
Abstract
During postgraduate medical education (PGME), individuals face both internal and external professional difficulties. This study examines the difficulties faced by medical residents, their consequences, and their coping strategies from the perspective of medical teachers. This phenomenological study, conducted during the 2024 to 2025 academic year, included 10 medical teachers (3 from Basic Sciences, 3 from Surgical Sciences, and 4 from Internal Sciences) from 3 medical faculties. Purposeful sampling with maximum variation was used to ensure diversity. Data were collected through semi-structured interviews were analyzed thematically. From the perspective of medical teachers, the difficulties encountered by residents during PGME were grouped into 7 themes: “curriculum,” “medical teachers,” “learners,” “health system,” “culture/climate,” “specialization area,” and “time/period.” Intergenerational differences influenced perceptions of education and coping strategies, adding another dimension to the conceptualization of challenges. The consequences of these difficulties were identified as feelings of inadequacy and deterioration in well-being. Coping strategies primarily included individual efforts and external support. The study highlights that residents’ difficulties arise from the complex interaction of educational, cultural, and systemic factors that shape PGME environments. While teachers often recognize these difficulties, they tend to frame them through personal or generational comparisons, reflecting limited pedagogical reflection. Sustainable improvement requires shifting from an individual resilience model to a relational and system-oriented approach that emphasizes empathy, reflective supervision, and psychological safety. Faculty development programs focused on mentoring, feedback literacy, and cultural awareness, together with institutional policies that balance service and education, are essential to foster humane, learning-centered environments. Such integrative strategies can enhance residents’ well-being, strengthen teacher–learner relationships, and contribute to the long-term sustainability of PGME.
What do we already know about this topic?
● Individuals in PGME face internal existential and external professional challenges. Previous research has explored difficulties faced by residents, with a 2024 study grouping these into themes like postgraduate medical education, culture/climate, health system, specialty, and time/period. Literature also mentions challenges such as service over education, residents’ lack of leadership or management skills, and issues with completing work on time. Mentoring and coaching are expected roles for teachers but are often unfulfilled. Additionally, there’s existing knowledge about the global prevalence of burnout among postgraduate medical trainees.
● This study contributes to the growing body of research on PGME by expanding the understanding of residents’ difficulties through the perspectives of medical teachers together with their assistants within the same institutional and cultural context. While most existing studies have described residents’ challenges based solely on learners’ self-reports, this research introduces a dual-lens framework that integrates medical teachers’ interpretations of residents’ struggles. In doing so, it offers a more comprehensive conceptualization of the phenomenon of “resident difficulties,” incorporating not only structural and systemic factors but also relational, cultural, and generational dimensions. The identification of “learner characteristics” as a new thematic domain—encompassing learning approaches, perceptions of difficulty, and coping mechanisms—provides an important conceptual expansion for future PGME research. Moreover, by highlighting the interaction between institutional culture, workload norms, and educational values, this study bridges individual experiences with broader organizational structures. It thereby contributes to the theoretical discourse on professional identity formation, workplace learning, and the socio-cultural dynamics of medical education.
● This study elucidates the complex nature of PGME by examining residents’ experienced difficulties and reinterpreting learning environments within a socio-cultural framework. The findings indicate that learning challenges stem not merely from individual deficiencies but from the dynamic interplay of personal, institutional, and systemic factors, underscoring the need to approach professional development and resilience through relational and contextual models. Within this framework, faculty development programs that strengthen empathy, reflective dialog, and learner-centered supervision—as well as structured mentorship, protected learning time, and consistent feedback mechanisms—are essential for maintaining a balance between education and service. Recognizing “learner characteristics” as a legitimate dimension of educational difficulty may enable faculty members to design adaptive learning environments that respond more effectively to diverse learner needs. At the institutional and national levels, policies that safeguard resident well-being, ensure equitable workload distribution, and integrate psychosocial safety into accreditation and quality systems are vital for cultivating a medical education culture centered on human sustainability. Future research should explore the interrelationships between cultural toxicity, psychological safety, and professional identity development using measurable indicators such as organizational climate scales, learning environment assessments, and well-being measures. Moreover, intervention-based studies examining the impact of structured orientation programs and Residents-as-Teachers initiatives on learner autonomy, feedback culture, and institutional belonging would offer valuable insights at both local and international levels. Ultimately, the sustainable improvement of PGME depends not only on individual resilience but also on institutional learning, cultural transformation, and the continuous reconstruction of educator–learner relationships.
Introduction
The concept of difficulty is defined in the Oxford English Dictionary
1
as: (i) how hard something is, (ii) the state or quality of being hard to do or to understand, and (iii) a problem or a situation that causes trouble. The term “difficult” is often framed as something complex and time-consuming.
2
Warren Weaver defines complexity as the difficulty of predicting the behavior of an activity or system due to the number of elements it contains and the interactions among them. He argues that an activity or system becomes more complex as the number of its parameters increases. For instance, solving a mathematical problem involves many interacting variables—prior knowledge, motor habits, emotional state, and environmental conditions—illustrating that difficulty depends on one’s knowledge, skills, perceptions, and experiences. Philosophically, difficulties can be classified as
The residency period corresponds to Levinson’s early adulthood stage of life, a phase during which all these types of difficulties can emerge or coexist. 3 Thus, challenges faced by residents are more complex and multifaceted than those encountered during undergraduate or continuing professional development stages. Residents, unlike their teachers, must simultaneously cope with professional demands and the internal developmental constraints of early adulthood, particularly existential concerns. Yet, if both teachers and residents experience similar systemic challenges, this shared ground may provide important insights into where interventions should begin.
Postgraduate medical education (PGME) represents a phase in which physicians shape their professional identity amid intense clinical responsibilities and intertwined service and learning demands. The literature consistently shows that difficulties during this period are multidimensional—arising from structural deficiencies in educational programs, imbalanced service-to-learning priorities, insufficient mentorship, heavy workloads, and hierarchical barriers to communication.4 -8 These factors negatively affect residents’ motivation, learning capacity, and well-being.9 -11
However, most existing studies define these difficulties
This study aims to explore and explain the difficulties faced by residents from the perspective of medical teachers within the context of postgraduate medical education. Specifically, it addresses the following questions:
According to medical teachers, what types of difficulties do residents experience in PGME?
What are the perceived consequences of these difficulties?
How do residents cope with such difficulties, and how do teachers observe and interpret these processes?
The study seeks to contribute to the understanding of the complexity of residency training and to inform context-sensitive approaches for faculty development, learner support, and learning environment enhancement in medical education.
Method
We reached out to volunteer medical teachers from basic, internal, and surgical sciences departments for the sample selection. Lincoln and Guba recommend sampling in qualitative studies until a point of saturation or redundancy is reached. 16 In our study, interviews were continued when no new information was received from the participants, when the same answers started to be given, or until there was no difference in opinions. 16 We achieved data saturation through the testimony of 10 medical teachers. Three from Basic Sciences (Anatomy, Biochemistry, Microbiology), 3 from Surgical Sciences (Obstetrics and Gynecology, General Surgery, Anesthesiology and Reanimation), and 4 from Internal Sciences (Neurology, Emergency Medicine, Pediatrics, Internal Medicine). Five participants were female and 5 were male. They have teaching experience ranging from 6 to 25 years.
The development of the semi-structured interview form was guided by a theoretical framework grounded in the conceptualization of “difficulty” and “complexity” and the philosophical classification of difficulties into epistemic, practical, existential, moral, and sociocultural domains. 2 This framework also incorporated existing literature4 -12 on difficulties in PGME, including issues related to educational climate, workload, system factors, and learner characteristics. Accordingly, the questions were structured to explore these dimensions in depth.
The questions were open-ended and designed to provide illustrative data. At the beginning of the interview, we requested descriptive information, followed by questions about the difficulties experienced and coping strategies. The semi-structured questionnaire included observation, experience, behavior; opinion and values; feeling and background/demographic questions.
Four experts from the fields of internal medicine, surgery, basic sciences and medical education were consulted about the content of the questionnaire. A pilot interview was conducted with 1 medical teacher who did not participate in the main study. Feedback from the pilot interview indicated that some questions were overly broad or ambiguous. Based on this feedback, we (i) simplified complex wording, (ii) added clarifying probes to encourage richer responses, and (iii) removed 1 redundant question that overlapped conceptually with others. The final version of the interview form was thus refined to ensure clarity, relevance, and alignment with the theoretical framework. The pilot interview also helped the researchers to estimate the average duration of interviews, assess the flow of questions, and make adjustments to ensure logical sequencing from descriptive to more in-depth probing questions.
Data were collected through semi-structured individual interviews conducted synchronously via Zoom. The interview guide, developed based on the literature and expert opinion, included open-ended questions about perceived resident difficulties and coping strategies. A pilot interview was conducted to refine the questions. All interviews were audio-recorded with verbal consent and transcribed verbatim by an independent transcriber under a confidentiality agreement.
Thematic analysis was applied in the study by following the steps below 16 : (1) The first step of qualitative data analysis is to explore the data. To get a general idea about the data and understand it as a whole, the researchers read the transcripts independently. (2) The second stage is the coding process. This process involves the identification of text segments, assigning a code word or phrase that accurately describes the meaning of the text segment. At this stage, the researchers identified quotes that fit the codes. The identified quotations were transferred to the excel database. (3) Three researchers came and worked on the database together. The coding process was carried out with individual opinions and explanations about the quotations. The consensus decision for each quote was determined in the same process. (4) The process was completed by reviewing the codes, sub-themes and themes. (5) Theme definitions were made and quotes were selected to represent the themes. The participant protocol number and department were included in the presentation of the quotes. (6) The findings were interpreted by comparing them with the relevant literature.
Data were analyzed manually using thematic analysis. Coding was conducted independently by 3 researchers. Consensus was reached through iterative discussion. No qualitative data analysis software was used. Representative quotations illustrating each theme were selected to ensure transparency and provide direct evidence from participants’ narratives. These quotations were anonymized and coded according to department and participant number. Rigor was ensured through member checking, peer debriefing, and triangulation across specialties. Reflexivity was maintained throughout the research process to mitigate researcher bias.
Results
It has been observed that teachers often compare the difficulties faced by residents with those they experienced during their own residency period and, in some cases, illustrate these difficulties with personal examples.
“During my residency, the mobbing I experienced was even more severe. Despite being a resident at this hospital and this university, I was unable to complete my thesis here. I had to collect my cases by leveraging personal relationships and friendships at hospitals that were formerly under SSK. This situation forced me to work outside the institution.” (P9, M, Anatomy)
Two teachers openly acknowledged their lack of complete knowledge regarding the difficulties faced by residents and their coping mechanisms.
“Some of them have hobbies. For instance, some ride bicycles. A few fall into depression; I know of some who go to psychologists. Frankly, I don’t know much about their personal lives or how they deal with certain difficulties. Usually, the ones who feel overwhelmed eventually come to talk to me.” (P2, M, General Surgery)
The findings are presented in line with the research questions.
1.
From the medical teachers’ perspective, difficulties of the medical residents’ face during PGME were grouped in 7 themes: “curriculum,” “medical teachers,” “learners,” “health system,” “culture/climate,” “specialty,” “time/period” (Table 1).
Difficulties Faced by Residents in PGME From the Medical Teacher’s Perspective.

“
“At the end of four years, making a competency decision based on a half-hour or one-hour exam is not appropriate. . . If we deem this individual incompetent, why did we entrust them with patients over the past four years?. . . Exam performance should not be the sole focus; it should include all aspects of performance, including social skills. . . Such a system exists on paper, but it is not implemented in practice.” (P3, M, Internal Medicine)
“
“It’s a very heterogeneous structure. We have 10 faculty members. . . For instance, there are faculty members whom residents haven’t seen in over a year. Let alone giving feedback to residents, some of them do not participate in any educational activities or ward rounds. So, it’s very heterogeneous.” (P3, M, Neurology)
“
“. . . In an increasingly mechanized world, they are becoming more and more socially isolated. Are the friendships among them as strong as ours, as strong as they were in our time? I don’t know. But this is a general global issue, not something specific to our program. People are gradually becoming less social.” (P2, M, General Surgery) “. . . Honestly, I’m not just saying this because they’re young, but they have an incredible sense of foresight and intuition. . . I was more blind and emotional. . . But they are much more rational and perceptive. They know very well what they can take from where and how far they can go. . . In that sense, I admire them greatly. . . We have a great mutual exchange.” (P11, FM, Anesthesiology)
“
"Currently, for instance, residents are on call every three days, and unfortunately, even when they are on duty in the emergency department (pediatric emergency included), they continue working the following day at their assigned posts until 5:00 PM. This has been the case for all of us since the past, but I would prefer for this to change. In fact, we have tried to make adjustments within our department, at least in the emergency rotation. Unfortunately, due to sudden and acute changes, we were unable to implement it." (P7, FM, Pediatrics) "Having a call every three days and then working until the evening post-call can indeed be a bit problematic. . . Personally, I did not experience any negative impact during my residency. Every moment I spent in the hospital made a significant contribution to my education. . . I never considered it a burden; instead, I thought of it as oriented toward education and patient care." (P3, M, Internal Medicine)
Teachers’ perceptions of these difficulties vary. For instance, some medical teachers consider intense call schedules and heavy workloads as inherent to the nature of specialty education.
“
Teachers view the hierarchical structure based on professional knowledge and experience (junior, senior, chief resident, specialist, faculty) as important for learning from those above. Hierarchy is also seen as significant in terms of ensuring patient safety and respecting knowledge and experience. One teacher stated that while hierarchy is important, it should not prevent questioning by those in lower positions. Another teacher mentioned that the high expectations from residents regarding academic work can source difficulty and stress, especially in the initial phases of training.
Interaction difficulties within the organizational climate may manifest as issues related to accessibility and communication with teachers or problems concerning team communication.
‘Here, the technician knows much more than the resident when the resident first arrives. Due to this knowledge disparity, difficulties have arisen in establishing hierarchy between technicians and residents. I clearly remember having to warn a few residents in the room because the noise levels could rise. It should be communicated to them that technicians know very little, but what they do know, they know well because they have been doing this for years. Of course, our knowledge cannot be compared to that of our colleagues; however, establishing a hierarchy or a superior-subordinate structure can complicate matters. We need to recognize that we are a team, and the better we understand each other as a team, the higher the quality of our work will be. (P4, FM, Microbiology) "Unfortunately, there have been behavioral patterns among some faculty members that undermine others through their residents. . . The thought process has been: ‘I don’t like you, so I don’t like your residents either. I will mistreat them, doing to them what I cannot do to you.’" (P9, M, Anatomy) "The senior resident will follow the directives of the chief resident, and the junior assistant will follow the senior. . . However, this hierarchy should not be unquestionable. They should be asking, ‘Why are we doing it this way?’. . . Ultimately, my knowledge and experience should exceed that of the chief resident. . . Therefore, a form of hierarchy is necessary in education. Consulting is the essence of the work." (P2, M, General Surgery)
“
"In the internal medicine training process, being a resident is very difficult. . . Residents are drowning in too much theoretical workload. . . When I was a resident, I realized this clearly — when we asked something about other departments, they could answer easily, but we couldn’t do the same for internal diseases. The area was too big to dominate. . . I tell my residents the same: you may feel inadequate — it is natural." (P3, M, Internal Medicine) "The enjoyable parts of what we do. . . are very satisfying — the patient can come back from the dead in an instant. There is never uniformity in anesthesia. . . everything can suddenly capsize, and a very exciting environment can occur. One of our professors used to describe anesthesia as ‘like riding a sailboat’ — when the weather is calm, it’s pleasant, but you never know when the wind will blow. You need to be alert at all times." (P11, FM, Anesthesia)
“
'. . .. On the one hand, you have to do a professional job, and on the other hand, you are in the status of a student as if you are not. Since the concept complexity of these two concepts is experienced and experienced both at the level of education and on the basis of teachers, especially the first periods of residency can become a torment. Of course, when you ask different professors about this, they respond that it is part of the training, but I don’t think so. (P9, M, Anatomy)
2.
Themes and sub-themes about the consequences of the difficulties of the medical residents’ face during PGME are presented in Figure 1

Consequences of the difficulties of the medical residents’ face during PGME from the teachers’ perspective.
“
“
“. . . The factors that lead to burnout are mostly the intense working environment. . . . a young patient can be lost with an unexpected complication. We are seriously exhausted . . . It takes a very long time to recover. . . . we question among ourselves . . . did we miss something? what went wrong? . . . we do everything much more meticulously with anxiety . . . we repeat the control steps over and over again. This leads to both burnout and obsessive-compulsive behavior. We check things over and over again. . . . You can never be completely comfortable. And this . . . brings obsessions and burnout after a while. It makes you tired.” (P11, FM, Anesthesia)
3.
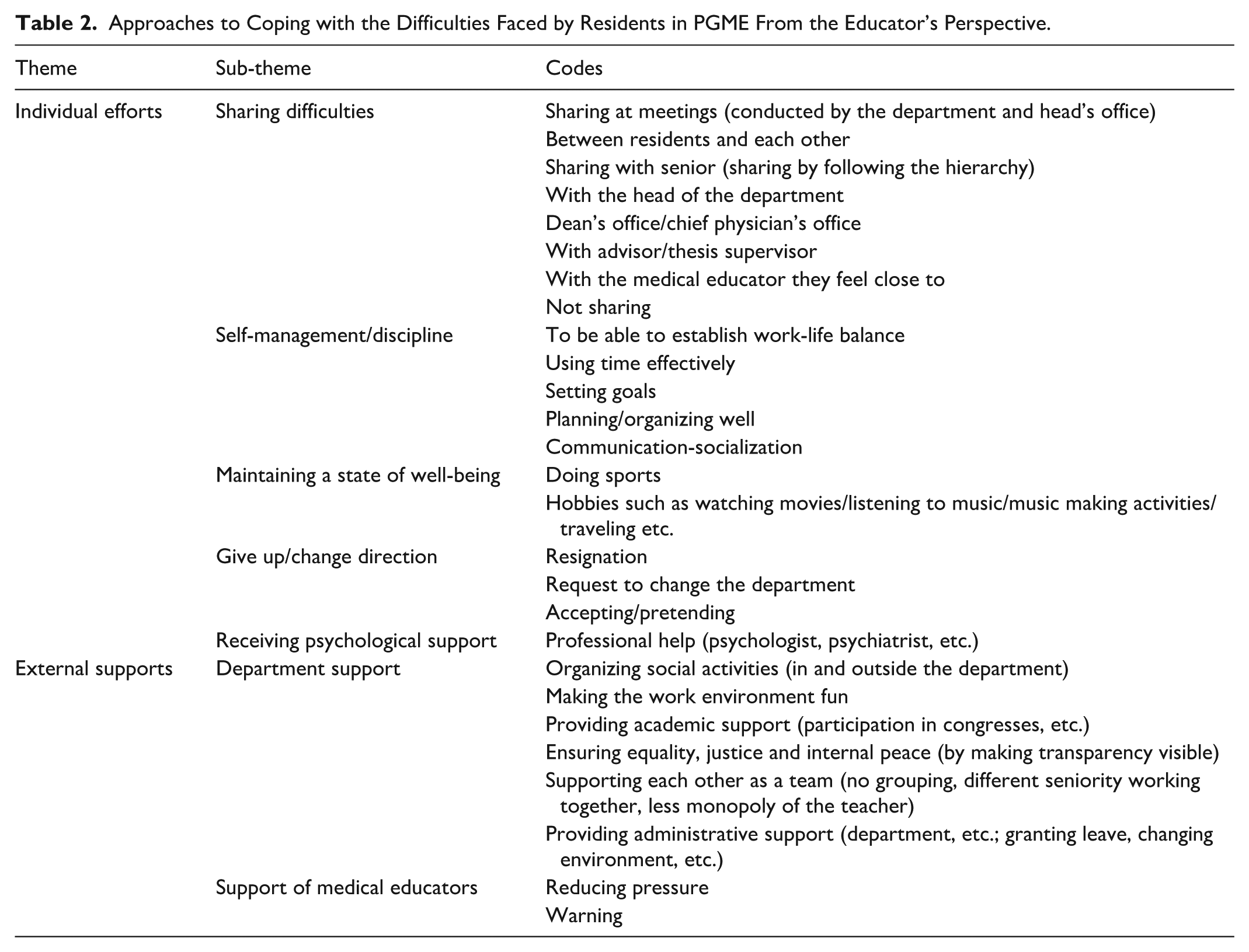
According to medical teachers, residents cope with difficulties through 2 main pathways: Individual efforts and External supports. The departmental climate and the perception of justice play a decisive role in this process.
Individual efforts
The themes in the dimension of individual efforts are: “Sharing difficulties,” “Self-management/discipline,” “Maintaining well-being” and “Giving up/changing direction.” Teachers observed that residents primarily rely on personal strategies to cope with stressors in PGME. One teacher stated that he did not have enough information about the residents’ individual efforts to cope (Table 2)
Approaches to Coping with the Difficulties Faced by Residents in PGME From the Educator’s Perspective.
“
“. . . But I have never come across an assistant who says that I am being mobbed here and goes out in public and expresses this. Personally, it happens in the form of closed rumors.” (P9, M, Anatomy)
“
“. . .. They probably have some motivation. At least they can survive with the ambition to reach a goal. There is also the fact that you endure certain difficulties as a resident. I think of myself as an assistant. The reason why you endure them is that you can choose the next period of your life.” (P11, FM, Anesthesia)
“
“Some of them try to protect their well-being by doing sports, spending time with friends or hobbies. I can say that those who manage to create such small spaces for themselves cope a little better. It doesn’t completely eliminate the stress, but it helps them to keep going.” (P7, FM, Internal Medicine)
“
“. . .This is the nature of gynecology. You know, those who can’t stand it quit. Well, those who do are counting the days, this will pass . . .” (P6, FM, Obstetrics and Gynecology)
External supports
Teachers also highlighted the role of structural and interpersonal support mechanisms that can ease the burden on residents. The themes in the context/dimension of
“
“. . .wherever there is equality and justice, there is more peace. . . this provides work peace and happiness at work in a positive sense.” (P11, FM, Anesthesia)
“
“They talk to me about everything — financial, emotional, or health-related problems, whether it’s about their children or their parents being ill” (P10, M, Neurology)
Discussion
Understanding the Complexity of Difficulties in Residency Training
This study extends our previous work 14 by exploring the difficulties faced by residents through the perspectives of medical teachers within the same institutional and cultural context. While the earlier study classified residents’ difficulties under 5 main themes—postgraduate medical education, culture/climate, health system, specialty, and time/period—this study identified 2 additional themes: curriculum and learners. The inclusion of these new dimensions broadens the conceptual framework for understanding PGME, integrating the dynamic interplay between teachers, curricula, and learners Importantly, many medical teachers contextualized residents’ challenges by reflecting on and comparing them with their own past experiences as residents, offering deeper insights into the ways these difficulties are conceptualized and interpreted within the profession.
Learner Characteristics as a New Dimension of Difficulty
The emergence of learner characteristics as a distinct theme aligns with global literature emphasizing learner diversity and self-regulation in PGME.4,5 Medical teachers often interpret residents’ difficulties—such as low stress tolerance or perceived lack of resilience—through the lens of generational differences. However, these differences are shaped not merely by age but also by sociocultural and institutional norms. Research on optimal learning environments6,17 underscores how organizational hierarchies, workload norms, and implicit expectations influence both teachers’ and learners’ professionalism, competence, and coping strategies. The intersection of professional culture, institutional climate, and intergenerational expectations offers a robust framework for understanding resident difficulties in the Turkish context.
While teachers viewed generational traits as a source of challenge, residents tended to attribute difficulties such as excessive workload or unclear protocols to cultural inertia and systemic resistance to change. This divergence reflects Bourdieu’s 18 concept of cultural reproduction, where entrenched hierarchies perpetuate existing norms and hinder transformation. The contrast between teachers’ normalization of hardship and residents’ expectation of reform signifies not only a generational gap but also a growing capacity for critical reflection and change among newer generations.
These findings invite a deeper question: are “learner characteristics” truly a difficulty for residents, or do they reflect medical teachers’ unmet pedagogical needs? Further research should examine whether these characteristics represent developmental constraints or relational challenges within the teacher—learner dynamic. 19 Faculty development programs must therefore move beyond didactic skill-building toward cultivating empathy, recognizing learner diversity, and supporting both professional and personal growth. 20
Programmatic and Medical Teacher-Related Challenges
Both this and our prior study 14 highlight persistent issues with unstructured programs, limited adherence to curricula, and insufficient assessment frameworks. The lack of structured evaluation tools, objectivity, and effective feedback mechanisms undermines competency-based education. Peer learning remains dominant, particularly in surgical fields; while valued by teachers, it often leaves residents isolated or dependent on variable peer mentorship quality.
Teacher-related difficulties—including low motivation, inadequate teaching skills, and poor role modeling—were consistently identified. Communication barriers and limited accessibility to teachers further exacerbate the issue. Feedback, when given, is often delayed, inconsistent, or emotionally charged. Although the literature widely recognizes mentoring and coaching as critical teacher roles,4,21 these remain underdeveloped in practice. Faculty development should thus prioritize feedback literacy, reflective teaching, and relational engagement.
Academic Climate and the Hidden Curriculum
Cultural tensions—manifested through stress, fear, perfectionism, and gender-based difficulties—persist within PGME and are often normalized as part of professional socialization. Teachers frequently frame such tensions as essential elements of professional maturation, whereas residents interpret them as reflections of systemic dysfunction. While hierarchical structures are valued for maintaining patient safety and professional respect, they can also suppress questioning, limit innovation, and inhibit open dialog. Residents in this study frequently described experiences of learned helplessness, diminished accountability, and organizational rigidity—phenomena seldom acknowledged by teachers. These discrepancies expose how hidden curricula perpetuate power asymmetries and silence dissent, mirroring global observations on
As highlighted in recent studies,
Cultural and Institutional Dynamics in PGME in the Context of Turkey
In this study, the phrase “in our time,” which frequently appeared in teachers’ narratives, reflects a culture of endurance, resonating with Bourdieu’s concept of cultural reproduction. 18 Systemic factors—such as performance-based payment models, excessive workloads, and limited institutional support—further normalize overwork and undermine the value placed on learner well-being. Within the Turkish context, PGME is shaped by a complex interplay of institutional, cultural, and systemic dynamics. Hierarchical structures are deeply embedded in Turkish medical education and are often justified as essential for ensuring patient safety and clinical efficiency. 25 However, these hierarchies may restrict psychological safety and open communication, negatively influencing interactions among residents, within teams, and between residents and faculty.
High patient volume, administrative burdens, and interdepartmental inefficiencies were frequently reported as key challenges. Nevertheless, teachers rarely referred to issues such as remuneration or inequities, reflecting their relative detachment from residents’ lived realities. Following the implementation of the “full-day law,” the shift toward performance-based and contractual systems has intensified service demands while marginalizing educational missions. In such environments, residents’ identities as learners are increasingly overshadowed by their service roles, leading to moral distress and burnout.25 -28
Understanding resident difficulties in the Turkish context therefore requires attention not only to systemic conditions but also to the cultural and institutional relationships that underpin them. The intertwined dynamics of hierarchy, communication patterns, and professional identity formation highlight the multidimensional nature of residency training—where learner well-being, institutional culture, and educational purpose continuously intersect and shape each other.
Coping and the Limits of Individual Resilience
Coping mechanisms identified in both studies 14 were predominantly individual—personal effort and limited external support—with minimal institutional backing. This reliance on individual resilience mirrors global trends that individualize well-being while neglecting systemic reform.9,10 Teachers’ limited awareness of residents’ struggles, often filtered through nostalgic comparisons to their own training, reveals an empathy gap. High resident-to-teacher ratios and overwhelming clinical workloads further reduce meaningful interaction, reinforcing “us versus them” divisions and dehumanizing tendencies within academic hierarchies.
Consequences and the Role of Empathy
Both residents and teachers recognized feelings of inadequacy/incompetence and deterioration in well-being as key outcomes of these difficulties. Teachers often rationalized these as temporary and developmental, inadvertently normalizing distress and labeling residents as “non-resilient.” Yet, instances where some teachers acknowledged learning from residents point toward emerging shifts in perspective. Bridging this empathy gap through reflective dialog, mutual understanding, and role modeling is essential for fostering humane and sustainable learning environments. 29
Recognizing the Learner and Implications for Reform
PGME is a form of training that centers on the development of specialist competencies within the context of healthcare delivery. It is well established that, beyond institutional factors, systemic issues pertaining to the broader health-care system also exert a significant influence on the nature and quality of specialty training. 30 Our findings suggest that residents should be regarded not as passive recipients of institutional or systemic pressures, but rather as active participants shaping the learning environment. In light of these results, several complementary directions are therefore proposed:
Embedding learner autonomy, reflection, mentoring, and shared well-being responsibilities into competency-based models.
Designing a reciprocal, adaptive learning model grounded in mutual respect, feedback culture, and empathy between teachers and learners.
Future research should operationalize these constructs using measurable indicators such as psychological safety, inclusivity, and institutional responsiveness.
Improving PGME requires recognizing residents as learners and developing professionals, ensuring that institutional structures align with these values to cultivate a more humane, reflective, and sustainable professional culture. To achieve lasting improvements in postgraduate medical education, we recommend the following:
Policy Recommendations
Practice Recommendations
Limitations
Because the findings of this study are based on the narratives of medical teachers working within a specific institutional and cultural context, their generalizability is limited. Variations across institutions and disciplines—particularly in terms of educational culture, administrative structure, and service workload—may yield different outcomes. Moreover, as this research reflects residents’ experiences indirectly through the perspectives of faculty members, future studies are recommended to employ multilayered qualitative designs that concurrently explore the viewpoints of both groups.
Conclusion
This study provides a multidimensional understanding of the difficulties in residency training by juxtaposing the perspectives of medical teachers and residents within a shared institutional and cultural context. By introducing curriculum and learner characteristics as new dimensions, it broadens the conceptual framework of PGME, revealing the intricate interactions among teachers, learners, institutions, and systemic forces. Findings underscore that many of the perceived individual deficits—such as low resilience or lack of adaptability—are in fact embedded within broader organizational, cultural, and systemic structures.
Addressing these intertwined challenges requires a paradigm shift from individual-based explanations toward a relational, culturally sensitive, and system-oriented approach. Strengthening empathy, feedback literacy, and reflective practice among educators, alongside structured orientation and Residents-as-Teachers programs, can bridge hierarchical divides and promote a more inclusive, supportive learning environment. Furthermore, confronting
Ultimately, recognizing residents not as passive recipients of training but as active agents in shaping the learning environment reframes PGME as a shared enterprise of professional growth. Sustainable improvement depends on aligning educational, institutional, and cultural systems with the values of learner well-being, reflective professionalism, and social accountability. Through such integrative efforts, PGME can evolve into a humane, adaptive, and resilient ecosystem that nurtures both competent specialists and compassionate physician.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251406010 – Supplemental material for Difficulties Faced by Residents and Clues to Solutions: A Qualitative Study From the Medical Teachers’ Perspective
Supplemental material, sj-docx-1-inq-10.1177_00469580251406010 for Difficulties Faced by Residents and Clues to Solutions: A Qualitative Study From the Medical Teachers’ Perspective by Ozlem Midik, Meral Demiroren and Zeynep Baykan in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580251406010 – Supplemental material for Difficulties Faced by Residents and Clues to Solutions: A Qualitative Study From the Medical Teachers’ Perspective
Supplemental material, sj-docx-2-inq-10.1177_00469580251406010 for Difficulties Faced by Residents and Clues to Solutions: A Qualitative Study From the Medical Teachers’ Perspective by Ozlem Midik, Meral Demiroren and Zeynep Baykan in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We thank our medical teachers for sharing their opinions and experiences with us.
Ethical Considerations
The study protocol (2021/260) was approved by the Ondokuz Mayıs University Clinical Research Ethics Committee; written and oral consent was obtained from all participants.
Consent to Participate
At the beginning of the interviews, the purpose of the research was explained, and permission for audio/video recording was obtained. All methods were performed in accordance with relevant guidelines and regulations.
Author Contributions
All three researchers contributed equally to the design and development of the interview tool, interviewing, analyzing, writing, reading, and finalization of the article. All interviews were coded individually, and a collaborative process was conducted.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Detailed information on the themes, sub-themes, and codes will be made available upon reasonable request. The Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist was utilized to ensure the comprehensive and transparent reporting of the study’s qualitative methodology and findings.
Clinical Trial Number
Not applicable.
Declaration of AI Use
No scientific data were generated or altered using artificial intelligence. The authors take full responsibility for the accuracy, originality, and integrity of all submitted materials. Deeply Translate and ChatGPT were used only for language translation, then it was subsequently checked by a professional.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.