
Abstract
In Nepal, community pharmacies serve as the primary source of medical care. The aim of the current study was to evaluate the effect of an educational intervention on knowledge and practice of dispensing, prescription handling and patient counseling among community pharmacists working in 3 districts (Kathmandu, Lalitpur and Bhaktapur) of Nepal. A quasi-experimental pre–post interventional study was conducted in 123 community pharmacies located in Kathmandu, Bhaktapur, and Lalitpur districts of Nepal. The research questionnaire was developed according to national and international good pharmacy practice guidelines. A structured questionnaire with mainly closed-ended and a few open-ended questions, exploring the knowledge and practice of community pharmacists in the 3 areas mentioned previously was prepared. Demographic information was also collected. The pre-tested questionnaires were completed by the community pharmacy in charge from the selected pharmacy. This data was considered as the pre-intervention data. Education sessions on good pharmacy practice were provided to all selected community pharmacists by expert pharmacists. Three weeks following the educational intervention, post-intervention data was collected at the same pharmacies. The percentage of pharmacies chosen were Kathmandu (48.8%), Lalitpur (30.9%), and Bhaktapur (20.3%). Seventy-four percent of respondents were Diploma in Pharmacy, 21.1% were bachelor’s in pharmacy. The major problems faced by the pharmacists during dispensing were inadequate instructions (30.1%), followed by missing duration of therapy (24.4%) and unavailable drugs
Introduction
In Nepal, community pharmacists are the most accessible healthcare providers, acting as the first point of contact for patients due to their widespread presence, flexible hours, and lack of consultation fees. A “community pharmacy” is also known as a retail pharmacy in Nepal or as a medical shop or store (Aushadhipashal). These terms are used synonymously, with the general population preferring the terms, medical shop or store. After registering with the Department of Drug Administration (DDA), pharmacists, assistant pharmacists, and other pharmacy professionals are permitted to work in community pharmacies in accordance with the Drug Act of 1978. 1 Pharmacists includes those who have completed Bachelor of Pharmacy (BPharm) or higher degrees (eg, MPharm, PharmD); they are fully licensed professionals with comprehensive training in pharmaceutical sciences, clinical pharmacy, and community practice. An Assistant Pharmacist includes those who have completed a Diploma in Pharmacy (DPharm), a 3-year program conducted after completing secondary education (10 years of schooling). Pharmacy professionals are a broader umbrella term that encompasses all categories of registered pharmacy personnel, recognized under the Drug Act. In 1992, the International Pharmaceutical Federation (FIP) created standards for good pharmacy practice in community and hospital pharmacy settings. The goals of good pharmacy practice are to improve patient self-care, supply medications, promote health, and improve pharmacist dispensing and medication usage. 2 In the context of Nepal, the implementation of GPP is particularly important because community pharmacies often serve as the first point of contact for patients seeking healthcare. With limited physician access in rural areas, pharmacy professionals frequently function as primary healthcare providers. However, challenges such as inadequate enforcement of GPP standards, variation in qualifications among practitioners, and widespread irrational dispensing practices continue to affect the quality of pharmacy service delivery.
The country’s health system is pluralistic, public facilities deliver primary care while a growing private sector (including retail pharmacies) supplies much of outpatient services, especially in urban areas. Although professional codes and regulatory frameworks promote separation of prescribing and dispensing, dispensing separation is inconsistently implemented: community pharmacies commonly supply medicines (including antibiotics) without prescriptions, and many outlets are staffed by personnel without formal pharmacist qualifications. 3 A study done in western Nepal showed that community pharmacists dispensed nearly two-thirds of medicines without a prescription. Commonly administered injections included Tetanus Toxoid, Depot-Medroxy Progesterone Acetate, and Diclofenac. Antibiotics were frequently dispensed without prescription, often by non-pharmacists, highlighting widespread irrational practices. 4 This creates both challenges (quality and antimicrobial stewardship) and opportunities: with better regulation, training, and integration into public health programs, community pharmacies could play a major role in expanding access, rational medicine use, and chronic disease management. 3
Pharmacy education in Nepal focuses heavily on theory and may lead to significant gaps in clinical skills, communication, and direct patient care, which are essential for effective pharmacy practice in hospitals and communities. Many pharmacies are operated or managed by non-pharmacists or pharmacy assistants with limited clinical training, restricting the scope and quality of pharmaceutical care. 5 The limited availability and uptake of continuous pharmacy education (CPE) hinders pharmacists’ ability to adapt to evolving healthcare standards and patient needs. Everyday pharmacy practice needs further strengthening to ensure optimal public health protection and professional service delivery. 6 The public visit pharmacies for various medical issues, such as checking blood pressure, injections, skin diseases, diarrhea, fever, and contraception. Since they can deliver medications and health advice on a walk-in basis without an appointment, pharmacies are regarded as affordable and accessible to the general people. 7 Nonetheless, community pharmacies in Nepal may have subpar pharmacy practices. Poor knowledge and reduced compliance with dispensing and counseling norms may be characteristics of practice. Dispensing plays a crucial role in the process of using medications. Commonly assessed factors for evaluating dispensing practices include the average time taken for dispensing, the proportion of medications that are properly labeled, and the extent to which patients understand the correct dosage. 8
Community pharmacy-based education interventions have improved knowledge, attitude and practice. Education is the most common approach employed to enhance the professional practices of pharmacists globally. 9 Educational interventions that incorporate interactive methods, role-playing, and feedback can enhance pharmacists’ confidence to apply newly learned skills in practice leading to sustainable improvements in professional practice and service delivery. A few educational interventions have been previously done among community pharmacists in Nepal. In Lalitpur district, Nepal knowledge and attitude scores toward pharmacovigilance and consumer pharmacovigilance improved after an educational intervention. 10 In the Kathmandu valley, Nepal total knowledge, attitude and practice (KAP) scores improved significantly among different subgroups of community pharmacists after an educational intervention. This was retained during follow-up. Participants perceived the intervention program to be useful. 11 A recent article highlighted the need for GPP implementation, identified key challenges, and outlined the potential opportunities. 12
This study aims to assess whether an educational intervention can improve knowledge and practice about dispensing practices and patient counseling among community pharmacists (pharmacy in charges) working in the studied community pharmacists. The knowledge and practice scores of community pharmacists before and 3 weeks after participating in the educational intervention were measured, exploring the effect of the intervention across different subgroups.
Methodology
Study Design
A quasi-experimental pre–post interventional study was conducted in community pharmacies located in Kathmandu, Bhaktapur, and Lalitpur districts of Nepal to assess community pharmacists’ dispensing knowledge and practice. Knowledge and practice in this pre-post-education intervention study was measured at 2 points, before and 3 weeks following an educational intervention. The study was done from November 2023 to February 2024 after obtaining ethical approval.
Sampling Method
Nepal was divided into 7 provinces after the country officially adopted a federal democratic republic system in 2015. We selected Kathmandu, Lalitpur and Bhaktapur districts of Bagmati province.
In this study, convenience sampling was used to select 1 in every 3 community pharmacies located in the vicinity of government and private hospitals. A complete list of all community pharmacies operating in the vicinity (approximately within a 2-km radius) of selected government and private hospitals (eg, Bir Hospital, Civil Hospital, Teaching Hospital, Alka Hospital etc.) was obtained from the Department of Drug Administration (DDA) 2021 report. This process was conducted separately for pharmacies located in Kathmandu, Lalitpur, and Bhaktapur districts to ensure proportional representation across the districts. A total of 123 community pharmacies were selected.
Slovin’s formula was used for sample size determination. It is commonly applied in survey research when the population size is known. 13 The minimum sample size(n) of this study was 100 pharmacies, it was determined by using the equation: n = N/1 + N(e)2, where N is the study population, which was 4913 pharmacies, and (e) an error margin of 0.1. The formula is based on a degree of variability of P = .5, and a 95% confidence interval.
The number of community pharmacies in the 3 districts as per the Department of Drug Administration [DDA] report is shown below.

Inclusion Criteria
The study covered the community pharmacies located around the vicinity of selected government and private hospitals in the districts of Kathmandu, Lalitpur, and Bhaktapur.
The Pharmacist Supervisor / Pharmacy In-charge who was registered with Nepal Pharmacy Council was included in the study. These persons held qualifications that could be registered. The “Pharmacist Supervisor” or “pharmacy in-charge” is the lead professional in the pharmacy who carries both supervisory authority and accountability for pharmacy service delivery.
Exclusion Criteria
The wholesale pharmacies, hospital pharmacies, ayurvedic medical shops and nursing homes was excluded from the study.
Drug seller who has obtained qualification of Certified Medical Assistant (CMA) and Health Assistant (HA) were excluded as there was no provision for their registration with the Nepal Pharmacy Council A CMA is a mid-level health worker in Nepal who has completed a 15-month training program after the School Leaving Certificate (SLC)/ Secondary Education Examination (SEE). An HA is a more advanced mid-level health professional who has completed a 3-year Proficiency Certificate Level (PCL) in General Medicine after the SLC/ SEE.
Informed Consent
Written informed consent was taken from each pharmacy in charge included in the study.
Study Instrument
The research questionnaire was developed by studying good pharmacy practice (GPP) guidelines in Nepal, and the Joint FIP/WHO GPP guidelines.1,14 A structured questionnaire containing closed-ended and a few open-ended questions was prepared. It comprises the pharmacists’ sociodemographic traits and their knowledge and practice in counseling, prescription handling, and dispensing. The survey was created in both Nepali and English language.
The researchers revised the questionnaire and evaluated its content validity by obtaining the opinion of 4 senior pharmacists who were experts on good pharmacy practices in Nepal and had several decades of experiences in the pharmacy field.
Two were officers at the Department of Drug Administration with a deep understanding of the regulatory aspects of pharmacy. The other 2 were academic pharmacists who each had more than a decade of academic experience in research and teaching on community pharmacy, which involves the provision of pharmaceutical care to patients in a community setting.
The questionnaire consisted of 73 questions. It had 4 parts; the first part consisted of 9 questions regarding sociodemographic characteristics. The second part comprised 19 questions about the knowledge among community pharmacists on dispensing practice and prescription handling. Of the 19 questions, 17 were closed-ended questions in which 1 question [Question number 5] was reverse-coded [maximum total score of 80] and 2 were open-ended questions The third part contained 19 questions regarding practice of community pharmacies in dispensing and counseling patients, among which 16 were closed-ended questions while 3 were open-ended questions [maximum total score of 80]. The knowledge and practice responses in the second and third section were on a 5-point Likert Scale: 5 = always, 4 = often, 3 = sometimes, 2 = rarely and 1 = never. The fourth part consisted of 7 questions assessing prescription-related problems faced by community pharmacists.
Reliability of the Study Questionnaires
A pre-test study was conducted on 10 pharmacists to ensure the clarity and appropriateness of the questions. The data from the pretest were not included in the final study. Ten community pharmacists, 3 from Lalitpur, 3 from Bhaktapur, and 4 from Kathmandu were randomly selected. The internal consistency of the questionnaire was evaluated using Cronbach’s alpha. The Knowledge questions showed Cronbach’s alpha .78 and the Practice question showed Cronbach’s alpha .71 which indicates acceptable reliability.
Data Collection Procedure
The validated questionnaire was administered among 123 community pharmacists by the first author. The pharmacist supervisor/ Pharmacy-In charge was chosen for the study. This information was utilized as pre-intervention or baseline data and served as the basis for the development of the educational intervention package. All the chosen community pharmacists from Nepal’s 3 districts were invited to an educational session. Expert pharmacists conducted education and training sessions on appropriate pharmacy practices. PowerPoint and other media were used as teaching aids. To spread knowledge about GPP, educational posters were also on display. The session lasted roughly 2 h. Senior pharmacists, recognized as experts in Good Pharmacy Practices (GPP) in Nepal, with several decades of professional experience and significant contributions to the pharmacy field, were selected to deliver the training.
For the post data collected after the intervention, the same pharmacists completed the questionnaire during visits to their pharmacies 3 weeks following the educational program, using the identical method as applied for the pre-intervention data. Knowledge and practices were evaluated 3 weeks post-educational intervention.
Educational Intervention
The educational workshop was held in 2 sessions on consecutive days, Friday, November 25, 2024, and Saturday, November 26, 2024. Saturday is the weekly off in Nepal. Each session was led by 4 senior pharmacy experts and took place in 2 separate seminar halls in Kathmandu. Participants were divided into 2 groups, with each group attending 1 workshop. Attendance was recorded for all participants. Two students enrolled in the diploma in pharmacy program but could not attend the training, so they withdrew from the study. Each session lasted 2 to 3 h and included PowerPoint presentations, videos, and scenarios. WHO guidelines and Nepal GPP guidelines were used to extract the content for educational training. The prepared contents were peer-review and verified by 4 pharmacy experts, then modified and final contents were prepared and delivered to participants.
The presentations covered: (1) the basic concept of good pharmacy practice and principles of dispensing, (2) prescription handling, (3) patient counseling, and (4) pharmacists’ role in overcoming barriers related to counseling. An informational leaflet containing key pharmacy practice guidelines was provided to the pharmacists through a closed group and discussed during the first workshop session. The training concluded with interactive group sessions, discussions, Q&A, and feedback. Additional feedback was solicited from participants regarding the practical application of the workshop and the extent of patient care provided as part of the practice.
Data Analysis
Descriptive quantitative analytical statistics were done in Ms. Excel 2013 and SPSS version 25. A P-value of <.05 was set as a measure of statistical significance. The normality of distribution of the scores was compared using the Kolmogorov-Smirnov test. Appropriate statistical tests to compare the average scores were chosen based on the normality of distribution of the scores. The scores before and after the educational intervention were compared using the Wilcoxon signed-rank test. Paired samples t-test used to compare pre- and post-intervention scores across the districts (Kathmandu, Bhaktapur, Lalitpur), age groups (15-25, 26-35, 36-45, 46-55 years), educational qualifications (DPharm, BPharm, MPharm) and to assess whether the average improvement in knowledge and practice scores was statistically significant. Pearson correlation was conducted to examine the relationships among knowledge and practice scores at pre- and post-test phases.
Ethical Approval
Approval was obtained from the Nepal Health Research Council [NHRC] with reference No. 895.
Result
Distribution of Sample
A total of 144 community pharmacists were approached. Of these, 123 pharmacists participated in the study, so the response rate was 85%. However, 21 dropped out of the study. The primary reasons for dropout were that 10 participants had only completed an orientation training program, and thus were not eligible to complete the survey, while 9 were holders of a Health Assistant (HA) degree and did not meet the inclusion criteria. The remaining 2 held diploma in pharmacy qualification but could not attend the educational training, so they withdrew from the study
Kathmandu District: Sixty community pharmacy in charges were from this district, accounting for 48.8% of the total sample. This indicates that almost half of the study’s subjects were located in Kathmandu. Lalitpur District: Represented by 38 participants, this district constituted 30.9% of the total. This signifies a substantial portion of the sample came from Lalitpur. Bhaktapur District: With 25 participants, Bhaktapur had the smallest representation, making up 20.3% of the total sample. This was proportional to the number of community pharmacies in the 3 districts. It was illustrated in Figure 1.

Geographical distribution of sample.
Demographic Characteristics of the Respondents (n = 123)
Out of the total 123 community pharmacists who participated, 61% were male (n = 75), while 39% were female. The age distribution showed that the highest proportion (56%) was in the 26 to 35 years age group, followed by the 18 to 25 age group at 21%. Additionally, most respondents reported having 1 to 5 years of experience as community pharmacists in the 3 districts. Table 1 shows the demographic characteristics of the respondents. Among 123 participants, the majority held a Diploma in Pharmacy (D. Pharm) degree (n = 89; 72.4%), followed by Bachelor in Pharmacy (B. Pharm) graduates (n = 26; 21.1%) and Master in Pharmacy (M. Pharm) graduates (n = 8; 6.5%).
Demographic Characteristics of the Respondents [N = 123].

Qualification Based Knowledge and Practice
Difference in knowledge and practice scores among community pharmacists on dispensing and counseling before (pre-test) and following an educational intervention (post-test) was explored by Wilcoxon signed-rank test (P < .05).
Knowledge Scores
Among DPharm pharmacists (n = 89), there was a statistically significant increase in knowledge scores from pre-test (M = 69.4) to post-test (M = 76.6), P < .001. Similarly, BPharm pharmacists (n = 26) demonstrated a significant improvement from pre-test (M = 68.9) to post-test (M = 76.6), P < .001. MPharm pharmacists (n = 8) also showed a significant increase from pre-test (M = 65.5) to post-test scores (M = 66.3), P < .005. These findings suggest that the intervention was effective in enhancing knowledge across all qualification groups. Table 2 shows the pre- and post-test knowledge scores by qualification.
Pre- and Post-Test Knowledge and Practice Scores by Qualification.

Note. Means (M) represent knowledge scores before and after intervention. Wilcoxon signed-rank test was used. P < .001 shows statistically significant.
Practice Scores
For practice outcomes, DPharm pharmacists (n = 89) showed a significant increase in scores from pre-test (M = 68.6) to post-test (M = 77.2), P < .001. BPharm pharmacists (n = 26) also demonstrated a significant improvement from pre-test (M = 65.5) to post-test (M = 66.3), P < .001. Likewise, MPharm pharmacists (n = 8) showed a significant improvement in practice scores from pre-test (M = 66.3) to post-test (M = 74.6), P = .019.
Overall, the Wilcoxon signed-rank test results indicate that the educational intervention had a significant positive impact on both knowledge and practice scores among pharmacists, irrespective of their qualification level. Table 2 shows the pre- and post-test practice scores by qualification.
Knowledge and Practice Scores Among Males and Females
The Wilcoxon signed-rank test revealed statistically significant improvements in both knowledge and practice scores among male and female pharmacists after the educational intervention.
Male pharmacists: Knowledge scores increased from 68.2 (pre-test) to 76.6 (post-test), P < .001. Practice scores improved from 66.6 (pre-test) to 76.4 (post-test), P < .001. This indicates a significant positive effect of the intervention on both knowledge and practice among males.
Female pharmacists: Knowledge scores increased from 70.3 (pre-test) to 76.7 (post-test), P < .001. Practice scores improved from 69.8 (pre-test) to 77.7 (post-test), P < .001. This also shows a significant positive effect of the intervention among females. Female pharmacists had slightly higher baseline knowledge and practice scores compared to males. However, both genders demonstrated similar improvements following the intervention, reaching comparable post-test scores. This suggests that the intervention was equally effective across genders in enhancing both knowledge and practice (Table 3).
Mean Pre- and Post-Test Knowledge and Practice Scores by Gender.

Note. Means (M) represent pre- and post-test scores of pharmacists’ knowledge and practice by gender. Wilcoxon signed-rank test was used. P < .001 shows statistically significant.
Correlation Between Knowledge and Practice (Pre-Testing and Post-Testing)
Pearson correlation was used to examine the relationship among knowledge and practice scores at pre- and post-testing. There was a positive correlation between knowledge and practice: as pharmacists’ knowledge scores increase, their practice scores also tend to improve. However, the relationship is moderate (since R² = 0.214, not very high). This suggests that participants with higher knowledge are more likely to demonstrate better practice. Correlation between knowledge and practice (pre-testing and post-testing) was illustrated in Figure 2

Correlation between knowledge and practice (pre-testing and post-testing).
Problems Pharmacists Face While Dispensing a Prescription
The study assessed the common prescription-related problems as perceived by the respondents. Among them, inadequate instruction was the most frequently reported issue, with 30.1% identifying its presence, while 26.8% did not observe it, and 43.1% were unsure. Unavailable drugs were noted in 22.0% of cases, whereas 25.2% did not encounter this problem, and 52.8% were uncertain. Similarly, missing duration of therapy was reported in 24.4% of prescriptions. This was shown in Table 3. Other issues included pharmaceutical dosage form errors (15.4%), illegible prescriptions (13.0%), dosing errors (13.0%), and drug interactions (13.0%). For all of these, a significant proportion of respondents reported “not sure” with values ranging from 35.0% to 62.0%. Notably, dosing errors had the highest uncertainty (62.0%), suggesting challenges in identifying such problems during routine practice. Table 4 shows the problems faced by pharmacists while dispensing prescriptions.
Prescription-Related Problems Reported by Respondents (N = 123).
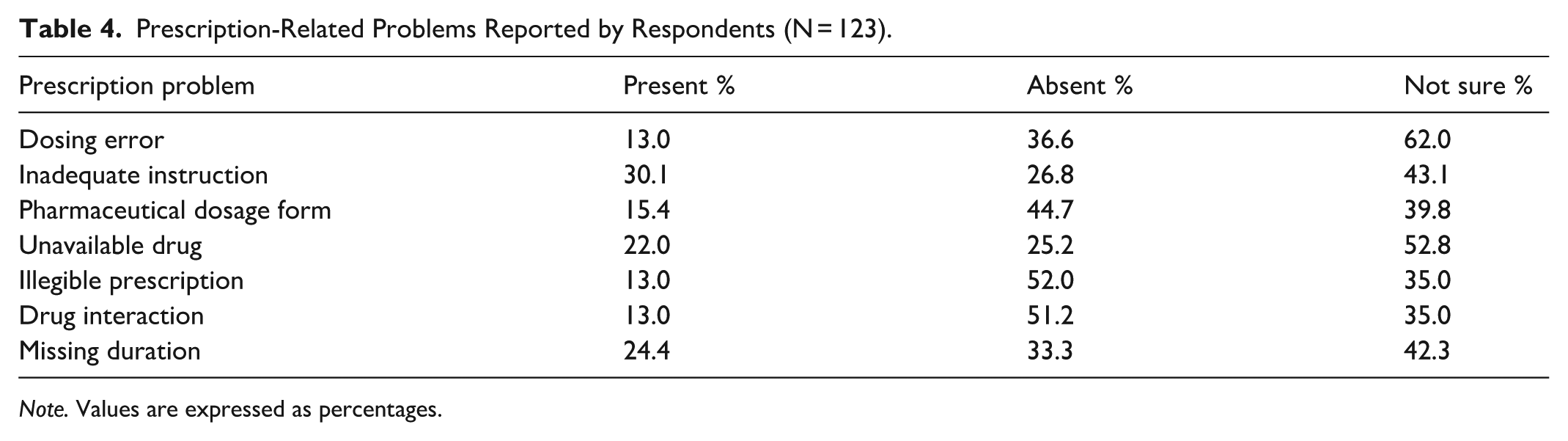
Note. Values are expressed as percentages.
Discussion
Good Pharmacy Practice (GPP) is a fundamental concept that lies at the very heart of the pharmacy profession. It represents a commitment to patients to not only “do no harm” but also to facilitate positive therapeutic outcomes through the responsible provision of drug therapy. 15
Demographic Characteristics of the Respondents
The present study included community pharmacists from 3 major districts of Nepal. As per gender distribution, our data showed that 61% (75 participants) are male and 39% (48 participants) are female. This distribution aligns closely with findings from some other studies in developing countries. For example, a study on pharmacovigilance among community pharmacists in Lalitpur District, Nepal, reported a similar gender distribution, with 60% male respondents and 40% female respondents. 10 In contrast, a study of community pharmacists in Turkey found that the majority were female (79.2%). 16 Similarly, in Moldova, 86.5% of surveyed pharmacists were female. This suggests that the gender composition of pharmacy workforces can vary significantly by region or country, even within similar economic development stages. 17
The age profile of the participants indicates a predominantly young to middle-aged workforce, with the largest group being 26 to 35 years old (56% or 70 participants). This demographic trend was observed in several studies. In Pakistan, the average age of pharmacy attendants was between 21 and 30 years (43.67%), which is consistent with our findings. 18 A study in Oman found that almost half (49.1%) of the pharmacists were in the 25 to 30 years age group. Similarly, most participants in a study of chain pharmacists in Indonesia were novice pharmacists under 30 years old. 19 This suggests that while a young workforce may bring enthusiasm for new practices, it also necessitates continuous professional development to prevent early career dissatisfaction and maintain competence. The high proportion of younger professionals in our data suggests a potential for adaptability to evolving pharmacy practices, given appropriate training and support.
The qualification breakdown reveals that the majority of personnel (74% or 91 individuals) held a Diploma in Pharmacy, while a smaller proportion have a Bachelor’s (21.1% or 26 individuals) or Master (6.5% or 8 individuals) degrees. 12 In Hetauda, Nepal, a significant portion (51.2%) of pharmacy in-charges had diverse qualifications like CMA, HA (Healthcare Assistants), and others. 20 The low representation of B. Pharm and M. Pharm graduates is consistent with findings in Pakistan, where only 9.49% of pharmacy attendants had professional pharmacy education. 21 There was a study surveying 246 community pharmacy personnel in eastern Nepal (Jhapa, Morang, Sunsari districts) about their education and experience: only 6.5% of respondents held a graduate-level pharmacy degree. The rest were certificate-level pharmacists (42.7%), and “others paramedics” or non-graduate pharmacy-qualified personnel (50.8%). 22 Overall implications for Pharmacy Practice states that the demographic profile presented suggests a workforce that is young, with a significant proportion holding diploma-level qualifications. This structure often leads to challenges in the implementation of advanced pharmaceutical care services and adherence to GPP guidelines. 2
Scores Before and 3 Weeks After the Educational Intervention
The findings of the study confirm that the education intervention positively affected practice and knowledge scores among the pharmacists regardless of gender. Among male pharmacists, the knowledge and practice scores greatly increased following the intervention. Similarly, the female pharmacists showed equally marked improvements, with higher initial levels of knowledge and practice compared to the males. This implies that while the females had slightly higher knowledge and practice levels at the beginning, both groups of pharmacists improved through the intervention.
The total gains that were demonstrated in this research highlight the effectiveness of guided educational interventions in improving pharmacists’ capability in professional practice. The gains in knowledge are most likely to have resulted in better practice outcomes, as stipulated by the precepts of social learning theory where enhanced understanding directs and supports behavior change. 23 Also, the results underscore the worth of continuous professional development interventions for pharmacists. By delivering recent knowledge and field practice skills, such interventions may ultimately result in improved healthcare delivery. The gender gap observed at baseline might be ascribed to variations in prior exposure, training, or professional experience; however, the sustained post-intervention gains across both groups confirm that successful educational interventions can bridge such gaps efficiently. This aligns with multiple sources that emphasize the effectiveness of educational programs in enhancing healthcare professionals’ knowledge, attitudes, and practices (KAP) in various domains, such as pharmacovigilance, hypertension management, and generic drug substitution. 5 Similarly, an intervention improved knowledge and attitude scores among health professionals in a Nepal cancer hospital. 6 Improved knowledge of pharmacists may also be transferred to patients. A study discovered that a "straightforward educational initiative conducted by community pharmacists enhanced patients’ understanding of the disease, as well as their practices and management of hypertension. 5
Educational interventions could play a transformative role in addressing these gaps. Training programs tailored for community pharmacy staff can improve knowledge of rational prescribing, dispensing, and counseling. Globally, similar interventions have shown success: for example, pharmacist-led educational workshops in Pakistan, India, and several African countries have reduced inappropriate antibiotic dispensing and improved adherence to Good Pharmacy Practice. Adapting such models in Nepal—and sharing lessons across low- and middle-income countries—could help tackle antimicrobial resistance, enhance medicine safety, and strengthen the integration of community pharmacies into broader health systems. In this way, educational interventions not only improve local practice but also contribute to global health priorities such as rational medicine use and antimicrobial stewardship.11,24
The present study found the extent of improvement in knowledge and practice scores varied according to educational qualifications, reflecting both the strengths and weaknesses across different segments of the pharmacy workforce. Diploma in Pharmacy qualified pharmacists demonstrated significant improvement in knowledge and practice following the intervention. This finding is particularly important as Diploma qualifiers typically form the “mainstay of pharmacy practice” in South Asia. 15 Their improvement suggests that training programs can effectively close knowledge and practice gaps for this large workforce category, in turn enhancing service delivery at the community level. Conversely, B Pharm graduates experienced great gains in knowledge but only slight gains in practice, though statistically significant. This finding is echoed from other research, for instance, studies conducted in Indonesia where pharmacists possessed good knowledge and attitudes but only moderate practice. 25 Inconsistencies between self-reported intention and dispensing practice again have been reported, along with persistent struggles to convert knowledge into behavior. For this group, training modules or interventions based on practice to overcome the bottlenecks—such as too much workload, low confidence, or lack of supportive systems—would be needed to ensure that developments in knowledge are incorporated into day-to-day working practices. For MPharm graduates, the intervention achieved only modest gains in knowledge but remarkable practice improvement. This makes sense, since postgraduate pharmacists already possess strong theoretical foundations, and thus there is not much room for enhancing knowledge further. But their remarkable practice improvement emphasizes the value of educational interventions even for trained staff, particularly when they are directed toward practical skills and daily practice.
In general, these findings indicate the importance of personalizing educational interventions based on different levels of qualifications. Though Diploma holders require extensive training to develop both knowledge and practice, BPharm graduates would most likely require interventions that help bring knowledge into practice daily. Meanwhile, for MPharm holders, practice-based interventions remain crucial to developing professional behavior regardless of their thorough preparatory studies. Overall, the educational intervention effectively strengthened community pharmacists’ competencies across multiple dimensions of dispensing and prescription-checking practices. By embedding both clinical and regulatory aspects of pharmacy practice, the program not only improved knowledge but also promoted safer, more rational, and patient-centered care. 26 The positive correlation indicates that improvement in knowledge (through training/education) is likely to enhance practice. Since this is based on pre- and post-test design, the result suggests the educational intervention may have been effective in strengthening the link between what participants know and how they apply it in practice. There is a statistically meaningful, positive correlation between knowledge and practice scores. Higher knowledge is associated with improved practice, and knowledge accounts for around 21% of the variability in practice behavior. This supports the idea that educational interventions can positively influence practice by improving knowledge. Our findings are consistent with previous studies that have reported a positive association between knowledge and practice in healthcare professionals. For instance, Mishore et al found that improved knowledge of antimicrobial stewardship among pharmacists in Ethiopia was significantly associated with better dispensing practices. 27 Educational interventions have been widely reported to enhance both knowledge and practice outcomes. A study by Nguyen et al demonstrated that structured training programs for community pharmacists in Vietnam led to improved counseling practices, which were strongly linked to knowledge gains. 28 This supports the effectiveness of training-based interventions in bridging the knowledge–practice gap. In the context of Nepal, Shrestha and Ghale also emphasized that continuing professional development programs significantly improved pharmacists’ practice behavior, highlighting the importance of sustained educational efforts. 29 Despite the moderate strength of the relationship in the current study, the results underscore the importance of capacity-building interventions. While knowledge is a critical foundation for appropriate pharmacy practice, knowledge alone may not be sufficient to guarantee consistent professional behavior. Factors such as resource availability, workload, patient demands, and policy enforcement may act as mediators of practice performance. Therefore, future interventions should integrate educational training with supportive supervision and regulatory reinforcement to maximize impact.
Problems While Dispensing Prescriptions
The high prevalence of “Inadequate instruction” (30.1% Present) and “Missing duration” (24.4% Present) directly impedes patient compliance, which is the primary purpose of patient counseling. Pharmacists have a “role and responsibility to instruct patients on how to use the medicines so that the benefits are maximized safely and risks were minimized.” This includes explaining “how to take the medication and for how long” 2 Problems like “Illegible prescription” (13.0% Present, but 83.1% in a Turkish study), “Dosing error,” and “Pharmaceutical dosage form” errors point to the need for rigorous dispensing practices. 16 Pharmacists are expected to verify the legality and completeness of a prescription, checking for missing information such as prescriber details, patient information, drug name, potency, dosage, total amount, instructions, refill information, signature, and date. 30 One of the most notable improvements after educational intervention was observed in prescription verification practices. Pharmacists reported being more attentive to checking the name and age of the patient, as well as verifying the prescriber’s signature and council registration number. This represents an important step toward ensuring prescription authenticity and patient identity, thereby reducing the risk of errors or misuse. Similarly, improvements were noted in checking the legality and completeness of prescriptions and ensuring the date of prescription is valid, particularly for controlled substances. Such practices strengthen the accountability and legal compliance of community pharmacies. They should also check for “appropriateness of medication for the individual,” including contra-indications and interactions. Any “incompleteness, ambiguities, confusions, shortcomings or anomalies” in a prescription should be brought to the prescriber’s attention. 2
The final review of a prescription and the correctness of dispensed medicines must be done personally by a pharmacist, who should also personally dispense the medicines. Numerous studies have documented similar gains in dispensers’ knowledge and practices following educational interventions. 26 A survey conducted in Sri Lanka, for example, reported a 60% increase in the mean score for detecting Drug-Related Problems (DRPs), indicating that the training had a significant impact on the capabilities of community pharmacists. 14 Educational interventions have also been shown to enhance pharmacists’ ability to assess the completeness and legality of prescriptions. According to a study in Pakistan, such interventions can improve the skills and knowledge of community pharmacy dispensers. 21 Better outcomes can be achieved by involving stakeholders in the design and implementation of these interventions. 31 Additionally, participants demonstrated increased awareness of drug interactions, contraindications, and patient history, including overuse, underuse, or misuse of medicines. The intervention also appeared to reduce inappropriate practices, particularly the dispensing of antibiotics without prescription. This finding is critical in the context of rising antimicrobial resistance in Nepal and globally, where community pharmacists play a pivotal role in ensuring antibiotics are used responsibly. Finally, the intervention reinforced pharmacists’ commitment to patient counseling and communication. Greater attention was paid to providing refill information, verifying whether the prescription was presented by the patient or a proxy, and checking for expiry dates before dispensing. A striking observation was the high percentage of respondents who were “not sure” about the presence of prescription errors. This suggests gaps in pharmacists’ ability to detect prescription-related problems, pointing to the need for capacity-building interventions, such as continuous professional training on Good Prescribing Practices (GPP), rational drug use, and the application of drug interaction checkers or electronic prescribing systems.
Limitation
The sample was limited to a specific geographic area and may not fully represent the practices of community pharmacists across the country. The results may be difficult to generalize to rural and isolated pharmacies. Secondly, the short follow-up period did not allow assessment of the long-term sustainability of the observed improvements. Finally, potential confounding factors such as differences in prior training, workload, or access to resources were not controlled, which may have influenced the extent of improvement across different qualification groups.
Conclusion
The educational intervention significantly improved knowledge and practice of prescription-checking, dispensing processes and counseling among community pharmacists. Pharmacists were more knowledgeable on Good Pharmacy Practice guidelines, including checking prescription details, assessment of dosage regimens, review of therapeutic appropriateness, and vigilance in screening for drug interactions and contraindications. The results of this research carry significant implications for both pharmacy practice and policy. To begin with, the observed enhancement in knowledge and practice after educational programs underscores the importance of integrating continuous professional development (CPD) initiatives within the national pharmacy framework. Lawmakers may want to think about adding structured training programs to the pharmacy licensing and renewal processes. These results demonstrate the potential of targeted education to optimize the clinical, regulatory, and patient-centered roles of community pharmacists and ultimately safer and more rational drug consumption within the community, rational drug use, and improved patient care outcomes.
Footnotes
Acknowledgements
The author takes this opportunity to thank all the participants of the study. I would like to give special acknowledge to my principle guide Dr Nur Akmar Taha for her consistent guidance throughout the studies. I also like to thank trainer of educational interventional Dr Shiv Bahadur Karkee, Dr Prayas Ghimire and other faculties from the department of Pharmacy at CIST College. My heartfelt thanks goes to University Grant Commission for funding my research
Abbreviations
CP: community pharmacists;
GPP: Good Pharmacy Practice
DDA: Department of Drug Administration;
NCDA: Nepal Chemist and
SPSS: statistical package for social sciences;
CMA: community medicine auxiliary;
B. Pharm: Bachelor in pharmacy; M.Pharm: Masters in pharmacy;
D. Pharm: Diploma in pharmacy.
H. A: Healthcare Assistant
Ethical Considerations
This study was approved by the National Health Research Council NHRC. The letter issued for the approval was numbered as 448/2023. All participants were informed about the aims and objectives of the study and invited to participate.
Consent to Participate
Written informed consent was obtained from all interested participants.
Consent for Publication
All authors have consented to publish the manuscript in INQUIRY journal and all authors have read and approved the final submitted version of the manuscript.
Author Contributions
Sangita Shakya, Dr Nur Akmar Taha and Dr Shiv Bahadur Karkee conceived and designed the study. SS, NAT and SB finalized the methodology and tools used. SS collected the data and analyzed the data. All the authors made significant contributions to writing the manuscript and reviewing the literature. Dr Ravi Shanker read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Authors acknowledge University Grant Commission UGC Sanothimi, Nepal for funding this research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.