
Abstract
The long COVID affects individuals that do not recover for several weeks or months following the onset of symptoms of COVID-19. Obesity could play a role in the long COVID syndrome. During the pandemic, various factors contributed greatly to aggravating obesity in women leading to a pro-inflammatory and prothrombotic status. The present commentary explores the relationship between long COVID and obesity in women.
Keywords
In the last years, the COVID pandemic has had important effects on human health and has conditioned our lifestyle by inducing major changes in diet, physical activity, sedentary habits, time spent at home, and the quality of sleep.1,2 All these factors, together with the reduction of preventive visits due to the crisis in the health system, have facilitated the development of pathologies and conditions predisposing the development of chronic non-communicable diseases. 3 Obesity is an important risk factor for the development of non-communicable diseases and has been favored by lifestyle changes that occurred during the pandemic. Several evidences have also pointed out that obesity is a frequent comorbidity in those affected by the infection in the most severe forms.4,5
Long COVID
In the current era, a new phenomenon is emerging: the “long COVID.”
The “long COVID” identifies the situation of affected people who do not recover for several weeks or even months after the onset of symptoms indicative of COVID-19.5-7 The name “long COVID” was created in the spring of 2020 to describe the non-recovery situation. 8 In long COVID, persistent symptoms are fatigue, shortness of breath, cough, and mental health problems. 9
Very recently, a consensus paper has been published about post-acute sequelae of SARS-CoV-2 Infection (PASC). 10
PASC includes a constellation of symptoms that emerge or persist weeks to months after recovery from COVID-19. The PASC usually lasts for 4–12 weeks.10,11
However, long COVID is not limited to patients with early severe disease. In many subjects affected by “mild” COVID-19, symptoms include persistent fatigue and dyspnea, palpitations, and headache. A large percentage of subjects also develop cognitive problems, including poor memory and concentration.
There is increasing evidence of long-term health damage across all different clinical presentations of COVID-19 infection.10-12
SARS-CoV-2 infection has been classified according to symptoms and clinical manifestations in several forms
13
: 1. Asymptomatic (or presymptomatic): Individual who tests positive for SARS-CoV-2 infection but has no symptoms consistent with COVID-19. 2. Mild illness: Individual who has symptoms or signs of COVID-19 (eg, fever, cough, sore throat, and malaise), without dyspnea or abnormal chest imaging. 3. Moderate illness: Individual who has lower respiratory disease (eg, pneumonia) with oxygen saturation $94% on room air at sea level. 4. Severe illness: Individual who has lower respiratory disease with oxygen saturation <94% on room air at sea level, ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) <300 mm Hg, a respiratory rate >30 breaths per minute, or infiltrates involving >50% of the lung fields on chest imaging. 5. Critical illness: Individual who has lower respiratory disease with respiratory failure, septic shock, and/or multiple organ dysfunction.
While many people with mild–moderate disease recover within 2 weeks, there is a percentage of the population which do not return to baseline even after 14–21 days. 14
Interestingly, in subjects with mild acute COVID-19, the burden of persistent symptoms seems to be associated with poorer long-term health status, poorer quality of life, and psychological distress. 15
The long COVID seems to be more prevalent among women, subjects with obesity and older people. 15
Obesity and Women
During the pandemic, women developed a significant risk of deteriorating health and an increased self-perception of symptoms of depression. 16 Women appear to have both a higher prevalence of risk factors known to worsen during a pandemic, including pre-existing depressive and anxiety disorders, and have been subjected to increased stress and risk of domestic violence. 17
Moreover, low socioeconomic status and sociocultural roles affect women disproportionately to men and are emerging as important in the development and manifestation of cardiovascular disease in women.17,18
Furthermore, women have a greater risk of developing obesity after menopause due to the hormonal changes that occur at this stage of life. Although men and women are largely exposed to the same environment, the way they interact with this environment varies according to sex (and other social factors such as age, diet, and socioeconomic status).19,20
The Framingham Heart Study showed that the excess risk of cardiovascular disease attributed to obesity was 64% in women vs 46% in men. 21
It is well known that biology as well as lifestyle and socioeconomic factors contribute to the differences in obesity prevalence between the sexes. 22 The physiology of subcutaneous and visceral adipose in women is different compared to men, with over 2800 genes differentially expressed. 23 Men have larger fat cell sizes in the intra-abdominal compartment, whereas women have larger fat cell sizes in subcutaneous depots. 24 These sex differences in adiposity distribution influence the flux of fatty acids that occurs in fasting and feeding. In the presence of obesity, both men and women have increased the release of fatty acids into the blood. Adiposity in the visceral compartment has a greater contribution to the delivery of fatty acids to the liver than adiposity from subcutaneous fat. 21 After menopause, fat distribution changes with a prevalence of visceral adiposity leading to similar cardiovascular risk in women and men. 24
Long COVID: Inflammatory and Prothrombotic Status
A possible link between obesity and long COVID disease in women is inflammation. COVID-19 is associated with a high level of inflammation and obesity is also a condition associated with systemic inflammation. This link predisposes obese individuals to develop a worse prognosis during the acute phase of COVID-19 disease. 25
Adipose tissue is an endocrine organ that has several functions. In an inflammatory state, it releases hormones and inflammatory proteins, that is, cytokines and adipokines. 26
Leptin and adiponectin are major adipokines of adipose tissue with pro-inflammatory and anti-inflammatory properties, respectively. In obese individuals, leptin levels are higher, and adiponectin levels are lower than in normal-weight subjects. 27
Factors Linking Obesity and COVID-19.
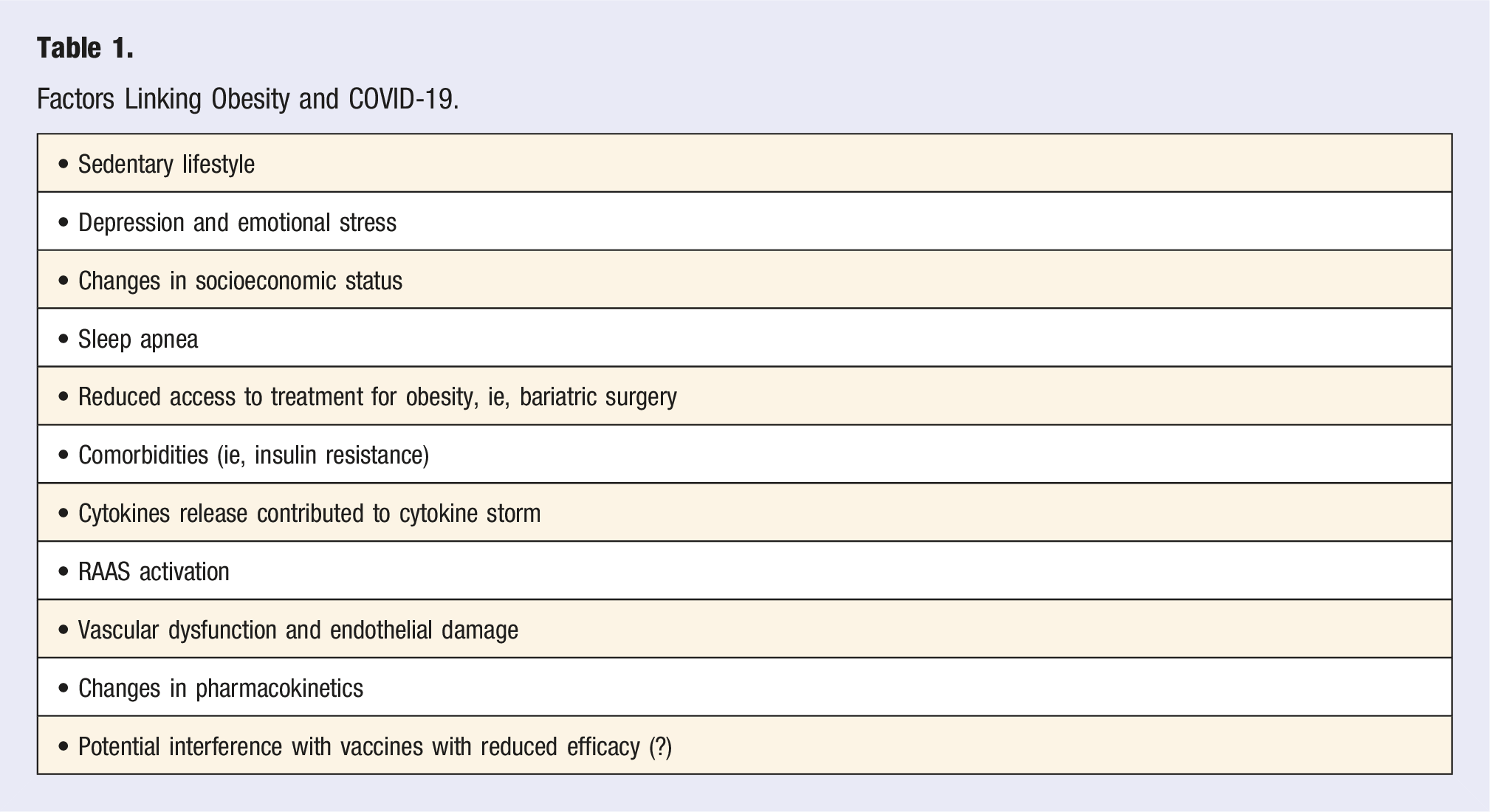
In the hypothesis that long COVID is associated with a persistent inflammatory state, it is well understood that obese subjects are at greater risk of developing long COVID symptoms. Furthermore, the same symptoms of long COVID, dyspnea, asthenia, and difficulty in doing activities involving muscular effort are aggravated by obesity.
During the pandemic, various factors contributed greatly to aggravating obesity in women and several of these environmental factors persist, aggravating the risk of obesity even in long COVID. Figure 1 shows some of the factors that contribute to aggravate the long COVID status in obese women: i.e. endothelial dysfunction, inflammation, socioeconomic distress, poor prevention of disease.17,28 Factors favoring long COVID in obese women: sex related biological and environmental features.
Moreover, it is well known that SARS-CoV-2 infection has been associated with a prothrombotic status, and recent reports suggest that prothrombotic condition persist during long COVID syndrome.29,30
COVID-19 was commonly associated with increased coagulopathy, disseminated intravascular coagulation (DIC), and acute inflammation, which resulted in higher morbidity and mortality. 29 The prothrombotic state seems to be the main contributing cause of adverse prognosis of severe COVID-19. In patients affected by COVID-19, hypercoagulable states and thromboembolic events in major blood vessels have been described. These lead to limb ischemia, associated with neurological symptoms, and complications, including stroke, macro-and micro-thromboembolic infarction.29,30
In patients developing long COVID-19, a prolonged elevation of D-dimer regardless of the inflammatory indices and the severity of the acute phase have been detected. This is a maker of an increased risk of thromboembolic complications. 31
Visceral obesity is associated to insulin resistance, systemic oxidative stress process, and inflammatory status. These changes determine the loss of the antithrombotic properties of the endothelium, platelets, and other circulating cells. In obese subjects, an increased production of microprocoagulant (MP) particles, IL-1β, plasminogen activator inhibitor-1 (PAI-1), and tissue factor (TF), which activates the factor 7 receptor, has been reported. 32
An interesting feature is the cross-talk between coagulation and inflammation which is facilitated by protease-activated receptors (PARs). COVID-19 targets these receptors, which are effectively able to activate local and circulating coagulation factors, thus inducing the generation of disseminated coagulopathies. 29 Acanfora and coworkers 29 analyzed these mechanisms to support the usefulness of anticoagulant therapy during the acute phase of the disease and also suggested caution and attention to the state of coagulation in the management of patients with long COVID.
Conclusions
Fighting obesity is a major challenge for women to maintain good health. The recent pandemic has compromised some aspects of a healthy lifestyle such as a healthy diet and regular physical activity and has increased sedentary lifestyle and stress.2,33
The various benefits of reducing overweight and obesity in women can also include reducing the risk of developing post-COVID symptoms. The visceral fat that accumulates in women especially in menopause is an active hormonal organ that produces adipokines that have a pro-inflammatory role.4,5 Furthermore, weight gain reduces physical activity by creating a vicious circle that leads to self-maintenance of being overweight.2,28 Several evidences have pointed out that obesity is a risk factor in contracting infections including that from SARS-CoV-2. The fight against obesity has several advantages and among these today we can also insert the reduction of the risk of developing symptoms of long COVID.
How to intervene? enhancing prevention and awareness campaigns especially involving women and young people. In addition, it is mandatory to develop supportive programs after COVID infection in obese women to prevent long COVID. It is also necessary to change the perception of cardiovascular risk mediated by obesity in postmenopausal women. 34
As suggested by The Lancet women and cardiovascular disease Commission “Prevention and management of cardiovascular disease in women require robust health-care systems supported by professionals who are aware of, and care about, the specificities of cardiovascular disease in women. It is imperative to create integrated health systems and to engage physicians.” 17
This action is essential to prevent both acute effects of infection and sequelae.
Footnotes
Acknowledgments
We thank Dr Melania Malpezzi for the production of Figure 1.
Author Contributions
AVM and SG conceived of the idea at the basis of the article, AVM, FC, MN, and SG developed the different part of the manuscript and performed the final supervision. All authors contributed to and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.