
Abstract
Violence during pregnancy is a significant public health concern, which is associated with different psychological consequences—including depression and suicidal ideation. Although several qualitative studies have been conducted, limited data are available on its prevalence during pregnancy and associated depression and suicidal ideation in Bangladesh. This study identifies the prevalence of violence against pregnant women and depression and suicidal ideation among affected individuals in rural Bangladesh. Our study is a secondary analysis of cross-sectional data, collected in a rural southern subdistrict in Bangladesh using the Edinburgh Postnatal Depression Scale (EPDS). The prevalence of domestic violence (DV), lifetime intimate partner violence (IPV), and IPV during pregnancy were 5.9% (n = 21; 95% CI: 3.7-8.9), 5.4% (n = 19; 95% CI: 3.3-8.3), and 9.9% (n = 35; 95% CI: 7.0-13.5), respectively. Among women exposed to DV, 66.7% (n = 14; 95% CI: 42.6-84.3) reported antenatal depression. Similarly, 68.4% (n = 13; 95% CI: 42.7-86.3) of those with a history of lifetime IPV and 42.9% (n = 15; 95% CI: 27.1-60.3) of those experiencing IPV during pregnancy had depressive symptoms. Suicidal ideation was present in 14.3% (n = 3; 95% CI: 4.2-38.7) of DV victims, 5.3% (n = 1; 95% CI: 0.6-33.8) of lifetime IPV victims, and 5.7% (n = 2; 95% CI: 1.3-21.4) of those experiencing IPV during their current pregnancies. The concerning prevalence of violence and associated mental health issues during pregnancy demands urgent targeted interventions, including policy reforms, health education, and community awareness initiatives.
Introduction
Violence against women is a major public health concern. One in 3 women worldwide experiences different forms of violence in their lifetime. 1 The World Health Organization defines violence against women as any act perpetrated by a partner, family member, or community that causes physical, sexual, or psychological harm. 2 This includes a range of harmful practices, including domestic violence. 3
Domestic violence (DV) includes psychological, physical, sexual, or economic abuse occurring within a family or between current or former partners, regardless of whether they live together. 4 Intimate partner violence (IPV), a specific form of DV, involves physical, sexual, and emotional abuse, along with controlling behaviors like isolation and restriction by the partner. 5 The difference between DV and IPV is, DV can be caused by household or family members, while IPV is committed by intimate partners.
According to the WHO, 641 to 753 million married or partnered women experience violence. 2 The global prevalence among the 15 to 49-year-old ever-partnered women is 27.0%. 6 A recent umbrella review identifies that 1 in every 4 women worldwide experiences at least one form of violence during pregnancy, with the highest prevalence in Africa and the lowest in Europe. 7 IPV is more common in low-income countries, and it increases the likelihood of depression, post-traumatic stress disorders, and suicidality. 8
The prevalence of DV in Asia ranges from 6.1% to 67.4%. 9 In South Asia, it is very high: 40% of married Indian women and 88.8% of married Pakistani women experience different forms of DV.10,11 In terms of IPV, Southern Asia has the second-highest prevalence (35.0%). 12 Bangladesh has the highest reported rate of IPV in the region, with 54.2% of women affected. 13
Violence during pregnancy has far-reaching physical and psychological consequences. In Bangladesh, 13.8% of maternal deaths occur due to violence, and nearly 25.0% of women experience pregnancy loss in the form of miscarriage, induced abortion, or stillbirth.14,15 A study conducted among Rohingya refugees found that different forms of IPV lead to forceful termination of pregnancies, miscarriage, and mental health disorders. 16
Violence against women is associated with a broad range of consequences for both maternal and child health. IPV leads to adverse pregnancy outcomes such as low birth weight (LBW) and preterm births. 17 It is a major risk factor for maternal suicidal behavior. 18 DV increases the risks of postpartum depression and postpartum blues in mothers. 9 Women with mental health disorders are susceptible to being victims of violence. 19 Unfortunately, the women’s mental health issues are neglected in Bangladesh.
Although several qualitative studies explored violence against women, the quantitative focus remains limited in Bangladesh. This study aims to address that gap by identifying the prevalence of DV, lifetime IPV, and IPV during pregnancy, as well as the mental health consequences—specifically depression and suicidal ideation—among affected pregnant women in rural southern Bangladesh.
A clear understanding of these issues will guide the development of strategic policies, community interventions, and mental health services to reduce violence, safeguard women’s rights and dignity, and promote psychological well-being.
Materials and Methods
Study Design and Setting
This is a secondary analysis of cross-sectional data collected between January 8 and January 30, 2024, at 2 healthcare facilities in Lohagara, a rural sub-district of Narail in southern Bangladesh. Facilities included the Upazila Health Complex, Lohagara, Narail, a government hospital, and Khan General Hospital, Lahuria, a private hospital.
According to the Bangladesh Government Health Bulletin (2025), the total number of residents in Lohagara is 262 501. From January to August, the estimated number of pregnant women was 6286, and the estimated number of births was 5715. The antenatal care receiving rate in the government hospital was 13.4% for the first visit, 10.5% for the second, and 5.5% for each of the last 2. The postnatal care receiving rate was 3.7% in the first visit, and 6.2% in the second visit. 20
The private hospital is situated in a remote village in Lohagara. Although there is no publicly available data on the services it provides, according to the hospital administration, around 350 pregnant women receive care or diagnostic services each month.
This study is designed to identify the prevalence at a single point in time. Due to the cross-sectional nature of the study, we are unable to determine the causal relationships.
Study Participants, Sample Size, and Sampling Technique
The study included pregnant women of different trimesters attending antenatal checkups at both hospitals during the study period. Non-residents, having cognitive difficulties, diagnosed with psychiatric disorders, or those who did not provide consent, were excluded from the study.
Participants were selected through systematic sampling. Every third patient attending antenatal care in both hospitals was invited for a face-to-face interview. The sample size was calculated using the formula:
Data Source, Measurement Tools, Management & Analysis
We used the ‘Characteristics of pregnant women in Lohagara, Narail, 2024’ data for this study. Two structured questionnaires were translated into Bengali for this data collection. The first included sociodemographic and health-related questions. The second was the validated Bengali version of the Edinburgh Postnatal Depression Scale (EPDS-B)21 -23 to evaluate antenatal depression. The EPDS consists of 10 items with a total score ranging from 0 to 30. A score of 10 or higher indicated probable antenatal depression.24,25 Suicidal ideation was assessed based on a score above 0 on the final EPDS item.26,27
A 15-min interview was conducted in a separate room to ensure confidentiality. Eligible participants provided written informed consent before the interview. We analyzed data using STATA version 17. The study followed the STROBE guidelines for cross-sectional studies. 28
Result
Sociodemographic Characteristics of Participants
The cleaned version of the original dataset contained 354 observations, with all missing values deleted by listwise deletion. Among participants, the majority (92.9%, n = 328) were 18 to 35 years old. Over half (53.8%, n = 190) were in their second trimester of pregnancy. A small proportion (7.3%, n = 26) had no formal or primary-level education, and most respondents were unemployed (96.1%, n = 340). Approximately one-quarter (26.3%, n = 93) reported a monthly household income below 10 000 BDT. The vast majority of participants (96.3%, n = 341) were Muslim, and nearly half (48.6%, n = 172) married before the age of 18 (Table 1).
Baseline Characteristics of Pregnant Women (n = 354).

Prevalence of Violence Against Pregnant Women in Bangladesh
As shown in Table 2, the prevalence of domestic violence (DV) among pregnant women was 5.9% (n = 21; 95% CI: 3.7-8.9). The lifetime prevalence of intimate partner violence (IPV) was 5.4% (n = 19; 95% CI: 3.3-8.3), while IPV during the current pregnancy was 9.9% (n = 35; 95% CI: 7.0-13.5).
Prevalence of Violence Against Pregnant Women (n = 354).

Prevalence of Antenatal Depression Among Pregnant Women Experiencing Violence
Figure 1 illustrates that antenatal depression was reported by 66.7% (n = 14; 95% CI: 42.6-84.3) of those who experienced DV, 68.4% (n = 13; 95% CI: 42.7-86.3) of those with a history of lifetime IPV, and 42.9% (n = 15; 95% CI: 27.1-60.3) of those who experienced IPV during pregnancy. Additional information on the underlying data is provided in the Supplemental Materials.
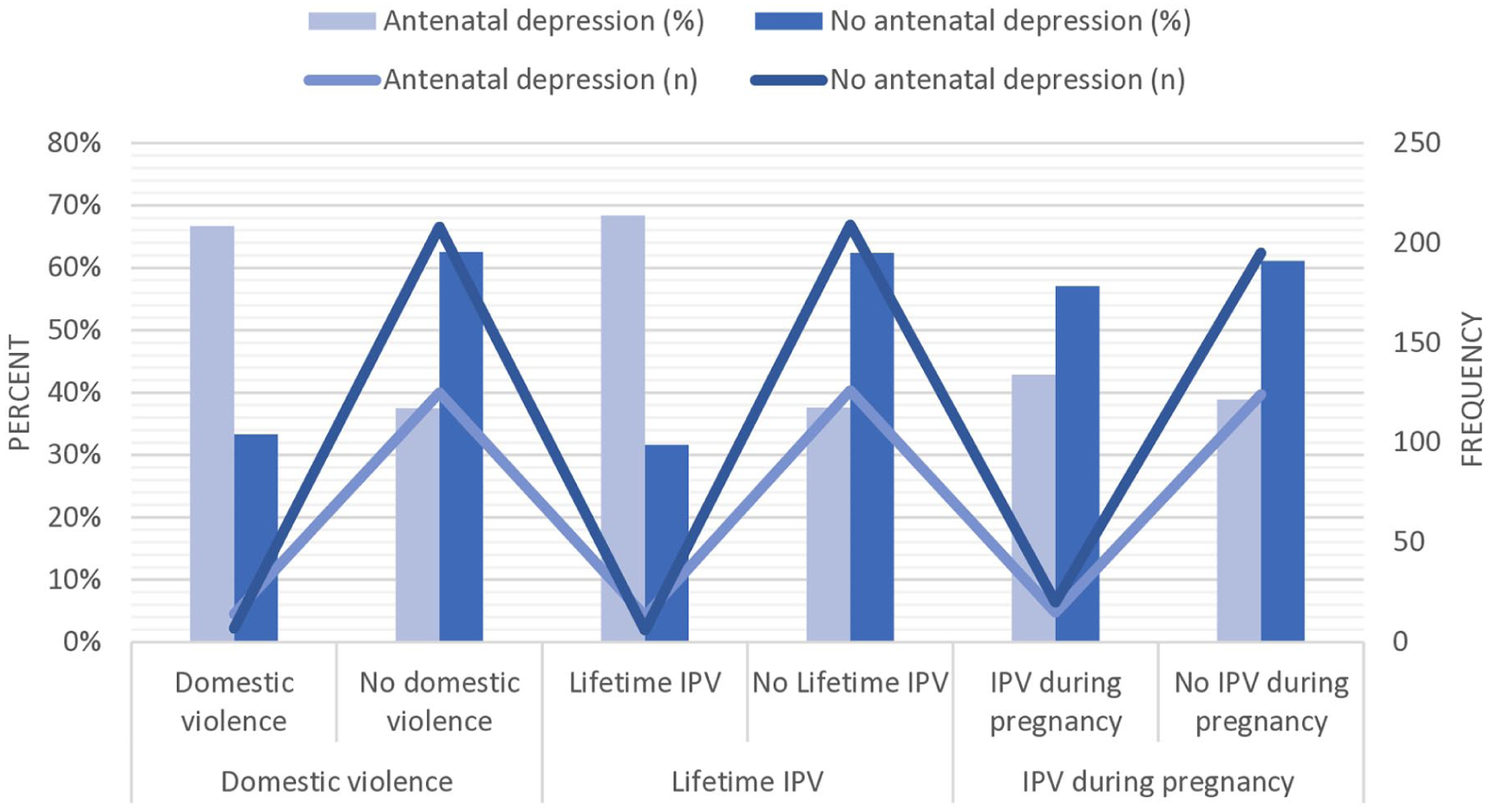
Antenatal depression among women experiencing violence (n = 354).
Prevalence of Suicidal Ideation Among Pregnant Women Experiencing Violence
As presented in Table 3, the prevalence of suicidal ideation among DV victims was 14.3% (n = 3; 95% CI: 4.2-38.7). Among those reporting lifetime IPV, the prevalence was 5.3% (n = 1; 95% CI: 0.6-33.8), and among those experiencing IPV during pregnancy, it was 5.7% (n = 2; 95% CI: 1.3-21.4).
Suicidal Ideation Among Pregnant Women Experiencing Violence (n = 354).

Discussion
This study identifies the prevalence of violence against pregnant women and examines antenatal depression and suicidal ideation among victims in rural southern Bangladesh. Although several qualitative studies have been conducted, few quantitative studies are available on this concerning issue, especially in rural settings. This study provides a quantitative assessment to understand the current status of violence, as well as depression and suicidal ideation during pregnancy in low-resource settings.
Our findings indicate that 5.9% (n = 21; 95% CI: 3.7-8.9) of participants experience domestic violence (DV), 5.4% (n = 19, 95% CI: 3.3-8.3) report lifetime intimate partner violence (IPV), and 9.9% (n = 35, 95% CI: 7.0-13.5) experience IPV during pregnancy. Women exposed to DV, 66.7% (n = 14; 95% CI: 42.6-84.3) report antenatal depression. The prevalence of depression is 68.4% (n = 13; 95% CI: 42.7-86.3) among those with a history of lifetime IPV and 42.9% (n = 15; 95% CI: 27.1-60.3) among those exposed to IPV during pregnancy. Suicidal ideation is 14.3% (n = 3; 95% CI: 4.2-38.7) among DV victims, 5.3% (n = 1; 95% CI: 0.6-33.8) among those with lifetime IPV, and 5.7% (n = 2; 95% CI: 1.3-21.4) among those currently experiencing IPV.
The prevalence of IPV during pregnancy in South Asian Countries is 23.4%. 29 In Pakistan, 51.0% of women experience DV in the 6 months before or during pregnancy, and 16.0% develop suicidal ideation as a consequence. 30 The prevalence of violence during pregnancy is 15.0% in India, with 72.0% suffering from depression. 31 Our findings indicate that rates of DV (5.9%) and IPV in pregnancy (9.9%) are lower in Bangladesh compared to India and Pakistan, probably because of cultural and regional variations.
A pre-pandemic study in 2 eastern subdistricts of Bangladesh identifies a 66.4% prevalence of IPV during the first 6 months of pregnancy, 32 which is relatively high compared to our findings. The probable reason for this variation can be the differences in the study populations; the previous study collected data from postpartum women, while our study participants are antepartum women. The prior research cannot completely ignore the possibility of recall bias, especially when postpartum women are emotionally vulnerable due to hormonal changes. Study periods and locations are also different. Some other studies identify a 36.8% prevalence of DV and approximately 45.0% IPV 33 during COVID-19. However, these studies explore violence against the female population in general, but our study primarily focuses on pregnant women.
A broad range of factors contribute to violence against South Asian women, which commonly includes male-dominated family structures and rigid cultural traditions. 34 In parts of India and Pakistan, women are often treated as second-class citizens, and minor mistakes are met with severe punishment. 34 Male child preference is another contributing factor for IPV during pregnancy in India. 35
Cultural constraints may work as an important factor for violence in Bangladesh. Approximately 90.0% of the population is Muslim. 36 Although Islam prohibits cruelty and family violence, patriarchal interpretations often misrepresent religious teachings. In some rural communities, religious leaders enforce social norms under the guise of religion, sometimes justifying abuse.37,38 Many rural families have limited awareness of the physical and mental health needs of pregnant women. Some families even justify violence against expectant mothers due to the likelihood of giving birth to a female child.
Additionally, a significant portion of Bangladeshi women internalize these norms: nearly one-third justify being beaten by a husband.39,40 Low education and conservative religious beliefs are associated with this justification. 41 Women exposed to violence in childhood are more likely to tolerate IPV. 32
Violence is associated with different health consequences, including prenatal depression and adverse birth outcomes. 42 In rural Bangladesh, 39.0% of pregnant women suffer from antenatal depression, and IPV is a key risk factor. A study conducted among the Rohingya refugees in Bangladesh explores different forms of IPV, including physical, economic, emotional, and sexual abuse, that Rohingya women experience. These abuses have significant consequences on their mental health and pregnancy outcomes. Victims often experience forceful termination of pregnancies, miscarriage, as well as anxiety, depression, and post-traumatic stress disorder (PTSD). 16
Suicide is a leading cause of maternal death globally 43 and is responsible for 20% of postpartum deaths. 44 In Bangladesh, 11.0% of pregnant women experience suicidal thoughts, and 6.5% attempt suicide. 45 Exposure to IPV during pregnancy significantly increases the risk of suicidal ideation. 46
We used data collected from both government and non-government hospitals to capture the diversity of the population. Participants were selected regardless of their background, education, employment, or socio-economic status. However, in the context of rural Bangladesh, there might be a subset of the population that does not attend antenatal care unless they face severe physical challenges. Additionally, the marginalized population has limited access to healthcare services, and severely sick women may be unable to attend these healthcare facilities. Therefore, this study may be subject to a generalizability bias.
As this is a secondary analysis, we have limited control over modifying or expanding the previous data collection process. This study identifies prevalence at a single point in time. However, causal relationships between variables cannot be assessed due to the cross-sectional nature.
Additionally, our study participants are free from psychiatric abnormalities, but previous mental health disorders might influence depression and suicidal ideation. We used the Edinburgh Postnatal Depression Scale (EPDS) for measuring suicidal ideation, which is a self-reporting questionnaire. Depression and suicidal ideation were measured based on participants’ statements. There is a possibility of underreporting due to sociocultural, psychological, and other barriers. Although some studies used the EPDS as a measure of suicidality,26,27 it may not completely reflect the severity and complexity. Further studies are recommended using multidimensional measures.
Conclusion
Violence against pregnant women in rural Bangladesh is a serious public health concern. Approximately 1 in 20 pregnant women experiences domestic violence, and nearly 1 in 10 reports intimate partner violence (IPV) during pregnancy. Among those exposed to violence, at least 40.0% suffer from antenatal depression, and over 5.0% report suicidal ideation.
Despite the gravity of the issue, limited measures have been implemented to address it. To reduce the burden, enforcement of robust legislation is required that protects women’s rights and holds perpetrators accountable. While the government has made efforts to promote women’s empowerment, these initiatives must be expanded to the grassroots level. Community-based health education programs and awareness campaigns must be implemented to engage women, families, and communities in addressing the issue.
A coordinated, multisectoral response is essential. Policymakers, law enforcement agencies, healthcare professionals, social activists, and local leaders should work collaboratively to develop and implement targeted policies and increase public awareness. Community health workers can play a proactive role in educating families about the importance of regular antenatal visits and mental well-being during pregnancy. Integrating routine IPV and depression screening during antenatal visits will help early detection and management, which can prevent their progression to suicidal ideation.
Through sustained, collaborative efforts, it is possible to significantly reduce violence against pregnant women and mitigate its devastating effects on mental health.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261418128 – Supplemental material for Violence During Pregnancy, Prevalence of Antenatal Depression and Suicidal Ideation Among Women Experiencing Violence: A Cross-Sectional Study
Supplemental material, sj-docx-1-inq-10.1177_00469580261418128 for Violence During Pregnancy, Prevalence of Antenatal Depression and Suicidal Ideation Among Women Experiencing Violence: A Cross-Sectional Study by Rifa Tamanna Mumu, Md Parvez Shaikh and Shadman Sakib Ayan in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580261418128 – Supplemental material for Violence During Pregnancy, Prevalence of Antenatal Depression and Suicidal Ideation Among Women Experiencing Violence: A Cross-Sectional Study
Supplemental material, sj-docx-2-inq-10.1177_00469580261418128 for Violence During Pregnancy, Prevalence of Antenatal Depression and Suicidal Ideation Among Women Experiencing Violence: A Cross-Sectional Study by Rifa Tamanna Mumu, Md Parvez Shaikh and Shadman Sakib Ayan in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
I am grateful to North South University for allowing me to conduct this research. I am thankful to Dr. Dipak Kumar Mitra, Professor and Dean, North South University, for his guidance. My gratitude extends to Dr. S M Mashud, UH&FPO, Upazila Health Complex, Lohagara, Narail, for his support in conducting the study.
Ethical Considerations
This study uses previously collected IRB-approved data from a prior study. The ethical approval for the original data collection was obtained from the Institutional Ethics Committee of North South University (Approval Number: 2023/OR-NSU/IRB/1224). Additional permissions were secured from both participating hospitals. Informed written consent was obtained from all participants aged 18 years or older. For participants under 18, consent was obtained from legal guardians. Participants were informed about the purpose of the study, potential risks and benefits, and assured of the confidentiality of their responses. Data were collected anonymously. The present study is a secondary analysis of the dataset. We referred patients with depressive symptoms or suicidal ideation to the District Hospital for specialist counseling. Those who were victims of any form of violence were referred to the Upazila Health and Family Planning Office for additional support and follow-up through the social welfare services.
Consent to Participate
During the original data collection, permission letters were obtained from both school authorities. Informed written consent was obtained from parents or legal guardians of participants. Informed written assent was taken from all participants before data collection. Respondents were assured of the confidentiality of information.
Consent for Publication
Not applicable as the data were collected anonymously, and no identifying information was included.
Author Contributions
Conceptualization, Methodology, Investigation, Data curation, Formal analysis, Review: Rifa Tamanna Mumu. Supervision, Writing (Original draft preparation, and Editing), Resources, Review: Md Parvez Shaikh. Data collection, curation, Review: Shadman Sakib Ayan. All authors approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available on ![]() . Characteristics of pregnant women in Lohagara, Narail, 2024. DOI: 10.6084/m9.figshare.24994110v3
47
. Characteristics of pregnant women in Lohagara, Narail, 2024. DOI: 10.6084/m9.figshare.24994110v3
47
Original Study
Prevalence and associated factors of antenatal depression in rural Bangladesh.
Clinical Trial Number
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.