
Abstract
Individuals with a history of adverse childhood experiences (ACEs) disproportionately have poor mental and physical health outcomes. These experiences affect individuals across the life span extending beyond health with deleterious impact on work-related outcomes. Low-wage workers are particularly at risk. Social service and health organizations are becoming aware of the extent to which the populations they serve have been affected by these experiences. Employment support programs may serve high-ACE individuals but likely are unaware of their histories and the developmental or health deficits that result and can impinge on successful employment. Occupational health nurses may be well-positioned not only to implement trauma-informed care in workplaces but also to influence the ways in which employment services for this vulnerable group are delivered. The purpose of this article is to consider how ACEs could affect vulnerable workers. The need for trauma-informed research and praxis to advance occupational health nursing is discussed.
Keywords
Work is central to individual identity, social roles and social status . . . Employment and socio-economic status are the main drivers of social gradients in physical and mental health and mortality.
Over the past two decades, adverse childhood experiences (ACEs) have emerged as risk factors for numerous negative health outcomes. The initial conceptualization of ACEs included exposures to physical, sexual, and emotional abuse and physical and emotional neglect, witnessing domestic violence, having a parent or guardian with a substance abuse disorder or other significant mental illness, having parental divorce or separation, and having an incarcerated family member (Felitti et al., 1998). More recently, the list of ACEs has been expanded to include exposures to peer victimization and social isolation, community violence, and low socioeconomic status (Finkelhor, Shattuck, Turner, & Hamby, 2015; Turner, Finkelhor, Shattuck, & Hamby, 2012). These exposures result in posttraumatic stress disorder (PTSD), substance use disorders, depression and suicide attempts, and obesity with high levels of ACEs linked to diseases later in life (e.g., ischemic heart disease, liver and lung disease, cancer and bone fractures) contributing to significant morbidity and early mortality (Dube, Anda, Felitti, Chapman, et al., 2001; Dube, Anda, Felitti, Croft, et al., 2001; Dube, Anda, Felitti, Edwards, & Croft, 2002; Edwards, Holden, Felitti, & Anda, 2003; Finkelhor et al., 2015). Although any single ACE can negatively impact the well-being of an individual, the most significant associations between ACEs and early morbidity and mortality arise when individuals are exposed to multiple ACEs over time, demonstrating a cumulative or compounding effect (Felitti et al., 1998). The goal of this article is to engage occupational health nurse clinicians and researchers in an essential conversation about how best to provide care for and conduct research with workers experiencing the long-term negative effects of ACEs, drawing from the literature and presenting a case illustration.
Youth with ACEs have been shown to experience both short- and long-term adverse health outcomes (e.g., high-risk sexual behaviors, poor mental and physical health, low self-esteem, and substance abuse; Dube et al., 2006; Finkelhor et al., 2015; Ratnani et al., 2015; Rojas & Coker, 2015). Thus far, most research regarding this vulnerable population has focused on exploring health-specific outcomes with less attention to other factors (e.g., developmental outcomes such as educational attainment, occupation, and family formation) that are highly correlated with well-being and quality of life. Specifically, participation in the workforce and work-related outcomes require attention because active participation in the workforce has been shown to improve individuals’ sense of self-worth and value to society, thus improving their mental and overall well-being (Harnois, Gabriel, & World Health Organization, 2000). Participation in the workforce is considered a rite of passage as a transition to adulthood.
In 2011, America’s Youth: Transitions to Adulthood report from the National Center for Education Statistics (NCES) noted that 47.1 million individuals between the ages of 14 and 24 years represented 15% of the total U.S. population. By 2025, the number of individuals between the ages of 14 and 24 years is projected to increase by 4.3 million to 51.4 million (Aud, KewalRamani, & Frohlich, 2011). Despite the increase in numbers in 2010 compared with earlier years, marked decreases in their labor force participation were identified. For example, between 1980 and 2010, workforce participation decreased from 61% to 35% for males and from 53% to 35% for females. Although an increase in continuing education enrollment and college attendance may have contributed to some of these changes, unemployment remains a particular problem for young adults, especially young people of color (Aud et al., 2011). Unemployment among Black youth (31%) exceeds that of their White, Hispanic, and Asian counterparts (ranging from 15%-21%; Aud et al., 2011). In the NCES report, it was also noted that in 2009, 21% of individuals between the ages of 17 and 24 years were living in poverty, with disparities corresponding to educational attainment, gender, and racial and ethnic identity.
The 2011 NCES report focused on individuals’ workforce participation without specific emphasis on those workers with high ACEs. Given the myriad of forces at play in their lives, the authors postulated that high-ACE individuals would more likely experience higher rates of poverty, lower education attainment, underemployment, and poorer work conditions as paid workers in light of evidence that persistent childhood poverty, itself an ACE, is associated with lower quality schools and education with poverty continuing into adulthood (Ratcliffe, 2015). As the number of high-ACE individuals increases (Finkelhor, 2009), occupational health nurses should consider factors influencing their successful transition to and retention in the labor force. Transition and retention are important because work itself has been found to be a significant factor in rehabilitation after trauma, specifically because work promotes socially productive behaviors and is a pathway to resilience (Bennett, 1970; Blank, Harries, & Reynolds, 2015). The occupational therapy literature has noted positive outcomes when employment assistance (including both job-related skills and cognitive and social skills) is provided to individuals with trauma histories or mental illness (Arbesman & Logsdon, 2011). Employee assistance programs (EAPs) have a long tradition in the United States of positively impacting substance use and abuse in the workplace and addressing work, home, and community challenges that interfere with workplace attendance and productivity (United States Department of Personnel Management). Employee assistance programs are an appropriate starting point for expanding trauma-informed care (TIC) to the workplace.
High-ACE Individuals in the Workforce: Damned if I Do, Damned if I Don’t
A cyclical conundrum for high-ACE individuals is related to their participation in the workforce. On one hand, their traumatic experiences, among other factors, often preclude them from developing the confidence and skills to engage in work and remain employed, leading to unemployment or underemployment (Johnson, 2015). On the other hand, given their likelihood of low-wage employment and high-risk jobs, these individuals are at risk for revictimization, continued exposure to traumatic experiences, and thus poor work productivity and ill health (Giovanelli, Reynolds, Mondi, & Ou, 2016; Metzler, Merrick, Klevens, Ports, & Ford, 2017).
A positive correlation has been found between ACE scores and outcomes such as substance abuse, mental health, and incarceration, each of which decreases workers’ probability of securing employment and remaining employed (Bellis, Lowey, Leckenby, Hughes, & Harrison, 2014). In addition, reports of a strong relationship between ACE scores and work-related outcomes (e.g., absenteeism [time away from work] and high likelihood of unemployment) have been published in the literature (Anda et al., 2004; Liu et al., 2013). Data from the Behavioral Risk Factor Surveillance System (BRFSS) show a grade–dose relationship between ACEs and reported outcomes such as income and unemployment (“Adverse Childhood Experiences Reported by Adults—Five States, 2009,” 2010; Centers for Disease Control, 2015). Impaired mental health and substance abuse, exemplars of ACE-associated outcomes, negatively affect work-related outcomes of absenteeism (time away from work) and presenteeism (impaired performance while at work).
In 2012, Liu and colleagues (2013) reported that high-ACE men and women reported significantly higher unemployment rates compared with those with no ACEs (p < .05). Among the 17,469 survey respondents in the study, 15% of the men and almost 20% of the women had four or more ACEs (Liu et al., 2013). Another study found that those with four or more ACEs were 2.3 times more likely to be unemployed and 1.6 times more likely to live in households reporting poverty compared with individuals with no ACEs (Metzler et al., 2017).
In their recent study of 199 Black men with history of ACEs who were seeking job services, Topitzes, Pate, Berman, and Medina-Kirchner (2016) found that exposure to ACEs hindered men’s ability to secure employment. They also found that such hindrance may be due to substance use and depressive symptoms (Topitzes et al., 2016). Such findings are not surprising given the high rates of substance abuse among individuals with high ACEs (Dube et al., 2002; Dube et al., 2006). In their study of 91 individuals who reported experiences of childhood trauma, Sansone, Dakroub, Pole, and Butler (2015) found a strong correlation between history of trauma and employment disability. Clearly, a need exists for interventions and programs to assist high-ACE individuals to not only secure but also maintain employment.
Existing Programs Assisting High-ACE Individuals’ Transition and Retention Within the Workforce
Washington State was the first state to publicly recognize the issues faced by high-ACE individuals including unemployment, financial instability, and frequent disability (Hall, Porter, Longhi, Becker-Green, & Dreyfus, 2012; Kagi & Regala, 2012). The Department of Vocational Rehabilitation was later instituted to assess high-ACE individuals with disabilities and assist them in securing employment (Washington State Department of Social and Health Services, 2016). Yet attention to the needs of high-ACE workers has not become widespread.
The authors explored the state of affairs in their own community. In Michigan, 35% of individuals, aged birth to 17 years, were reported to have one or two ACEs, and 14% reported having three or more ACEs (Sacks, Murphey, & Moore, 2014). These numbers are similar to national statistics which report that 35% of U.S. children aged birth to 17 years have one or two ACEs, and 11% have three or more ACEs (Sacks et al., 2014). Economic hardship and parental divorce or separation are the most common ACEs children in the U.S. encounter, with parental substance use problems identified as the third most common ACE (Sacks et al., 2014). Programs in Michigan have been developed to assist individuals to achieve their employment goals (e.g., Ozone House, 2016; Michigan Works Southeast, 2016; Washtenaw Community College Workforce Development, 2017). However, none of these programs appeared to be explicitly trauma-informed. Rather, these programs provide services specifically to individuals across the life span including those aged 16 years to 24 years to improve their education and skills for successful employment. In addition to the variety of ages, the individuals in these programs also varied in background and experiences. For example, some programs targeted homeless, runaway, or at-risk youth, young adults, and families. Examples of assistance that they provide include resume building, counseling, case management, food, housing, life skills, job training and coaching, paid internships, skill building in the individual’s field of interest, assistance in securing an ideal job, and general education development (GED) preparation and completion. Success stories that emanate from these programs include reports of using the money earned from internships to pay for various everyday life essentials such as food and housing.
Currently, a dearth of programs, especially in the state of Michigan, self-identify as being trauma-informed. Given that over one third of the future Michigan workforce has been identified as having at least one to two ACEs (Sacks et al., 2014), more trauma-informed and trauma-focused programs with the end goal of creating a skilled, healthy, and productive workforce are needed.
Implication for Occupational Nurse Scientists and Clinicians
Trauma-Informed Occupational Health Nursing Research and Praxis
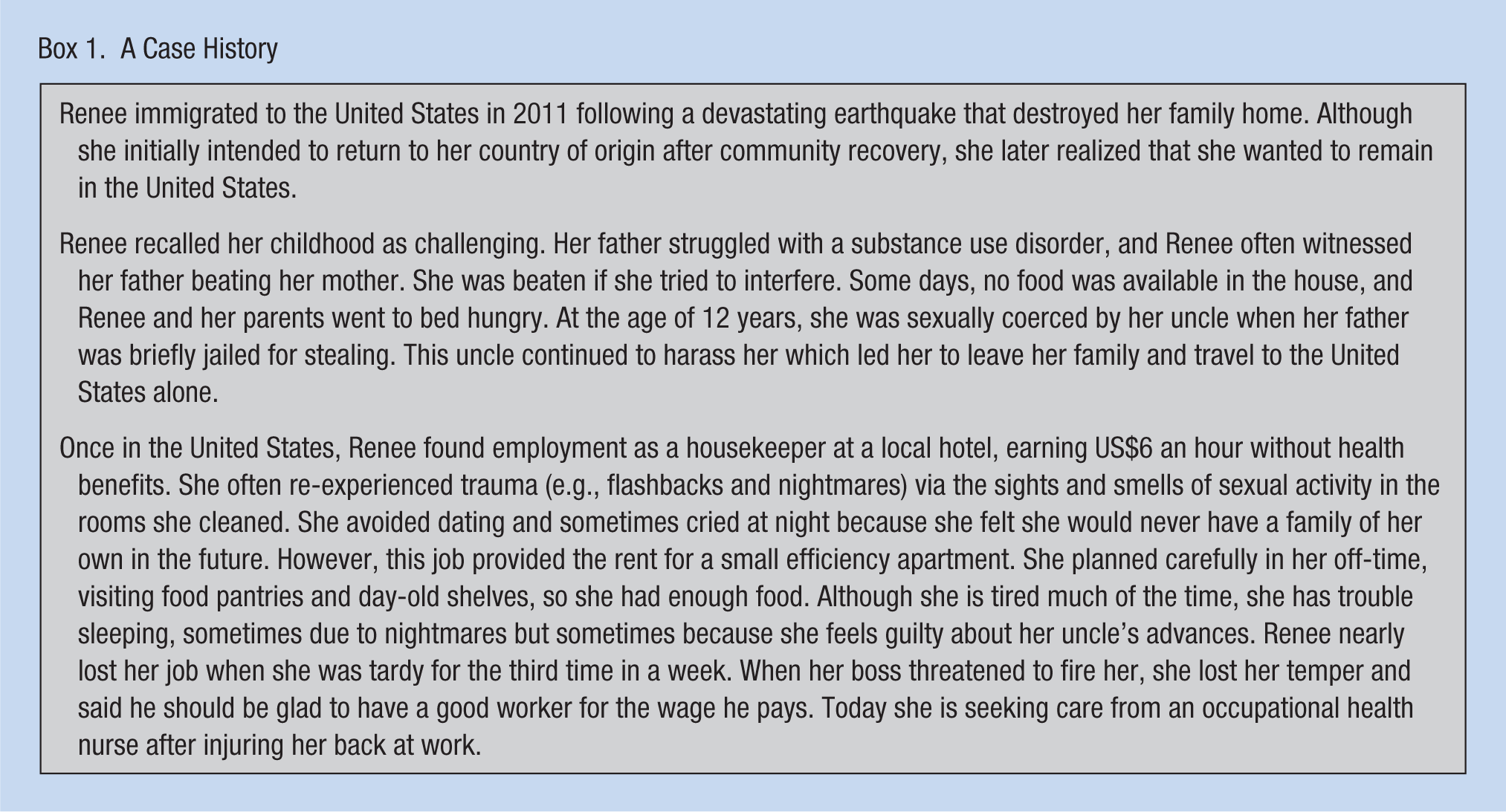
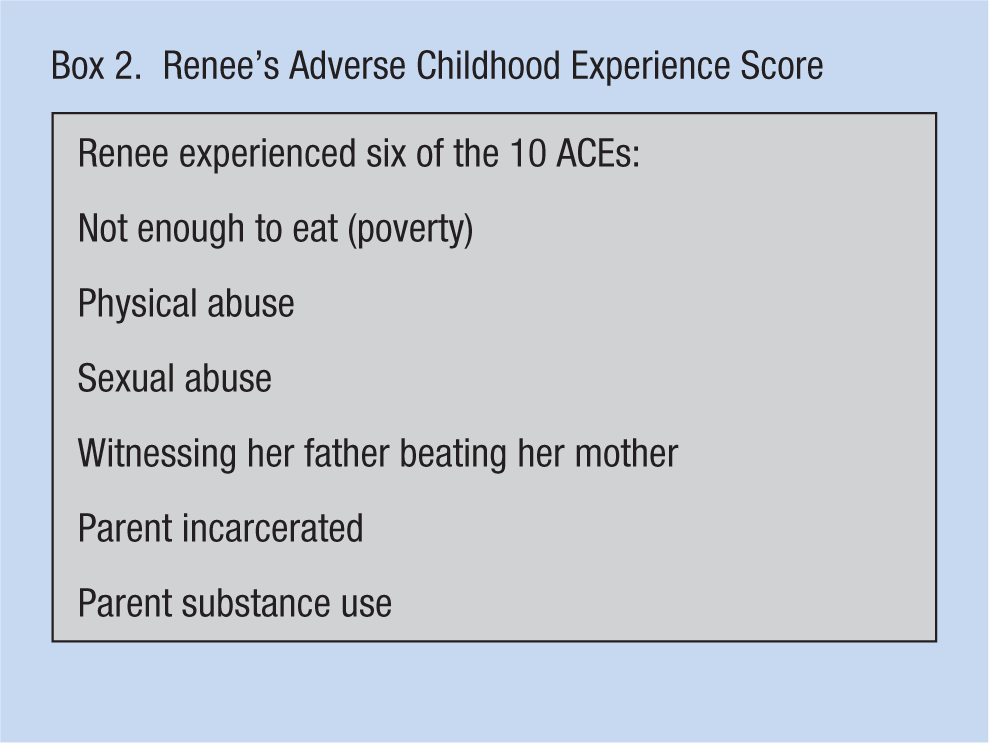
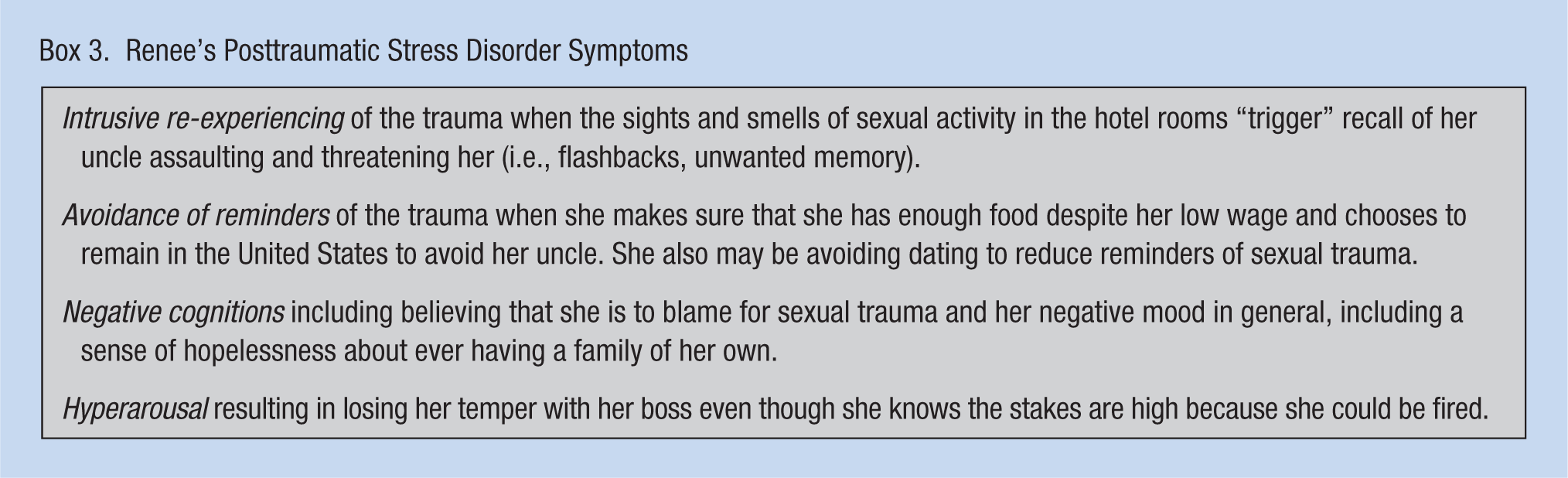
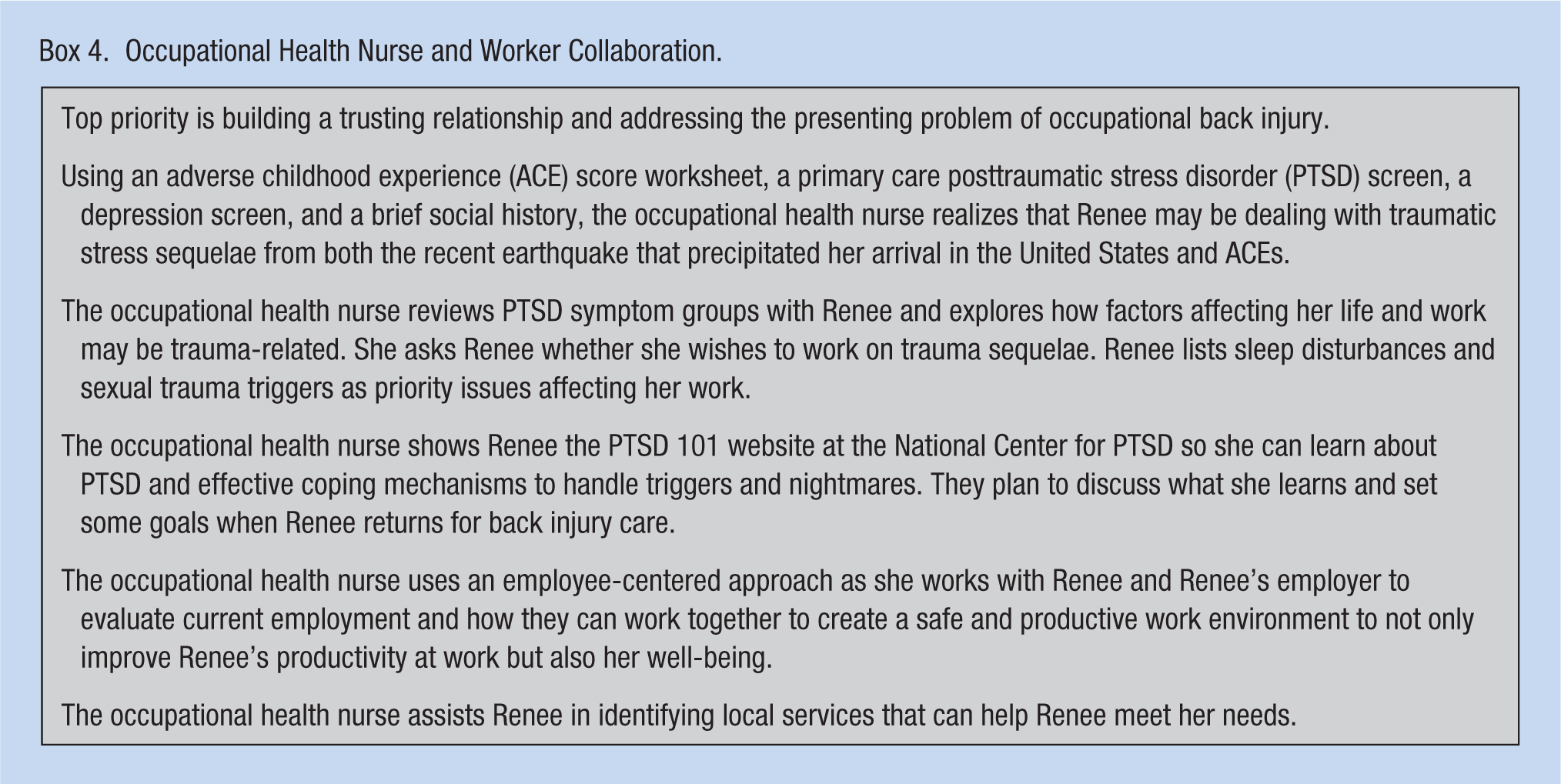
A recent review of TIC literature argued that nurses are in ideal positions to lead the paradigm shift to TIC (Munro-Kramer, Gultekin, & Seng, under review). Unfortunately, the occupational health nursing field is lagging behind the movement toward implementing a trauma-informed lens to guide research and praxis with high-ACE individuals. Trauma-informed care is important for occupational health nurses to consider because these nurses often provide care for and conduct research with individuals with high ACE scores. For example, low-wage workers may have trauma histories that include an amalgamation of abuse, neglect, witnessed domestic violence, or childhood homes and neighborhoods where parental discord or crime was prevalent. Boxes 1 through 4 showcase an example of a low-wage worker with high ACEs and possible occupational health nursing interventions.
A Case History
Renee’s Adverse Childhood Experience Score
Renee’s Posttraumatic Stress Disorder Symptoms
Occupational Health Nurse and Worker Collaboration.
With increasing evidence of the devastating effects of ACEs on individuals’ health- and work-related outcomes, occupational health nurse clinicians and researchers are called upon to address the needs of high-ACE workers. As noted by Tsai and Salazar (2009), “Occupational health nurses are in a prime position to recognize, identify, and respond to at-risk workers” (p. 425). These individuals are likely to seek or require more health care services related to chronic physical and mental health conditions associated with high ACE scores than their low- or no-ACE peers (Arbesman & Logsdon, 2011; Center for Substance Abuse Treatment, 2014); thus occupational health nurses are likely to interact with these individuals more than low- or no-ACE workers. In addition, occupational health nurses may enhance successful posttrauma rehabilitation of workers experiencing chronic posttraumatic distress and impaired functioning. This support also can be applied to those experiencing acute traumatic stress after a recent trauma exposure (e.g., sexual assault, sexual harassment on the job, injury, or criminal victimization) that might otherwise derail an already vulnerable worker.
The current approach in occupational health nursing focuses on workers’ socioeconomic, political, and cultural context with less attention to traumatic experiences that occurred during earlier years of life (ACEs). Yet ACEs are associated with long-term debilitating physical, mental, and behavioral outcomes, all of which correlate with ability to secure work and performance at work. One occupational health and safety goal is to promote a healthy workforce and ensure that individuals can function at their maximum occupational capacity, achieving high productivity. In addition, research guided through a trauma-informed lens aligns well with the goals and research priorities of occupational health nursing (Rogers, 1989). Thus, assuming a history of ACEs and developing workplaces that are trauma-informed should be embedded in the occupational health nursing approach.
Commonly Used Models in Occupational Health Nursing
In considering how TIC fits within occupational health nursing practice, nurses should consider the theoretical models that already inform practice and research. The ecological systems model (Bronfenbrenner, 1979), for example, emphasizes the multiple levels of influence that shape individuals and their environments (Salazar & Primomo, 1994). The ecological systems model acknowledges that growth and development occur within nested spheres of influence over time; aspects of health and behavior must be considered the contextual lenses. Occupational health nurse clinicians providing care for young workers with histories of childhood trauma need not only explore workplace exposures and address workplace safety issues but also explore other factors that may impact individual health and behaviors both at the workplace and in the community. In providing care to this group of individuals, nurses must address prior and ongoing exposure to ACEs and how ACEs and their effects (e.g., substance abuse, mental health symptoms, physical health status, sleep disturbances, angry affect) may impact work (e.g., workplace safety practices and attendance). The model aligns well with another key framework that may serve as a familiar starting point for addressing occupational health among workers with high ACE scores, the Total Worker Health (TWH) initiative.
TWH Initiative and High-ACE Workers
The National Institute for Occupational Safety and Health (NIOSH) instituted the TWH initiative as a framework to advance worker well-being. In 2015, TWH was defined as policies, programs, and practices that integrate protection from work-related safety and health hazards with promotion of injury and illness prevention efforts to advance worker well-being. (Schill & Chosewood, 2016, p. 4)
Total Worker Health uses the hierarchy of controls (e.g., encourage, educate, redesign, substitute) that call for an integrative approach at the organizational level (i.e., workplace) and other social systems that can impact workers’ well-being.
Given the TWH’s emphasis on a holistic approach (i.e., employer-work and community environment), nurse clinicians and researchers should explore how factors such as exposure to ACEs impact workers’ overall health and ability to achieve occupational productivity. Such an approach is not only beneficial to employees but to employers as well. Untreated childhood trauma, or ACES, have been shown to result in lost productivity stemming from mental health problems (Eastern Iowa-Western Illinois Trauma-Informed Care Consortium, 2011). Lost productivity costs employers over US$150 billion annually (Eastern Iowa-Western Illinois Trauma-Informed Care Consortium, 2011). Moreover, work absenteeism related to anxiety, depression, and substance abuse cost employers US$125 and US$246 billion, respectively (Eastern Iowa-Western Illinois Trauma-Informed Care Consortium, 2011). Costs continue to increase (e.g., liability claims) when employees ignore safety practices because they are distracted or impaired at work (Eastern Iowa-Western Illinois Trauma-Informed Care Consortium, 2011).
Total Worker Health has several implications for occupational health nurses (Campbell & Burns, 2015; Schill & Chosewood, 2016). Occupational health nurses’ scope of practice and research expands to a systems level, focusing not only on workers but also on employers and communities at large.
The TIC paradigm can be symbiotically applied within the TWH framework given several overlapping factors. For example, both frameworks emphasize the importance of promoting psychological health and the need to eliminate factors that minimize social inclusion and sense of contribution to society (NIOSH, 2016; Substance Abuse and Mental Health Services Administration [SAMHSA], 2014b). Examples of these factors include history of trauma, factors that increase absenteeism, and other behavioral issues that mirror heightened stress and limit resilience and coping skills. In addition, both frameworks (TIC and TWH) emphasize the prevention of community and workplace trauma that could retraumatize high-ACE individuals due to their heightened reactivity. Examples of workplace retraumatization include social exclusion, workplace violence, or other cumulative psychologically disturbing aspects of work (e.g., demeaning work conditions, prejudice, unclear job expectations, lack of control, excessive workloads, mistreatment from coworkers and supervisors, and job insecurity; NIOSH, 2016; Schill & Chosewood, 2013)
Trauma-Informed Occupational Health Nursing Approach
Trauma-informed occupational health nursing practice requires attention to the guiding principles of TIC. The National Center on Trauma-Informed Care (NCTIC; 2017) provides expert guidance and technical assistance on implementing TIC in health and human service organizations. The six fundamental principles of TIC include the following:
Establishing organizations that provide physical and psychological safety for all individuals seeking care,
Developing organizational standards that promote trustworthiness and transparency between providers and their clients,
Developing an organizational culture that promotes collaboration and mutuality,
Recognizing and building upon client strengths and decision-making capacity through empowerment, voice, and choice,
Peer support and mutual self-help,
Taking into consideration cultural, historical and gender issues (SAMHSA, 2014a).
Occupational health nurses must consider the “3 Es” of trauma experiences: the event that inflicts traumatic stress, the subjective experience of trauma (i.e., not all trauma is experienced in the same way by all individuals), and the effects of trauma or traumatic stress (SAMHSA, 2014b). This understanding of trauma and traumatic stress is then applied to interactions with clients in a universal approach to care that is consistent with the “4 Rs” where trauma is
recognized as a broad range of experiences with
realization that trauma has a lasting impact on individuals and their well-being (SAMHSA, 2014b).
The health care provider must
respond to trauma by integrating awareness and recognition of traumatic stress into their interpersonal practice, and
resist retraumatization of clients by being attentive to and avoidant of power dynamics and body intrusions that may revicitimize a client.
For vulnerable workers (e.g., low wage as presented in the case example earlier in the article), nurses must provide supportive services that recognize the potential existence of trauma in their lives and the impact of trauma on workers’ physical, mental, and functional well-being. Assuming trauma could be an issue in all interactions with clients will ensure that those workers who are most vulnerable are protected and those who have not been impacted by traumatic stress understand that they have a safe place to address and manage whatever traumatic stress they may encounter in the future. Occupational health nurses must work with employers and employees to recognize and reduce potential triggers for retraumatization in the workplace, including acts of harassment, workplace violence, and racism. The benefit to both employees and employers include potential for cost savings by reducing presenteeism and absenteeism. As proposed by the National Center on Domestic Violence Trauma & Mental Health (National Center on Domestic Violence Trauma & Mental Health, 2011) in interaction with and research with vulnerable workers, occupational health nurses should
consider history of trauma
be knowledge of and provide workers with information about mental health services
discuss feeling safe at work
explore job history including difficulties encountered in previous jobs and coping mechanisms
discuss concerns or fears about starting employment or returning to work
explore possible triggers at work (e.g., violence, racism, sexual harassment) and discuss possible ways to address those triggers
work in partnership with employers and high-ACE workers to design, implement, and maintain safe workplace environments (Schill & Chosewood, 2016)
embrace TWH in partnership with employers and employees to advocate for a holistic understanding of all factors (including trauma history) that contribute to worker health and safety (Campbell & Burns, 2015)
Occupational health nurses can use specific tools when working with high-ACE workers. Roy and Perry (2004) conducted an extensive review of the literature and provided tables with both observer and self-rated instruments to assess for ACEs among adults. Examples of such tools include the retrospective childhood questionnaire for adults (CECA.Q [Childhood Experience of Care and Abuse Questionnaire]), the Childhood Experience of Care and Abuse Interview (CECA; Bifulco, Brown, & Harris, 1994), the Life Experience Questionnaire, and the Life Events Checklist. Each of these instruments has been validated and used in published research.
Conclusion
Adverse childhood experiences (ACEs) affect individuals throughout their lives (Larkin, Shields, & Anda, 2012). In addition to physical and mental outcomes, financial stability remains a major challenge for this population. Workforce participation is specifically of concern. High-ACE individuals often face poor mental health, low-self esteem and confidence, limited education, substance abuse, and incarceration, all of which are precursors for unemployment and underemployment. To that end, a paradigm shift is needed; a trauma-informed lens could impact the quality of both occupational health nursing research and praxis.
In this article, the authors examined local Transition to Work programs for vulnerable individuals and assessed whether they were trauma-informed. Much work is needed to promote trauma-informed employment services to high-ACE individuals. Given their multitude of challenges, simply training high-ACE individuals on skills such as resume building and interviewing will not suffice. Mental and behavioral support services also must be embedded in the programs. Occupational health nurses have a role in building workplace health and safety programs that include assessments and interventions to identify and manage the sequelae of ACEs and traumatic stress.
Footnotes
Acknowledgements
The authors acknowledge the CAsCAid (Complex ACEs, Complex Aid) faculty group at the University of Michigan School of Nursing for their support and encouragement in manuscript preparation. All three authors are members of CAsCAid, with funding for the work group provided by the University of Michigan School of Nursing’s Dean’s Centennial Seminar Series.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Marie-Anne Rosemberg is an assistant professor at the University of Michigan School of Nursing. She has training and expertise in occupational health nursing. Her work focuses on optimizing the health of low-wage workers.
Laura Gultekin is an assistant professor at the University of Michigan School of Nursing. Her work focuses on high-ACE homeless individuals.
Michelle Pardee is a clinical assistant professor at the University of Michigan School of Nursing. Her work focuses on trauma-informed care among high-ACE adolescents.