
Abstract
The United States spends more on health care than any other nation, yet hundreds of thousands of Americans die each year from conditions that could be prevented through basic lifestyle changes. Although about 80% of premature deaths are linked to unhealthy behaviors, Lifestyle Medicine (LM) receives little emphasis in most medical school and residency curricula. LM offers a low-cost, accessible approach to preventing and even reversing chronic disease through evidence-based lifestyle interventions (EBLI). Although LM fellowships exist, residency training is also important because it strongly shapes long-term clinical practice. However, most programs do not routinely teach LM principles or practical EBLI counseling skills. From October 2024 to June 2025, we delivered ten sessions introducing Family Medicine (FM) and Osteopathic Neuromusculoskeletal Medicine (ONMM) residents to core EBLI concepts. To measure impact, we retrospectively reviewed clinical notes, using keyword searches to assess the frequency and quality of documented EBLI recommended 3 months before and after the curriculum. Five independent reviewers scored notes using a standardized rubric. After training, mean scores increased from 0.9 to 1.9 for frequency (P = 0.023) and from 0.6 to 1.7 for alignment with EBLI (P = 0.011). These results indicate that integrating LM into routine resident didactics is feasible and improves EBLI integration into patient care.
“Experiential education is a pedagogical approach that emphasizes learning through direct engagement, reflection, and application of knowledge in real-world contexts.”
Introduction
Poor lifestyle factors—such as tobacco smoking, physical activity/sedentary behavior, and dietary inflammation index—impact noncommunicable disease mortality. These 3 factors were reported to lead to 80% of premature deaths in the United States 1 and cost over $400 billion each year in direct medical care and lost productivity at work. 2 Yet low-cost EBLI, which specifically address poor lifestyle factors, are not part of standard medical school training.3,4 Even though lifestyle prescriptions have been shown to reduce the incidence, morbidity, and mortality of cardiovascular diseases, type 2 diabetes, obesity, cancers, chronic respiratory diseases, depression, and many others, 5 many residency programs provide limited and inconsistent education in prevention and lifestyle promotion. There have been multiple calls to reform curricula to address this issue.6–9 Officially, the American College of Preventive Medicine, American College of Lifestyle Medicine, and the American Medical Association promote inclusion of lifestyle medicine into graduate medical education, but some residency programs lack funding or leadership to incorporate this training into the curriculum. Residency programs have been shown to reflect future expenditures for care, 10 aggressive vs conservative management ability, 11 and practice quality. 12 There is a wealth of evidence supporting efficacy with the use of LM for disease prevention, treatment, and reversal of chronic lifestyle-related disease. 13
One potential roadblock to effective EBLI implementation is that most think of prescribing medications as an event, however prescribing EBLI is a process (i.e., prescribing weight loss). If physicians aren’t trained in effectively prescribing EBLI—personalized and actionable prescriptions with frequency, duration, and intensity, where applicable—then even if the best evidence is conveyed, the patient may not buy into the lifestyle change, effectively negating the prescription. One significant challenge is that physicians are seen as more believable if they adhere to the recommended lifestyle modification themselves. For example, patients are less likely to respond to prescribed obesity treatment if their physician is obese. 14 Lifestyle medicine training courses for residents have shown improvement in managing patients in regard to smoking, obesity, and physical activity. An improvement in self-reported physical activity has been observed in overweight participants in these training sessions. 15 The American College of Lifestyle Medicine has residency training programs readily available, however, some programs may not have the leadership to conduct one of these programs. It is therefore suggested that an intentionally developed EBLI program will increase residents’ integration of LM into patient care.
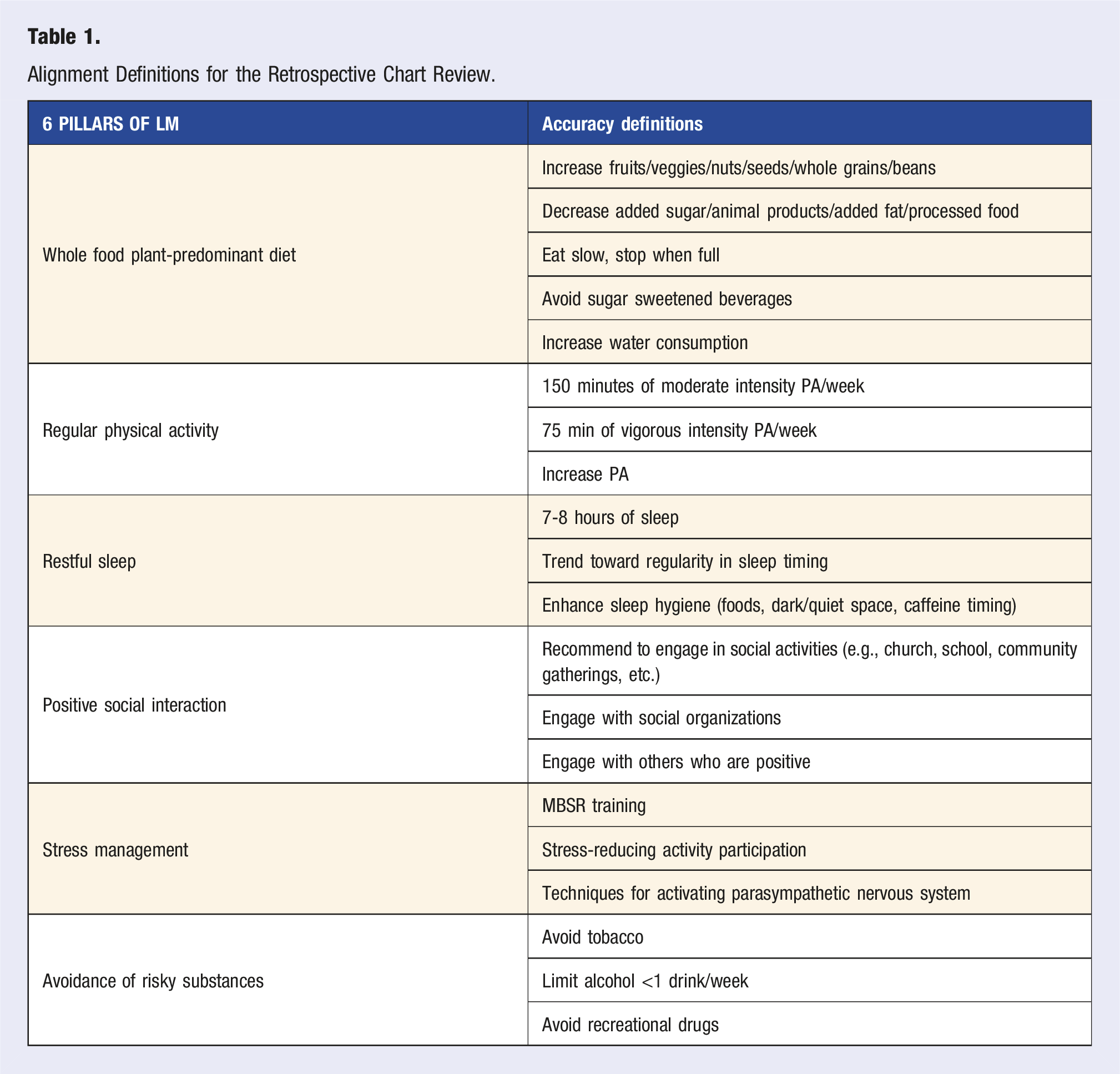
LM education is required to improve both physician understanding and EBLI skills of the 6 pillars of LM to provide higher quality care. Namely, a whole food plant-predominant eating pattern, regular physical activity, restful sleep, stress management, positive social interaction, and the avoidance of risky substances. Many of these EBLI are low cost or even free. Active learning strategies with multifaceted interventions are suggested to be most effective in training residents. 16 Our hypothesis is that this LM training program, as described in the methods section, will add to the high educational standards of the American College of Lifestyle Medicine by demonstrating potential pathways to increase interest, frequency, and alignment with the best available evidence of EBLI in primary care residents in the context of rural residency programs without substantial LM leadership.
Methods
LM Training Program
Alignment Definitions for the Retrospective Chart Review.
Study Design
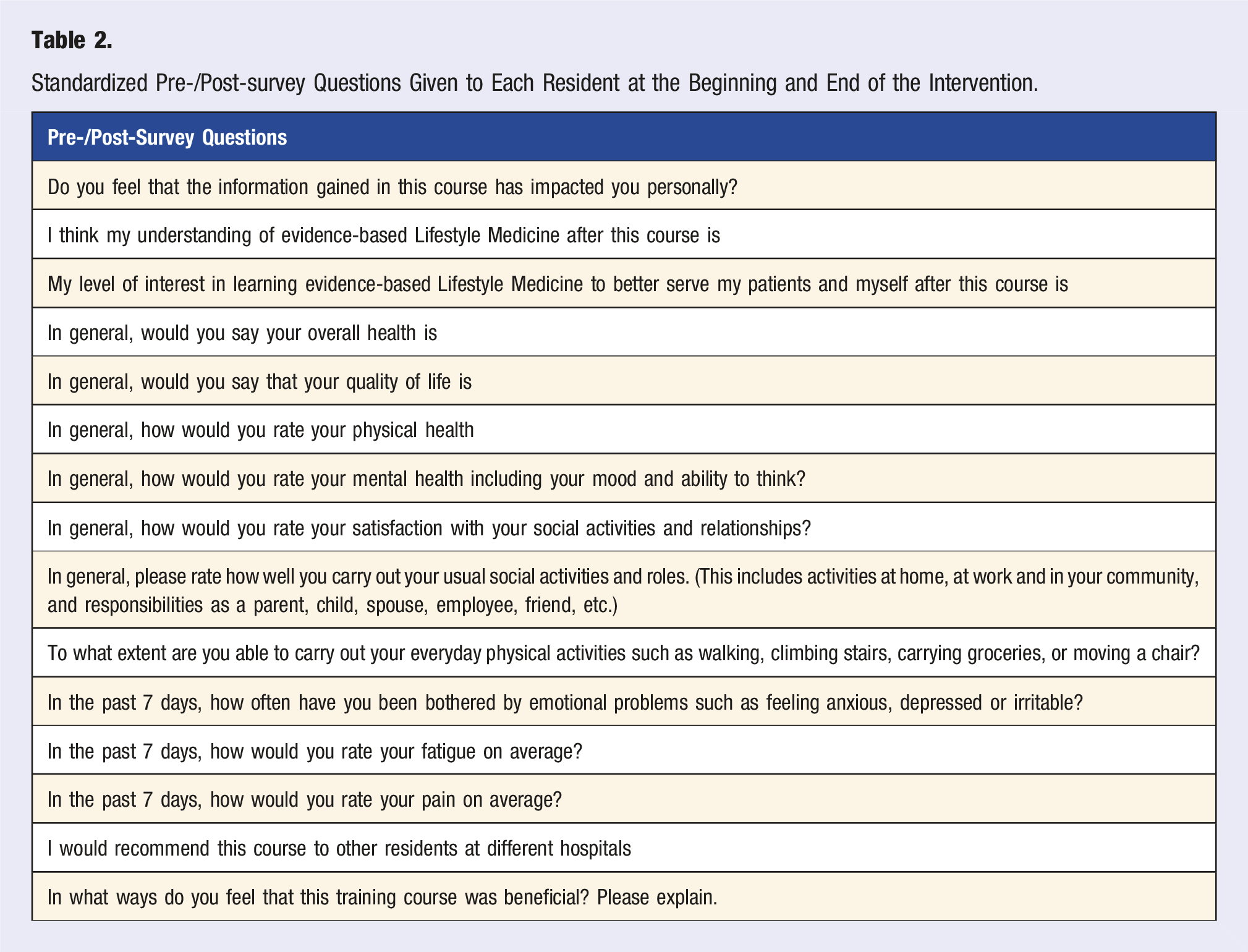
Pre-/post-attitude surveys were collected from residents immediately prior to and following the intervention. Comprehension surveys were also collected after each session.
Standardized Pre-/Post-survey Questions Given to Each Resident at the Beginning and End of the Intervention.
Inclusion criteria for chart audit participation in this study is shown for this study for all FM and ONMM residents at NRMC for the 2024/2025 academic year. They must have seen patients in their own clinic during both timeframes: 7/1/2024 and 9/30/2024 (T1) and 4/1/2025 and 6/30/2025 (T2). Exclusion criteria include leadership in the study, not seeing patients in T1 or T2. EBLI were determined by adherence to the included rubric (Table 1). The chart audit took place over a 2 week time frame. Each chart was individually reviewed and graded by 3 independent reviewers, then discrepancies were reconciled by 2 different reviewers and a final report was delivered to the statistician.
10 pre-intervention and 10 post-intervention charts from each resident were reviewed by 5 independent reviewers. A case discussion occurred on each disagreement until ratings were unanimous. In order to evaluate the effectiveness of this intervention, a rubric (Table 1) was created and verified by the FACLM physician mentioned previously using the 6 pillars of LM model. Assessment of frequency and alignment of EBLI was performed based on a retrospective chart audit, searching for keywords in the plan section of the notes for all visits 3 months before and 3 months after the intervention. Systematic alignment to EBLI is defined by the rubric. The chart audit was performed by 5 independent reviewers who graded and reconciled their scores. Residents were classified as either “adopters” or “nonadopters” by improving their alignment scores. The first 10 charts during each time period for each resident were selected for review.
Statistical Procedures
Mean (SD), median (interquartile range [IQR]) and frequency (percentage) are used to summarize the survey responses and the chart audit results. For survey questions that were asked in Week 0, Week 3 and Week 9, Friedman test was used to test for the overall difference, followed by a pairwise comparison with Bonferroni correction when an overall difference was detected. For questions that were asked only in Week 0 and Week 9, Wilcoxon signed ranks test was used. Wilcoxon signed ranks test was also used to compare the pre- and post-intervention frequency of EBLI and alignment with the scoring rubric identified by the chart audit. The effect size was calculated by dividing the Z statistic by the square root of the total number of observations. 17
Results
Survey Results of 11 Residents Demonstrated an Increase in Self-Perceived Improvement of Knowledge of Lifestyle Medicine and No Other Significant Findings.
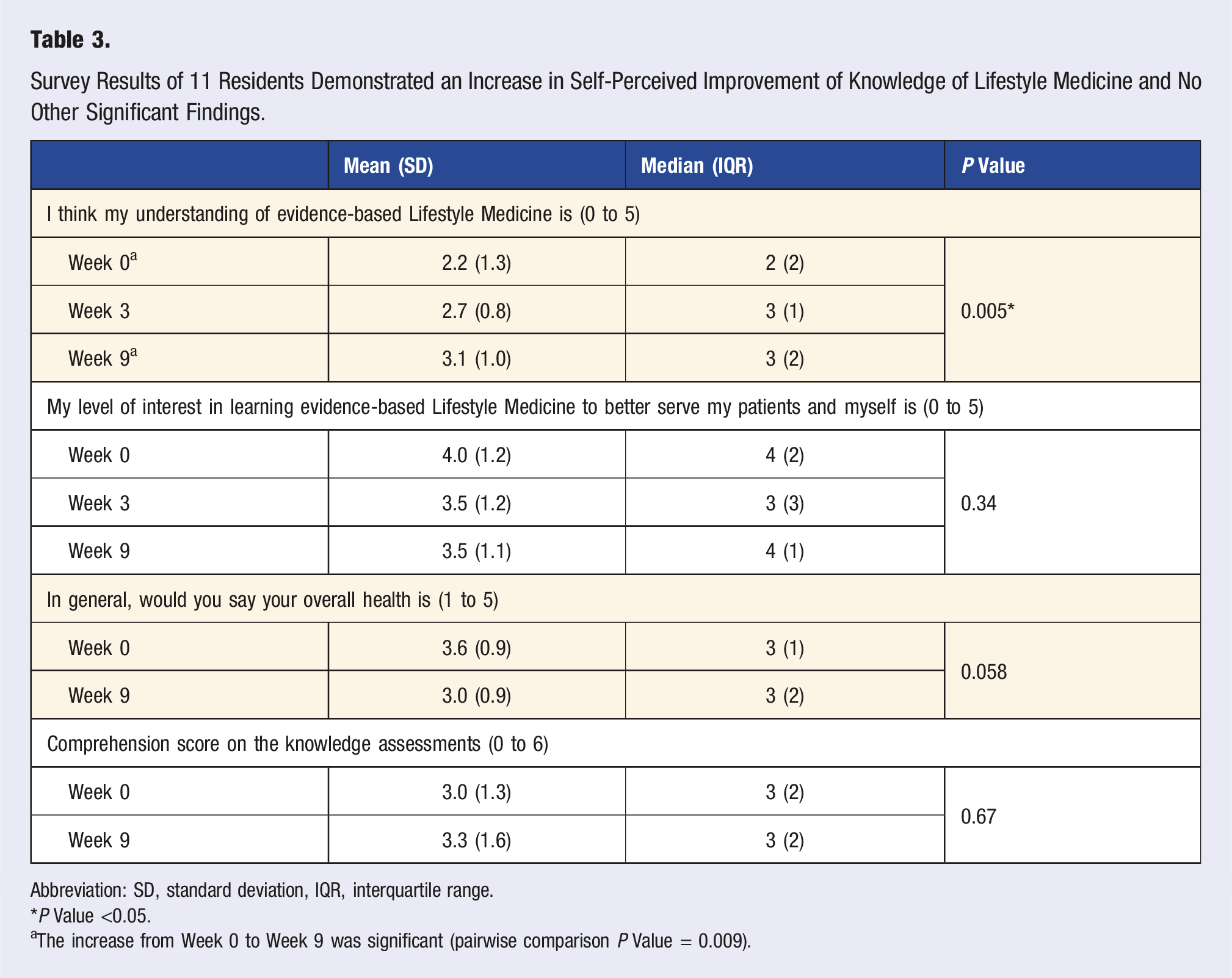
Abbreviation: SD, standard deviation, IQR, interquartile range.
*P Value <0.05.
aThe increase from Week 0 to Week 9 was significant (pairwise comparison P Value = 0.009).
Out of 19 residents, two residents’ chart audits were disqualified: one was involved in data analysis and study design and the other was on out rotations and didn’t see any patients during T2, as shown in the flow chart (Figure 1). During the chart audit, the 5 independent reviewers agreed on all of the final results with the exception of 6 charts for a final 98.3% concordance rate. For these 6 questions, a board certified LM physician was consulted to provide insight, and a final decision was made by the reviewers. In total, 340 charts were audited from 17 residents.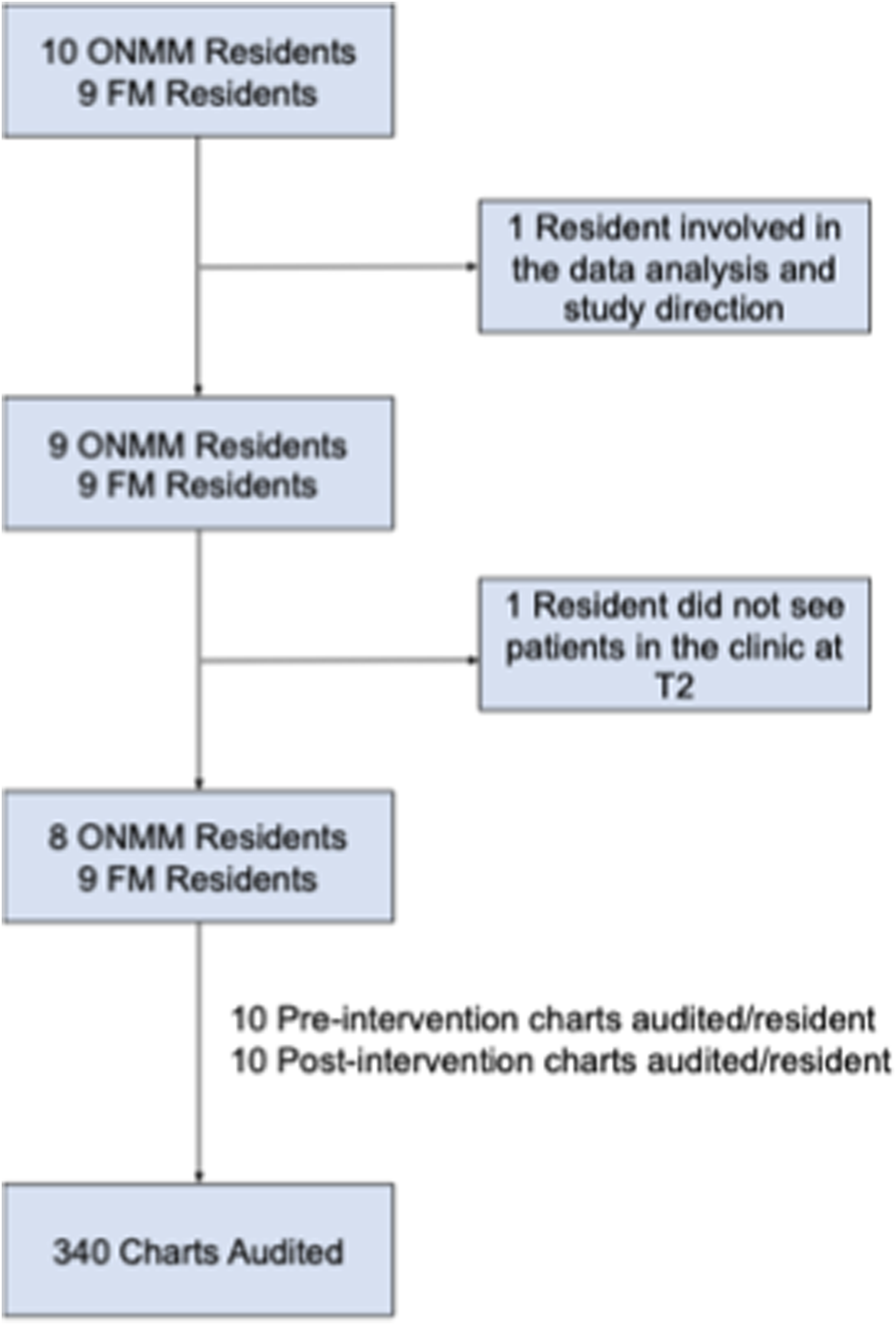
Pre/Post Frequency Demonstrated That Total Number of Charts With EBLI Prescriptions Given Increased Specifically Mentioning Diet and Stress Management. Also, the Alignment of Charts to the Guidelines in Table 3 Increased Significantly.
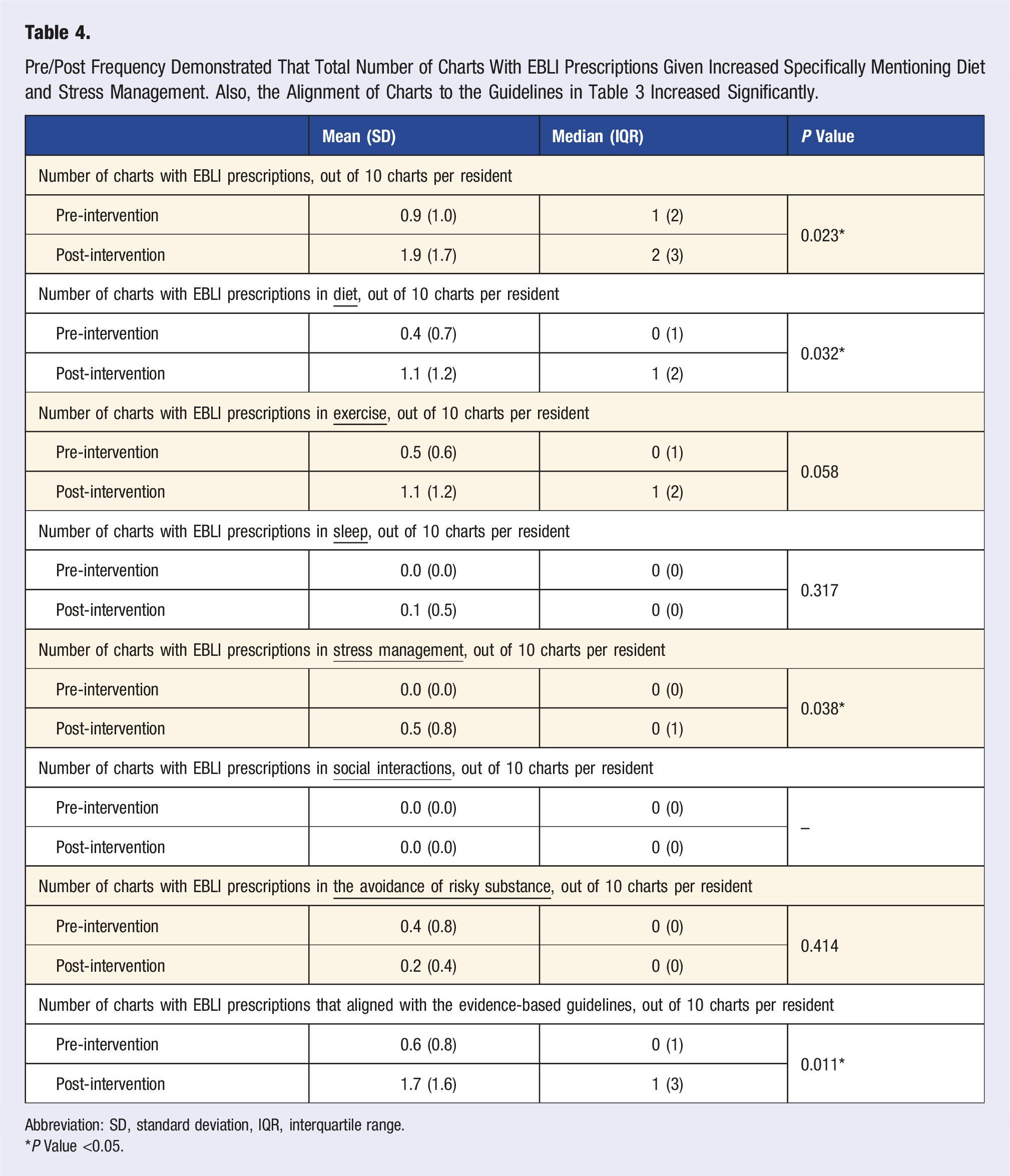
Abbreviation: SD, standard deviation, IQR, interquartile range.
*P Value <0.05.
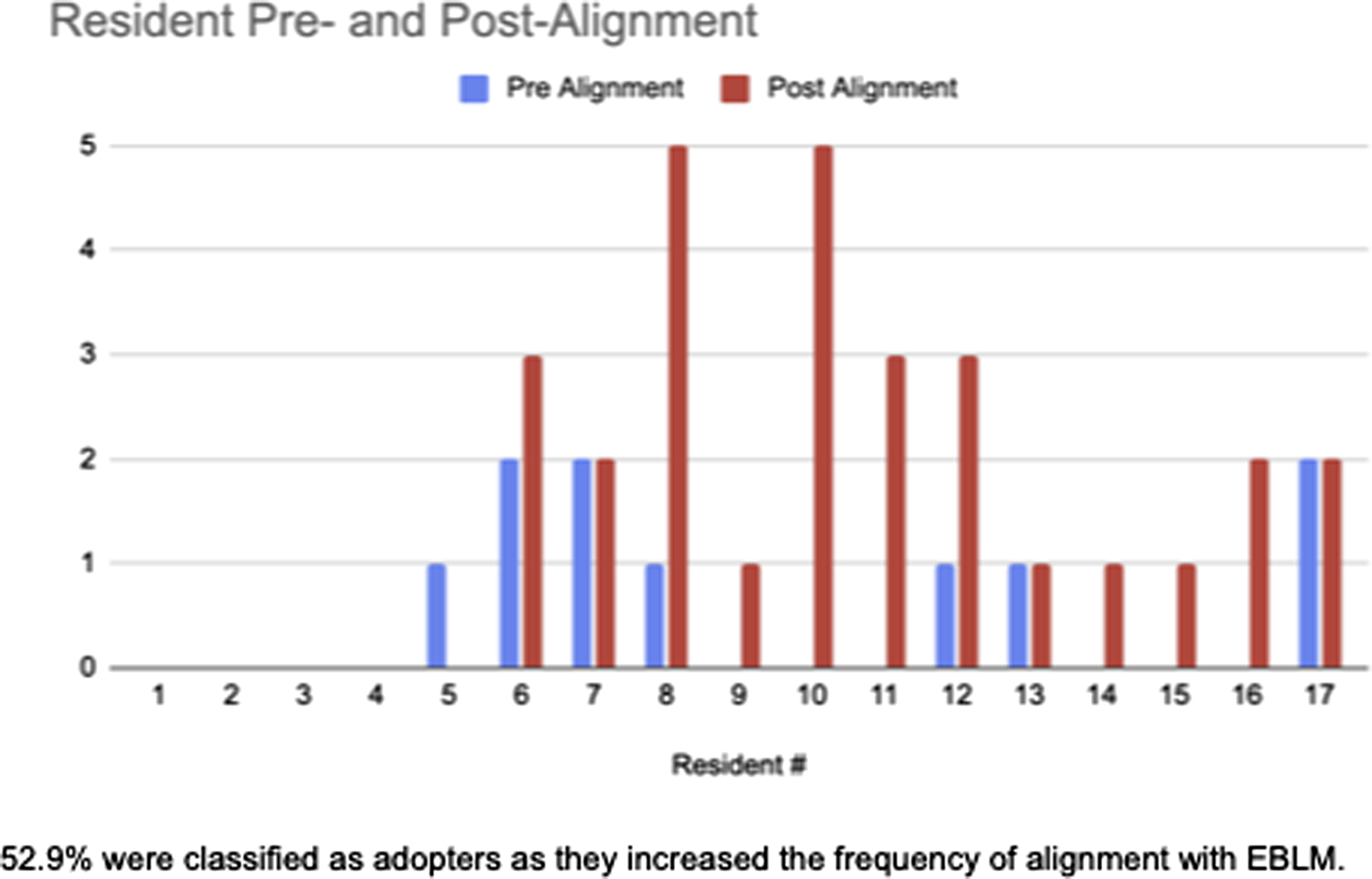
Alignment improved or remained the same with all residents except one.
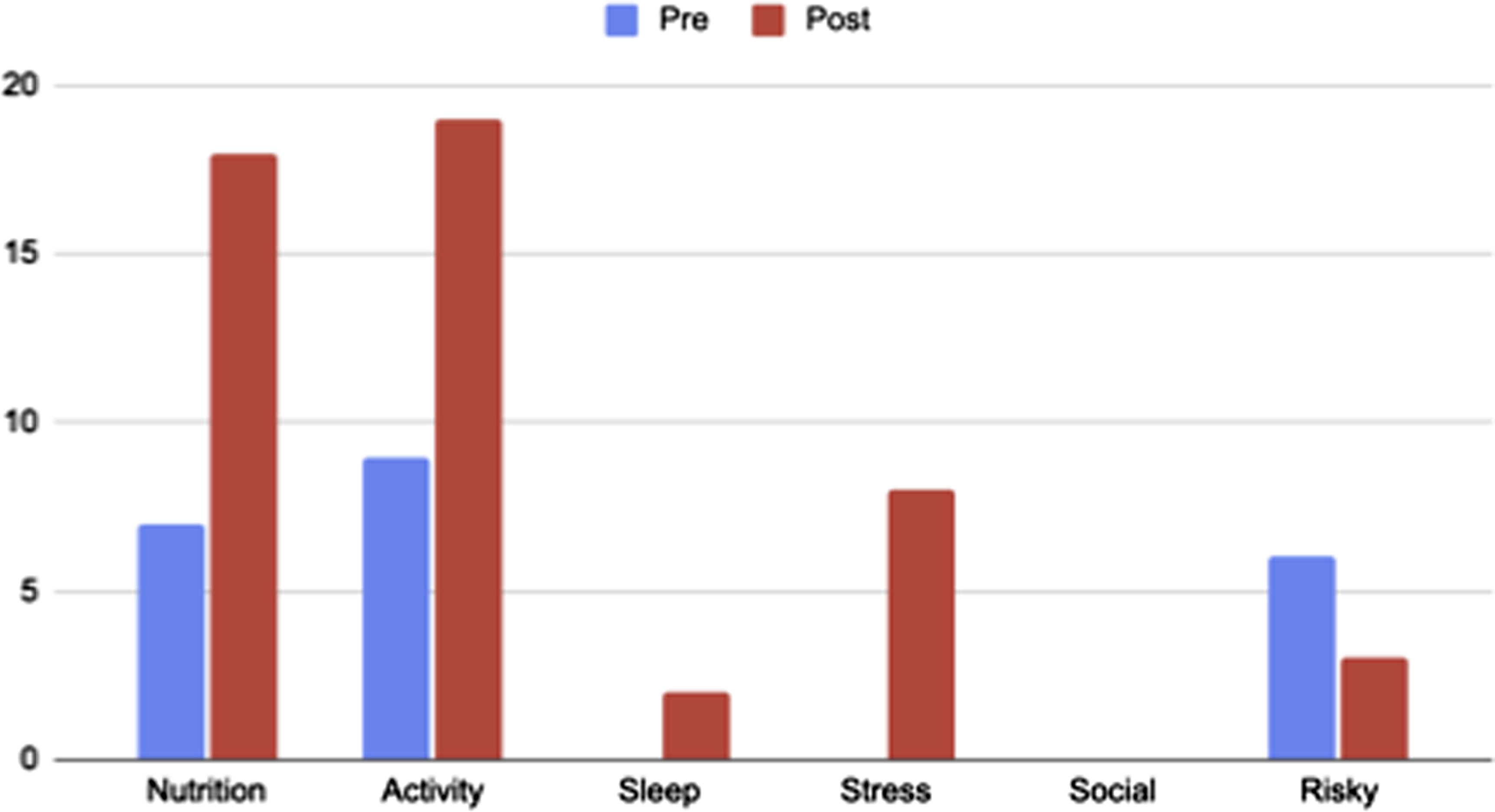
Activity and Nutrition were the most common categories for lifestyle prescriptions. There were a moderate amount of stress of risky behavior prescriptions, and minimal mentions of Sleep and Social prescriptions.
Discussion
Primary Findings and Clinical Significance
The statistically significant improvements in both frequency (P = 0.023) and alignment (P = 0.011) of EBLI, with medium effect sizes, represent meaningful changes in clinical practice behavior. The 111% increase in EBLI (mean from 0.9 to 1.9 in every 10 charts) demonstrates that residents not only learned LM principles but actively implemented them in patient care. This behavioral change is particularly noteworthy given the well-documented challenges 18 in modifying physician prescribing patterns 16 and the limited time typically allocated to lifestyle counseling in residency training.
A study in 2003 by McGlynn et al, found that patients received recommended care 54.9% of the time, in 12 different metropolitan areas of the United States. 19 However, this is with fully trained practitioners and not physicians in training. The classification of 52.9% of residents as “adopters” indicates that the majority of participants meaningfully integrated EBLI into their practice and felt it important enough to document, suggesting the educational format was both acceptable and effective. We saw 6% of the charts (mean 0.6 in every 10 charts) properly aligned at the beginning of the study and 17% at the end. Even though this is a great improvement (183% increase), we would hope to double this number by simplifying the documentation procedure within our EMR. It is understood that these physicians are still trainees and this rate will also likely increase once residents gain more experience and comfort utilizing EBLI. A couple of residents documented 0% EBLI and others were documenting it in 50% of their charts by the end of the study. This was also without prompting the residents to increase their documentation of EBLI. These high documenting residents recognized that the EBLI was important to include in the patient’s medical record. The observed improvements likely represent a conservative estimate of actual behavior change. As noted in resident feedback, many lifestyle recommendations may have been given verbally but not documented in the medical record. This finding highlights a critical gap between clinical practice and documentation that has implications for quality metrics, billing, and continuity of care. Future interventions should incorporate specific documentation training and potentially electronic medical record template development to capture the full extent of LM integration.
The decrease in risky substance counseling (from 6 to 3 EBLI) may reflect baseline saturation of tobacco cessation documentation rather than decreased attention to substance use. Since tobacco cessation counseling is often automatically documented regardless of relevance, residents may have developed more targeted approaches to substance use counseling post-intervention.
While diet, and stress management had the most significant increase in EBLI frequencies, we also saw modest increases in physical activity EBLI due to a high baseline frequency of physical activity EBLI. Risky substance use was the only category to decrease in frequency, whereas social interactions did not have a single EBLI. Noticing the decrease in risky substance counseling, it was possibly due to baseline high documentation of tobacco cessation, sampling error, or missed rankings by the reviewers. This is an outlier we believe. There is much focus on smoking cessation, that it’s easier to talk about with your physician. It is also something that has been demonstrated to be grossly deleterious to numerous aspects of human health for years and a significant contributor to morbidity and mortality, 20 however other lifestyle choices like diet, exercise, sleep, stress management, and positive social interactions are challenging to consistently make in the real world. 21
There was no statistically significant difference in interest level during the study.
National Importance
It is imperative for physicians in America to gain experience and competency prescribing EBLIs, as these lifestyle-related conditions are preventable, treatable, and reversible when compared to traditional medical care, as these make up the most common causes of death in America. 1 Lifestyle also plays a substantial role in the financial health of the United States, as ∼90% of health care spending is due to chronic lifestyle-related conditions, 22 which can be prevented, effectively treated or at times reversed with EBLI. As an example, the number one cause of death, cardiovascular disease, takes the lives of more than 843 000 Americans every year, with over $233.3 billion in health care costs, and $184.6 billion in lost job productivity. This is financially unsustainable.
Acceptability
Only one resident’s survey was removed from analysis due to inauthentic answers, such as marking that they had the level of knowledge to give national presentations in LM at the beginning of the study and then having no knowledge of LM at the end of the study. All other submitted surveys indicated that they thought this training was worthwhile to their training and that it had a positive effect on participants’ lives. More effort may need to be taken to inform all of the participants in future iterations that prevention is an important form of medicine and is part of the normal FM and ONMM residency programs. Efforts were made to avoid adding additional workload to resident physicians’ schedules. All ten educational sessions were completed within the regularly scheduled hospital didactic training schedule. The majority of residents reported that they would absolutely recommend this training for other residency programs.
Educational Format
Experiential education is a pedagogical approach that emphasizes learning through direct engagement, reflection, and application of knowledge in real-world contexts. This educational philosophy, rooted in the work of John Dewey 23 and later formalized by David Kolb’s 24 experiential learning theory, involves a cyclical process where learners encounter concrete experiences, reflect on those experiences, form abstract concepts based on their reflections, and then test these concepts through active experimentation. In the context of medical education, experiential learning moves beyond traditional didactic instruction to immerse learners in authentic clinical scenarios where they can observe, practice, and refine their skills while receiving feedback.
The two-phase educational approach proved successful in creating practice change in resident physicians. Phase 1’s foundation-building through lectures, self-reflection, and surveys appeared to prepare residents for Phase 2’s more intensive pillar-specific training and assessments. The inclusion of a health-promoting group meal and peer discussion session may have reinforced learning through experiential and social components, aligning with Kolb’s experiential learning cycle and Constructivist Learning Theory.
Implications for Medical Education
These findings support the integration of LM education into residency training curricula. The demonstrated feasibility of the educational format and the significant practice changes suggest that similar programs could be implemented across residency programs with reasonable resource investment. The fact that objectively, resident knowledge did not substantially increase on the 6-question assessments given after each session, but the frequency and alignment both did increase of their EBLI usage in the clinics, suggests that the assessment was not valid for assessing the end result. This could be either because the initial questions were too easy or that asking only 6 questions lacked statistical power to differentiate knowledge retention from baseline. This does not demonstrate that this education program is insufficiently robust because residents were ultimately successful with increasing both their frequency and alignment with EBLIs, though it suggests that the interval assessment method of knowledge retention subsequent to each session with 6 questions is not a valid measure of post-session competency, likely more questions and clinical situations would provide a fuller assessment of their knowledge. The 9-session format appears to provide sufficient exposure without overwhelming already intensive training schedules, though it is important to emphasize at home study. The intention behind this project was to provide LM education for residents at sites that lack adequate support or leadership for more comprehensive LM residency education.
The study also suggests that LM education should emphasize documentation practices to ensure that clinical activities are accurately captured for quality improvement, research, and patient care coordination purposes.
Limitations
Several limitations should be acknowledged. The single-site design and small sample size (n = 17) limit generalizability, though the effect sizes suggest the findings may be robust. The retrospective chart audit methodology, while objective, depends on documentation quality and may underestimate actual counseling provided. Additionally, the 3-month post-intervention follow-up period, while adequate to demonstrate initial behavior change, does not address long-term sustainability of practice changes. There is no intrinsic assessment of success of the active learning based program. In order to keep the questionnaire short, we only had 6 questions to assess knowledge in the survey.
However, next time, we would ensure that the interval quizzes were more robust at distinguishing EBLI knowledge between groups. This could be done either in addition to longer quizzes or instead by having them deliver EBLI to a standardized patient, which would be a valid assessment of the intended outcome. We would also create a click box in our EMR beforehand to make this intervention more effective. There is a substantial need to keep documentation streamlined for the residents. Optimally, we would have the LM questions available in the EMR to refer to during the visit if necessary to serve as prompts.
Strengths
EBLI education is required to provide higher quality care. Strengths of this research are that even with the EMR challenges, residents still interpreted the importance of these lifestyle modifications as “important enough” to document in the patient’s medical record. This intervention showed that their behavior was indeed impacted, even though some may have less perceived interest in LM. That could have been due to generalized over-exuberance when starting residency and then feelings of being worn out after the year of residency/internship at the conclusion of the study, the presentations could have been inadequately engaging, or they may have been trying to pare down their learning requirements to just the necessities and didn’t see LM as a necessity. What was a large success of this study was that it was able to positively impact resident EBLI utilization patterns and was part of regular didactic programming; it didn’t add additional work for the residents. This does mean that if other programs are interested in adopting this model, then ten 50-minute-sessions might need to be created inside the pre-existing curriculum.
Future Directions
Future research should include multi-site studies with longer follow-up periods, patient outcome measures, and potentially direct observation of counseling behaviors. Investigation of optimal documentation methods and electronic health record integration would enhance clinical implementation. Additionally, exploring the differential response by training level could inform targeted educational approaches.
Conclusion
This pilot study successfully demonstrates that structured LM education can produce significant, measurable changes in resident behavior. The intervention’s effectiveness in improving both frequency and evidence-based alignment of EBLI, coupled with high resident acceptability, supports the feasibility and value of integrating LM education into residency training. These findings provide a foundation for larger-scale implementation studies and contribute to the growing evidence base supporting LM education in medical training.
Given the critical role of lifestyle factors in chronic disease prevention and management, and the limited exposure to LM in traditional medical education, this study offers a practical, evidence-based approach to addressing a significant gap in physician training. The results suggest that with appropriate educational interventions, resident physicians can become effective practitioners of LM, potentially improving patient outcomes and health care quality while reducing health care costs through prevention-focused care.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.