
Abstract
Artificial intelligence offers students more personalised and adaptive learning, which encourages educators to better understand students’ learning processes. This study aims to determine the readiness levels of medical faculty students in medical artificial intelligence and to examine whether these levels vary based on gender and class year. The study was conducted with 322 medical students. Research data were collected using the “Medical Artificial Intelligence Readiness Scale for Medical Students.” Results showed that medical students rated themselves as moderate in the “cognition” and “vision” dimensions, slightly higher in the “ability” and “ethics” dimensions, and overall at a “neutral” level in medical artificial intelligence readiness. Compared to females, males showed significant differences at a “small effect” level in cognition, ability factors and overall scores. Regarding class levels, significant differences were found between 2nd graders and both 5th and 6th graders, favouring the 2nd graders at an “intermediate effect” level. In the cognition dimension, there was also a significant difference between the 2nd and 4th grades in favour of the 2nd grade and at the level of “small effect.” In order to increase medical artificial intelligence readiness of students, it is important to comprehensively include the subject in the medical school curriculum and to develop it according to needs. In future research, long-term follow-up studies aimed at improving medical students’ education in the field of medical artificial intelligence (AI) are considered to be very beneficial. Furthermore, future studies should also consider potential changes in medical AI readiness that may occur over time.
Introduction
Technology offers new solutions to improve the quality of healthcare services and facilitates access to these services. Information processing technologies, in parallel with the geometric increase in their capacity, have become capable of instantly processing data that is too complex for the human brain to calculate. In addition to sectors such as banking, manufacturing, agriculture, transportation, education, psychology, etc., artificial intelligence has also begun to have an impact on the field of health. 1
The concept of artificial intelligence (AI) was first described by McCarthy in 1956.2 -4 Artificial intelligence is the ability of a machine to imitate cognitive tasks such as image recognition, speech recognition, and caption generation. 5 In recent times, AI systems have gained popularity in the field of medicine. 6 AI systems can perform numerous functions to support clinicians in various medical fields, including drug development, disease diagnosis, health monitoring, clinical data management, and personalised medicine. 7 With the emergence of the latest AI tools and technologies, artificial intelligence has come to represent the ability of a digital machine to perform tasks typically associated with intelligent beings. These tasks include planning, disease diagnosis, summarisation, self-correction, decision-making, creativity, and enhancing learning, teaching, assessment, and education management.4,8 -12 The rapid growth of AI systems is increasingly transforming the ways in which people interact and communicate, live, learn, and work.13 -15 In education, artificial intelligence offers students more personalised and adaptive learning, which encourages educators to better understand students’ learning processes. Artificial intelligence has a high potential to enhance learning, teaching, assessment, and education management by providing instant feedback. 9 The impact of artificial intelligence in various fields, including medical education, has emerged as an important topic with the increasing integration of AI technologies. 16
It is anticipated that today’s AI applications will be able to help physicians make more reliable diagnoses, improve treatment outcomes, and reduce malpractice. Learning the fundamentals of artificial intelligence will help students understand its effects on medical procedures. 1 Educators can better prepare students for success in the digital age by using AI-powered tools. Through personalised learning platforms and intelligent tutoring systems, AI tools offer innovative ways to engage students and support learning outcomes. The use of AI tools in educational settings helps promote lifelong learning. 17
Considering the rapid changes and transformations in technology, the development of AI technologies and the potential challenges they pose will significantly impact medical education. Therefore, in order to use and adapt to the constantly evolving AI technologies, medical students should learn about clinical AI systems and modelling methods before graduating. Their awareness of these topics should be increased and they should be prepared for AI applications through professional practices. 18 In order to educate future physicians about artificial intelligence, it is important to conduct curriculum development studies that aim to equip students with AI-related knowledge and skills in curricula. 19
In education, readiness is considered an indispensable element of the teaching and learning process. 20 The emergence of a new behavioural change in education depends on the student’s level of readiness. Therefore, the student must possess the cognitive, affective and psychomotor behaviours necessary for acquiring new behaviours. 1 Measuring the level of readiness allows for guidance appropriate to the individual’s personal and characteristic traits from the very first day, enables the examination of the individual’s needs, and facilitates planning, programming and preparations in line with those needs. Therefore, measuring medical students’ perceived readiness for medical artificial intelligence is important in terms of guiding various educational design and development processes such as curriculum development, instructional design or needs analysis.1,18
The aim of this study is to determine medical students’ levels of readiness for medical artificial intelligence and to investigate whether these levels differ by gender and grade level.
Methods
Research Model
This study aims to determine medical students’ levels of readiness for medical artificial intelligence. It also determines whether their levels of readiness for medical artificial intelligence differ by gender and grade level. The study has been designed using the survey model. This study was designed as a cross-sectional study. The Medical Artificial Intelligence Readiness Scale for Medical Students (MAIRS-MS) developed by 1 Karaca, Çalışkan and Demir (2021) was used in the study. Data collection was conducted between March and May 2024 with volunteer participants. The Medical Artificial Intelligence Readiness Scale and the questionnaire were administered face-to-face to the sample group.
Participants
This study was conducted with students (n = 322) enrolled in the Faculty of Medicine at Trakya University during the 2023-2024 academic year and who voluntarily participated, following the approval of the Trakya University Non-Interventional Scientific Research Ethics Committee (Decision No: 16/13, Date: 23.10.2023). A sample of 322 students was selected from a population of 1851 students attending the 1st, 2nd, 3rd, 4th, 5th and 6th grades at the Faculty of Medicine with a 95% confidence level and a 5% margin of error. The required sample size was calculated using the Cochran formula. The formula is n = n0/(1 + [n0–1]/N), where n0 = Z 2 p(1–p)/e 2 . This calculation was made assuming a 95% confidence level (Z = 1.96), a 5% margin of error (e = 0.05), and a maximum variability (p = 0.5). Accordingly, the minimum sample size was found to be 318 for a population of 1851 students from 1st to 6th grade. Consequently, 322 students volunteered, thereby exceeding the minimum requirement. Students, who provided incomplete responses, were under the age of 18, were not enrolled in the Faculty of Medicine, or did not provide informed consent, were excluded from the analysis. The researchers personally checked the data upon receipt. Therefore, there was no missing data. In addition to administration of a scale, data on grade level and gender variables were collected. The distribution of the study participants by grade level and gender is presented in Table 1.
Distribution of Study Participants By Grade Level and Gender.

Data Collection Tool
The Medical Artificial Intelligence Readiness Scale for Medical Students (MAIRS-MS) developed by 1 Karaca, Çalışkan and Demir (2021) was used in the study. This scale was developed by working with students from the faculty of medicine and is aimed at determining medical students’ level of readiness for medical artificial intelligence. The scale consists of 22 items and 4 factors explaining 50.9% of the variance, and is structured as a Likert-type rating scale (1: strongly disagree to 5: strongly agree). The first factor is “Cognition”. This factor encompasses medical students’ perceived readiness regarding their terminology and understanding of the logic and logic of artificial intelligence and data science, particularly in the medical field. The second factor is “Ability.” This dimension primarily reflects medical students’ perception of their ability to integrate appropriate AI applications with professional medical knowledge and to avoid disclosing the situation. The third factor is “Vision.” This dimension reflects students’ perceptions of their ability to anticipate opportunities and threats related to AI. The final dimension is “Ethics.” This dimension reflects their perceived competence in adhering to legal and ethical principles in the use of AI and in data privacy.
The scale factors are as follows:
Cognition Factor: Items 1-8, Min: 8 Max: 40 points
Ability Factor: Items 9-16, Min: 8 Max: 40 points
Vision Factor: Items 17-19, Min: 3 Max: 15 points
Ethics Factor: Items 20-22, Min: 3 Max: 15 points
Medical Artificial Intelligence Readiness Scale Items 1-22, Min: 22 Max: 110 points
In this study, a confirmatory factor analysis (CFA) was conducted to determine whether the scale maintained its existing structure. The internal consistency coefficient, Cronbach’s alpha, was also checked. The values in the article that developed the scale and the values obtained from this employee’s data are presented in Table 2.
Values of CFA and Reliability.

The normality of the data distribution was assessed, and analyses were conducted to determine whether there was a statistically significant difference in medical artificial intelligence readiness levels according to grade level and gender.
Data Analysis
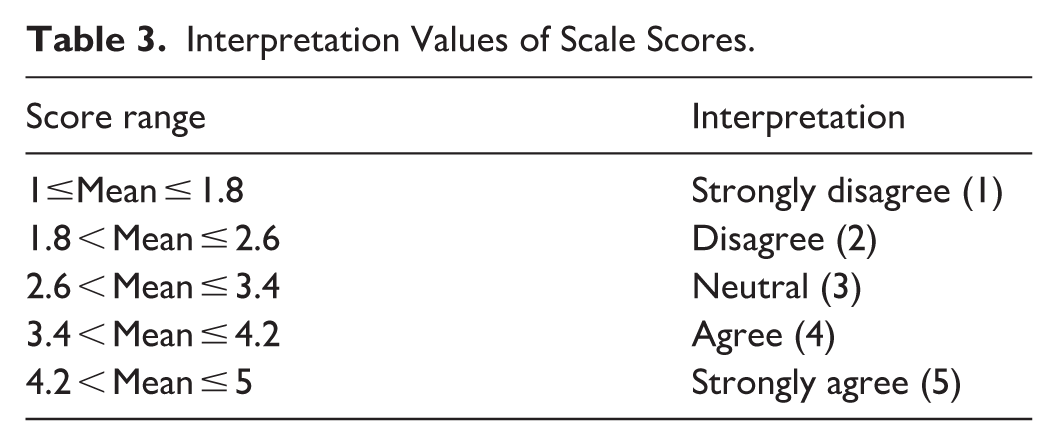
Mean and standard deviation were calculated to determine the overall status of medical students’ medical artificial intelligence readiness. When interpreting the means, the intervals were determined using the formula “range / number of groups” suggested by 24 Tekin (2019). Accordingly, based on the calculation 5–1/5 = 0.8, the means were interpreted as shown in Table 3.
Interpretation Values of Scale Scores.
To determine whether there was a significant difference between levels of readiness for medical artificial intelligence according to gender, the distributions were first checked. If the skewness and kurtosis values divided by their standard errors fell within the range of ±1.96, the t-test was conducted (for cognition); if this assumption was not met, the Mann-Whitney U test was performed (for ability, vision, ethics and overall test score). The significance value was set at 0.05.
To determine whether medical students’ levels of readiness for artificial intelligence differed significantly according to their grade level, the distribution by year was checked and it was determined that none of the dimensions or the total score met the criteria for normal distribution. Therefore, the Kruskal-Wallis test was performed. In cases of significant difference, the source of the difference was determined using the Mann-Whitney U test with Bonferroni correction.
Effect sizes were calculated for results that showed a significant difference. In line with Lakens, 25 the Cohen d coefficient for independent t-tests and the correlation coefficient (r) for Mann-Whitney U tests were calculated. If the Cohen’s d coefficient is <0, it is interpreted as an “adverse effect,” 0-0.19 as “no effect,” 0.2-0.49 as “small effect,” 0.50-0.79 as “intermediate effect,” 0.80 and above as “large effect” 26 (Cohen, 1988). The interpretation of the correlation coefficient r is different. If the correlation coefficient r is less than 0, it is interpreted as an “adverse effect,” 0-0.09 as “no effect,” 0.10-0.23 as “small effect,” 0.24-0.33 as “intermediate effect,” and 0.37 and above as “larger effect.” 26 All analyses were performed using JASP 0.95.4.0 software.
Results
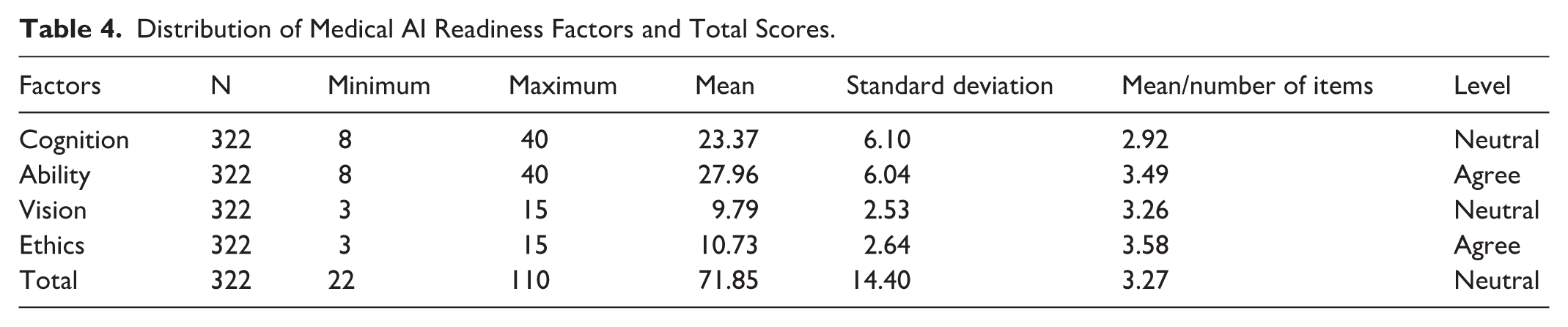
In order to determine medical students’ levels of readiness for medical artificial intelligence, the distribution of the scale factor scores and the total score were examined and the results are presented in Table 4.
When Table 4 is examined, it can be said that medical students felt that they had a moderate level of readiness in the cognition and vision factors of medical artificial intelligence, and a somewhat higher level of readiness in the ability and ethics factors. The total score is at the neutral level, and it can be stated that the prospective doctors felt moderately prepared in this area.
Distribution of Medical AI Readiness Factors and Total Scores.
To examine scores according to gender, the t-test was conducted for the cognition factor, which met the assumption of normality, while the Mann-Whitney U test was conducted for the vision, ability, ethics factors and total score. The results are presented in Tables 5 and 6.
Comparison of Cognition Dimension By Gender.

p < .05.
Tables 5 and 6 show a significant difference in the levels of medical AI readiness in favour of males in the cognition and ability factors, as well as in the total score, with a small effect size.
Comparison of Ability, Vision, Ethics Dimensions and Total Score By Gender.

p < .05.
In order to determine whether there was a significant difference between levels of medical AI readiness according to grade level, the distribution of the scale factor scores and the total score were examined according to grade level, and it was determined that none of them met the assumptions of normality. Therefore, the Kruskal-Wallis test was conducted, and in cases of significant difference, the Mann-Whitney U test was performed with Bonferroni correction to determine the source of the difference. The results are presented in Table 7.
When examined at the grade level, a significant difference was determined between the 2nd grades and the 5th and 6th grades in favour of the 2nd grades in the cognition and ability dimensions, as well as in the total score, with a medium effect size (Table 7). In the cognition dimension, there is also a significant difference between the 2nd and 4th grades in favour of the 2nd grades, with a small effect size (Table 7).
Comparison of All Dimensions and Total Scores By Grade Level.
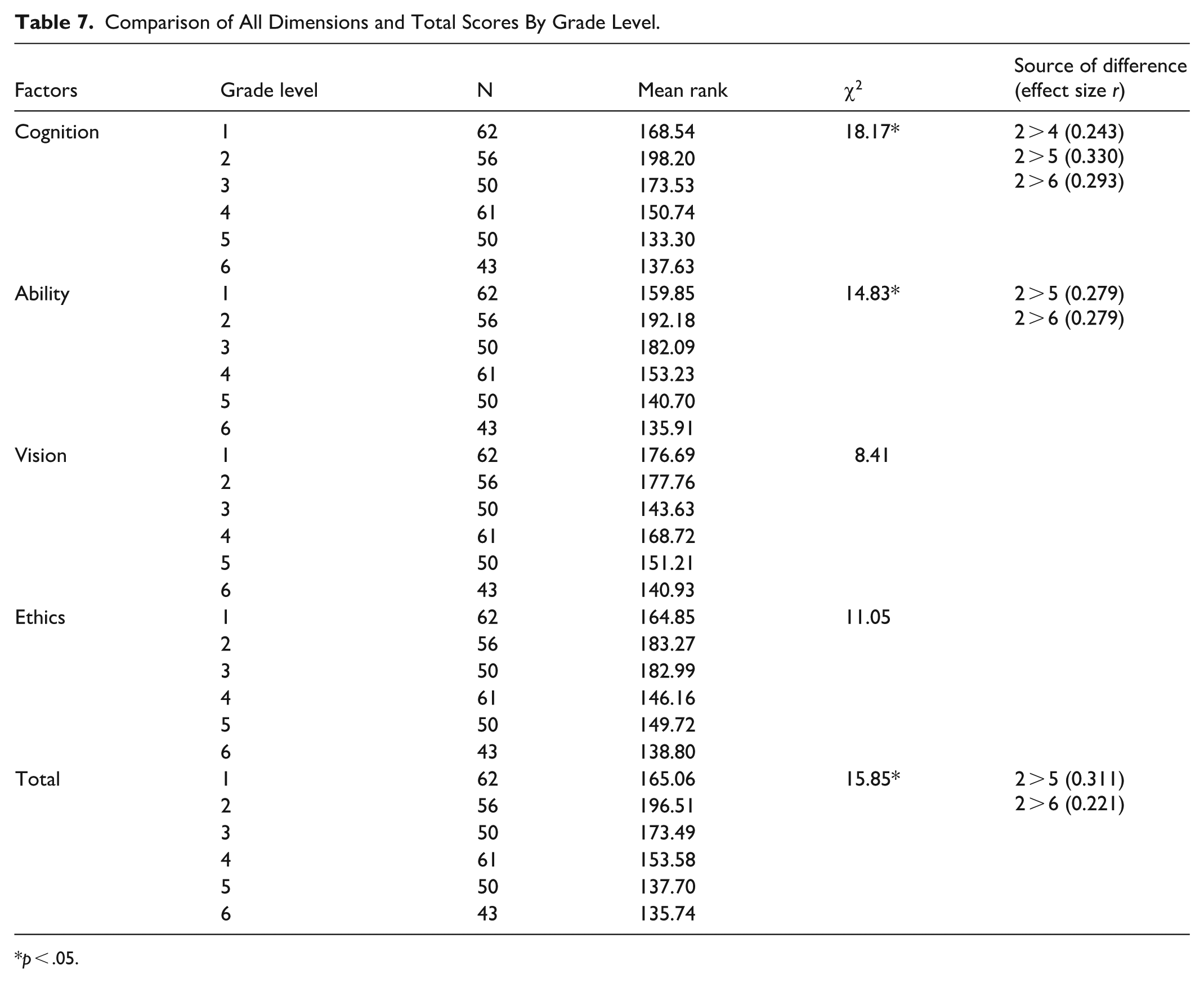
p < .05.
Discussion
The study was conducted to determine medical students’ levels of readiness for medical artificial intelligence. Analyses were also conducted to investigate whether there was a statistically significant difference in medical artificial intelligence readiness levels according to grade level and gender.
As a result of our study, it was determined that medical students perceived themselves as moderately prepared in the cognition and vision dimensions and somewhat better prepared in the ability and ethics dimensions with regard to medical artificial intelligence readiness. The total score was at the neutral level, and it can be stated that the students perceived themselves as moderately prepared in this area. The findings obtained in the scale dimensions can be explained by the educational and cultural context of medical education. The neutral outcome of the cognition dimension may be related to students’ lack of sufficient basic knowledge about what artificial intelligence is, how it works, how it is used in clinical practice, and the uncertainty surrounding its future. Students may be uncertain about the future impact of artificial intelligence in clinical practice. It is also thought that students may be uncertain or cautious about the future impact of artificial intelligence and its role in medical education. This may have led to neutral vision scores. The high ability score may be related to medical students’ familiarity with using digital information technologies to acquire clinical skills and their use of information technologies. Ethics is one of the most important components of medical education. Students take theoretical courses on medical ethics concerning patient safety, the importance of data privacy, and issues related to artificial intelligence. Therefore, their ethical awareness regarding artificial intelligence may be high. In line with the findings of our study, in another study aiming to evaluate the readiness of medical students for medical artificial intelligence and to determine whether this differed according to demographic characteristics, it was determined that the students’ overall level of readiness for medical artificial intelligence as well as their mean scores in the ability, vision and ethics subscales were high, while their mean scores in the cognition subscale were low. It was also determined that their overall readiness level for medical artificial intelligence was above average. 18 When the gender variable was examined in our study, a significant difference was found in the students’ perceptions of medical artificial intelligence readiness in favour of male students in the cognition and ability factors, as well as in the total score, with a small effect size. The reasons for this finding can be explained by social gender. The effects of men’s and women’s social gender roles on their relationship with technology are different. Male students generally have a higher perception of self-efficacy and more experience with technology. Research shows that males interact with technology more from an early age, are more confident in using digital tools, and are more likely to be directed towards STEM fields.27,28 This situation may contribute to male students being more open to artificial intelligence technologies and appearing more prepared to embrace innovations in this field. When examined in terms of grade level, a significant difference was determined between the 2nd grades and the 5th and 6th grades in favour of the 2nd grades in the cognition and ability factors, as well as in the total score, with a medium effect size. In the cognition dimension, a significant difference was also found between the 2nd and 4th grades in favour of the 2nd grades with a small effect size. In contrast to the results of our study, Denizli 18 found that female students had higher overall levels of readiness for medical artificial intelligence, as well as higher mean scores in the cognition, ability, and ethics subscales compared to male students. The study also revealed that 4th grade students had higher overall readiness levels than 1st and 3rd grade students; 4th grade students’ mean cognition subscale scores were higher than those of 1st, 2nd and 3rd grade students; 4th grade students’ mean ability subscale scores were higher than those of 3rd grade students; 6th grade students had higher mean scores in the vision dimension than 1st grade students; and 4th grade students had higher mean scores in the ethics dimension than 1st, 2nd, 3rd, 5th and 6th grade students. Students in higher grades may have increased awareness of the role of artificial intelligence in clinical practice, which may also lead to an increase in their readiness level. In another study conducted with medical students, it was determined that there was a moderate level of AI readiness among medical students and female students had significantly higher AI readiness scores compared to male students, and that 4th, 5th and 6th grade students had significantly higher medical AI readiness scores than 1st, 2nd and 3rd grade students. 29 In parallel with the findings of our study, the findings of another study conducted with medical students showed that students had a moderate level of readiness for AI. 30 In another study conducted with medical students, it was determined that the scores in the ability and cognition dimensions were higher than in the vision and ethics dimensions, and that they had an average score in terms of overall medical AI readiness. 31 A study conducted to evaluate readiness for medical AI among medical students showed that medical students had a high mean score in the four domains of medical AI readiness, that there were significant correlations between grade level and the ability, vision, and ethics dimensions of medical AI readiness, and that preclinical students had higher mean scores on the ability, vision, and ethics dimensions of medical AI readiness compared to clinical students, whereas there was no significant relationship between grade level and the cognition dimension of medical AI readiness, and gender was not significantly correlated with medical AI readiness. 32 In a study conducted with medical students from 17 universities in Malaysia, it was determined that students received an average score of 21 out of 40 for the cognition factor, 25 out of 40 for the ability factor, 10 out of 15 for the vision factor, and 11 out of 15 for the ethics factor, and overall, the students’ total mean score was 67 ± 14.8 out of 110. Participants performed relatively poorly in the cognition and ability factors compared to the vision and ethics factors. This suggests that medical students in Malaysia may not be sufficiently prepared to work with artificial intelligence, especially with regard to knowledge, understanding and application. 33
As a result of our study, the high scores in the ability and ethics dimensions of the MAIRS-MS show that students possess practical competence and ethical sensitivity regarding AI applications, while the moderate scores in the cognition dimension indicate that students do not possess sufficient knowledge about the fundamental concepts and theoretical foundations of artificial intelligence. In another study conducted with students recruited from the International Collaboration and Exchange Programme, it was revealed that participants’ mean levels of readiness in each factor of the MAIRS-MS were: cognition: 2.95 (SD = 1.06), ability: 3.20 (1.04), vision: 3.54 (0.90) and ethics: 3.42 (0.90). The overall mean AI readiness score was 3.18 (1.03). These results emphasised the need for increased efforts to strengthen students’ readiness for artificial intelligence. 16 In a study conducted with medical and health science students, it was determined that students’ medical AI readiness was poor. When the four dimensions of medical AI readiness were compared, students rated the ability dimension as the highest, followed by ethics and then vision. The cognition dimension received the lowest mean score among the four dimensions. 34
In a study conducted with dentistry students, it was revealed that the total scores for the factors of the scale (cognition, ability, vision and ethics) were 23.92, 27.65, 9.98 and 10.64, respectively, and that dentistry students had a moderate level of readiness for medical artificial intelligence. It was determined that there was a significant difference according to grade level, but no significant difference according to gender. 35 In another study conducted with dentistry students, the AI readiness scores were average (3.3 ± 0.64 out of 5); participants appeared to be better prepared in the vision and ethics dimensions, but showed lower levels of readiness in the cognition and ability dimensions. It was determined that students’ readiness for medical artificial intelligence was at a moderate level. No significant correlation was found between readiness scores and age, gender or grade level. The highest readiness score among participants was in the vision dimension, followed by ethics and ability dimensions, while the lowest readiness score was in the cognition dimension. Students perceived themselves as relatively well prepared in the ethics domain, which is related to compliance with legal and ethical norms when using AI technologies in healthcare. Although the results showed an average score (3.43 out of 5) for the ethics domain of the MAIRS-MS, it was concluded that this should be interpreted with caution, with a greater emphasis on ethical dilemmas related to artificial intelligence when educating dental students, in order to better prepare them as future healthcare professionals. 36
Limitations of the Study
This study has several limitations. The study is single-centre and cross-sectional. Therefore, the findings obtained from the study reflect only a specific time period and cannot be generalised to different periods or institutions. No power analysis was performed prior to data collection; therefore, the possibility of a Type II error cannot be entirely ruled out. Finally, variables such as the socio-economic background of the students were not examined.
Conclusion
The use of AI technologies can facilitate the execution of information-intensive complex processes and important repetitive tasks in every area of our lives. In order to increase knowledge, skills, awareness and readiness regarding the use of medical artificial intelligence, which is increasingly impacting medical practices, it is important to comprehensively include the subject in the medical school curriculum and to develop it according to needs. Therefore, it is recommended that medical schools consider including information-sharing mechanisms on artificial intelligence and develop educational programmes that will equip students with the competence to use artificial intelligence tools. For this purpose, it is necessary not only to provide theoretical training on artificial intelligence but also to increase clinical practice opportunities, and to integrate practical training hands-on applications related to AI use into medical education programmes.
In future research, long-term follow-up studies aimed at improving medical students’ education in the field of medical AI are considered to be very beneficial. Furthermore, future studies should also consider potential changes in medical AI readiness that may occur over time. In addition, a qualitative approach can be used to complement quantitative data. Through qualitative research, the different reasons for students’ readiness for artificial intelligence can be investigated in depth alongside quantitative methods. This can provide a richer discussion about different factors that affect students’ readiness for artificial intelligence. Since this study recorded students’ attitudes and readiness at only one point in their medical education, future research can conduct a longitudinal study to follow medical students at every stage of their professional development and record changes throughout the process.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261418133 – Supplemental material for Medical Students’ Readiness for Medical Artificial Intelligence (AI)
Supplemental material, sj-docx-1-inq-10.1177_00469580261418133 for Medical Students’ Readiness for Medical Artificial Intelligence (AI) by Albena Gayef and Gökhan Ilgaz in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We would like to thank all participants of the study.
Ethical Approval
We received ethics approval from the Trakya University Non-Interventional Scientific Research Ethics Committee (Decision No: 16/13, Date: 23.10.2023).
Consent to Participate
Written informed consent was obtained from all individual participants included in the study.
Author Contributions
All authors designed and secured funding for the study. A.G has provided substantial contributions to the conception, design of the work, literature review, collecting data and writing the manuscript. G.I was involved in analysing, interpreting data, and writing the method and results. All authors commented on and/or edited the paper. All authors give their final approval for this version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets of the study are available from the corresponding author; on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Human Ethics
This study was performed in line with the principles of the Declaration of Helsinki. All methods were carried out in accordance with relevant guidelines and regulations. We received ethics approval from the Scientific Researches Ethics Committee of the Medical School of Trakya University (Decision No: 16/13, Dated: 23.10.2023).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.