
Abstract
We implemented and evaluated the impact of an innovative, pandemic-responsive nutrition education program, Enhanced-10 Tips for Adults (e-TTA), on food security, socialization, and perceived health and wellbeing of residents (aged 60+) in a low-income senior housing setting in Maine. The program was tailored to meet needs of older adults during the COVID-19 pandemic and utilized health professions students to support the program. A quasi-experimental research design was employed to measure participant psychosocial and dietary outcomes. Participant, student and nutrition educator experiences were explored through qualitative interviews. Quantitative data analysis included frequencies, means, and paired sample t-tests. Qualitative data were coded and analyzed using a rigorous thematic content analysis approach. Participants (N = 68) reported satisfaction with the program. Healthy Eating Index scores were significantly improved as were fatty acid ratios, self-reports of changing meals to be healthier, and confidence in choosing healthy budget-friendly foods to buy. Recommendations for program improvement are also reported.
Keywords
This manuscript adds to the existing literature in the following ways, by providing:
An innovative approach to provide needed nutrition education and socializing for vulnerable older adults while providing university health professions students with opportunities for practice experiences;
Evidence for the effectiveness of a pandemic-responsive nutrition education program for low-income older adults;
Recommendations for successful program implementation of the program.
Applications of study findings to gerontological practice, policy and/or research include:
A program that can be successfully implemented during a time when limited in-person contact is recommended to improve nutrition among vulnerable older adults;
Recommendations to ensure a virtual or hybrid nutrition education program for vulnerable older adults is effective.
Background
Older adults experienced far-reaching negative impacts of the COVID-19 pandemic on personal health and wellness, including on nutrition—arguably the most important factor for healthful independent aging.1 -6 Food insecurity, the state of not having reliable access to a sufficient quantity of affordable nutritious food, is significantly associated with undernutrition and adverse health outcomes, 7 and has been increasing in the U.S. since 1995 when it was first measured, affecting nearly 45 million Americans (17%) in 2020. 8 The State of Senior Hunger in America report in 2017 found that 5.5 million older adults (7.7%) were food insecure. 9 During the COVID-19 pandemic, aging Americans, already among the most vulnerable to the virus, were hit especially hard, with an estimated 60% increase in food insecurity. 10 Physical distancing measures required to control viral spread during the pandemic had particularly profound consequences for older adults, denying them assistance with daily living from informal networks, congregate meals, and important social opportunities which contribute to overall wellbeing. Maine has the largest proportion of older adults of all states (22.6% aged 65+ years per the 2020 US Census), and Maine older adults suffer disproportionately from poverty. The rural nature of the state adds additional barriers for service provision.6,11,12
Potentially effective interventions to impact social isolation during the COVID-19 pandemic include virtual components, cognitive or educational components, or facilitated communication between peers and yet recent reviews have suggested more studies are needed to understand how to feasibly impact social isolation and other important risks such as nutrition during a pandemic.13,14 Innovative approaches to addressing food insecurity and undernutrition among older adults while promoting social connection under such conditions are paramount for maintaining health and wellbeing in this population. Overcoming barriers to the use of technology, maintaining engagement and tailoring programs for older adults, including lifesaving nutrition services, were challenging during the pandemic, and these challenges have continued. Yet these difficulties have also provided valuable opportunities for innovation.
e-TTA Program
The 10 Tips for Adults (TTA) nutrition education program, on which the intervention (e-TTA) was based, was developed by the Maine Supplemental Nutrition Assistance Program-Education (SNAP-Ed) to support healthy eating on a budget and was added to the national SNAP-Ed toolkit in September 2020. 15 The curriculum reinforces messages related to increasing fruit and vegetable consumption, increasing physical activity, consuming more water, and providing low-income adults with the skills to purchase healthy foods on a budget.It can be applied in a variety of community-based settings and was designed to be implemented by professional Nutrition Educators.The curriculum is a practice-tested, evidence-based approach, designed to promote nutritional and health equity nationwide among low-income populations including older adults. The curriculum includes 2 distinct but complementary 4-session series: Series A: Choosing MyPlate and Series B: Eating Better on a Budget. These series are designed to be implemented separately or in sequence. Lessons are 60 min each but can be reduced to 30 to 45 min if needed. An accompanying cookbook was developed with recipes designed to be incorporated into the lesson plans, contributing to learning outcomes.
The COVID-19 pandemic compelled SNAP-Ed program coordinators to adapt the core TTA program in several fundamental ways at the onset of the pandemic. To overcome barriers identified by nutrition educators, program coordinators modified the curriculum to facilitate virtual delivery modalities and virtual participation. They created virtual slide decks, sample lesson plans, pre-recorded lessons, and pictorial recipes to support the original TTA curricula. Guidance was also modified to address virtual adaptations, and evaluation tools incorporated feedback on virtual modalities.
These modifications to TTA provided evidence for the updated TTA curriculum to potentially serve older adults in situations where social distancing is required such as during a pandemic. We then adapted the TTA program and implemented a pandemic-responsive
Westbrook Housing/University of New England Wellness Center
The mission of Westbrook Housing is toprovide opportunities for quality affordable housing and to encourage independence within a supportive community. The community is comprised of about 650 residents aged 55 years and older (mean age = 72 years). Eighty percent (80%) pay less than 30% of median rents in the local area. University of New England (UNE) health professions students work with residents through a shared Wellness Center in one of the Westbrook Housing buildings which served as the foundation for our e-TTA programing. 21 Students volunteer their time for various wellness activities and educational programs, work one-on-one and in small groups with residents on applied UNE course assignments, and engage in formal internships. Over 200 UNE students have provided targeted services to over 400 residents since 2021.
Description of e-TTA Implementation Process
e-TTA recruitment activities included posting flyers about the program, offering recruitment tables at Westbrook Housing wellness fairs, hosting several recruitment meal programs, and phoning residents over a 3-month period of time. The project ran five 8-session series over 13 months. Each cohort included 8 to 12 individuals, and 2 cohorts were implemented simultaneously. Two sessions per week (1 for each cohort) were provided for 8 weeks in a row. Participants were allowed to join the other weekly session if scheduling required (eg, due to health appointments).
UNE students—from dental hygiene, public health, and nutrition programs—and the research team prepared for each educational session in advance and worked together on data collection and recruitment between series (usually about 2 weeks). Before each session, ingredient packages were prepared, and frozen lunches were picked up from the Southern Maine Agency on Aging (SMAA). These lunches were stored in a freezer at the wellness center, and heated for each session using a portable oven provided by SMAA. Participants were encouraged to come early and socialize with each other. The nutrition educator provided opportunities for discussion and posed questions to engage participants throughout each session. Masking guidelines followed those of UNE and the Westbrook Housing Authority.
Aims
This project aimed to implement and evaluate the impact of
Methods
We employed a quasi-experimental, pre-post mixed methods approach to evaluate outcomes and processes for ongoing improvement. We used the RE-AIM model22,23 which includes 5 key constructs (Reach, Effectiveness, Adoption, Implementation, Maintenance) developed to evaluate community public health interventions including internal contextual issues affecting its success. Our approach was focused on 3 RE-AIM constructs: (1)
Outcomes, Measures, Data sources, and Timing (RE-AIM Effectiveness).

For measures on nutrition, we used the 6-item food security screening instrument
24
and the
For Socialization, we measured loneliness and engagement. For loneliness, we used the 8-item UCLA Loneliness Scale 26 and the 3-item Campaign to End Loneliness Measurement Tool (CELMT). 27 For engagement, we used the 8-item Flourishing Scale. 28
For Health and Well-Being, we used a single question on general health and the 9-item depression module from the Patient Health Questionnaire (PHQ-9), 29 and the 6-item Exercise Behaviors scale from the Self-Management Resource Center. 30
Description of Evaluation Tools
A participant tracking form tracked recruitment of participants by demographics and reason for refusal, drop-outs, and session no-shows. A 30-min enrollment survey administered in REDCap31,32 was completed by participants upon enrollment and included demographics (age, gender, race, ethnicity), income, disability, prior cooking experience, meal planning KABS, physical activity, and questions related to food access and purchase during the pandemic. A 15-min exit survey collected participants’ perceptions of the e-TTA program (whether content, time required, and setting were appropriate and helpful), satisfaction with congregate meals, and weekly take-home meal ingredient package (adequacy, ease of receiving package) and participants’ ideas for improvement, in addition to the key outcome measures described above. We also asked participants about their experiences during study recruitment, enrollment, and data collection. We repeated a shortened version of the exit survey 3 months after the final e-TTA session to assess whether changes in key KABS outcomes were sustained. The ASA-24 (described above) was used to calculate Healthy Eating Index (HEI-2015) overall and component scores. Participants were offered a $20 incentive for each of 2 completed ASA-24’s (1 weekday and 1 weekend day) at baseline and again at the end of the intervention.
The ASA-24, a web-based tool developed by the National Cancer Institute, enables automatically coded, self-administered 24-h recalls. Respondents are guided through the recall using a modified version of the USDA Automated Multiple-Pass Method. Participants in e-TTA were scheduled to complete each of the 2 ASA-24s online on 2 days before the first e-TTA session based on availability of the research assistant, and were offered assistance completing the surveys from trained UNE students, if desired. Participants were asked to complete 2 additional ASA-24s after the final e-TTA session using the same approach.
Participants were asked to complete a 5-min paper-and-pencil
Finally, 30-min Participant, Staff, and Nutrition Educator Key Informant Interviews (KIIs) were conducted to complement the quantitative data collected during the evaluation process. The qualitative key informant interviews (KIIs) were administered over the phone by trained staff with a subsample of participants at the conclusion of their cohort’s e-TTA program. Interview participants were recruited from each of the 5 educational series cohorts (total participants = 10). Participants who completed the series and those who dropped out of the program were recruited to help inform recommendations for improvement. Each interview participant received a $25 grocery store gift card as an incentive. The gift card could be used for any product the supermarket sold and was paid for through grant funding. The interviews explored the ways in which participants’ knowledge, attitudes, and behaviors around healthy eating and meal planning were affected. Similarly, KIIs were also conducted with program staff, student helpers, and the nutrition educator after the conclusion of the final cohort to help elucidate successes and barriers associated with implementation.
Data Analysis
Quantitative data analysis included descriptive analyses consisting of frequencies, proportions, and means (for Reach); and chi-square tests and paired sample t-tests using SAS version 9.4 (the SAS Institute, Cary, NC) to assess differences in key outcomes between pre-and post-intervention and between post-intervention and 3-month follow-up (for Effectiveness: knowledge, attitudes, beliefs and skills related to nutrition, socialization, health and well-being, Healthy Eating Index (HEI) scores, loneliness and engagement, general health, depression, and exercise behaviors).
Qualitative data from key informant interviews and notes in the project database were coded using NVivo 12 software (QSR International, Victoria, Australia) and analyzed using a rigorous thematic content analysis approach to enrich and expand quantitative findings.33 -35 For example, the key informant interviews with participants provided a deeper understanding how e-TTA was experienced, and the key informant interviews with staff and nutrition educators yielded detailed suggestions for specific process improvements in the implementation of e-TTA.
Results
Reach
One hundred and two (102) Westbrook Housing residents (out of 650) expressed interest in participating. Thirty-four (34) declined to participate. Thirteen (13) decided not to participate for unknown reasons, 8 could not be reached again after initial interest, and 5 declined at informed consent, 5 for scheduling reasons, and 3 for health reasons. Sixty-eight (68) participants were enrolled into 5 cohorts, each of which was provided 8 educational sessions. Of the 68 participants, 3 dropped out: 1 for mobility reasons and 2 for scheduling conflicts. Fifty-three (53) completed all surveys offered.
The average age of participants was 74 years with a range in age from 60 to 93, 81% (n = 55) were female, and 93% (n = 63) were White, non-Hispanic. Most (78%, n = 52) reported living alone and the majority (60%, n = 41) had annual incomes below $25 000. Thirty-four percent (n = 23) reported using SNAP, 57% (n = 37) reported mobility issues and 76% (n = 40) reported good, very good or excellent health; See Table 2.
Participant Characteristics (N = 68).

Effectiveness
Regarding meal planning knowledge, attitudes, beliefs, and skills, several highly significant changes were found including changing meals to be healthier, confidence in choosing healthy foods to buy and choosing healthy meals that fit a budget (Table 3). No changes were found in depression, physical activity, socialization, loneliness, or food security pre- versus post-intervention. However, the scores for social engagement demonstrated a positive trend.We saw no significant changes between the immediate post and 3-month post survey.
Knowledge, Attitudes, Beliefs and Skills, Pre- versus Post-Intervention.
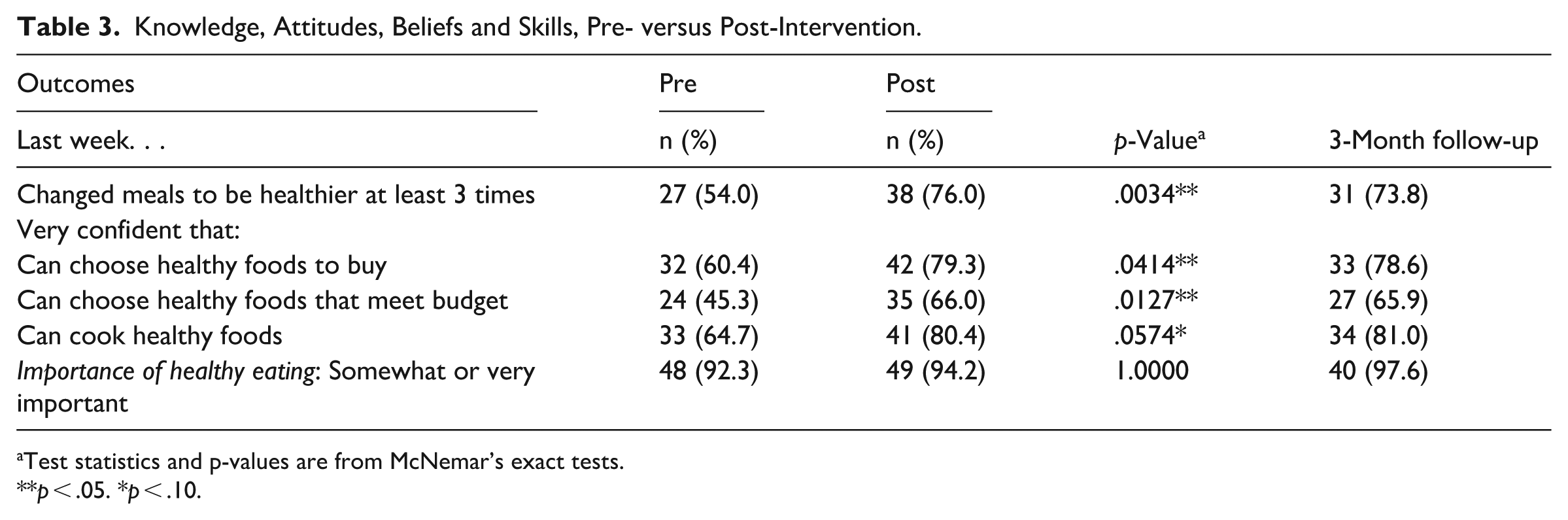
Test statistics and p-values are from McNemar’s exact tests.
p < .05. *p < .10.
Assessment of dietary intake demonstrated significantly improved outcomes for overall Healthy Eating Index scores and Fatty Acid Ratio scores as well as positive trends for “greens and beans” and “seafood and plant protein” (Table 4).
Dietary Intake, Pre Versus Post-Intervention.

Test statistics are from McNemar’s exact tests for categorical variables and Wilcoxon signed rank tests for continuous variables.
p < .05. *p < .10.
Implementation
Program implementation reflected a high level of fidelity to the implementation plan (Table 5). All planned sessions for each of the 5 educational series (8 sessions each) were held, and each participant was offered a meal at every session and a take-home package of ingredients for the recipe that was demonstrated. A few of the educational sessions were recorded and provided asynchronously due to illness or unavailability of the nutrition educator. Session evaluations reflected a high level of participant satisfaction (average Likert-type score where 1 is extremely unsatisfied and 5 is extremely satisfied).
Summary of Session-Specific Participant Evaluations, Total Mean Scores.

Ten (10) participant interviews were conducted. The nutrition educator and 2 students were also interviewed, and the research assistant provided written reflections and ideas for improvement (Table 6). Lessons learned included:
assure adequate space (eg, walkers, wheelchairs and for physical activity);
assure adequate technology (eg, adequate sound, strong WIFI/cell service and visual size);
don’t use tablets for data collection, use computers or interview participants for better data collection process;
minimize data collection, this can be a barrier (eg, fear of fraud);
make sure to prioritize socializing with group; ensure maximum engagement (eg, for the recipe demo have individuals prepare themselves);
serving a meal may not be best use of resources (eg, timing, personal preferences, issues with frozen meals);
maximize participant time with students;
provide both basic and in-depth learning and tie nutrition education to specific disease/health issues;
Assure that recipes and ingredient packages minimize need for preparation such as chopping;
provide small portions of things like vinegar; tailor recipes/cookbook to those ideal for older adults (eg, prep needed, chewing issues, tools required).
Examples of Key Themes, Strengths, Weaknesses, and Quotes.

Discussion
Enhanced-10 Tips for Adults (e-TTA), a pandemic-responsive nutrition education series adapted from SNAP-Ed’s Ten Tips for Adults (TTA) program, in partnership with a low-income older adult housing community and a local Area Agency on Aging partner, demonstrated potential positive outcomes on participant knowledge, attitudes, beliefs, skills, and diet before and after intervention among older adults in southern Maine. No significant changes in food security, socialization, engagement, or loneliness were detected, although a marginally significant increase in engagement was measured. The lack of change in these outcomes over an 8-week timeframe was not necessarily surprising. Previous studies found effective to impact depression and social isolation under similar circumstances included psychological components and greater social engagement than we were able to provide.13,14 Qualitative insights indicated strong participant satisfaction with the program particularly related to interactions with the students consistent with evidence from student-led and intergenerational support interventions shown to positively impact psychological wellbeing.13,17,18,36 The qualitative interactions also identified some missed opportunities with regard to socialization before, during, and after the educational sessions as well as maximizing time with the student helpers to interact with participants, a component expressly desired by participants but not maximized by our program. Our findings on nutrition-related psychosocial and behavioral improvements underscore the effectiveness of the SNAP-Ed-based curriculum in encouraging small and incremental behavioral changes and a greater emphasis on cost-savings.
Older adults generally have lower caloric needs, but similar or even increased nutrient needs compared to younger adults. Older adults already have the highest diet quality compared to other age groups in the US, with an average national HEI score of 63 out of 100. 37 Average baseline HEI scores for our participants was 57, below the national average for older adults in the US. Our participant population therefore had, and still has plenty of room for improvement with a post-intervention score of 62. The Office of Disease Prevention and Health Promotion (ODPHP) of the US Department of Health and Human Services (DHHS) recommends older adults eat more protein—especially adults ages 71 and older. And, because older adults tend to meet recommendations for meats, poultry, and eggs, it is important to encourage the consumption of seafood, dairy and fortified soy alternatives, beans, peas, and lentils given the additional benefits that these protein sources provide (eg, additional nutrients, such as calcium, vitamin D, vitamin B12, and fiber). e-TTA showed significant dietary improvements in these areas among participants and therefore may be considered a tool to help achieve expert recommendations.
Given what we learned our participants would have liked more information about, improvements in e-TTA could include components of programs like those endorsed by the National Council on Aging (NCOA) that focus on chronic disease management and healthy aging, teaching older adults how to manage their health conditions through diet. 38
Other nutrition education programs that have been successful in promoting the consumption of more fruits, vegetables, whole grains, and dairy while reducing intake of added sugars, sodium and saturated fats though few have taken a hybrid online/in person approach that can easily be shifted to completely virtual if needed. With changes based on our quantitative and qualitative findings, e-TTA may be a useful and scalable tool combining the resources of a health sciences university to keep older Americans safe during a pandemic or another situation requiring physical distancing while supporting nutrition and overall wellbeing.
Limitations
There are several key limitations inherent in our study’s quasi-experimental design. There was no comparison or control group. It is possible that our findings could be attributed to changes in the general older adult population’s dietary intake, although we have observed no evidence of this. We recruited a convenience sample of older adults who were willing and able to participate and there might have been something about them that made it more likely they would have benefited from our program or they were different in some other way from the general population of older adults living at Westbrook Housing. In addition, our small sample size and the fact that participants were mostly white and rural and while reflective of Maine, our study population does not reflect that of other populations in the US and therefore our findings may not be generalizable to other populations. Further, we experienced challenges to data collection. Some of our participants did not compete all of the surveys offered to them. The participants who did complete surveys may have been different from those who did not. For example, those who did not may have been more reticent about their KABS or dietary intake. We also offered some residents technical assistance completing surveys (eg, reading the dietary intake to then and filling it out on their behalf). While we did our best to assure participants that there were no right or wrong answers, this practice may have introduced a social desirability bias into our findings.
In addition, given the congregate context the participants were living in, baseline engagement scores may have been higher and loneliness scores lower than among the general population of older adults.It is therefore is possible that improvement in these measures may have been less likely to increase given our intervention and population of participants. The 8-week length of our curriculum and its emphasis on skills-building, reading and understanding food labels well as providing shopping tips (eg, buy what’s in season to save money, frozen fruits and vegetables are healthy) may also have contributed to measured improvements in KABS and diet. Further, our participants may have benefited from having a large discount grocery store (Market Basket) within a 5-min walk or very short drive from most locations within Westbrook Housing.
Conclusion
An evidence-based nutrition education series for older adults can be effectively implemented in partnership with a health science university in a pandemic-responsive way to improve healthy eating knowledge, attitudes, beliefs, and practices and healthy eating among low-income seniors in congregate settings. SNAP-Ed or other programs could use our findings to make simple, inexpensive changes to adapt this program to low-income older adults.
A partnership between low-income housing and a health science university can provide important skills building opportunities for students needed for graduation and with sufficient student interaction may provide desired companionship and services for older adult residents.
Footnotes
Acknowledgements
We wish to thank UNE health professions students as well as the Westbrook Housing Authority staff who participated in this project.
Ethical Considerations
The University of New England Office of Research Integrity determined that the project (IRB # 0823-03-01) was exempt from IRB review and oversight as defined by 45 CFR 46.104.
Consent to Participate
Written informed consent was obtained from each participant.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported, in part, by grant number 90INNU0032, from the Administration or Community Living, U.S. Department of Health and Human Services, Washington, D.C. 20201. Grantees undertaking projects with government sponsorship are encouraged to express freely their findings and conclusions. Points of view or opinions do not, therefore, necessarily represent official ACL policy.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.