depressive symptoms in women. Moreover, the benefits of alcohol consumption were observed only in older men.
Associations Between Living Arrangements and Depressive Symptoms by Sex.
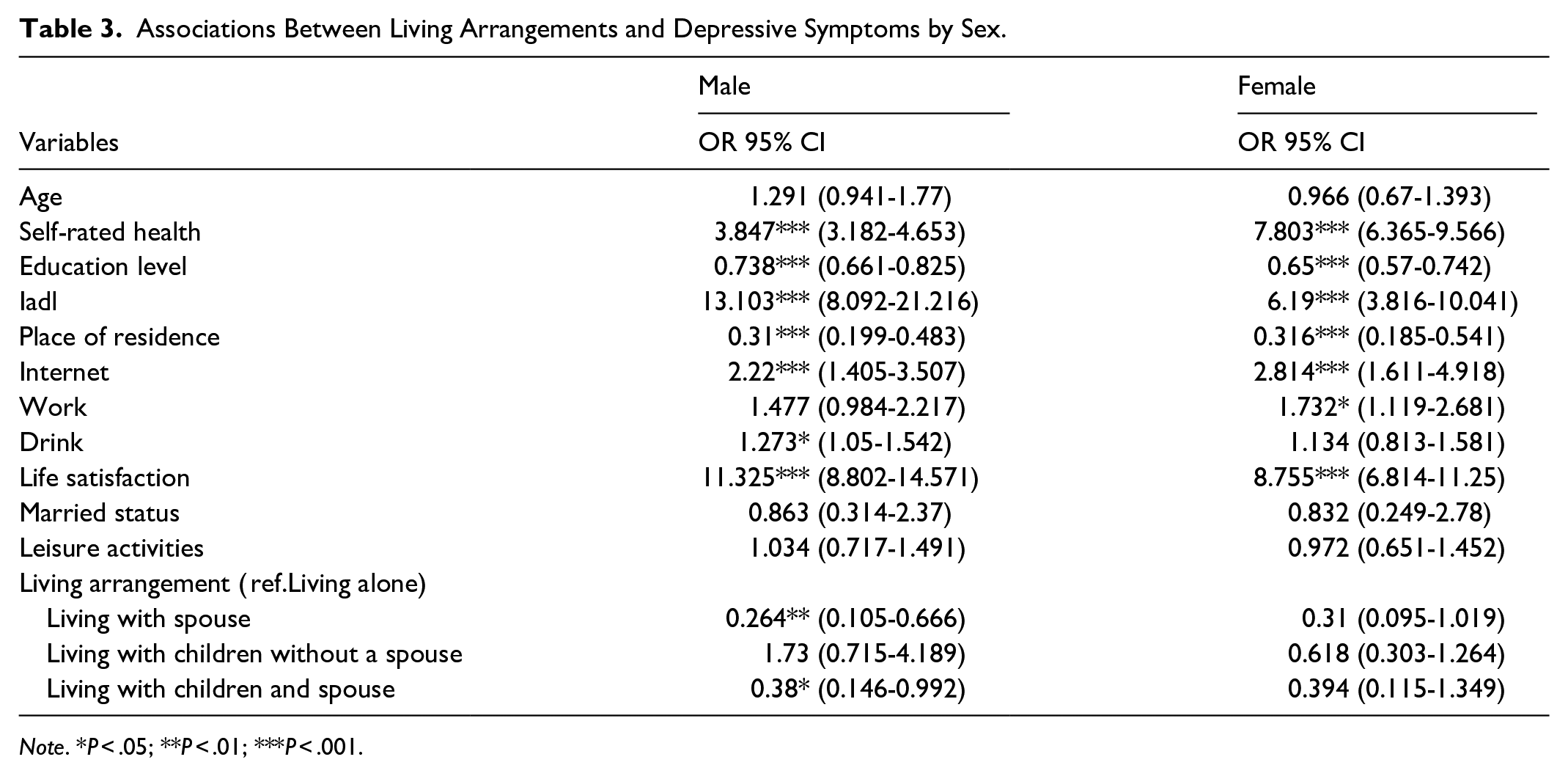
Note. *P < .05; **P < .01; ***P < .001.
Table 4 presents the results for the 4 different living arrangement styles and depression. We found that education, health, and life satisfaction were significantly related to depressive symptoms across all 4 living arrangements. Gender differences were not significant in the group not living with a spouse but with children and were significant in the other living arrangement relationships; place of residence was not significant in the group living alone and was significant in the other groups; use of the internet was not significant in the group living with children without a spouse and was significant in the other groups; work was not significant in the group living with children without a spouse and in the group living with a spouse and children and was significant in the other groups; alcohol consumption was significant only in the group living with spouse and children and not significant in the other groups.
Analysis of the Influencing Factors Associated With Depressive Symptoms With Different Living Arrangements.
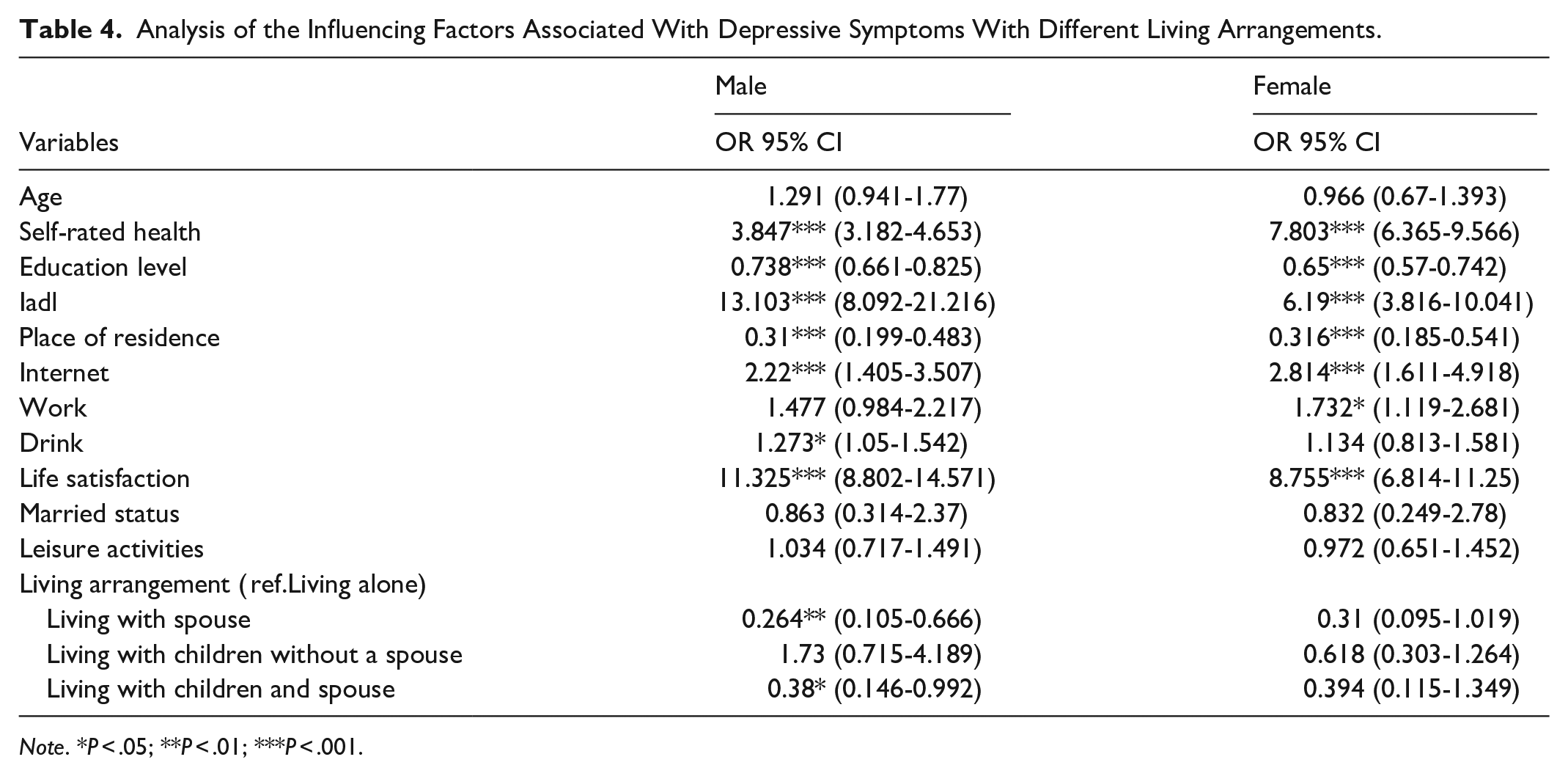
Note. *P < .05; **P < .01; ***P < .001.
Discussion
In the context of China’s growing population aging, different living arrangements can influence older adults’ daily lives, and numerous studies have indicated that living arrangements may be an important predictor of mental health.29-31
This study found that older adults living with spouse or living with children and spouse have a significantly lower risk of depression compared to those living alone. The underlying mechanism for this result is that living alone easily exposes older adults to social isolation and loneliness, both of which are significant contributors to exacerbated depressive symptoms.32,33 In contrast, within the Chinese context where traditional family values still hold influence, the instrumental support (such as daily care and assistance with tasks) and emotional support (such as emotional comfort and companionship) gained from living with family members play a positive role in alleviating depression.34,35
However, the key finding of this study is that older adults living with children without a spouse show no statistically significant difference in depression risk compared to those living alone. This result is inconsistent with the theoretical expectation that “family care reduces depression.” The transformation of living arrangements during China’s social transition is a possible reason for this discrepancy. Declining fertility rates and urbanization have jointly eroded the foundation of the traditional “multigenerational co-residence” family structure. 36 Population mobility among young adults has made spatial separation between generations the norm. Concurrently, the improvement of the social security system and the development of community services have further diminished the instrumental value of “living with children.” This has significantly reduced older adults’ dependence on their children for economic support and daily care. Consequently, the impact of “living with children” on mental health now depends more on the quality of emotional interaction than on the co-residence arrangement itself. Furthermore, the awakening of individual consciousness is driving a shift in living preferences, with older adults increasingly emphasizing their need for “autonomy in daily life.” If “living with children” is accompanied by intergenerational value conflicts (such as differences in consumption habits or lifestyles), it may instead become a psychological burden. This is also a crucial reason why “living with children” did not demonstrate a significant buffering effect against depression.
Based on this, we further hypothesize that among family members, the spouse, rather than the children, has a significant impact on the depression risk of older adults. The results of Model 2 confirm this hypothesis. This is because a spouse can not only provide more regular routines and meals37,38 but also, compared to children, offer more consistent emotional support and higher-quality companionship. The long-established emotional bond between spouses is difficult for children to replace. In contrast, support from children to older adults manifests more in instrumental aspects (such as material provision and handling affairs) and is often limited in frequency and depth of interaction due to multiple responsibilities like work and their own families. Additionally, the positive and negative influences of children on older adults may cancel each other out, resulting in a non-significant difference. On one hand, children can provide material support and emotional care; on the other hand, intergenerational conflicts or blurred privacy boundaries may impair the older adults’ well-being.39,40 This cancellation of positive and negative effects further weakens the protective role of “living with children.” These factors collectively explain why living with children shows no significant association with depressive symptoms.
Consequently, interventions should not only target solo-living older adults but also pay close attention to the subgroup living with children but without a spouse. This population has received limited attention in prior research, yet their depressive levels are now comparable to those of solo-living individuals. With rising divorce rates, this group is growing rapidly, 41 underscoring the need for tailored mental health support to address their unique challenges.
In addition, our study revealed that lower educational attainment was associated with depressive symptoms in older adults, which is similar to the results of a previous study. 42 One possible explanation is that educated older adults have greater cognitive ability and economic power, which improves their overall mental health. 43 Additionally, the prevalence of depressive symptoms is greater among rural than among urban older adults, which is consistent with the findings of previous studies.44,45 Disparities in social security between rural and urban areas may account for this difference. 46
We also found that working older adults were more likely to be depressed than those who did not work, possibly because a large proportion of rural older adults are required to work in agriculture to increase their income, and long hours of hard work may be detrimental to their health. 47
With respect to health, we found that all 4 variables describing health were significantly associated with depression, which is consistent with previous studies showing that physical health is an important foundation for mental health. 48 A decline in physical functioning in older adults can seriously affect their normal life and lead to negative emotions. 49 In addition, we found that alcohol consumption reduces the risk of depression compared with never drinking.50,51 A possible reason for this is that drinking is more commonly a group activity in China, where older adults can communicate emotionally with others through drinking, and drinking alone can release stress. Model 3 revealed that this association was only observed in the male subgroup, a finding potentially explained by the low proportion of drinkers among females, which may have limited the ability to detect an effect in this group.
With respect to social activities, the internet variable indicated that internet use could help alleviate depression in older adults, which is consistent with previously reported results that internet use can help older adults obtain more information and connect with others more often than groups that do not use the internet. 52 However, we found that the relationship between leisure activities and depressive symptoms was not significant, which is inconsistent with many findings.53,54 One possible explanation is that merely engaging in leisure activities has a negligible effect on reducing depressive symptoms, suggesting that the frequency of participation should also be considered. 55
We stratified the sample by gender and found that females exhibited a higher prevalence of depressive symptoms, consistent with prior research. 56 This finding may be attributed to the differences in the division of family responsibilities between men and women: under traditional Chinese values, it is customary for men to focus on external affairs and women to manage domestic duties. As a result, women usually assume caregiving responsibilities and bear heavier family burdens. Demanding duties and biological factors exacerbate their susceptibility to depression. 57 Notably, no significant association was observed between living arrangements and depressive symptoms among females. One possible explanation is that Chinese women, regardless of cohabitation partners, traditionally take on primary family care responsibilities, 21 such that changes in living arrangements have minimal impact on their mental health. In contrast, among males, those living with a spouse (with or without children) reported fewer depressive symptoms compared to those living alone—a pattern suggesting that spousal cohabitation provides males with essential daily care, thereby alleviating depressive tendencies in later life. 21
Finally, each lifestyle was also examined separately, and the study revealed that the relationship between each variable and depression was roughly the same as that in the overall sample but varied across the different living arrangements.
For the group not living with a spouse but with children, there was no association between gender and depressive symptoms, possibly because men are required to take on some of the family responsibilities without a spouse, and their depressive symptoms are relatively elevated without the assistance of a spouse.
Rural–urban differences in depression were not significant in the living alone group, possibly because interindividual contact is not as strong in urban areas than in rural areas, and reduced interaction with others may diminish the advantages of urban living.
Depression was not associated with work for those who lived with children without a spouse and those who lived with children and spouse, possibly because living with children is more likely to be supported by them than living in a household with no children, and work may be a means of maintaining socialization in addition to a means of earning a living; therefore, work and depression were not statistically associated.
Alcohol consumption plays a role in alleviating depression only in the group with spouses and children. First, the level of depression is lower in this group than in the other groups, and in the presence of a spouse and children, alcohol consumption is more likely to be a means of enriching life; therefore, alcohol consumption is significantly associated with a reduction in depression.
Although this study is grounded in China’s unique socio-cultural context, its core findings hold significant reference value for aging societies worldwide. In contemporary society, low fertility rates, shrinking family sizes, and intergenerational spatial separation driven by urbanization have become common global trends of aging. This lends cross-cultural universality to the central role of the spouse in the mental health of older adults.
Simultaneously, this study’s revelation of the “high depression risk among those living with children without a spouse serves as a warning to other aging societies. Sole reliance on children for instrumental support is increasingly inadequate to meet the psychological needs of older adults. Social support systems are required to compensate for the support gap arising from the absence of a spouse.
Strengths and Limitations
The article’s strengths lie in its use of the latest database, which helps derive results more relevant to contemporary life. Additionally, the study provides a more accurate categorization of the “living arrangements” variable based on census data, facilitating a deeper understanding of the relationship between different living arrangements and depression.
This study has several potential limitations. First, it relies exclusively on recently published cross-sectional data. Future researchers should acknowledge the inherent limitations of cross-sectional designs and build upon this work by conducting longitudinal studies to establish causal relationships between living arrangements, depressive symptoms, and other associated variables among older adults. Second, many data points in the questionnaire were collected through interviewer observation, meaning the reliability of these data partially depends on the consistency of interviewer training. Additionally, depressive symptoms—a key variable in this study—were measured using the CES-D scale. Since the analysis did not include clinically diagnosed depression, scale-based results may under or overestimate the true prevalence of depression in older populations. Furthermore, for older adults, particularly those in rural China, educational disparities may lead to varied interpretations of survey questions, as responses could be influenced by individual understanding of items and interviewers’ clarification—factors that may affect result accuracy. Next, as the sample size of older adults living in institutions was relatively small and there are significant differences between institutional care and home-based care, older adults living in institutions were excluded from the analysis. Future studies could collect a sufficient number of samples of older adults living in institutions to conduct more in-depth research on them. Finally, the current research did not distinguish between older adults who voluntarily chose to live alone and those who became solo-living due to spousal or child loss. Future studies could benefit from categorizing this population to explore subgroup differences in depression risk.
Conclusions
Older adults who lived alone or lived with children without a spouse are more likely to experience depressive symptoms. It is the spouse, not the children, that influences depressive symptoms in older adults. The government and communities should provide differentiated social services for older adults based on their family living compositions. For example, for older adults without spouses, more social networking activities can be organized to provide them with opportunities to meet new friends, increase social interactions, enrich their daily lives, and expand their social circles. For older adults living with spouses, men should be encouraged to pay more attention to their spouses’ mental health and assume more family responsibilities to reduce their spouses’ stress.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251366147 – Supplemental material for It Is the Spouse, Not the Children, That Influences Depressive Symptoms in Older Adults: Evidence From CHARLS
Supplemental material, sj-docx-1-inq-10.1177_00469580251366147 for It Is the Spouse, Not the Children, That Influences Depressive Symptoms in Older Adults: Evidence From CHARLS by Chaoqun Ma and Nanfu Hu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We are grateful to the China Center for Economic Research at Beijing University for providing us with the data, and we thank the CHARLS research and field team for collecting the data.
Ethical Considerations
During the field survey, each respondent who consented to participate was required to sign two copies of the informed consent form. One copy was to be retained by the respondent him/herself, while the other was stored in the CHARLS office and scanned and saved in PDF format. Informed consent was obtained from all the participants, and the study was approved by the Institutional Review Board of Peking University (IRB00001052-11015).
Author Contributions
N.H. and C.M. designed the study. N.H. contributed to data cleaning. N.H. performed the statistical analysis. N.H. and C.M. written first draft. The final manuscript was contributed by all authors.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.