
Abstract
The prevalence of non-communicable diseases is high globally and in the Americas. This study aimed to evaluate nursing and dietetics students from the Americas with a survey about non-communicable diseases and the use of both conventional and lifestyle healthcare approaches to address these conditions. It also sought to identify specific demographic, academic, and psychographic characteristics that influence students’ overall survey response outcomes. In a cross-sectional multi-center study design, an electronic questionnaire was developed with specific demographics along with objective and psychographic parameters related to non-communicable diseases and integrated healthcare approaches. It was pilot-tested and utilized to survey a convenience sample of targeted students from 3 universities in the United States of America and the Caribbean region, including extension campus sites. Responses from 298 students were coded, scored, and analyzed using descriptive statistics, Chi-square tests, Kruskal-Wallis tests, Dunn-Bonferroni Multiple Comparisons post hoc tests, and Binary Logistic Regression analysis. Most respondents were female undergraduate nursing majors aged 20 to 24. Dietetics majors, graduate/postgraduate students, Hispanics, and students enrolled at specific campus sites, obtained significantly higher total survey scores than others. High total scores were significantly influenced by knowledge and psychographic characteristics. Response outcomes were significantly influenced by students’ specific healthcare discipline, ethnicity, the availability of lifestyle-inclusive graduate or post-graduate curricula, the strength of undergraduate training programs, and enrollment at campuses in specific geographical locations. Nutrition and health-related knowledge along with healthcare perception, perspective, and practice parameters, contributed significantly to survey responses in favor of integrated lifestyle and conventional healthcare approaches.
Keywords
Introduction
The epidemiological reports about non-communicable diseases (NCDs) around the world are very disconcerting, especially in certain regions. 1 In the Region of the Americas for example, NCDs are the leading causes of death and disease burden. 2 This region includes Latin America, the Caribbean, and North America. The 4 main groups of NCDs include heart diseases, cancers, respiratory diseases, and diabetes, which accounted for over 80% total deaths or 5.8 million deaths in the Americas in 2019. 2 Some of the most common risk factors of NCDs are unhealthy diets, physical inactivity, and alcohol and tobacco use, which are all lifestyle-related. These factors together with air pollution and inadequate sleep increase the development of other conditions such as respiratory disorders, obesity, hypertension, and stress. This adds to the strain of chronic ailments that clinicians, government officials, health agencies, professional health associations, and policy makers have been battling for decades.
Conventional medicine has been the more mainstream or predominantly used healthcare approach for NCDs, particularly in Western societies. It is a system of healthcare in which medical doctors and other healthcare professionals such as nurses, pharmacists, and therapists treat symptoms and diseases using drugs, radiation, or surgery. 3
However, lifestyle approaches have been found to be particularly useful in addressing conditions such as obesity, diabetes, heart disease, and some cancers through the years. 4 This approach uses therapeutic lifestyle interventions as a primary modality to treat chronic conditions by applying 6 lifestyle pillars. These include a whole-food plant-predominant eating pattern, physical activity, restorative sleep, stress management, avoidance of risky substances, and positive social connections. 5
The approach is sometimes used alone without complementary or integrated efforts. At other times when an attempt is made to utilize the approach along with conventional methods, it is seemingly done without sufficient or professional knowledge and training in the field.6 -8 Some have also pursued the integration of approaches without consultation or referral to a more qualified interdisciplinary team or member with the requisite competencies. 9 Oversight, remuneration issues, lack of knowledge, individual attitudes, biases, and personal beliefs concerning one approach in relation to the other, may have all contributed to this reality. The desired integrated lifestyle and conventional approach involves inclusion of lifestyle elements in conventional curricula and training, and collaboration of professionals from both disciplines in healthcare practice.
The scope of healthcare practice describes the services that a qualified health professional is deemed competent to perform, and permitted to undertake in keeping with the terms of their professional license. Nurses and dietitians are common examples of healthcare counterparts who are independently trained in their respective conventional or lifestyle approaches. The American Nurses Association believes that patients’ interests are best served by a healthcare system in which many different types of qualified professionals are available, accessible, and working together collaboratively. 10 The main functions of nursing are patient evaluation, medical management, wound care, controlling infections, education, and health promotion. The scope of dietetics is usually guided by evidence-based research and the standards for nutrition and dietetics professionals. 11 Their emphasis of practice incorporates food, nutrition, and medical nutrition therapy, utilizing the nutrition care process.
Members of the 2 disciplines already work together in some clinical settings with an integration of certain discipline-specific practices. For example, dietitians are required to know about certain medications because of possible food-drug interactions,12 -14 and nurses and other medical practitioners are expected to advise on lifestyle behaviors like diet modification and physical activity as a first or concurrent approach to address and control conditions like pre- and type-2 diabetes. 15 But more comprehensive healthcare integration and collaboration are needed in clinical training and practice.
Statement of the Problem
The high prevalence and incidence of NCDs across the globe, and the burden of its existence in regions like the Americas necessitates healthcare team collaborations and specialized training. It has therefore become necessary to address the potential for interdisciplinary integration of conventional and lifestyle-intensive approaches early in the healthcare training process, to ensure that patients experience the full benefits. In some regions, including the Americas, the full potential and contribution of nutrition and lifestyle components in patient care are not always recognized, valued, or adequately incorporated in healthcare curricula, professional practice systems, or policies.16 -19
Rationale of Study
The environment of academia and training in healthcare provides the earliest formal applications for conventional and lifestyle approaches, and the desired integration of the same. Surveys and surveillance of relevant students and academic programs at different universities might be needed in order to gather necessary information that can be used to positively impact desired integrated practice 20 and healthcare policies.
Socio-demographic factors can influence students’ knowledge and impressions about different kinds of healthcare approaches, including non-conventional ones.21,22 These factors may include educational experience, cultural background, race or ethnicity, age, gender, religion, and income. Additionally, psychographic impressions such as clinicians’ attitudes and beliefs can influence the implementation of lifestyle risk factor management in primary healthcare. 23
According to Schrader and Lawless, 24 knowledge along with psychographics such as perception, perspectives, and practice, can impact the performance outcomes of students. These parameters are typically measured using individual scores. However, these researchers conclude that because the relationship between knowledge, attitude, and behavior constructs is dynamic and sometimes even reciprocal, there is benefit in conducting some research from the perspective that these dimensions can and do interact. 24 As such, the combined or overall score measure can also be successfully used for evaluation.
Current Study Objectives
To evaluate nursing and dietetics students from the Americas with a survey about non-communicable diseases and the use of both conventional and lifestyle approaches to address these conditions.
To identify specific demographic, academic, and psychographic characteristics that influence the students’ overall survey response outcome.
The authors are unaware of any other study having the same objectives or focus.
The Multi-Center Context
This study is unique as it provides opportunity for using total survey score as our main outcome parameter to represent overall potential for integrated lifestyle and conventional healthcare in the current context of both student disciplines. It is conducted within a multi-centered context at 3 universities where both nursing and dietetics programs are offered along with other health or nutrition-related programs. One university has only undergraduate programs, while the others have both undergraduate and graduate or postgraduate programs. All 3 universities have a main campus and extension sites. The enrolled nursing students outnumber other healthcare disciplines, including dietetics, at all the main campuses.
The main and extension campus sites are in different geographical locations, including the United States and in more than one Caribbean island. Different proportions of ethnicities are represented at each site, but there are cultural similarities for 2 of the sites. The university locations targeted in the study are part of the Americas, a region with high non-communicable disease prevalence and death rates.
Methods
Study Design
This was an original study involving a cross-sectional multi-center design which utilized a de novo-developed online questionnaire to survey the target student population.
Questionnaire Development
The online survey was developed using Google Forms, and designed for healthcare students, including undergraduates, interns, graduates, postgraduates, and registered practitioners pursuing further education. It includes an informed consent section, clear instructions for completion, a demographic section, and the healthcare and evaluation section. The consent section also includes a brief description of the study, the purpose and benefits of the study, the survey process and dates, a statement of confidentiality, the assurance of no risk to participants, and explanation of the voluntary nature of the study, allowing participants to discontinue at any time if they so choose. A consent button is provided below the statement of consent, which required participants to indicate their consent before being allowed to proceed to the demographic survey section.
The demographic section was designed to gather information on age, gender, religion, race/ethnicity, university affiliation, academic program/discipline, academic year/level status, and full-time/part-time student status combined with mode of class delivery (ie, online, face-to-face, or blended). The main section of the survey outlined objective or knowledge items and psychographic items (eg, attitudes, values, perceptions, behaviors, etc.) related to health, nutrition, and integrated lifestyle and conventional healthcare approaches.
The survey questions are not based on any pre-existing survey. They were generated by the research team with suggestions from colleagues in the targeted career fields, and then finalized by pilot-testing. They are also based on literature review of information germane to the study’s objectives.
Pilot-Testing and Questionnaire Refinement
In order to evaluate the effectiveness of the survey questions, the questionnaire was pilot-tested on a small sample (n = 24) of the targeted student population from the select universities, and was proof-read by educators in the targeted career fields. Cronbach’s alpha was then used to assess the internal consistency of the survey.
Ethical Procedures and Institutional Approvals
The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) cross sectional reporting guidelines, was used as a checklist for the study protocol. 25
All necessary School or Department permissions and approvals from the Institutional Review Board or Ethics Committee of the participating universities, were obtained. Consent was electronically obtained from all participants.
Participants
Eligible participants were 18 years or older, and enrolled in either nursing or dietetics programs; or were already registered and practicing nurses or dietitians who were doing continuation education or higher degrees in their career field, or another public health or human ecology field, at 1 of the 3 universities. Figure 1 provides the campus site structure of the universities.

Campus sites structure of participating universities.
Recruitment, Sampling, and Data Collection
Promotion of the study was done using a flyer sent via email, shared in classes, or posted on Learning Management Systems. Recruitment and participants’ access to the survey were done using convenience sampling. An emailed link or QR code was sent directly to students via the official communication offices of the specific University Schools, Faculties, or Departments. Students were then free to voluntarily complete the questionnaire. Response data were collected from March 2024 to July 2024.
Data Management and Statistical Analysis
Completed responses were imported to a Microsoft Excel Spreadsheet and examined before copying to an IBM Statistical Package for Social Sciences (SPSS) version 30 file. Recoding of relevant variables for clearer interpretation, labeling of missing data, scoring of question responses, and various statistical analyses were then performed.
Demographic information and other relevant attributes were analyzed using summary statistics including means, medians, standard deviations, and frequency distributions. Chi-square test of independence was used for examining associations between categorical demographic variables and attributed category levels of total survey scores. The Kruskal-Wallis H test along with Dunn-Bonferroni Post Hoc Multiple Comparisons adjustment tests were used to identify the specific influencers of statistically significant variations between student demographics and total survey scores. Binary Logistic Regression was used to evaluate the contribution of the students’ objective and psychographic score levels to total survey score.
Results
The Research Instrument
Based on the pilot-test results, some questions were revised for clarity to improve participant understanding and response accuracy. A final 40-item online survey with 8 demographic items, and 32 nutrition, health and healthcare evaluation items, was generated. A Microsoft Word-version of the electronic Google Form survey is available as Supplemental Material.
Recategorization of some demographic questions was done for analysis. Various question types were used for objective and psychographic items including True and False, Likert Scaled, Single Choice, and Multiple-Choice questions; and were coded for correct versus incorrect or more desirable versus less desirable interpretation and analysis. An overall Cronbach’s Alpha of .61 and a standardized items alpha of .7 (n = 32) were produced.
Scoring involved summing responses. Incorrect or less desirable responses had a score of 0, while correct or desired responses had a score of 1 for True and False and Single response answers. Questions requiring choice of more than 1 response were scored based on the number of correct responses chosen. Total survey score was the main outcome measure used based on the interactive complexity of the different constructs. 24 A high total score indicated responses that were more in favor of integrated healthcare approaches. The total possible survey score was 42.
Final Study Participants
At the time of the study, the total number of eligible students enrolled in the relevant Schools, Faculties, and Departments at the 3 universities combined, was reportedly 2033+. A calculated sample size was not used because the sampling frame for a specific nursing major at one of the universities was not readily made available.
Responses from the 298 students who completed the survey were examined for usability and then analyzed. For all participants, the inclusion criteria were fulfilled and missing response data were found to be less than 5% (ranging from 0% to 3%) per different variables.
Table 1 shows the frequency and percentage distribution regarding the socio-demographic characteristics of the participants. The number of participants from each of the 4 sites ranged from 15 (Campus B2) to 120 (Campus A). The majority of participants were Black, under 30-year-old female nursing students who were attending full-time face-to-face undergraduate classes at either Campus A or B1.
Socio-Demographic Characteristics of Study Participants.

Socio-demographics & Psychographics with Total Survey Scores
Among selected socio-demographic groupings, higher mean scores were obtained by:
Campus C (33.7)
Dietetics students (33.2)
Graduate/Postgraduate students (33.6)
25 to 34-year-old students (33.3)
Hispanics (34.4)
The non-demographic survey items summed to a possible maximum total score of 42. The highest score obtained by the students was 38, which 4 (1.3%) of the students obtained. Figure 2 shows the scaled score distribution.
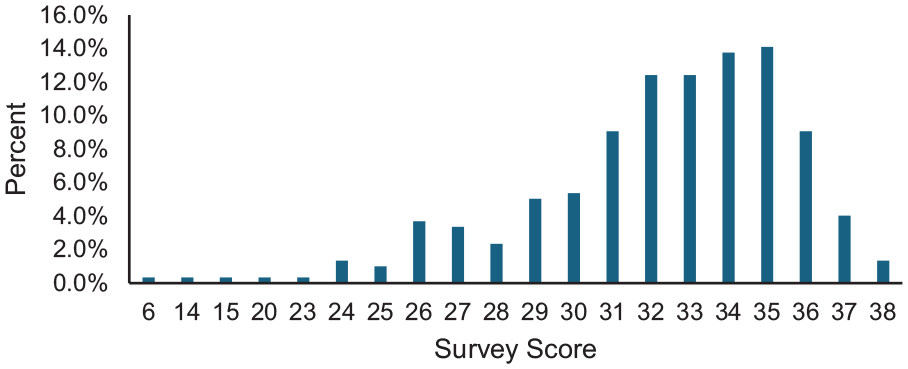
Distribution of students’ total survey scores.
Total survey score was also given criterion-referenced attributed levels based on the least conservative academic grade-scale used among the universities: Good/High = 33-42 (≥79%); Fair = 23-32 (≥55% <79%); Poor = 1-22 (<55%). Figure 3 shows the overall levels of the students’ score performance. Chi-square test results of poor to fair score levels versus good score levels with participants’ socio-demographic characteristics, and Kruskal-Wallis analysis of participants’ scaled scores, are presented in Table 2.

Students’ total survey score levels.
Chi-Square and Kruskal-Wallis Analyses of Total Survey Score Levels and Ranks With Select Student Attributes.

χ2 = Chi-square Test Statistic with at least 80% cells having expected counts of 5 or more.
H = Kruskal-Wallis Test Statistic.
P-value is less than .001.
P-value is less than .01.
P-value is less than .05.
With alpha levels of less than .05, the Chi-square post hoc tests showed that significantly higher percentages of students with good/high score levels were obtained by:
Campus B2 and Campus C (73.3% and 74.2%, respectively) versus other sites
Graduates and postgraduates (70%) versus undergraduates (53%)
Nutrition and dietetics students (64%) versus nursing students (50%)
Significant differences were also observed in the percentage of students from the different races/ethnicities who scored above the poor-to-fair level (1-32): East Indian (59%), Black/African descent (39%), Caucasian (77%), Hispanic (91%), Asian (82%), Mixed Race (58%), and Other Races (80%).
Dunn-Bonferroni Post Hoc Multiple Comparison Tests revealed the following additional information from the ranked Kruskal-Wallis data scores:
Campus C obtained a significantly higher total score rank than students from Campus B1 (+62.01, P = .000) and Campus A (+53.41, P = .000).
Students of African descent (Black) obtained a significantly lower total score rank than Hispanic students (−84.209, P = .024), Caucasian students (−78.822, P = .008), and Asian students (−72.884, P = .005).
Nutrition and dietetics students obtained significantly higher total score ranking than nursing students (+32.91, P = .002).
Collectively, graduate and postgraduate level students obtained a significantly higher total score rank than undergraduate level students (+41.74, P = .002).
Year 1 Freshman students obtained significantly lower total score rank than graduate/postgraduate students (−92.481, P = .001).
Year 3 Junior students (−73.864, P = .040), Year 3 Final-year students (−80.320, P = .037), and Year 4 Senior students (−76.905, P = .033) also obtained significantly lower total score rank than graduate/postgraduate students. But interestingly, the total scores of Year 2 students were not statistically different from graduate/postgraduate students (−72.93, P = .054). This was an unexpected outcome.
Graduate/postgraduate score ranking was not significantly different from already practicing professionals and interns (ie, students in on-the-job training programs, and registered nurses and dietitians). Most of the already practicing professionals were in fact also enrolled as graduate or postgraduate students.
Healthcare and Evaluation Contributors to Total Survey Score Levels
Binary Logistic Regression of total survey score levels (low to fair vs high) revealed a 67% Nagelkerke Pseudo R-square contribution of objective and psychographic categorical characteristics (lifestyle and integrated healthcare knowledge, perception, perspective, and practice score levels). Table 3 highlights these findings.
Binary Logistic Regression Healthcare & Evaluation Contributors to Total Survey Score Levels.

Note. Reference Category is High/Good/Desirable Total Score Level.
OR = odds ratio.
Knowledge Levels: Low (0-10) to Medium (11-15) versus High (16-20).
Perception Levels: Low (0-2) versus High (3-4).
Perspective Levels: Low (0-2) to Fair (3-5) versus High (6-8).
Practice Levels: Poor (0-2) to Fair (3-5) versus Good/Desirable (6-10).
P-value is less than .01.
P-value is less than .001.
It was observed that high knowledge score levels increased the odds of being grouped among students with high total survey score levels by 51.
For the perception, perspective, and practice levels, the odds of the same grouping probability were increased by 6, 23, and 18, respectively.
Discussion
The Lifestyle-Inclusive Healthcare Approach
The call for primary healthcare workers to be more appropriately trained in various aspects of lifestyle approaches is not a new endeavor. 26 Introducing complementary lifestyle elements within the conventional curricula can have a very positive influence on future practice, along with interdisciplinary healthcare team collaborations.
Among the various lifestyle factors that impact health, good nutrition, increased physical activity, stress management, adequate sleep, and avoidance of alcohol and tobacco, all play critical disease prevention and healthcare roles.1,27 The current study survey was designed to highlight these lifestyle factors and the integrated healthcare approach.
Types of Survey Question Measures
The research team sought to identify demographic, academic, and psychographic characteristics that impact the targeted students’ overall score results from a de novo questionnaire. Questions focused on nutrition, lifestyle, and integration of associated healthcare approaches pertaining to NCDs. Similar to Schrader and Lawless’ findings in their comparison of 12 studies, 24 the current study used a variety of question types to evaluate socio-demographic, knowledge, and psychographic constructs such as perception, attitude, and practice.
Overall Findings
Fifty-five percent of the students obtained high total survey scores of 33 to 38 out of a possible maximum of 42. Knowledge, significantly contributed to high total scores. Perspectives, practice, and perception also contributed, but to a lesser extent. Significant association was observed between total survey score and demographic factors such as specific healthcare career/degree program, year/level of academic exposure, enrollment at specific campus sites in certain geographical locations, and race or ethnicity.
Career Discipline/Degree and Integrative Healthcare Approach Potential
In the current study, dietetic students obtained higher total scores than nursing students.
Perspective and Perception Contributions to Career Discipline Score Outcomes
In terms of psychographic contribution to this outcome, 55% of both nursing and dietetics students in our study obtained high perspective scores. Various other studies have also reported positive attitudes toward complementary healthcare, which includes major nutrition and lifestyle-intensive components. van Rensburg et al conducted a study on nursing students’ attitude toward complementary medicine. 28 They observed positive attitudes and an openness to enhance knowledge in the area. Similarly, Poreddi et al, also observed that nursing students had positive attitudes toward complementary and alternative therapies. 29 In a review of Midwestern University student dietitians’ perspective on complementary medicine, Novotny and Novik also reported positive attitudes. 30 Their study concluded that complementary medicine should be made available in practice, and be integrated with conventional medicine. Unlike most of these studies, however, the research design of the current study used interdisciplinary comparisons.
While no difference in perception was observed between the nursing and dietetics students about the integrated healthcare approach, the latter obtained higher perspective scores (not shown). One likely explanation for this is that dietetics students have greater academic exposure to and understanding of the lifestyle approach. This can also hold true for students and professionals of any discipline in their own sphere, which typically has a more positive effect on attitudes. 31
Knowledge and Practice Contributions to Career Discipline Score Outcomes
High percentages of this study’s participants obtained good knowledge scores (75%) and potential practice scores (84%) with dietetic students obtaining significantly higher knowledge scores than nursing students (not shown), but similar actual/potential practice scores. These 2 disciplines usually have both theory and varying degrees of practical training components throughout all levels of study, but with very different scope and focus.
This difference is very apparent in the report by researchers who conducted a national survey on faculty about students’ performance in existing nursing programs. They found that the majority of the programs met the requirement for nutrition education outlined by the National Research Council but lacked training in chronic ambulatory nutrition. 32 In another study, the administration of tube feeding in Jordan private hospitals showed that nurses had high scores for responsibility and documentation, but limited knowledge about enteral nutrition and expressed the need for such training. 33 Chepulis and Mearns focused on knowledge gaps. 34 Their nursing participants had low mean scores. They recommend that in order to provide intervention for conditions like obesity, nutrition education and effective training are essential for the preparation of nursing students.
While nurses may be taught to recognize the importance of nutrition in overall health and disease prevention, it is not their primary focus. 35 Even when nutrition knowledge is integrated into nursing curricula, it lacks the requisite training for detailed, personalized nutritional counseling or interventions. For example, nursing students do not typically develop deep knowledge about macronutrient management, dietary patterns, or specific dietary modifications for different lifestyle disease conditions. 36 They would more than likely refer patients to nutrition professionals. Therefore, whether via referral or curricula, integrated efforts can be beneficial. A study was conducted in Finland to assess the effectiveness of an interprofessional diabetes management education intervention with nursing students. It demonstrated an improvement in diabetes knowledge and the ability to provide diabetes education to colleagues and patients. 37
Academic Year or Level and Integrative Healthcare Approach Potential
Total survey scores and knowledge scores (not shown) were significantly lower for students completing undergraduate programs than those completing higher level degrees. This was also seen with students at the first year or Freshman level compared with successively higher-class levels, except Year 2.
Possible explanations for the unexpected year 2 outcome include: the majority (56%) of Year 2 students were dietetics majors; most may have been high-achievers with strong academic foundations; the fact that exposure to core nutrition curricula content at the universities becomes more comprehensive from year 2, which would have overlapped with the concurrent information; and for dietetics majors, the survey content was aligned with their career interests.
Knowledge Contribution to Academic Year or Level Score Outcomes
Some researchers suggest that it might be beneficial to adjust undergraduate nursing curricula to enhance nutrition knowledge. 34 This suggestion concurs with Almomani et al’s study of undergraduate students concerning their knowledge about chronic non-communicable diseases. 38 The suggestion is also useful for the participating universities in the current study since the campus site with students who scored comparatively low, currently has no graduate or postgraduate curricula. This may explain the consistently higher score performance from the university with the majority of enrolled master’s and doctoral students who participated. It should also be noted that in some countries, students studying Nutrition & Dietetics are required to have a Master’s degree in order to meet the eligibility criteria to become a registered dietitian.17,39
Race /Ethnicity and Integrative Healthcare Approach Potential
Findings from the current study seem to suggest that cultural background in terms of geographical location, ethnicity or race, and environmental influences, may play an important role in the study’s outcome interest. The study comprised of students from North America and different Caribbean islands that may have either developed Western diet trends or maintained more whole food, or traditional dietary choices. Campus B1 and Campus A are located in closer proximity to each other than the other campus sites, and consistently exhibited similar results.
Knowledge and Perception Contributions to Race/Ethnicity Score Outcomes
The largest ethnic group among participating students was Black students, and the majority of Black, East Indian, and Mixed students, were undergraduates. This academic level unsurprisingly exhibited lower scores than graduates/postgraduates. But at the highest performing university, 80% of the Black students obtained high scores. Furthermore, that campus site emphasizes healthy diet patterns, preventative healthcare, and wellness programs.
Belogianni et al indicated that students from minority ethnicities may exhibit lower nutrition knowledge scores compared to Caucasian students, potentially due to factors like cultural differences in food practices, language barriers, or limited access to culturally relevant nutrition information. 40 In the current study, however, Hispanics obtained the highest scores. This may have resulted because 58% of the Hispanic students were graduate/postgraduate dietetics students, and the majority were enrolled at university C, which generated the highest scores.
Race and ethnicity can also influence the educational resources available to nursing and dietetics students. If students are not introduced to culturally specific nutrition information such as foods from different ethnic diets, they may have limited understanding of the nutritional needs of certain populations. This gap in knowledge can affect the quality of care they provide to diverse patient populations. 41
Practice and Perspective Contributions to Race/Ethnicity Scores
Different racial and ethnic groups have distinct dietary practices influenced by their cultural norms and access to certain foods. For instance, African American, Hispanic, and Asian populations may have unique dietary preferences shaped by traditional foods and beliefs around health and nutrition. These cultural differences can impact students’ knowledge of nutrition, particularly if their education does not include culturally relevant nutrition practices, or is limited to a Western diet framework. 42
Furthermore, some cultures are more open to non-conventional dietary and health practices, emphasizing balance and traditional or natural foods. Some parts of the Caribbean exhibit this characteristic. But other cultures may not be so inclined. This diversity in approach can shape how students understand the role of nutrition in disease prevention and management, especially when they encounter patients with different health beliefs and dietary practices. 43 Cultural awareness should be an essential module in the training of healthcare professionals. 44
General Applicability of Study
From the previous studies reviewed and highlighted above, there is indication that their findings share similar overall outcomes with the current study. The generalizability of results to other geographic areas or cultures therefore holds notable practical significance, but with various statistical limitations.
Limitations
The cross-sectional design of the study has inherent limitations. According to Wang and Cheng, cross-sectional studies analyze data from a population once and there is no continuous follow-up of data collection. 45 The design also has limitations when it comes to measuring incidence or assessing causal inference and external validity. We, however, sought to incorporate multi-center participation in order to capture information beyond a single area of the targeted region.
We obtained incomplete records for one university (ie, the exact enrollment for one of its specialized nursing programs was not readily made available), so sample size could not be accurately calculated. Convenience sampling was employed, relying mainly on willing participants and ease of access. Our survey therefore used an online mode and provided a direct link or QR code for students to easily gain access on any of their devices. Keith et al suggest other advantages of using electronic surveys that can outweigh different disadvantages. 46 For example, we benefited from inexpensive and quick data collection and management of multiple variables at the same time.
The survey-type nature of the study was also prone to issues such as non-response bias and item omissions. Interdisciplinary prejudices, limited time commitment, or lack of tangible incentives or motivation may have influenced the less than desired degree of response participation. However, in the promotion activities and the consent section of the survey, we sought to encourage participation by outlining the importance of the study and potential benefits the integrated healthcare approach would bring to the students’ future patients and practice.
The study did not investigate or include the cultural practices of participants within their given territory. An understanding of cultural practices remains critical in healthcare delivery. 47 But with a fair knowledge of the ethnic mix on the various campus sites and in the region, the researching team was still able to gather useful insights from the students’ responses for analysis and interpretation.
Significance and Implications of Study
This study significantly diverges from the current literature by introducing a novel methodology that enhances data collection and analysis, leading to more precise results. Unlike previous research, it explores previously overlooked factors, contributing to a broader understanding of the subject. The findings reveal that knowledge, psychographic characteristics, dietetics students, Hispanics, graduate/postgraduate students, and enrollment at campuses in specific cultural environments, significantly impacted response outcomes.
This research provides practical applications for integrated lifestyle-intensive and conventional healthcare approaches, an area that has not been adequately addressed in some prior studies and in the region of the Americas. Overall, this work not only expands on existing knowledge but also opens new avenues for future research. There are important theory, practice, and policy implications for evaluating nursing and dietetics students with respect to non-communicable diseases and the implementation of integrated healthcare approaches.
Evaluation of healthcare students:
The survey tool can be used to assess a more diverse population of healthcare students.
Further research can employ mixed methods utilizing qualitative interviews with students, faculty/staff members, and professionals from the clinical setting.
The educational setting:
Curricula for nursing and medical students can include basic and advanced nutrition, lifestyle, and metabolism courses.
A nutrition therapy course with both theory and practicum components is needed to cover modules related to management of common non-communicable disease conditions.
The clinical practice setting:
Retaining already-in-place use of coordinated lifestyle and clinical efforts.
The intentional practice of interdisciplinary healthcare team consultation between nursing or medical practitioners and dietetics experts in united healthcare efforts.
Ensuring that in-patient and out-patient NCD patients and those who are treated in private clinical practice settings are seen by or referred to a registered dietitian.
Policy Potential:
The results of the study can influence advocacy for the inclusion of nutrition and lifestyle-intensive protocols in healthcare delivery systems regionally, and internationally.
Conclusion
Based on the study’s results, demographic factors such as students’ specific healthcare discipline, ethnicity, the availability of lifestyle-inclusive graduate or post-graduate curricula, the strength of undergraduate training programs, and enrollment at campuses in specific geographical locations, significantly impacted response outcomes. Nutrition and lifestyle health-related knowledge, along with psychographics such as healthcare perception, perspective, and actual/potential practice characteristics, contributed significantly to survey responses in favor of integrated lifestyle and conventional healthcare approaches.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580251340177 – Supplemental material for Evaluating Nursing and Dietetics Students Regarding Nutrition, Non-Communicable Diseases, and Integrated Healthcare: A Multi-Center Survey Study
Supplemental material, sj-pdf-1-inq-10.1177_00469580251340177 for Evaluating Nursing and Dietetics Students Regarding Nutrition, Non-Communicable Diseases, and Integrated Healthcare: A Multi-Center Survey Study by Patricia A. Dyett, Lesley Ann Foster-Nicholas, Claudette Mitchell, Vanessa Jones-Oyefeso and George Legall in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580251340177 – Supplemental material for Evaluating Nursing and Dietetics Students Regarding Nutrition, Non-Communicable Diseases, and Integrated Healthcare: A Multi-Center Survey Study
Supplemental material, sj-pdf-2-inq-10.1177_00469580251340177 for Evaluating Nursing and Dietetics Students Regarding Nutrition, Non-Communicable Diseases, and Integrated Healthcare: A Multi-Center Survey Study by Patricia A. Dyett, Lesley Ann Foster-Nicholas, Claudette Mitchell, Vanessa Jones-Oyefeso and George Legall in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors acknowledge the nursing and nutrition and dietetics students who took the time to participate in the study. The administration and communication office personnel of the universities are also acknowledged for facilitating the recruitment of participants by sharing the link and QR code to the survey. Sincere appreciation is also extended to the Statisticians from the participating universities; and to the Nurse Educators who assisted in making suggestions during the pilot-testing of the survey, and in the promotion of the study: Mrs. Valerie Sealey-Tobias, Dr. Adana Adams-Robinson, and Dr. Paula Valley-Thom.
Ethical Considerations
All necessary School or Department permissions were obtained based on approvals from the Institutional Review Board or Ethics Committee of the host university (Ref.# CREC-SA.2437/12/2023).
Consent to Participate
All participants were required to indicate informed consent via the consent section of the electronic Google Form questionnaire.
Author Contributions
PD conceptualized the study and contributed to the design of the work along with LFN and GL, who also contributed in areas of methodology and analysis. These authors along with CM and VJO contributed in areas of data acquisition, interpretation, drafting of the manuscript, and critical revision of relevant intellectual content. All authors approved the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.