
Abstract
Adverse childhood experiences (ACEs) are linked to lasting health and socioeconomic challenges; however, less is known about how primary care providers’ own trauma histories impact their provision of trauma-informed care (TIC). This cross-sectional survey study assessed the relationship between primary care providers’ personal trauma history (ACE scores), personal reaction to trauma (burnout, compassion fatigue, and vicarious victimization), and TIC practice. A total of 167 primary care providers were recruited between March 2024 and August 2024 and completed a 38-item online survey. Measures included the Trauma Informed Care-Provider Assessment Tool (TIC-PAT), the Professional Quality of Life Scale (ProQLS), the ACEs Study Questionnaire, and demographics. Descriptive statistics and multiple linear regression analysis was conducted. Respondents were an average of 59.73 years old, white (88.89%) and medical doctors (90.48%). Average ACE score of respondents was 1.4 (SD = 1.47). Analysis revealed that providers with higher ACEs scores were significantly more likely to implement TIC (B = 0.11, P = .02). However, no significant association was found between personal reaction to trauma and TIC provision. Findings suggest that primary care providers with personal trauma histories may be more attuned to the effects of trauma, leading to greater TIC implementation. The study highlights the importance of TIC training for all providers—particularly for those with lower ACE scores—while also recognizing that providers with higher ACE scores may benefit from training to manage personal trauma and enhance their clinical practice.
Highlights
● Primary care providers with higher adverse childhood experiences (ACEs) scores were more likely to implement trauma informed care (TIC).
● No significant association was found between providers’ personal reaction to trauma—burnout, compassion fatigue, or vicarious vitimization—and TIC provision.
● Primary care providers’ average ACEs scores were low.
● Personal trauma history among primary care providers may foster empathy and patient-centered care, highlighting the need for TIC training and institutional support.
Introduction
Traumatic childhood experiences of abuse, neglect, family dysfunction, parental separation, and violence are common. These preventable adverse events before age 18, also referred to as adverse childhood experiences (ACEs), are associated with negative short- and long-term physical, mental, and emotional outcomes; health-risk behavior; and socioeconomic hardship. 1
ACEs are widespread in the United States (U.S.) population. Close to 64% of U.S. adults experienced at least 1 ACE and close to 17% reported 4 or more ACEs based on the 2011 to 2020 BRFSS data from the 50 states and the District of Columbia. 2 An earlier study based on the 2015 to 2027 BRFSS data from 25 states showed similar results. Close to 16% (15.6%) of U.S. adults reported 4 or more ACEs. 1 Although there are state-level jurisdictional variations in the total number of ACEs, these adverse experiences were highly prevalent among certain sociodemographic groups. 2 Specifically, ACE exposure is more common among women, young individuals aged 25 to 34, native American Indian or Alaska Native adults, multiracial adults, non-high school graduates, and the unemployed. 2
Given the lasting impacts of trauma, including ACEs, trauma-informed care (TIC) has emerged as a framework for addressing the effects of trauma in healthcare and other settings. Core components of TIC include: (1) increasing physician education about emotional trauma, (2) learning how to identify and treat trauma, and (3) learning how to ensure the patients feel safe and are not retraumatized by healthcare providers. 3 Research has shown that TIC interventions focused specifically on ACEs positively impacts patient and provider outcomes. For patients, one study demonstrated that physicians were 3 times more likely to document referrals when patients were screened for ACEs. 4 Qualitative research has revealed that patients and providers feel positively about ACEs screening and acknowledge its potential for building trust and improving care. 5 Psychological therapies for patients experiencing ACEs has demonstrated the strongest evidence for improving outcomes. 6 For caregivers, TIC training among clinicians has been shown to increase knowledge of TIC principles and increase the intention to provide TIC. 7 Major challenges with implementing ACEs related TIC trainings is the inconsistency in standards across healthcare disciplines and time constraints. 8
Despite its importance, implementation of TIC has been inconsistent in healthcare. 9 Research indicates that a providers’ personal belief and experiences shape their willingness to practice TIC. 9 Additionally, TIC is not just about accessing patients ACEs scores; comprehensive provider training is needed to ensure they can help their patients without inadvertently hurting or retraumatizing them. 10
The TIC Pyramid provides a conceptual framework for integrating the provision of TIC in healthcare settings. 11 This framework outlines principles related to universal trauma precautions and trauma-specific strategies that may be employed and considered by providers. Universal trauma precautions involve those things providers can do without knowing about a patient’s trauma history that can help with establishing trust and rapport. These precautions include patient-centered communication and care and understanding the health effects of trauma. Trauma-specific strategies apply when providers know or strongly suspect a patient has a trauma history and includes interprofessional collaboration (coordinating service such as mental healthcare, social work, and case managers), understanding provider’s own history and reactions to trauma, and screening for trauma history among patients.
Healthcare providers are not exempt from adverse childhood events or their negative health consequences. A history of ACEs among U.S. healthcare providers, especially among those at the frontline, can potentially affect not only how they interact with their patients but also their adoption of trauma-informed care (TIC) in clinical settings. According to a 2021 study of 1125 U.S. physicians, having one or more ACEs was associated with mild to severe depression. 12 Experiencing ACEs, adverse occupational events (AOEs), and medical errors, including COVID-19-related events, were likewise associated with physician burnout. 12
Despite increasing awareness of ACEs, little is known about providers’ own childhood experience with trauma (personal ACE score), even though many have their own personal trauma. 13 While some evidence suggests that providers present lower quality of care when they personally have PTSD, the direct relationship between TIC and provider trauma history remains unclear. 14 Some research suggests that providers who assess their personal ACE scores may better understand the clinical and scientific foundations of TIC, 15 but no studies have specifically examined how a provider’s own ACEs influence their adoption of TIC principles.
Beyond personal trauma histories, a provider’s personal reaction to trauma or the emotional toll of responding to patient trauma can impact their well-being. The spectrum of negative impacts of vicarious victimization on health providers includes vicarious traumatization, secondary traumatic stress, burnout, PTSD, unhealthy behaviors, and compassion fatigue. 16 A meta-analysis of studies on trauma experienced by providers during traumatic childbirths revealed 4 major themes for providers experience: (1) an instantaneous response to the trauma, (2) finding hope in the midst of chaos, (3) dealing with the aftermath, and (4) resolving to move on. 17
Compassion fatigue has been widely used to describe the negative reaction of trauma related work among clinicians.16,18 Research has indicated that compassion fatigue is prevalent across healthcare practitioner groups.19 -22 Burnout among healthcare providers is also highly prevalent, ranging from 14% to 70.1% depending on the practitioner’s specialty.23,24 High sensitivity to stress and low job satisfaction have been identified as significant risk factors. 25 While this body of research is useful in understanding the impact of personal trauma on care, it does not fully address how a provider’s own trauma history influences their ability to practice TIC.
The aim of this study was to examine how primary care providers’ personal trauma histories (measured by ACE scores) and their personal reactions to trauma (measured by professional quality of life) are associated with their practice of TIC. Specifically the study examined: (1) What is the prevalence of ACEs among primary care providers? (2) How is provider’s personal trauma history associated with their provision of TIC? And (3) Does a provider’s emotional reaction to trauma impact their provision of TIC?
Method
This study utilized a cross-sectional survey design to assess the relationship between primary care providers’ personal trauma history, personal reactions to trauma, and their implementation of TIC. The research team included researchers with previous experience studying TIC and ACEs with 1 member of the team being a medical doctor.
Participants and Procedures
The non-probably, convenience sample included 167 respondents who self-identified as primary care providers throughout a variety of clinical settings including but not limited to: Family Practice, Psychiatry, Pediatrics, Internal Medicine, and Obstetrics/Gynecology. Respondents were recruited from March 2024 to August 2024. Inclusion criteria required that respondents be practicing primary care providers working in U.S. clinical settings, able to reach English, and willing to provide implied consent. Exclusion criteria included incomplete survey responses. A total of 41 participants were excluded from the final analyses due to incomplete responses and thus the final sample consisted of 126 primary care providers.
A survey was administered online to primary care providers across the U.S. using Reaction Data’s proprietary research cloud platform (https://reactiondata.com/). This platform is comprised of a network of 800 000+ employees across the U.S. healthcare system including but not limited to hospitals, clinics, payers, and pharmaceutical companies. Of particular interest was their ability to reach primary care providers across the U.S. in a variety of clinical settings such as in Family Practice or Internal Medicine.
Reaction Data sent 6 email invitations to potential primary care respondents. Out of 3447 individuals who confirmed opening the email invitation, 165 initiated the survey, resulting in a non-response rate of approximately 95% among those who opened the email. The survey was initiated when participants agreed to an implied consent letter. Participants opted into this study voluntarily and were able to terminate their participation at any time. They were informed the survey would take approximately 5 min to complete and were provided with the option of receiving preliminary results through email. No incentives other than survey results were provided for participation in the study. The study was approved by the Brigham Young University Institutional Review Board and deemed as exempt.
All data collected from surveys were stored on password-protected servers managed by Reaction Data and the lead author. Survey responses were anonymous, and no personally identifiable information was collected by the research team. Only the research team had access to the raw data with data retained in accordance with IRB guidelines for a minimum of 3 years.
Measures
The survey included 38 questions: 9 demographic questions (age, sex, marital status, race/ethnicity, children in the home, profession, years in practice, region of healthcare facility, and type of healthcare facility), 10 TIC questions, 9 personal reaction to trauma questions, and 10 personal trauma history questions. The validated Trauma Informed Care-Provider Assessment Tool (TIC-PAT) 26 was used to assess how well primary care providers implement universal trauma precautions and trauma specific care in their current practice. The TIC-PAT measures the 5 principles of the TIC pyramid: community and care, health effects, interprofessional collaboration, history, and reactions, screening. The TIC-PAT includes 10 items on a 5-point Likert scale ranging from “strongly disagree” to “strongly agree” for items measuring how well providers implement universal trauma precautions and from “never” to “always” to assess provision of TIC. Sample items included “I ask what can be done to make patients more comfortable during the appointment” (agreement) and “I screen for trauma in every new patient” (provision of TIC). The 10 items were averaged for an average mean score that could range from 1 to 5. Cronbach’s alpha for the current sample was .84.
The Professional Quality of Life Scale (ProQLS) was used to assess primary care providers’ personal reaction to trauma and reflects respondents’ professional quality of life at the time of the survey. The ProQLS is a 9-item validated measure of burnout, compassion fatigue, and vicarious victimization of healthcare providers. 23 Respondents indicated agreement on a 5-point scale ranging from “never” to “very often.” Sample items included “I feel trapped by job as a helper,” “I feel worn out because of my work as a helper,” and “I am happy that I chose to do this work.” Some items were reverse coded so that higher scores indicated higher professional quality of life. The 9 items were averaged for an average mean score that could range from 1 to 5. Cronbach’s alpha for the current sample was .85.
The ACEs Study Questionnaire was used to assess primary care providers’ personal trauma history. This measure is retrospective and refers to events during childhood. The questionnaire is a 10-item validated scale and is a product of the collaboration between the Centers for Disease Control and Prevention (CDC) and Kaiser Permanente.27 -29 The more toxic experiences, the higher the ACE score. The questionnaire asks about exposure and/or experience with 5 types of maltreatment and 5 types of family or household dysfunction during childhood. Maltreatment is comprised of (1) physical abuse, such as hitting, punching, or burning; (2) emotional abuse, such as verbal or emotional criticism, threat, or rejection; (3) sexual abuse, which includes molestation and exploitation; (4) physical neglect, which involves the lack of necessities such as food, clothing, and shelter; and (5) emotional neglect or the deprivation of love, emotional support, and nurturing. On the other hand, family or household dysfunction ranges from experiencing the loss of a parent due to divorce, death, or abandonment; witnessing and/or experiencing violence in the household, including being bullied and/or being exposed to violence in the community; to living with a family member or caregiver with mental illness, substance use disorder, and/or a history of incarceration. Response options were dichotomized (0 “never experienced the ACE” and 1 “experienced ACE at least once.” Sample items included “Were your parents every separated or divorced?” and “Did you live with anyone who was a problem drinker or alcoholic, or who used street drugs?” Items were summed for total scores that could range from 0 to 10 ACEs.
Analysis
Descriptive statistics were calculated for the demographic variables and primary measures of interest: TIC-PAT, ProQLS, and ACEs. Multiple linear regression analysis was conducted to explore the associations between ACEs and ProQLS with TIC-PAT. Due to a high rate of missing data among demographic variables, pairwise correlations were conducted to assess their relationship with the independent and dependent variables. None of the demographic factors were correlated with TIC-PAT or the covariates of interest. As no significant associations were found, no demographic controls were included in the regression analyses. All analyses were performed using STATA SE, Version 18 (StatCorp, College Station, TX).
Results
Sample Description
Most respondents were an average of 59.73 years old, white (88.89%), female (56.19%), married (84.13%), a Doctor of Medicine (MD; 90.48%), and have worked an average of 28.61 years (see Table 1). Half of the sample was practicing in academic affiliated organizations (25.00%) and community health centers (25.00%). The composite mean score of the ProQLS scale was 2.96 (SD = 0.502), the TIC-PAT mean score was 3.81 (SD = 0.758), and the average ACE score was 1.4 (SD = 1.47).
Descriptive statistics.
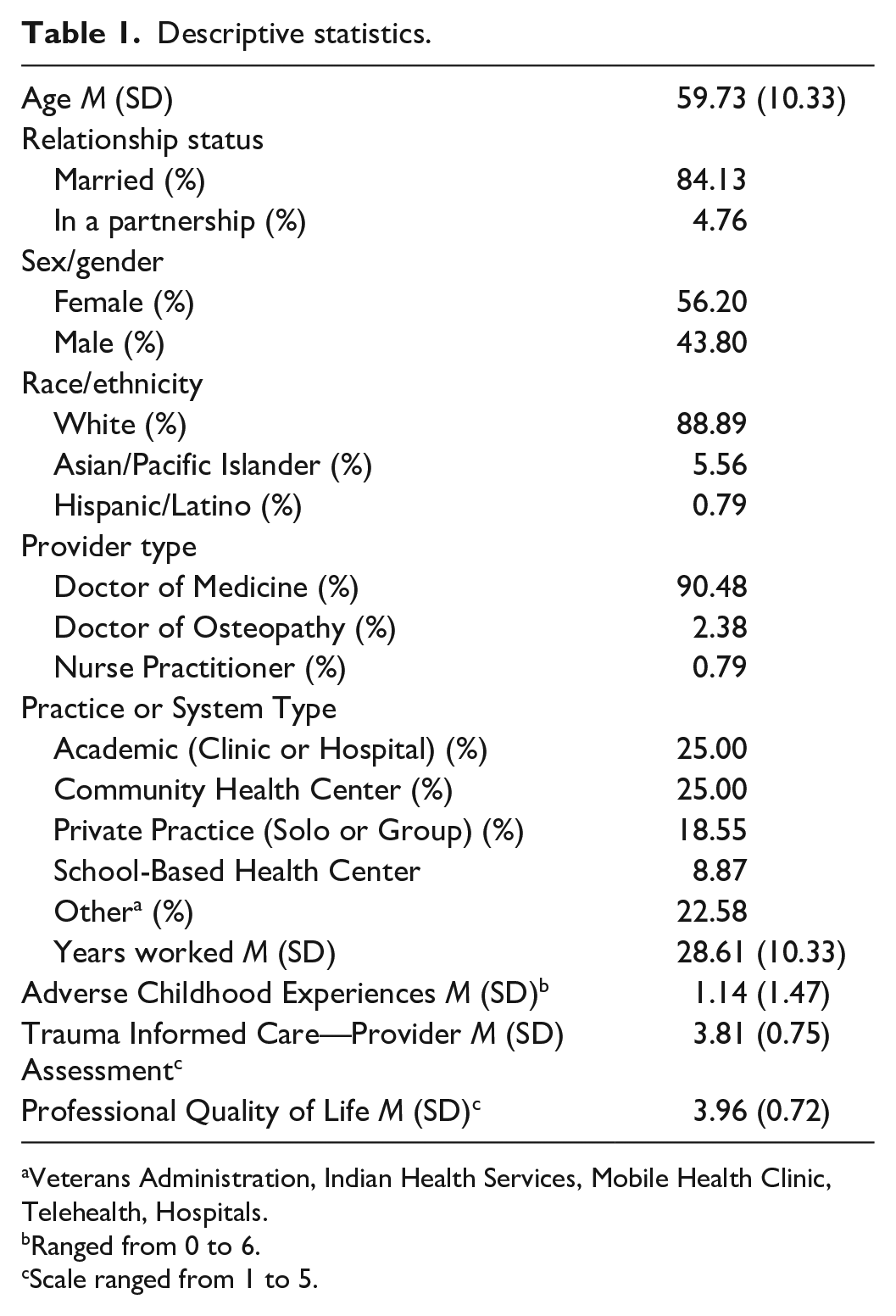
Veterans Administration, Indian Health Services, Mobile Health Clinic, Telehealth, Hospitals.
Ranged from 0 to 6.
Scale ranged from 1 to 5.
Provider Childhood Trauma, Reaction to Trauma, and Trauma-Informed Care Provision
Results of the multiple linear regression revealed that primary care provider trauma history (personal ACE score) was positively associated with the provision of TIC (B = 0.11, P = .02). That is, the higher their personal ACE score, the greater their practice of TIC as healthcare professionals (see Table 2). No association was observed between primary care provider reaction to trauma (ProQLS) and their provision of TIC. Since no demographic variables were pairwise correlated with the dependent or independent variables of interest, it was elected not to include them in the multiple linear regression analysis.
Multiple linear regression of the association between ProQLS and ACEs with trauma-informed care (TIC) among primary care providers, N = 126.

Discussion
This study investigated the impact of personal trauma history (ACEs) and personal reaction to trauma (professional quality of life) among U.S. primary care providers on the provision of TIC. The total of 126 primary care providers had an average of 1.14 ACEs. Collectively, respondents’ ProQLS scores indicated a cohort with low personal reaction to trauma (burnout, compassion fatigue, and vicarious victimization). Multiple linear regression analysis showed that a history of trauma was positively associated with the provision of TIC. This means that the higher the reported cumulative ACE score, the more likely an individual was to practice TIC. Thus, the cumulative ACE score serves as a predictor of TIC implementation in clinical settings. However, no significant relationship was found between personal reaction to trauma and TIC adoption.
A key finding of the study was that primary care providers with higher trauma history (personal ACE score) were more likely to practice TIC. This aligns with previous research that suggests primary care providers who have experienced trauma at the formative stage of life may develop a deeper sense of empathy, sensitivity, and awareness of the impact of trauma on others. 30 In addition, providers with ACEs and exposure to other traumatic events were more confident in examining their patients’ own trauma histories and displayed greater empathy in their relationships with patients. 31 As such, providers with higher ACEs may be more cognizant of the presence of stressors, ACEs, and other harrowing emotional experiences among their patients, and are thus, more likely to apply TIC in clinical settings compared to those with lower ACE scores. This highlights the importance of TIC training, especially to those providers without trauma exposure, in order that trauma sensitive care might be provided to patients.
The mechanisms linking primary care provider trauma history (personal ACE score) with the application of TIC are undoubtably complex and multifaceted. Although this study showed the positive influence of physicians’ trauma history on the adoption of TIC, other studies have reached a different conclusion. A history of ACEs can elevate the risk of provider anxiety, and depression, which could likewise hinder the practice of TIC. 32 High patient workload, long hours, and repeated exposure to human suffering, such as pain, trauma, life-threatening conditions, and pandemic conditions, including death, can take an emotional toll on healthcare providers.12,33 The direct and/or indirect exposure to patients’ traumatic experiences, on top of a personal history of ACEs, can render a provider susceptible to vicarious trauma—an alteration of the response to trauma and of the general view of the world, which includes secondary traumatic stress (STS), compassion fatigue (CF), and critical incident stress (CIS).34,35 These responses to trauma can consequently deter the provision of an empathetic and supportive healing environment. 12
Contrary to expectations, this study did not find a significant association between personal reaction to trauma (professional quality of life) and provision of TIC. This finding may be because in this sample, primary care provider ACE scores were relatively low (M = 1.14, SD = 1.47). While prior research has suggested that burnout, compassion fatigue, and vicarious trauma can negatively impact healthcare provider well-being,16,17,19 the current study found that these factors did not impact the likelihood of providing TIC. Although no association was found, primary care providers with higher rates of burnout, compassion fatigue, and vicarious victimization may be pushing through these struggles and remain committed to providing TIC to their patients. It is possible that other factors such as workplace culture, institutional support, and professional values may have a greater influence on TIC. Indeed, multiple factors play a role in the delivery of TIC in clinical settings—from harboring residual trauma, increasing susceptibility to secondary stress and compassion fatigue, blurring professional boundaries, and neglecting self-care, to institutional factors that promote re-traumatization. 36 Recognizing and responding to these mechanisms requires a comprehensive approach, such as screening for ACEs and other adverse occupational experiences, 37 promoting an empathetic healing environment, adopting workplace culture, and mental health resources that support providers and staff, 33 and applying primary care interventions to increase trauma prevention and awareness. In addition, future primary care providers can benefit from trauma-informed medical education to prevent lapses in professionalism, particularly for those with ACEs. 35
Implications of the findings of this study suggest the importance of TIC training for healthcare providers, including those with low ACE scores, as TIC adoption was positively associated with providers’ personal trauma history. In addition, these findings align with prior research showing limited physician training and experience on TIC in clinical settings. 36 Training on TIC could focus on all core TIC principles, including screening and health effects, together with self-care and resilience even when healthcare providers report strong compassion saturation and low burnout. Additionally, because reaction to trauma (professional quality of life) was not associated with TIC provision, these results suggest the need for workplace and institutional support for TIC implementation. Factors such as workplace culture, institutional policies, and leadership support may play a stronger role in maintaining the provision of TIC. Future research might explore what allows primary care providers to maintain TIC provision in the face of personal trauma reaction. Initiatives implemented at organizational levels could potentially include screening for ACEs among physicians, not only as a preliminary step to TIC training but to also increase physicians’ cognizance of their ACEs and any unresolved trauma that can influence their professional behavior and interactions with patients. 36 Finally, these findings provide preliminary support that a personal history of trauma does not necessarily hinder a provider’s provision of TIC. Given low provider ACE scores and smaller sample size, further research with a larger sample in needed to explore this relationship more definitively.
Findings from this study should be viewed through the lens of several limitations. First, this was a cross-sectional study and causation between variables cannot be established. The associations between the variable of trauma history, professional quality of life, and TIC provision are correctional and should be interpreted as such. Second, the sample size was relatively small, consisting of 126 completed surveys, and was largely white, and all physicians. As such, it may not be reflective of healthcare providers from minority groups or other healthcare specialties such as nurse practitioners (NP) and physician assistants (PA). Close to 50% of PAs and 85% of NPs likewise serve in primary care settings, particularly among vulnerable, disadvantaged, and marginalized populations in urban poor, and rural areas. 38 As such, we highly recommend that future studies aim for a larger and more racially and professionally diverse sample size. Additionally, the research could be expanded to include NPs and PAs. Third, the response rate was low. Many participants stopped the survey after the first set of Likert response questions related to their provision for TIC (TIC-PAT). This early dropout may have introduced bias as those who completed the survey may differ in their experience or perspectives on personal reaction trauma (ProQLS) and trauma history (ACEs). There is evidence that offering monetary incentives to healthcare provider can increase response rates, potentially leading to a larger sample size and less dropout.39,40 Fourth, Green’s rule of thumb 41 was used to determine the sample size for regression analysis with no power analysis conducted. Fifth, some of the data were skewed. A structural equation model was run in Mplus using a robust weighted least squares estimator, which is appropriate for categorical data. This estimator relaxes many of the assumptions required for multiple linear regression. The results were substantively the same as our results using multiple linear regression. Finally, data were not collected relating to previous and current TIC training or availability of institutional and system-level support—both of which could influence the decision to apply TIC. Future research should evaluate how such training and institutional supports affects the practice of TIC.
The strengths of this study include the use of an online survey that allowed for the diverse sampling of primary care providers across various states and regions that we might not otherwise have access to and the enhanced understanding of the impact of personal trauma history on providers’ bedside manner and care of their patients. As primary care providers are typically the first point of contact for patients who are experiencing trauma and who may also have a history of ACEs, it is important to understand the factors that may contribute to the universal and optimal adoption of TIC and its core principles. Further, these findings provide support for TIC training among all types of providers to improve patient care and clinical outcomes.
Conclusion
A personal history of trauma (ACEs) can influence a primary care provider’s decision and ability to apply TIC in clinical settings. Although other studies showed that ACEs may exert a negative influence on the adoption of TIC, this study’s findings among predominantly white physicians with low ACE scores showed that the higher the cumulative ACE score among primary care providers, the more likely they were to implement TIC practices. Overall, the results contribute to the emerging research on how personal trauma shapes not only the quality of interpersonal interactions but also professional behavior within the healthcare setting—both consciously and unconsciously. As TIC continues to be widely adopted in interdisciplinary settings, it is vital to address the individual, institutional, and system-level factors that promote or hinder TIC implementation, ensuring care environments of healing and resilience, especially for trauma survivors.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251365460 – Supplemental material for The Influence of Adverse Childhood Experiences on Trauma Informed Care Among Primary Care Providers: A Cross-Sectional Study
Supplemental material, sj-docx-1-inq-10.1177_00469580251365460 for The Influence of Adverse Childhood Experiences on Trauma Informed Care Among Primary Care Providers: A Cross-Sectional Study by Kayla Gardner, Benjamin Ivins, Trinity Mathis Peters, Len Novilla, Ali Crandall and Carl L. Hanson in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580251365460 – Supplemental material for The Influence of Adverse Childhood Experiences on Trauma Informed Care Among Primary Care Providers: A Cross-Sectional Study
Supplemental material, sj-docx-2-inq-10.1177_00469580251365460 for The Influence of Adverse Childhood Experiences on Trauma Informed Care Among Primary Care Providers: A Cross-Sectional Study by Kayla Gardner, Benjamin Ivins, Trinity Mathis Peters, Len Novilla, Ali Crandall and Carl L. Hanson in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
Not applicable.
Ethical Considerations
The study was approved by the Institutional Review Board at Brigham Young University on February 15, 2024 (IRB2024-022).
Consent to Participate
Implied consent was obtained from all participants before inclusion in the study by selecting “yes” to the informed consent letter after reading the study information.
Author Contributions
Conceptualization: CLH, KG, TMP, BI; methodology: CLH, KG, TMP, BI; analysis: AC, CLH; writing—original draft: KG, TMP, BI, LN, AC, CLH; writing—final review, and editing: AC, CLH.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available from the corresponding author upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.