
Abstract
Acute rheumatic fever (ARF) and rheumatic heart disease (RHD) remain significant public health challenges in low- and middle-income countries, including Nepal. This study aimed to develop and validate a tool to assess children’s knowledge of ARF and RHD. A 14-item multiple-choice questionnaire was developed through expert consultation and a systematic translation and back-translation process. Content validity was evaluated by 10 experts using item-level and scale-level content validity indices (I-CVI and S-CVI) and the Content Validity Ratio (CVR). A cross-sectional survey of 207 students aged 11 to 16 years was conducted in public schools. Item difficulty and discrimination indices were calculated, and internal consistency was assessed using the Kuder-Richardson Formula 20 (KR-20). Known-groups validity was tested by comparing scores across grades and prior exposure to RHD screening programs. The scale demonstrated excellent content validity (S-CVI/Ave = 0.91) and good internal consistency (KR-20 = 0.772). Item difficulty indices ranged from 0.32 to 0.61, and discrimination indices from 0.23 to 0.36, both within ideal ranges. The mean knowledge score was 6.05 ± 3.43. Higher knowledge scores were observed among older students, those in higher grades, and those previously screened for RHD (P < .05). The RHD Knowledge Scale is a valid and reliable instrument for assessing children’s understanding of ARF and RHD. Although this study was limited to a single municipality and did not include test–retest reliability, the tool shows strong potential for adaptation and validation across different cultural, linguistic, and geographical contexts. Beyond research settings, this tool can serve as a practical means to integrate ARF and RHD education into school health programs and to monitor the effectiveness of nationwide prevention initiatives.
Keywords
Rheumatic heart disease remains a major global public health challenge, and existing knowledge assessment tools are largely context-specific, single-use instruments with limited or no evidence of validation, reliability, or psychometric rigor.
This study introduces and validates a psychometrically robust RHD Knowledge Scale, providing a standardized tool to measure, compare, and evaluate school-based ARF and RHD educational interventions.
Introduction
Streptococcus pyogenes or Group A β-hemolytic Streptococcus primarily affects children and adolescents.1,2 If untreated, ARF can progress to rheumatic heart disease (RHD), a chronic condition causing permanent heart valve damage.3,4 The World Health Organization (WHO) estimates RHD contributes to 288,348 deaths annually, with a disproportionate burden in low- and middle-income countries (LMICs). 5 In 2019, global RHD incidence reached 2.79 million cases, a 49.7% increase since 1990. 6 South Asia reports the highest prevalence (12.17 million cases), while Western Sub-Saharan Africa has seen the largest case increase (162.05%) from 1990 to 2019. 6 Despite a 15.6% reduction in RHD-related deaths globally, 0.31 million deaths were attributed to RHD in 2019. 6
In resource-constrained settings, barriers such as limited awareness, financial constraints, and inadequate access to healthcare hinder early antibiotic treatment of streptococcal infections, a key preventive measure for ARF.2,5 Several studies from LMICs have demonstrated that low RHD-related knowledge persists even among trained health personnel and community members. In Uganda, only 43.8% of health workers showed good knowledge of ARF and RHD, 7 while in Ethiopia, fewer than half of nurses (48.7%) demonstrated adequate understanding of RHD prevention and management despite working in cardiac centers. 8 Similar studies from Africa and the Middle East have assessed RHD or ARF-related knowledge using self-developed or adapted questionnaires.7,9,10 Although these tools varied in length and content, they were largely context-specific instruments designed for single-use surveys, with little or no evidence of validation or reported psychometric properties such as content validity, reliability, or item performance.
In Nepal, RHD poses a significant public health challenge, particularly among school-aged children. In 2019, RHD accounted for 1.5% of all deaths, up from 1.1% in 1990. 11 Data from the Nepal Heart Foundation (NHF) screening program estimated an RHD prevalence of 2.22 cases per 1000 schoolchildren, with the burden highest among those aged 11 to 16 years. 12 Despite this, studies assessing ARF and RHD knowledge in Nepal are scarce, with few investigations focusing on healthcare workers or community adults, leaving a critical gap in child-focused knowledge assessment.13,14
Given the preventable nature of ARF, improving knowledge among children is an essential public health priority intervention.2,5,15 Schools offer an ideal platform for health education, enabling early engagement with children during formative years to initiate preventive behaviors and promote timely health-seeking practices. 16 To address this, the “Colours to Save Hearts” project (ClinicalTrials.gov: NCT07065474) was designed as a school-based intervention to improve awareness of ARF and RHD among Nepalese children. However, the absence of validated, child-appropriate tools to measure ARF and RHD knowledge prompted the research team to develop a scale for evaluating such educational interventions. This study aimed to develop and validate the RHD Knowledge Scale, an instrument designed to assess knowledge of ARF and RHD to fill a critical methodological gap in global RHD awareness research.
Methods
Study Design and Participants
This cross-sectional study was conducted as a preliminary phase of the Colours to Save Hearts project in Nepal to enhance awareness of acute rheumatic fever (ARF) and rheumatic heart disease (RHD) among school-children. The cross-sectional phase of this study was designed, conducted, and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, and the completed STROBE checklist is provided in the Supplemental materials. To assess students’ knowledge of ARF and RHD before and after the educational intervention, the RHD Knowledge Scale was developed and validated in 3 sequential phases: item generation, content and face validity assessment, and field testing for reliability and item performance.
Item Generation and Refinement
The initial pool of questions was developed through a review of relevant literature and previously conducted studies on RHD awareness,13,17,18 along with a review of reference materials, such as World Health Organization (WHO) guidelines for RHD. 15 Expert consultations with cardiologists, pediatricians, public health professionals, and education specialists contributed to listing the potential questions. From this process, 16 multiple-choice questions were generated, covering 4 key domains: (i) basic knowledge and symptoms of ARF/RHD, (ii) risk factors, (iii) prevention, and (iv) treatment. Each question included 4 response options, of which 1 was correct, and 3 were distractors. Responses were scored dichotomously (1 for correct, 0 for incorrect or no response). The initial set of items was developed and reviewed in English by the panel of experts. After finalizing the content, the tool was translated into Nepali to ensure cultural and linguistic appropriateness for the target population. The translation process followed a standardized approach involving 2 independent bilingual experts with health-related backgrounds who were fluent in both English and Nepali. One expert translated the items from English to Nepali, while the second performed a back-translation from Nepali to English without access to the original version. The back-translated version was compared with the original English version to identify and resolve discrepancies through consensus. This process ensured conceptual and technical equivalence between the 2 versions, thereby enhancing the clarity and accuracy of the questionnaire for use among Nepali-speaking schoolchildren.
Content and Face Validity
Face validity, a preliminary subjective assessment of a tool’s ability to appear relevant and appropriate for its intended purpose from the perspective of both test participants and domain experts, 19 was carefully examined. To achieve this, cognitive interviewing was employed as a qualitative method that assesses how respondents interpret and respond to survey items, thereby identifying ambiguities, comprehension issues, and opportunities for improved clarity.20,21
Cognitive interviews were conducted in 2 phases. Participants for cognitive interviews were purposively selected to ensure diversity in grade level, gender, and prior exposure to RHD screening programs, enabling the assessment of comprehension across different subgroups. In the first phase, 5 schoolchildren were individually interviewed to assess their understanding of each item, elicit subjective impressions, and identify problematic wording. This process led to important modifications, such as simplifying technical terms (eg, replacing “streptococcal infection” with “throat infection caused by bacteria”) and rephrasing items for clarity, such as revising “What is the main risk factor of rheumatic heart disease?” to “Which infection can lead to rheumatic heart disease?”; revising “How can doctors conform RHD?” with “What is the most effective test to detect rheumatic heart disease?”
Two questions were ultimately removed because they were deceptively difficult despite appearing straightforward. The first, “What increases the chance of getting rheumatic heart disease?”, was too vague, as children tended to select factors such as diet or hygiene at random, since these are commonly associated with many illnesses, rather than demonstrating specific knowledge about RHD. The second, “Which of these are signs of rheumatic fever?,” required students to differentiate between multiple symptoms. During interviews, children frequently chose symptoms they had seen in other common illnesses, indicating confusion and difficulty in identifying disease-specific signs. Because these items introduced misunderstanding and added cognitive burden, they were removed. Following these refinements, the tool was finalized with 14 items, each scored dichotomously (1 = correct, 0 = incorrect or no response), yielding a possible total score range of 0 to 14, with higher scores indicating greater knowledge.
Following this, the revised items were then evaluated by a panel of 10 experts in cardiology, pediatrics, public health, and education, who rated each item for relevance, clarity, and appropriateness using a 4-point scale (1 = not relevant/clear/appropriate, 4 = highly relevant/clear/appropriate). Agreement among experts was quantified using the Content Validity Ratio (CVR) and Content Validity Index (CVI). The CVR was calculated using Lawshe’s formula CVR ([n e −N/2]/[N/2]), where n e is the number of experts rating the item as “quite relevant” or “highly relevant,” and N is the total number of experts. The minimum acceptable CVR threshold was determined based on Lawshe’s criteria for 10 experts. 22 The Content Validity Index (CVI) was computed at both the item level (I-CVI) and the scale level (S-CVI). The I-CVI was calculated as I-CVI (Number of experts rating the items as 3 or 4)/(Total number of experts). The scale-level CVI (S-CVI) was determined by averaging the I-CVI scores of all retained items. 22 The second round of cognitive interviews among 4 students (n = 4) was conducted after the expert’s assessment. The new set of cognitive interviews confirmed no further issues, ensuring age-appropriate language and comprehensibility.
Field Testing: Sampling and Data Collection
The pre-final tool was pilot tested among a sample of 207 schoolchildren. The sample size was determined based on established recommendations for validation studies, which suggest a subject-to-item ratio of at least 10 participants for each scale item (10:1), with an absolute minimum of 100 participants and preferably up to 200.19,23,24 Given that the tool consisted of 14 items, a minimum of 140 participants would have been sufficient. In Budhanilkantha Municipality, there are a total of 19 public schools; from these, 3 schools were randomly selected to balance representativeness and logistical feasibility. Within each school, 1 grade between Grade 6 and Grade 9 was chosen using simple random sampling. All students present in the selected classrooms (n = 207) were included in the study. Data were collected in classroom settings from August 14 to 15, 2025, under the supervision of trained facilitators, who provided standardized instructions to ensure uniform administration. The questionnaire was self-administered, and students completed the survey independently within approximately 15 min.
Statistical Analysis
Data were entered into Microsoft Excel with data validation commands to ensure accuracy. All questionnaires were reviewed for completeness at the time of collection, and no missing data were observed. Each response sheet was cross-checked during data entry to ensure data integrity. Descriptive statistics (means, standard deviations, frequencies, and percentages) were calculated to summarize sociodemographic characteristics (eg, age, sex, grade, parental education) and the distribution of knowledge scores. Excel was also used to compute I-CVI and S-CVI for content validity. Item performance was evaluated using item difficulty (proportion of correct responses per item) and discrimination indices. 25 Item difficulty index, also referred to as item easiness, reflects the proportion of correct answer on a given item where its general purpose scales will focus on items with medium difficulty ranging between 0.4 and 0.6. 19 Item discrimination was assessed using point-biserial correlations between individual item scores and total scores additionally upper-lower discrimination index (D = PH − PL) was calculated where PH and PL are proportions correct in the top and bottom 27% of scorers (n = 56 each) based on total score ranks where D ≥ 0.20 was considered acceptable, with ≥0.40 excellent. 26 Internal consistency of the RHD Knowledge Scale was assessed using the Kuder-Richardson Formula 20 (KR-20), which is mathematically equivalent to Cronbach’s alpha for dichotomously scored items. A KR-20 value ≥ 0.70 was considered acceptable for reliability. 27 Construct validity was assessed in 2 ways through Pearson correlation coefficients examined associations between knowledge scores and continuous variables such as age and grade and, known-groups validity was evaluated by comparing mean knowledge scores across sociodemographic subgroups (eg, age groups, sex, grade level, parental education, and prior exposure to RHD screening) using independent-samples t-tests or one-way ANOVA with Tukey’s post-hoc tests where appropriate.
Ethical Statement
Ethical approval for the Colours to Save Heart project has been obtained from the Institutional Review Board of the Nepal Health Research Council (REF: 2678, Protocol No: 152_2025). Permission was obtained from each selected school before data collection. Written informed consent was secured from parents or guardians, and written assent was provided by all participating students. Separate consent and assent were obtained for those who participated in the cognitive interviews. All study procedures adhered to the principles of the Declaration of Helsinki.
Result
A total of 207 students participated in the study, with a mean age of 13.8 years (SD = 1.2; range 11–16). Two-thirds (66.2%) were aged ≤ 14 years, and males comprised 59.4% of the sample. Grade distribution was 42.0% in grade 6, 19.8% in grade 8, and 38.2% in grade 9. Parental education levels were low: 33.3% of mothers and 18.8% of fathers had no formal education, while 41.5% of mothers and 46.4% of fathers had completed only primary school (Table 1).
Sociodemographic Characteristics of the Participants (n = 207).

Content validity was assessed by 10 experts who rated each item on relevance, clarity, and appropriateness. Item-level CVIs ranged from 0.70 to 1.00 for relevance, 0.80 to 1.00 for clarity, and 0.80 to 1.00 for appropriateness, with an overall mean I-CVI of 0.91. Scale-level CVI (S-CVI/Ave) was 0.91, indicating strong overall content validity, although universal agreement (S-CVI/UA) was achieved for only 57% of items (8/14). Content Validity Ratios (CVR) for relevance ranged from 0.40 to 1.00 across items, with most exceeding the minimum acceptable threshold. Two items with slightly lower CVR values (0.40) were retained after qualitative review because they captured conceptually essential aspects of RHD knowledge, particularly regarding early symptom recognition and treatment-seeking behaviors, which experts agreed were critical for educational interventions despite marginally lower quantitative ratings. Most items showed acceptable difficulty (0.30–0.70), indicating that the tool was neither too easy nor too difficult. Discrimination indices were ≥0.20 for most items, demonstrating the tool’s ability to distinguish between students with high and low knowledge levels. (Table 2).
Content Validity Indices, Item Difficulty, and Discrimination Indices for the RHD Knowledge Scale.

I-CVI = item-level content validity index; S-CVI/Ave = scale-level content validity index (average method); CVR = content validity ratio (based on Lawshe’s formula); Item difficulty index = proportion of correct responses per item; Discrimination index (D) = proportion correct difference between upper and lower 27% of scorers; KR-20 = Kuder-Richardson Formula 20.
The percentage of students answering each item correctly ranged from 32.37% (Item 6) to 61.35% (Item 13). Items 4, 11, and 13 had the highest proportion of correct responses (>55%), while Items 3, 6, 12, and 14 were the most challenging (<36%). The final tool consisted of 14 items, and responses were scored dichotomously (1 for correct, 0 for incorrect or no response), yielding a possible total score ranging from 0 to 14, with higher scores representing greater knowledge. Overall, the mean total knowledge score was 6.05 (SD = 3.43) out of a maximum of 14, reflecting limited knowledge of acute rheumatic fever and rheumatic heart disease among schoolchildren. The detailed items are provided as Supplemental File 1 (Figure 1).

Proportion of correct responses for each item of the RHD knowledge scale (n = 207).
Pearson correlation analysis showed that knowledge scores were positively correlated with age (r = .16, P = .022) and grade (r = .23, P = .001), indicating that older students and those in higher grades tended to have greater knowledge (Table 3).
Correlations Between Age, Grade, and Knowledge Scores.

Pearson correlation significant at the .01 level (2-tailed), *significant at the .05 level (2-tailed).
Group comparisons further supported known-groups validity. Knowledge scores differed significantly by grade (F = 5.71, P = .004), with post-hoc analysis confirming higher scores among Grade 9 students compared to Grade 6. Scores were also significantly higher among students previously enrolled in an RHD screening program compared to those without prior exposure (6.54 ± 3.44 vs 4.98 ± 3.16, t = 3.11, P = .002). No significant differences in knowledge were observed by gender or parental education (Table 4).
Comparison of Knowledge Scores by Demographic and RHD Exposure Characteristics.
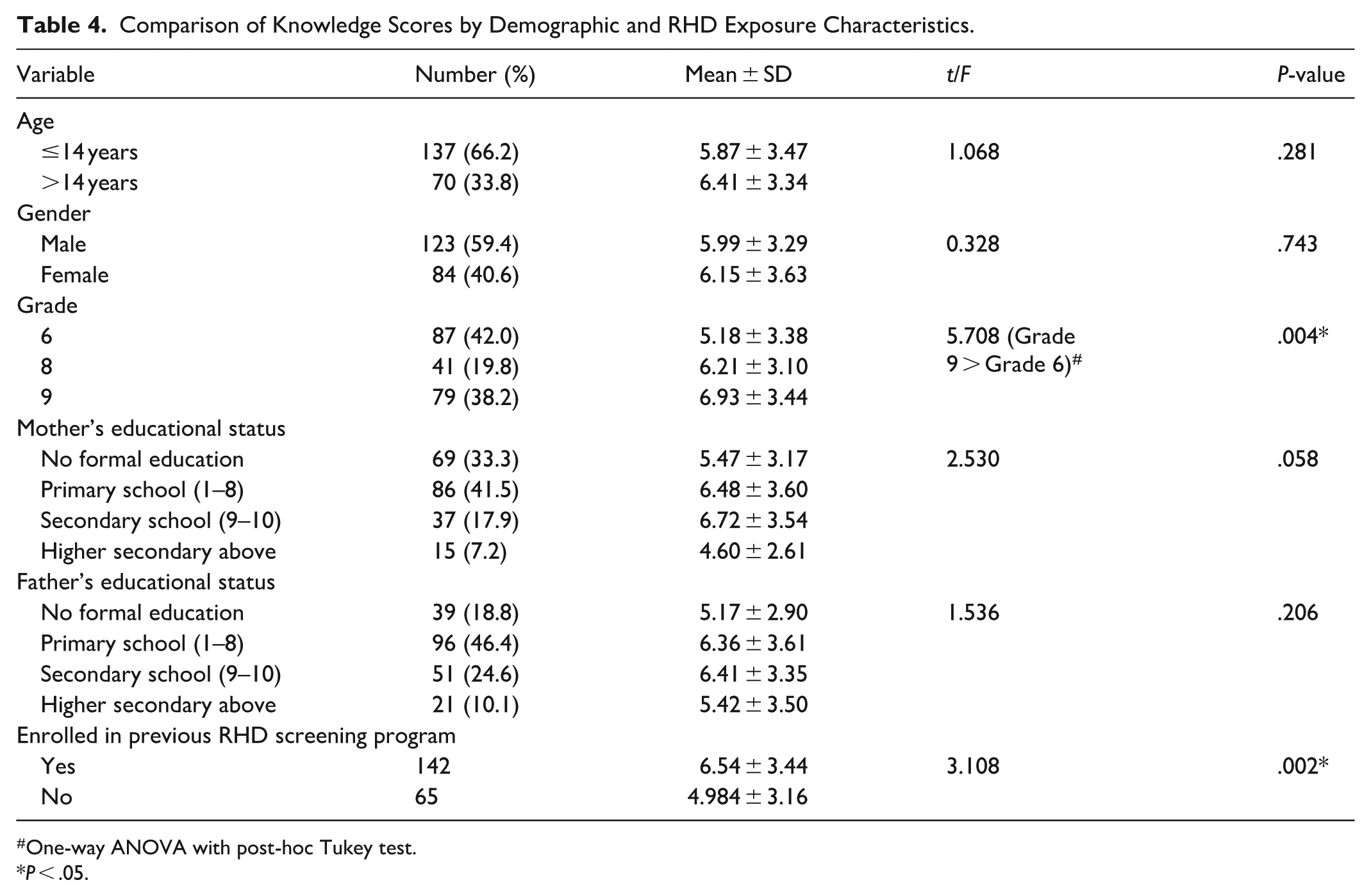
One-way ANOVA with post-hoc Tukey test.
P < .05.
Discussion
This study presents the development and preliminary validation of a 14-item tool designed to assess children’s knowledge of ARF and RHD in Nepal. The findings demonstrate that the scale has strong content validity (S-CVI/Ave = 0.91) and acceptable reliability (KR-20 = 0.772), supporting its utility as a standardized instrument for measuring RHD-related knowledge among school-aged children.
Globally, several studies have assessed ARF and RHD knowledge across diverse populations using self-developed or adapted tools. For example, studies conducted in Uganda, Egypt, Ethiopia, and Saudi Arabia have reported varying knowledge levels, with only 21% to 44% of respondents demonstrating satisfactory understanding of RHD causes, prevention, and treatment.7,8,10,28 However, these instruments were without formal validation or reporting of psychometric indicators such as content validity indices, reliability coefficients, or item discrimination parameters. Although these studies generated valuable descriptive data, the lack of validated instruments limits comparability and generalizability. In contrast, the present study systematically applied a structured, evidence-based scale-development framework, addressing this methodological limitation and offering a psychometrically sound instrument. The mean knowledge score of 6.05 (SD = 3.43) out of a potential 14 points reflects moderate awareness among participants. This finding aligns with existing literature in Nepal, where community-level knowledge of ARF and RHD remains notably low. For instance, Regmi et al reported that overall knowledge regarding ARF and RHD was low, as only 3.1% of participants had good knowledge, which increased to 17.6% following an educational intervention, with misconceptions prevalent about risk factors and prevention. 17 Similarly, Bhatt et al documented that even healthcare providers in rural settings exhibited limited baseline knowledge (9.98 ± 2.4), which improved significantly following targeted educational interventions (13.78 ± 1.9). 13 However, the tools used in these studies were designed for adults and healthcare workers and contained complex content, such as the natural history of rheumatic fever, drug regimens, and advanced clinical presentations, making them unsuitable for children. The lower scores observed in our school-aged population are expected, given their age and lack of prior exposure to health education campaigns.
Importantly, students who had participated in previous RHD screening activities scored significantly higher than their peers, providing evidence of the tool’s ability to distinguish between groups with differing knowledge levels and highlighting the value of repeated school-based engagement. Collectively, these findings underscore the persistent gap in RHD awareness across multiple levels of the health system, from community members to students to frontline providers. Addressing these gaps through targeted educational interventions in schools may be critical to breaking the cycle of undiagnosed streptococcal infections and preventing progression to RHD.
Content validity is a cornerstone of instrument development, ensuring that the tool adequately covers all relevant domains of the construct being measured. In this study, 10 subject matter experts evaluated each item based on relevance, clarity, and appropriateness. The I-CVI ranged from 0.70 to 1.00 for relevance, 0.80 to 1.00 for clarity, and 0.80 to 1.00 for appropriateness. Polit and Beck recommend an I-CVI threshold of ≥0.78 when 6 or more experts are involved, indicating that nearly all items in this tool met or exceeded the minimum standard. 29 The overall S-CVI/Ave was 0.91, surpassing the widely accepted benchmark of ≥0.90 for excellent content validity. 29 While the universal agreement method (S-CVI/UA) yielded a lower value of 0.57, this is not uncommon. In addition to CVI, CVR was calculated to evaluate the degree of expert agreement on the essentiality of each item. Following Lawshe’s criteria, a minimum CVR of 0.62 was required for items reviewed by 10 experts. 22 In this study, CVR values ranged from 0.40 to 1.00, with most items meeting or exceeding the recommended threshold. Items with CVR ≥ 0.80 demonstrated very strong agreement and were retained without modification. Two items fell slightly below the threshold, with CVR = 0.40. These were retained after careful qualitative consideration because they addressed areas of critical importance to RHD knowledge. Collectively, these findings confirm that the tool comprehensively addresses the essential concepts related to ARF and RHD, including symptoms, risk factors, prevention, and treatment.
Item difficulty and discrimination indices were analyzed to evaluate how effectively each question distinguished between students with high and low knowledge. Item difficulty represents the proportion of participants answering each question correctly, with an ideal range of 0.30 to 0.70 recommended for knowledge tests.26,30 Most items in the RHD Knowledge Scale fell within this range, indicating appropriate difficulty as items below 0.30 were considered too difficult, while those above 0.70 were too easy and may warrant future revision. 31 In this study, all items were within the ideal range. The discrimination index (D) assesses an item’s ability to differentiate between high and low scorers. Following classical test theory, discrimination is considered poor if D < 0.15, good if between 0.15 and 0.24, and excellent if ≥0.25.26,30 In this study, the minimum observed D was 0.23, while most items exceeded 0.25, indicating that nearly all questions effectively distinguished between varying levels of student knowledge. This demonstrates that nearly all items effectively distinguished between varying knowledge levels among students, supporting the appropriateness of the final 14-item structure.
Internal consistency reliability was evaluated using the Kuder-Richardson Formula 20 (KR-20), which is specifically suited for dichotomous response formats such as multiple-choice questions. Cronbach’s alpha and KR-20 are mathematically equivalent for binary data, making KR-20 the preferred metric for this tool.30,32 A reliability coefficient of 0.70 or higher is generally considered acceptable for early-stage validation studies. 30 The KR-20 coefficient for the RHD Knowledge Scale was 0.772, demonstrating good internal consistency and exceeding the minimum threshold. This suggests that the items collectively measure a coherent construct while allowing for some variation in knowledge levels among participants. Knowledge tests typically yield slightly lower inter-item correlations than attitudinal or behavioral scales because factual knowledge is more domain-specific.19,33 When compared to established psychometric benchmarks, the performance of the RHD Knowledge Scale was favorable. The high S-CVI/Ave and I-CVI values confirm strong expert agreement on the relevance and clarity of the tool. The KR-20 coefficient exceeded the minimum acceptable standard, while the item difficulty and discrimination indices were within ideal ranges. Together, these results demonstrate that the tool is psychometrically sound and appropriate for use in both research and public health program evaluation.
While exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) are commonly employed in psychometric studies to examine underlying constructs, their applicability in knowledge-based instruments is limited. Knowledge-based instruments often involve assessing factual knowledge or skills that have a clear, objective scoring system rather than latent constructs, which reduces the relevance of EFA and CFA.34 -36 The RHD Knowledge Scale was specifically developed to measure a single construct of children’s factual knowledge of ARF and RHD, using multiple-choice questions with dichotomous (correct/incorrect) scoring. Unlike Likert-type scales that capture subjective perceptions or attitudes, knowledge tools focus on objective recall. Inter-item correlations in such tools are often low and do not necessarily represents latent factors. Although EFA and CFA can technically be applied using tetrachoric correlation matrices, their interpretive value is limited and may lead to misleading conclusions.36,37 For this reason, the current study prioritized, including KR-20 and item-level indices, which are more suitable and widely recommended for the validation of knowledge assessments. 27
The scale’s ability to detect differences between predefined groups provides evidence of construct validity. In this study, older students and those in higher grades scored significantly higher than younger students, consistent with the expectation that knowledge increases with age and educational exposure. Similarly, students who had previously participated in RHD screening programs scored higher than those without prior exposure. This pattern aligns with findings from Bhatt et al, who observed improvements in RHD knowledge following targeted educational interventions. 13 As knowledge scores were significantly higher among students with prior RHD screening exposure and those in higher grades, this further supports the tool’s known-groups validity and its sensitivity to detecting differences based on prior exposure and educational level.
Beyond its psychometric strengths, the RHD Knowledge Scale has important public health implications and fills a critical gap in child-specific ARF and RHD measurement. It provides a standardized, validated instrument for assessing children’s understanding of ARF and RHD, which can be integrated into school health programs to establish baseline knowledge, track changes over time, and monitor the effectiveness of school-based awareness campaigns. By systematically identifying districts and populations where knowledge gaps remain, the tool can guide resource allocation and inform national strategies for prevention. In the future, the RHD Knowledge Scale could be digitally adapted for large-scale, real-time data collection, enhancing accessibility in resource-limited settings. Aligning the tool with the World Health Organization’s school-health framework could further strengthen its integration into global and national child health initiatives, promoting sustainable RHD prevention through early education. Future studies should focus on validating the RHD Knowledge Scale in other geographic, linguistic, and cultural contexts, assessing its predictive validity, and exploring its adaptation for older adolescents or adults. Multisite studies could also test its applicability for longitudinal tracking or integration with other health promotion programs.
Despite being one of the few studies to develop and validate a child-specific RHD knowledge tool, several limitations must be acknowledged. First, it was conducted in a single municipality and included only public schools, which may limit generalizability to private school settings or other regions of Nepal. Because only 3 public schools were included, the findings may not fully capture variations in knowledge across different types of schools or geographic areas. Second, although the sample size adhered to established psychometric recommendations, a formal sample size or power calculation was not performed. While the achieved sample size of 207 exceeded recommended thresholds for validation studies, the absence of a formal power analysis should be considered a methodological limitation. Additionally, although the tool demonstrated good internal consistency, we were unable to assess test-retest reliability due to logistical challenges. Shortly after baseline data collection, the participating schools were enrolled in another RHD-related project from other organizations, which could have exposed students to educational materials and confounded repeated measurements. Future research should include test–retest reliability assessments to evaluate the temporal stability of the RHD Knowledge Scale and may also employ advanced psychometric approaches such as item-response theory or tetrachoric correlation analyses to further strengthen the tool’s validity evidence. Finally, while the scale captures essential factual knowledge, it does not assess attitudes or practices, which are also important determinants of health behavior.
Conclusion
The RHD Knowledge Scale demonstrated strong content validity, with both CVI and CVR values meeting established psychometric thresholds, and good internal consistency (KR-20 = 0.772). Item-level analyses indicated that all questions fell within the ideal range for difficulty and discrimination, supporting their appropriateness for differentiating varying levels of knowledge. This tool fills a critical gap by providing a standardized measure to evaluate children’s understanding of ARF and RHD, which is essential for monitoring the effectiveness of school-based interventions and informing national prevention strategies. Beyond the national context, the RHD Knowledge Scale also holds potential for adaptation and validation in other countries and linguistic populations, thereby facilitating cross-cultural comparisons and strengthening global RHD prevention efforts.
Supplemental Material
sj-doc-1-inq-10.1177_00469580251405997 – Supplemental material for Measuring Children’s Knowledge of Acute Rheumatic Fever and Rheumatic Heart Disease: Development and Validation of RHD Knowledge Scale in Nepal
Supplemental material, sj-doc-1-inq-10.1177_00469580251405997 for Measuring Children’s Knowledge of Acute Rheumatic Fever and Rheumatic Heart Disease: Development and Validation of RHD Knowledge Scale in Nepal by Sandeepa Karki, Shishir Paudel, Rudra Prakash Hada, Prashant Khadka, Ganesh Shetty, Dhurba Khatri, Yamuna Chhetri, Sakar Khanal and Bhagawan Koirala in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We would like to express our heartfelt gratitude to all the schools, students, and parents for their generous cooperation and unwavering support throughout the course of this study. We are especially thankful to our experts Dr Saurav Shrestha, Dr Saurav Singh, Dr Kunjan Sherpa, Dr Urmila Shakya, Dr Dipankar Prajapati, for their constant support and expert opinion.
Ethical Considerations
Ethical approval for the Colours to Save Heart project has been obtained from the Institutional Review Board of the Nepal Health Research Council (REF: 2678, Protocol No: 152_2025). Permission was acquired from each selected school.
Consent to Participate
Written informed consent was obtained from parents, and written assent was provided by all participating students. Separate consent and assent were also obtained for students who participated in cognitive interviews.
Consent for Publication
The author consents to the publication of this manuscript in this journal.
Author Contributions
SK: conceptualization, tool development, project administration, fund acquisition, validation, methodology, and writing–review and editing. SP: conceptualization, tool development, project administration, data analysis, investigation, methodology, visualization, validation, and writing–original draft, writing–review and editing. RPH: tool development, visualization, and writing–review and editing. PK: data curation, investigation, writing–review and editing. GS: data curation, investigation, writing–review and editing. DK: visualization, tool development, writing–review and editing. YC: investigation, writing–review and editing. SakK: writing–review and editing. BK: Supervision, writing–review and editing. SK and SP shared equal contribution as lead authors for this manuscript. All the author have read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All relevant data are within the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.