
Abstract
Long COVID increases healthcare utilization, yet differences in healthcare spending patterns between individuals with and without long COVID remain poorly characterized, especially at the national level. To evaluate differences in healthcare expenditures among U.S. adults with and without long COVID using nationally representative data. This cross-sectional study analyzed data from the 2022 Medical Expenditure Panel Survey (MEPS), including 16 762 unweighted adults (weighted population: 239 915 159). Healthcare spending outcomes included total expenditures and specific categories including office-based care, outpatient services, emergency room visits, hospital admissions, home healthcare, and prescription medications. A survey-weighted generalized linear model (GLM) with a log link and gamma distribution was used to estimate adjusted differences in expenditures between groups. Individuals with long COVID had significantly higher total healthcare expenditures (mean $11 567; SD $25 334) compared to those without long COVID ($7448; SD $21 734, P < .01). After adjusting for demographic characteristics, insurance status, chronic conditions, and other potential confounders, individuals with long COVID incurred 40% higher total expenditures (β = 1.40, P = .01). Expenditures were significantly elevated for office-based visits (35% higher; β = 1.35, P = .02) and outpatient services (118% higher; β = 2.18, P < .01). No significant differences were found in emergency room, hospital admissions, or dental care expenditures. Long COVID imposes a substantial financial burden on individuals and healthcare systems, primarily through increased outpatient and office-based service utilization. Understanding these spending patterns can help inform policy decisions, optimize healthcare resource allocation, and guide targeted interventions to manage long COVID more effectively.
Introduction
Long COVID, also referred to as post-acute sequelae of SARS-CoV-2 infection (PASC), is defined as symptoms persisting for at least 3 months after the initial infection and not explained by alternative diagnoses. 1 Long COVID has emerged as a significant contributor to healthcare burdens worldwide. Individuals affected by long COVID experience a wide range of prolonged symptoms, including fatigue, shortness of breath, cognitive difficulties, and mental health issues like anxiety and depression.2 -4 Symptoms may fluctuate over time and vary in severity, making diagnosis and management challenging.
Several risk factors have been associated with the development of long COVID. Studies suggest that individuals who experienced severe acute COVID-19 illness, required hospitalization, or had preexisting conditions such as obesity, diabetes, hypertension, asthma, and autoimmune diseases may be at higher risk.5 -7 Additionally, women, older adults, and those with multiple comorbidities appear to be disproportionately affected. 6 There is also evidence suggesting that individuals with a history of mental health disorders or those who were unvaccinated at the time of COVID-19 infection may be at increased risk of developing long COVID.8,9 The course of long COVID varies, with symptoms lasting weeks to over a year. Some people recover over time, while others face long-term health issues. Research suggests that ongoing inflammation, nervous system dysfunction, and immune system problems may explain persistent symptoms.10,11
The growing recognition of long COVID’s health impacts has led to increasing concerns about its economic burden on both individuals and healthcare systems. Research from various countries has indicated that individuals with long COVID tend to use healthcare services more frequently, including more visits to outpatient clinics, emergency departments, and rehabilitation services.12,13 This increased utilization leads to higher healthcare costs, 14 not only because of the volume of services used but also due to the complexity of managing the condition, which often involves multidisciplinary care, extensive diagnostic testing, and ongoing pharmacological treatments.15,16 Moreover, long COVID patients often experience hospital readmissions and a greater need for long-term care, further compounding healthcare costs. 17
Despite the growing body of research on healthcare utilization in long COVID, there remains a gap in the literature on direct comparisons of healthcare spending between individuals with and without long COVID. While long COVID drives higher utilization, the exact differences in healthcare expenditure have not been comprehensively studied. Previous studies have estimated the increased healthcare costs associated with long COVID,18 -20 however, they often focus on specific healthcare systems or localized data and tend to exclude indirect or less visible cost domains-such as outpatient rehabilitation, home health services, and prescription drugs- potentially overlooking the full scope of healthcare expenses.
Given the increasing recognition of long COVID as a significant public health challenge, understanding the differences in healthcare spending between those with and without the condition is essential. Identifying these disparities is crucial for informing healthcare policies, optimizing resource allocation, and developing targeted interventions to improve care for individuals affected by long COVID, while also alleviating financial strain on healthcare systems. This study aims to address this gap by providing a detailed breakdown of healthcare spending across various categories and offering a comprehensive comparison of expenditures between individuals with and without long COVID using national survey data.
Methods
Data and Resources
This study used a cross-sectional design with data from the 2022 Full Year Consolidated Medical Expenditure Panel Survey (MEPS), a nationally representative survey of the U.S. civilian noninstitutionalized population. The MEPS provides comprehensive data on a wide range of variables, including demographic characteristics, income, health status, disability status, access to healthcare, employment, health insurance coverage, healthcare utilization, and expenditures. It is an important resource for estimating national healthcare expenditures and analyzing the costs associated with various chronic conditions. 21 In 2022, the MEPS introduced a new set of questions specifically addressing long COVID, reflecting the growing importance of understanding the long-term effects of COVID-19 on healthcare systems. These additions enable researchers to examine the economic and healthcare impacts of long COVID, including patterns of healthcare use and associated costs. More detailed information on MEPS methodology and applications can be found in related publications and reports.21,22 Because publicly available data was used in this study, an Institutional Review Board (IRB) approval was not needed.
Inclusion and Exclusion Criteria
The study included adults aged 18 years and older from the 2022 MEPS dataset. Subjects were excluded if they did not respond to long COVID-related questions, provided inapplicable answers, or had missing values in key outcome or covariate variables.
Outcomes Measures
The primary outcomes assessed in this study were healthcare expenditures across multiple categories, including total healthcare expenditure, office-based expenditure, outpatient expenditure, emergency room (ER) expenditure, hospital expenditure, home healthcare expenditure, and prescription medication expenditure. Healthcare expenditures include both out-of-pocket payments and third-party payments from insurers such as private insurance, Medicaid, and Medicare. 21
Total healthcare expenditure refers to the sum of all medical-related spending incurred by an individual, covering payments made for office visits, outpatient care, hospitalizations, ER visits, home healthcare services, medications, vision aids, and other medical supplies and equipment. Office-based expenditures are defined as spending associated with medical consultations that occur in a healthcare provider’s office or a clinic setting, typically involving primary care or specialist consultations. Outpatient expenditures refer to spendings associated with non-hospital-based medical services where patients receive care without being admitted to a healthcare facility. ER expenditure, hospital expenditure, home healthcare expenditure, and prescription medication expenditure refer to spendings associated with ER visits, hospital admissions, home healthcare services and prescriptions, respectively. 21
Independent Variable
The independent variable was a binary indicator for long COVID, based on the MEPS question: “Has the person had symptoms lasting 3 months or longer that they did not have prior to having COVID-19?” This variable, added in the 2022 MEPS Long COVID module, allows identification of self-reported long COVID symptoms. Respondents answering “yes” were categorized as having long COVID.
Covariates
The regressions included several variables associated with healthcare spending.23 -28 These variables were age category (18-30, 31-40, 41-50, 51-64, and ≥65 years), sex (male vs female), race/ethnicity (non-Hispanic White, Hispanic, non-Hispanic Black, non-Hispanic Asian, non-Hispanic others/multiple races), census region (Northeast, West, South, Midwest), insurance type (private, Medicaid, Medicare, uninsured), marital status (married, widowed/divorced/separated, never married), high school graduation status (yes/no), family income as a percentage of the poverty line (poor, near poor, low income, middle income, high income), any physical limitations (yes/no), any cognitive limitations (yes/no), and smoking status (yes/no). Additionally, the study controlled for the presence of chronic conditions, which included hypertension, diabetes, asthma, high cholesterol, cancer, arthritis, heart disease, and pain. 29 The presence of pain was assessed using the MEPS question, “In the last 4 weeks, pain limits normal work.” Respondents who answered, “not at all” or “a little bit” were categorized as “no,” while those who responded “moderately,” “quite a bit,” or “extremely” were categorized as “yes.” Individuals with “inapplicable” responses to this question were excluded from the analytics.
Statistical Approach
Survey weights were applied to account for the complex survey design and to ensure estimates are nationally representative. Weighted summary statistics including means, standard deviations (SD), and proportions were calculated to describe characteristics of individuals with and without long COVID. Group differences were tested using t-tests for continuous variables and chi-square tests for categorical variables.
Given the right-skewed and heteroskedastic nature of healthcare cost data, we used survey-weighted generalized linear models (GLMs) with a log link and gamma distribution to assess adjusted differences in spending. This approach improves interpretability and statistical robustness over methods such as the ordinary least squares (OLS) in skewed distributions. 30 Covariate effects were exponentiated and interpreted as percent differences in healthcare expenditures relative to the reference categories. Standard errors were estimated using Taylor-series linearization as recommended for the MEPS. 21
To test the robustness of our findings, we also estimated survey-weighted 2-part models for all cost categories. The first part used a probit model to estimate the probability of incurring any expenditure, and the second part modeled the level of positive spending using a GLM. This modeling strategy addresses the prevalence of zero-expenditure observations, especially in categories like outpatient or home healthcare. In addition, we performed a sensitivity analysis categorizing participants into no COVID, short COVID, and long COVID groups to assess the extent to which outcomes differed between long COVID and short COVID. All analyses were conducted using Stata version 18.0, with statistical significance defined as a 2-sided P < .05. This study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines for cross-sectional studies (Supplemental Material). 31
Results
A total of 260 980 061 adults (unweighted n = 18 101) were included in the 2022 MEPS data. After excluding individuals who did not respond to the long COVID question (ie, missing responses), 925 882 (unweighted n = 58) subjects were excluded. Further exclusion of subjects with missing covariate data resulted in a final study population of 239 915 159 (unweighted n = 16 762). Among the final population, 93% reported no long COVID, while 7% reported having long COVID.
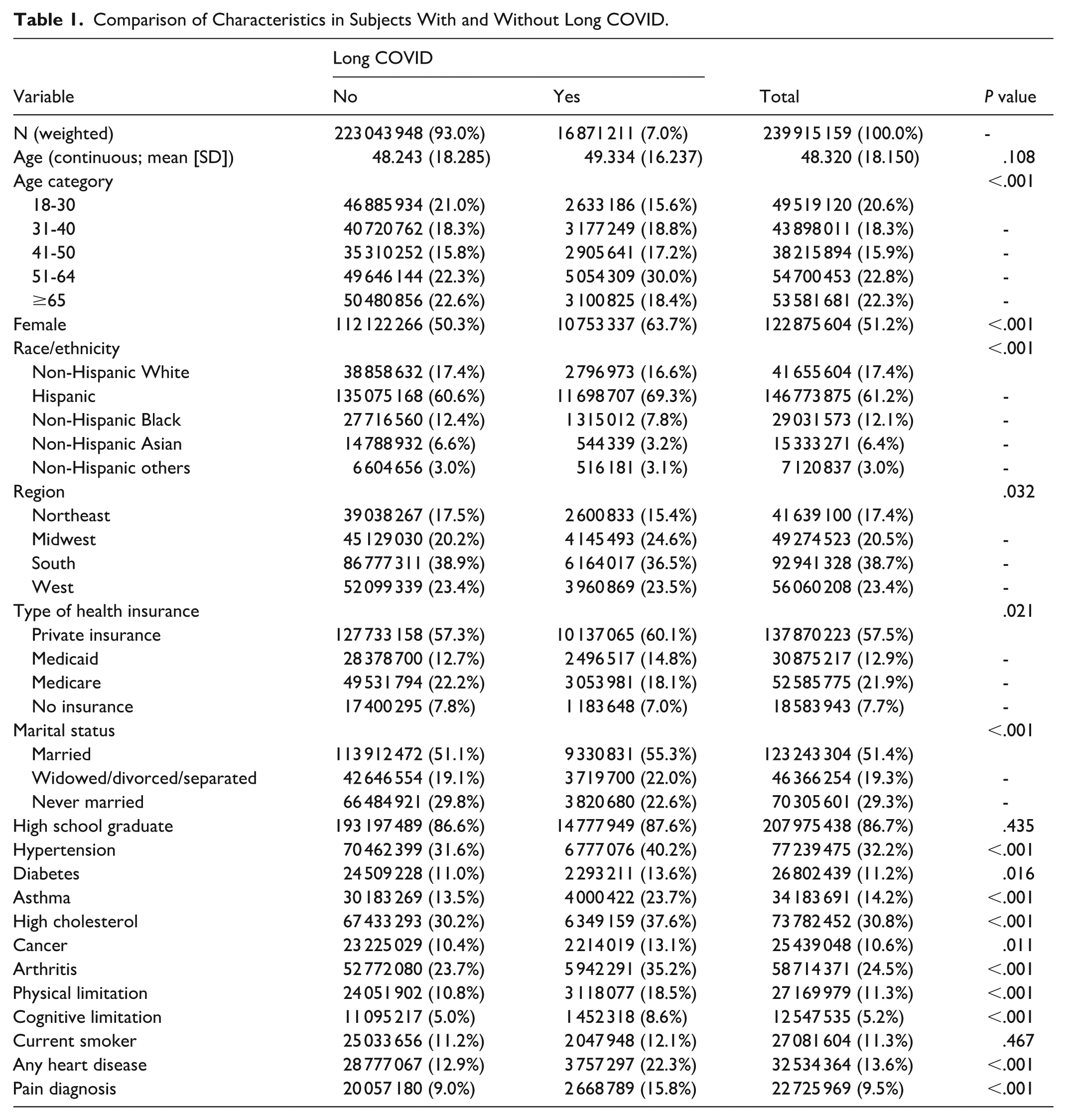
The highest prevalence among individuals with long COVID was in the 51 to 64 age group, reaching 30%, compared to 22.3% in those without long COVID. Approximately 51% of the population were female, and 61% identified as non-Hispanic White. Individuals with long COVID were more likely to report chronic health conditions compared to those without long COVID. In our study, 40% of individuals with long COVID reported hypertension, and 35% reported arthritis (Table 1).
Comparison of Characteristics in Subjects With and Without Long COVID.
The average total expenditure for individuals with long COVID was $11 567 (SD = $25 334), compared to $7448 (SD = $21 734) for those without long COVID (P < .01), indicating that individuals with long COVID spent $4119 more on healthcare. Specifically, office-based expenditures were higher among subjects with long COVID, averaging $2963 compared to $2026 for those without long COVID (P < .01), a difference of $937. Similarly, outpatient care spending was $1666 for individuals with long COVID versus $925 for those without (P < .01), a difference of $741. Prescription drug expenditures were also higher for individuals with long COVID, averaging $3671 compared to $1908 for those without long COVID (P = .03), a difference of $1763 (Table 2).
Healthcare Spending Comparisons Between Subjects With and Without Long COVID.

P values reflect comparisons of group means based on an unequal variance t-test.
Total healthcare expenditure refers to the sum of all medical-related spending incurred by an individual, covering payments made for office visits, outpatient care, hospitalizations, ER visits, home healthcare services, medications, vision aids, and other medical supplies and equipment.
In the regression analyses, after controlling for potential confounders, individuals with long COVID had 40% higher total healthcare expenditures compared to those without long COVID (β = 1.40, P = .01). Long COVID was also associated with increased spending in specific healthcare categories. Subjects with long COVID had 35% higher office-based expenditures (β = 1.35, P = .02) and 118% higher outpatient spending (β = 2.18, P < .01) than those without long COVID. Although prescription spending was 70% higher among individuals with long COVID, this difference was not statistically significant (β = 1.70, P = .06). In contrast, there were no significant differences in expenditures for emergency room visits (β = 1.07, P = .62), hospital admissions (β = .89, P = .61), or dental care (β = 1.15, P = .41) between the 2 groups. However, home health spending was 60% lower for individuals with long COVID compared to those without (β = .40, P = .03; Table 3).
Adjusted Estimates of Healthcare Spending Associated With Long COVID.

Note. Detailed multivariable regression results are provided in Appendix A1.
Female participants had 28% higher total healthcare spending than males (β = 1.28, P < .01). Additionally, chronic conditions such as diabetes (β = 1.62, P < .01), arthritis (β = 1.44, P < .01), and heart disease (β = 1.56, P < .01) were also independently associated with higher spending (Appendix A1).
Two-part models produced similar results to those from the GLM models total healthcare expenditure for those with and without long COVID was $10 382 and $9031, respectively, with the long COVID group spending $1351 more (P = .13). Outpatient expenditure ($1378 vs $1073; P = .11) and prescription expenditure ($3363 vs $2500; P = .13) were also higher in the long COVID group compared to those without long COVID (Appendix A2). However, they were not statistically significant.
In the sensitivity analysis comparing subjects categorized as no COVID, short COVID, and long COVID, those with long COVID as compared to no COVID had significantly higher total healthcare expenditures (β = 1.59, P = .01), office-based expenditures (β = 1.82, P = .01), outpatient expenditures (β = 2.56, P = .03), ER expenditures (β = 2.04, P = .04), and prescription expenditures (β = 3.34, P < .01). Subjects with short COVID also showed higher expenditures than the no COVID group in several categories, including office-based care (β = 1.55, P < .01), dental care (β = 1.33, P = .01), and prescription expenditures (β = 2.94, P < .01). That spending patterns also differ between long COVID and short COVID groups.
Discussion
This study provides new insights into the healthcare costs for individuals with and without long COVID using a nationally representative data from the 2022 MEPS. Our findings show that individuals with long COVID had significantly higher healthcare expenditures across several categories compared to those without long COVID. Individuals with long COVID incurred higher total healthcare costs, office-based visit costs, and outpatient expenditures. These differences remained statistically significant even after adjusting for covariates such as age, sex, race/ethnicity, insurance type, and the presence of chronic conditions. These findings are consistent with earlier studies documenting increased healthcare utilization among individuals with long COVID,14,32 -34 showing that individuals with long COVID are more likely to seek medical care frequently and use specialized services, including rehabilitation and mental health care, which are often associated with higher costs. This also includes more outpatient visits and higher medication use, compared to those without long COVID. However, while these studies primarily emphasized service utilization, our analysis provides a granular breakdown of direct costs, expanding the evidence base on the economic burden of long COVID at the national level. Although the GLM results indicated statistically significantly higher total, office-based, and outpatient expenditures among individuals with long COVID, the 2-part model sensitivity analyses did not show statistically significant differences for these categories. This divergence is expected given the different modeling frameworks. The GLM with a log link and gamma distribution models all observations in a single step, incorporating both zero and positive expenditures, whereas the 2-part model separates the probability of any spending from the amount spent among those with positive expenditures. When the probability of incurring any expenditure is similar across groups but the distribution of positive costs is highly variable, the second stage of the 2-part model often produces wider confidence intervals, attenuating statistical significance despite similar point estimates. 35 Given these discrepancies between the 2 statistical approaches, the findings should be interpreted with caution. Future research could employ more advanced modeling techniques, such as the 3-part model proposed by Karlsson et al., which are explicitly designed to address the heavy right-tail problem. 36
In our adjusted models, individuals with chronic illnesses such as diabetes, arthritis, and heart disease also exhibited significantly higher healthcare expenditures, consistent with prior evidence.37 -39 While it is plausible that individuals with both long COVID and chronic conditions experience compounded cost burdens, our analysis did not include formal interaction terms to test for these effects. Therefore, our findings reflect the independent associations of long COVID and each comorbidity with healthcare spending, rather than any combined or interactive effects. Future studies should explore these potential interactions to better understand whether the coexistence of long COVID and specific chronic conditions leads to amplified financial burdens.
We also found no significant differences in healthcare expenditures for emergency room visits, hospital admissions, or dental care between individuals with and without long COVID. This suggests that the cost burden of long COVID may be driven more by ongoing outpatient management than by acute care episodes. Persistent symptoms such as fatigue, brain fog, or pain may prompt repeated office-based consultations rather than hospitalization. This pattern may reflect efforts to manage long COVID in lower-intensity care settings, potentially reducing reliance on emergency or inpatient services.
One unexpected finding was the 60% lower home health spending among individuals with long COVID. This likely reflects the younger age profile of our long COVID group, 81.6% being under 65 years in comparison to 77.4% for individuals without long COVID. Because home health services are typically used by older adults or individuals with advanced disability, lower spending in the long COVID group may reflect both age and functional status. It may also indicate a stronger preference for outpatient or self-directed care, aligning with utilization patterns observed in younger populations with chronic illness. 40
While this study did not focus on disparities in healthcare spending by race/ethnicity or socioeconomic status, future research should examine whether certain populations are disproportionately affected by the costs associated with long COVID. Studies have demonstrated that marginalized groups, such as racial/ethnic minorities and individuals from lower socioeconomic backgrounds, often face greater challenges in accessing healthcare, which could exacerbate the financial impact of long COVID. 41 Understanding these disparities could inform the development of equitable policies that address the needs of the most vulnerable populations and ensure that all individuals with long COVID receive appropriate care.
Several limitations should be considered when interpreting these findings. First, classification of long COVID was based on self-reported responses to the MEPS question: “Has the person had symptoms lasting 3 months or longer that they did not have prior to having COVID-19?” While this definition captures persistent symptom burden, it is subject to recall bias, misinterpretation, and stigma-related underreporting. Importantly, the survey item does not define specific symptoms, nor does it require a medical diagnosis, which introduces the risk of misclassification. Some individuals may attribute unrelated symptoms to long COVID, while others may fail to report symptoms that qualify. Second, the lack of a universally accepted clinical definition for long COVID complicates comparisons across studies. The RECOVER initiative and related efforts have emphasized the heterogeneity in symptom presentation, timing, and severity, 42 and recent review have raised concerns about methodological inconsistencies in long COVID research, including selection bias and the challenges of separating causal effects from comorbid conditions. 43 Third, our estimates are based on U.S. survey data and may not generalize to countries with different healthcare systems, reimbursement models, or access dynamics. Additionally, the findings are specific to adults and may not reflect patterns in pediatric or adolescent populations. Fourth, MEPS includes only the noninstitutionalized civilian population, excluding individuals in nursing homes, correctional facilities, or other long-term care settings. As such, healthcare expenditures among institutionalized adults who may have different risk profiles or care needs are not captured. Although we controlled for a wide array of sociodemographic and clinical variables, residual confounding cannot be ruled out. In particular, MEPS does not capture symptom severity, duration of long COVID, or COVID-19 vaccination status, which could influence healthcare utilization. Although we adjusted for age category in the analysis, the no long COVID group included ~16 times more respondents aged 65 and older than the group reporting long COVID, and age distributions were statistically different between the 2 groups. These differences may contribute to residual confounding and could limit the precision of estimates for the long COVID group. Lastly, this is a cross-sectional study. While it documents associations between long COVID and healthcare spending, it cannot establish temporal or causal relationships. Longitudinal studies are needed to better understand the progression of costs over time and the long-term economic consequences of long COVID.
Despite these limitations, this study has notable strengths. It leverages the nationally representative 2022 MEPS dataset and includes detailed expenditure data across a range of healthcare services. By providing one of the first comprehensive comparisons of healthcare spending between individuals with and without long COVID, our study contributes critical evidence to a growing policy conversation. The findings underscore the substantial financial burden associated with long COVID and support the need for targeted care models and policy interventions. As healthcare systems evolve to manage post-COVID conditions, a dual focus on cost-efficiency and equitable access will be essential to ensure patients receive the care they need without undue financial hardship.
Conclusion
This study demonstrates that long COVID is associated with significantly higher healthcare spending, driven primarily by outpatient and office-based care. As the healthcare system continues to adapt to the ongoing impacts of the COVID pandemic, it is crucial to allocate resources efficiently and develop care models that meet the unmet needs of individuals with long COVID, while containing healthcare costs. It is also important to understand where subjects with long COVID visited the most to provide targeted interventions. This information is critical to provide targeted treatment for subjects with long COVID.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251410890 – Supplemental material for Comparison of Healthcare Expenditures Among Individuals With and Without Long COVID in the United States
Supplemental material, sj-docx-1-inq-10.1177_00469580251410890 for Comparison of Healthcare Expenditures Among Individuals With and Without Long COVID in the United States by Emeka Elvis Duru, Godwin Okoye, Sanghoon Lee, Peter Weir and Jaewhan Kim in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Appendix
Marginal Effects in Dollars From 2-Part Models.

| Spending category | Long COVID | Margin ($) | 95% CI | P value | |
|---|---|---|---|---|---|
| Total healthcare expenditure | .13 | ||||
| No | 9031 | 8468 | 9593 | ||
| Yes | 10 382 | 8659 | 12 104 | ||
| Total office-based expenditure | .60 | ||||
| No | 2336 | 2170 | 2502 | ||
| Yes | 2480 | 1956 | 3004 | ||
| Total outpatient-based expenditure | .11 | ||||
| No | 1073 | 978 | 1168 | ||
| Yes | 1378 | 1015 | 1741 | ||
| Total ER expenditure | .48 | ||||
| No | 266 | 242 | 291 | ||
| Yes | 295 | 219 | 371 | ||
| Total hospital admission expenditure | .99 | ||||
| No | 1443 | 1312 | 1574 | ||
| Yes | 1441 | 1049 | 1833 | ||
| Total dental care expenditure | .98 | ||||
| No | 424 | 404 | 444 | ||
| Yes | 425 | 353 | 497 | ||
| Total prescription expenditure | .13 | ||||
| No | 2500 | 2146 | 2854 | ||
| Yes | 3363 | 2235 | 4492 | ||
| Total home healthcare expenditure | <.01 | ||||
| No | 498 | 423 | 572 | ||
| Yes | 297 | 169 | 425 | ||
Note. Other controlled variables are not shown.
Ethical Considerations
As we utilized a publicly available dataset, IRB approval for the study was not required.
Consent to Participate
As we utilized a publicly available dataset, informed consent for the study was not required.
Author Contributions
J.K. conceptualized the study, led the data analysis, provided methodological and statistical oversight, drafted the manuscript, and critically reviewed all sections of the manuscript. E.E.D. and G.O. prepared the initial manuscript draft and critically reviewed the manuscript. S.L. and P.W. validated the analytic approach and provided critical revisions throughout the manuscript. P.W. also offered clinical insight into long COVID outcomes and contributed to the interpretation of the findings.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.