
Abstract
Current fall prevention guidelines are largely reactive to a history of falls and are thus an ineffective approach to primary fall prevention. This work aims to identify objective measures that predict fall risk to facilitate broader implementation in primary care settings. Longitudinal data were available from 952 men (48%) and women aged 60 to 97 enrolled in the Baltimore Longitudinal Study of Aging who had an index and subsequent visit approximately 2.5 years apart. Participants received objective measures at index visit and answered “yes” or “no” to the question “Have you fallen in the past 12 months?” at both visits. Main predictors included muscle strength (hamstrings/quadriceps), narrow walk, progressive static balance (semi-tandem, full tandem, single leg stance) tests and performance on conditions I and II of the modified Clinical Test of Sensory Interaction in Balance (mCTSIB). Each test was parameterized using validated methods. Logistic regression models adjusted for age, sex, race, and BMI were used to predict fall risk. Persons who failed the semi-tandem, full tandem, single leg stance, narrow walk, and condition II had, respectively, 2.59 (95% CI 1.51, 4.46), 1.57 (95% CI 1.06, 2.33), 1.54 (95% CI 1.15, 2.06), 2.21 (95% CI 1.37, 3.58), and 3.56 (95% CI 1.01, 12.57) times the odds of a future fall than persons who did not fail these tests. Observation of standing balance by assessing sway with eyes closed (condition II), ability to hold progressively challenging standing positions, or inability to traverse a narrow walk are all prognostic of a future fall. As these tests require no special equipment and take only 30 s to administer, identifying older persons at elevated risk of falling is feasible. Whether identifying persons at risk of falling can proactively prevent a future fall remains to be demonstrated.
Highlights
● Older adult fall incidence in the U.S. has been on the rise. Current fall prevention guidelines are largely reactive to an existing balance deficit as there has yet to be momentum towards prevention of an initial fall. It is possible that early detection of a decline in status could be beneficial in the prevention of falls. This study evaluates several objective assessments to idendentify their predictive validity for future falls in older adults.
● In adjusted logistic regression models, persons who failed the STS, SLS, NW, and condition II of the mCTSIB had, respectively, 2.48 (95% CI 1.37, 4.49), 1.58 (95% CI 1.12, 2.24), 2.15 (95% CI 1.27, 3.64) and 4.36 (1.12, 16.97) times the odds of having a future fall than persons who successfully performed these assessments.
● In adjusted logistic regression models, persons who failed the STS, FTS, SLS, and NW were, respectively, 3.14 (95% CI 1.73, 5.71), 1.61 (95% CI 1.04, 2.49), 1.50 (95% CI 1.06, 2.12), and 2.44 (95% CI 1.44, 4.12) times the odds to have had a previous fall than persons who did not fail.
Introduction
Falls are the leading cause of injury and death in adults over the age of 65 in the United States. 1 Healthy People 2030 identified both fall related injury and death as health indicators for older adults, with fall related deaths increasing 30% between 2007 and 2016.2,3 Every 11 s, an older adult is treated in the emergency department for a fall related injury, with falls accounting for over $50 million in medical costs annually.4,5 A fall related death of an older adult occurs every 19 min. 5 Falls are multifactorial and can occur due to side effects of medication, vision problems, improper foot attire, foot pain, both indoor and outdoor environmental hazards, and gait and balance deficits. 1
Balance and fall risk can be improved through intervention. Multiple studies support the use of rehabilitation to improve balance, with some improvements lasting up to 2 years.6 -13 The Centers for Disease Control and Prevention and the British and American Geriatric Society guidelines suggest a multidisciplinary approach to fall reduction which includes medication review, screening for fall history, and performing a risk factor assessment if a fall has occurred within the past 12 months or if a patient reports difficulty with balance or gait.14 -16 Medicare’s Merit-based Incentive Pay System (MIPS) for providers incentivizes completion of a risk assessment if a patient has had 2 or more falls, or a fall resulting in an injury within the last 12 months. 17 These guidelines and incentives are secondary prevention methods, and although important, do not address the problem at its core. Despite a multitude of fall prevention research, there has yet to be momentum toward proactive prevention of an initial fall. Introducing balance testing prior to fall occurrence may be a more effective strategy for fall prevention.
Determining the cause of falls and employing primary prevention practices are important to diminish injury and disability. Currently, the majority of fall prevention efforts are reactive to a history of falls and do not involve functional evaluations of impaired balance, a known risk factor for falls, until a fall has occurred.14 -17 Aging-related research has developed a broad variety of objective measures of balance that reliably predict past falls; less research has evaluated the predictive validity for identifying future falls risk in community dwelling individuals without cognitive decline or neurological comorbidities.18 -24 Fall risk batteries typically require multiple steps, take more time than primary care providers have available and are not administered until after a patient has either complained of a balance problem or has incurred a fall.17,25,26 Clearly, both static and dynamic balance should be assessed prior to a complaint or incident fall event for early detection of a decline in status.
Clinical tests of balance are performed to determine deficits and help identify best practices for fall prevention intervention. This study evaluates several objective assessments to identify their predictive validity for future falls in older adults. The performance-based tests include muscle strength (quadriceps and hamstrings), semi-tandem stance (STS), full tandem stance (FTS), single leg stance (SLS), a narrow path walk test (NW), and conditions I and II of the modified Clinical Test of Sensory Interaction in Balance (mCTSIB). Multiple studies have identified below average performance on these tests as contributing to disability, functional or mobility decline, and having a history of prior falls.27 -37 The specific tests evaluated in this study were selected for ease of administration in a primary care setting.
Methods
Participants
Quantitative data were available for 952 men (48%) and women aged 60 to 97 years participating in the Baltimore Longitudinal Study of Aging (BLSA) between January 2005 and March 2020 who received objective assessments including muscle strength testing (hamstring, quadriceps), conditions I and II of the mCTSIB, narrow path walk test, and progressive standing balance testing. The BLSA began in 1958 and is a continuous enrollment study that allows participants 20 years and older who are free from disease and comorbidities to enroll. Participants younger than age 60 receive 3 days of testing every 4 years, those between the ages of 60 and 80 receive testing every 2 years, while persons over the age of 80 receive yearly testing. Standardized instructions were given to each participant prior to performance of each objective measure. Written informed consent was provided by all participants. Research was approved by the Institutional Review Board of the Intramural Research Program of the NIH.
Balance Measures
The use of an assistive device was not permitted during testing. Persons who were unable to follow test instruction, or unable to begin in the starting position were excluded from testing.
Standing Balance Tests
The standing balance tests consisted of a battery of progressively challenging static tests including a semi-tandem (STS), full tandem (FTS), and single leg stance (SLS). Participant was able to select lead foot or stance leg for testing. Timing was recorded by use of a stopwatch. Each position has a 30 s goal, and participants were allowed up to 2 trials of each test, with the best time recorded. Timing started when the participant was in position without support, and timing ended either when the participant was no longer able to hold the position or when 30 s had been reached. For the purposes of this study, participants received a score of “pass” or “fail” for each test (STS, FTS, and SLS). If a participant was able to hold the position for a full 30 s, they were considered a “pass.” If a participant was unable to hold the position for the full 30 s (<29 s), they were considered a fail. 38
Narrow Path Walk Test (NW)
The NW was performed on a 6 m long, 20 -cm-wide course marked by tape in a tiled corridor. Participants were allowed up to 3 trials with 2 deviations outside of the tape. Timing started after the command of “Go” and with the first foot fall over the starting line and ended with the first footfall on or over the finish line. Time was recorded to the nearest 0.01 of a second. If a participant was unable to complete, or more than 2 deviations occurred, the trial was considered a fail. Participants were made aware of deviations post-trial. Persons who were able to complete the NW were considered a pass. 38
Modified Clinical Test of Sensory Interaction on Balance (mCTSIB)
Conditions I and II of the mCTSIB were performed using the BalenSens body worn microelectromechanical sensors (Biosensics, LLC, Watertown, MA) to detect anterior/posterior sway quantity, with larger sway indicating poor postural control strategies. Sensors were placed at anatomical reference points per equipment instructions, which were at the lower back/waist and the anterior aspect of the lower leg. Condition I required the participant to stand on a hard surface level floor with feet together, eyes open, and hands on hips. Condition II required the participant to stand on a hard surface level floor with feet together, eyes closed, and hands on hips. Participants were given up to 3 attempts to hold the position for 40 s. If the participant was unsuccessful in condition I, they still progressed to condition II. Failure was defined as being unable to complete the condition, a fall occurred, or sway was above the cut point. Cut points were determined by mirroring the CTSIB sway grid scores and utilizing the 68% cut score from the gold standard Computerized Dynamic Posturography Sensory Organization Test using the participant with the greatest sway as reference.39 -41 Persons below this cut point were considered to have passed. The mCTSIB was administered to a subset of the BLSA from August 2014 through June 2016, covering 54.3% of the cohort included in this study.
Muscle Strength
Isokinetic muscle strength of the left hamstrings and quadriceps were measured concentrically at 180° peak torque (Nm) using the Biodex System 4 Dynamometer (Biodex Medical System, Shirley, NY) Dynamometer settings were adjusted for individuals’ leg length as per manufacturer’s instructions prior to testing. Only the left leg data was used in analysis, as previous literature has found no muscle strength difference between dominant and nondominant legs in healthy, non-injured persons. 27 Test exclusions included blood pressure during physical examination equal to or exceeding 220 mmHg systolic or 115 mmHg diastolic, knee replacement or reconstruction on the knee to be tested, or severe osteoporosis, which affected 42.0% of the cohort. For the purposes of this study, those performing within the first quartile were considered “weak” while all other scores were considered “normal” strength. Test results from muscle strength testing were stratified by sex specific quartiles and normalized for height. 42
Self-Reported Falls and Perceived Balance
In a validated structured interview, 43 participants were asked, “In the past 12 months, have you fallen and landed on the ground or floor?” Persons who reported “yes” were then asked, “How many times did you fall to the ground in the past 12 months?” Answers included “one”, “two or three”, “four or five”, “six or more.” To determine the severity of falls, the following questions were asked: “Did you break or fracture a bone on any fall in the past 12 months?,” “Did you hit or injure your head on any fall in the past 12 months?,” and “Did you have a sprain or strain on any fall in the past 12 months?” Self-perceived balance concerns were captured with the questions: “In the past 12 months, did you limit your activities, for example, what you did or where you went because you were afraid of falling?” (answers included “yes” or “no”) and “Do you have any problem with keeping your balance when you are standing with your eyes closed, such as standing in the shower?” Answers included “always,” “very often,” “often,” “sometimes,” and “never.”
Covariates
Covariates included age, sex, race (self-designated Black or non-Black), and body mass index (BMI). BMI was calculated by standardized methods using measured height and weight. Covariates were selected due to their possible impact on health.
Statistical Analysis
The cross-sectional analyses use data from the index visit, that is, the first visit at which the participant had been administered the balance related performance tests, the falls history questions and the strength measures. Although the BLSA was established in 1958, functional performance tests were not introduced until 2005. In the cross-sectional analysis, participant characteristics were compared separately between the responses of “yes” or “no” to falls, number of falls, injuries from falls, and self-perceived balance concerns. Secondary to limited responses to the question “How many times did you fall to the ground in the past 12 months?,” responses of “four or five” (n = 6) and “six or more” (n = 7) were combined with the response “two or three” (n = 79) to create the category of “two or more” (n = 92). For the question “Do you have any problem with keeping your balance when you are standing with your eyes closed, such as standing in the shower?” answers of “always” (n = 15), “very often” (n = 6), “often” (n = 26) and “sometimes” (n = 146) were combined to form the category of “yes” (n = 193). Unadjusted and adjusted logistic regression models were utilized to determine the odds of having a history of falling with failure of each objective measure. Objective measures and self-reported history of falls were taken at the index visit to obtain baseline data. A complete case analysis was conducted, excluding participants with missing data from the study. Chi-Square Test of Independence was conducted to assess the relationship between paired balance tests (semi-tandem, full tandem, single leg stance, narrow walk, and condition II of the mCTSIB) To predict future falls, objective measures were obtained at the index visit with self-reported falls obtained at a subsequent visit, averaging 2.5 years later. Values (n, %) were compared separately between pass or fail of each objective measure to the answers of “yes” or “no” for self-reported falls. Unadjusted and adjusted logistic regression models were utilized to predict the odds of falling with failure of each objective measure. In addition to covariates, longitudinal analyses were also adjusted for length of follow-up.
Results
Cross-Sectional Associations
Table 1 shows participant characteristics, self-reported falls within the past 12 months, and severity of falls obtained at the subsequent visit. Participants (n = 952) were aged 60 to 97 years with a mean age of 74.6 (SD = 8.9). Forty-eight percent (n = 452) were male, and 24.3% (n = 231) were of Black race. A total of 243 participants (25.5%) reported falling within the previous 12 months; 151 (62.1%) reported falling one time and 92 (37.9%) reported falling 2 or more times. Of those who reported falling in the last 12 months, 11.1% (n = 27) reported fracturing a bone, 26.3% (n = 64) reported hitting or injuring their head, and 17.7% (n = 43) reported a sprain or strain from falling. Of the participants who fell, 109 denied that an injury occurred. Two participants who answered “yes” to falling did not indicate how many falls had occurred in the past year.
Participant Characteristics for Self-Reported Falls and Fall Severity.

Injury from falling in persons who reported a fall within the past 12 months.
In adjusted logistic regression models, participants who reported having a problem with their balance when their eyes were closed (n = 193, 21.5%) had 1.85 (95% CI: 1.30, 2.66) times the odds of falling than persons who denied balance concerns with their eyes closed. Ninety-five percent (n = 852) denied limiting their activities, but the 5% (n = 49) who reported limiting their activities had 3.36 (95% CI: 1.85, 6.10) times the odds of falling than persons who did not express concern for balance. Chi-Square Test of Independence indicate an increased likelihood of failing both tests in several paired scenarios: STS and FTS (x2 (1) = 91.19, P < .001), STS and SLS (x2 (1) = 21.02, P < .001), FTS and SLS (x2 (1) = 113.03, P < .001), and STS and condition II (x2 (1) = 4.17, P = .04).
Table 2a compares the results of the objective measures and self-reported falls obtained at the index visit. The majority of participants were able to successfully pass the objective measures, with the exception of the SLS where 55.7% of persons who reported a fall failed. Having weak leg strength was not associated with falling.
Objective Measures, and Past and Future Falls.

Values obtained by objective measures and self-reported falls at index visit.
Values obtained by objective measures at index visit and self-reported falls at subsequent visit averaging approximately 2.5 years post testing.
Table 3a shows the association between objective measures of balance by self-reported fall history at the index visit. In adjusted logistic regression models, persons who failed the STS, FTS, SLS, and NW were, respectively, 3.14 (95% CI 1.73, 5.71), 1.61 (95% CI 1.04, 2.49), 1.50 (95% CI 1.06, 2.12), and 2.44 (95% CI 1.44, 4.12) more likely to have had a fall than persons who did not fail. Figure 1a illustrates the adjusted logistic regression results in log odds.
Failure of Objective Measures, and Past and Future Falls.
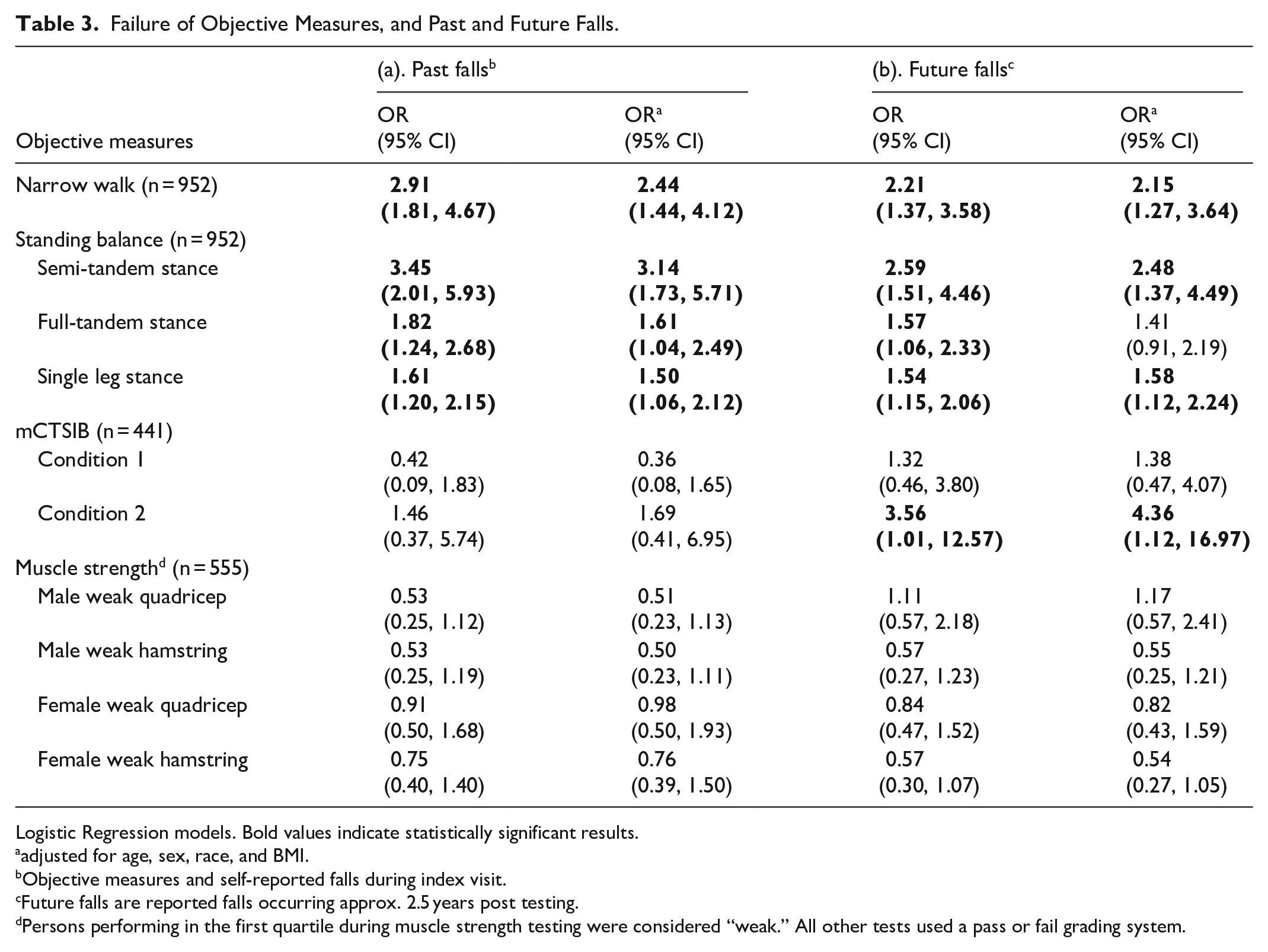
Logistic Regression models. Bold values indicate statistically significant results.
adjusted for age, sex, race, and BMI.
Objective measures and self-reported falls during index visit.
Future falls are reported falls occurring approx. 2.5 years post testing.
Persons performing in the first quartile during muscle strength testing were considered “weak.” All other tests used a pass or fail grading system.
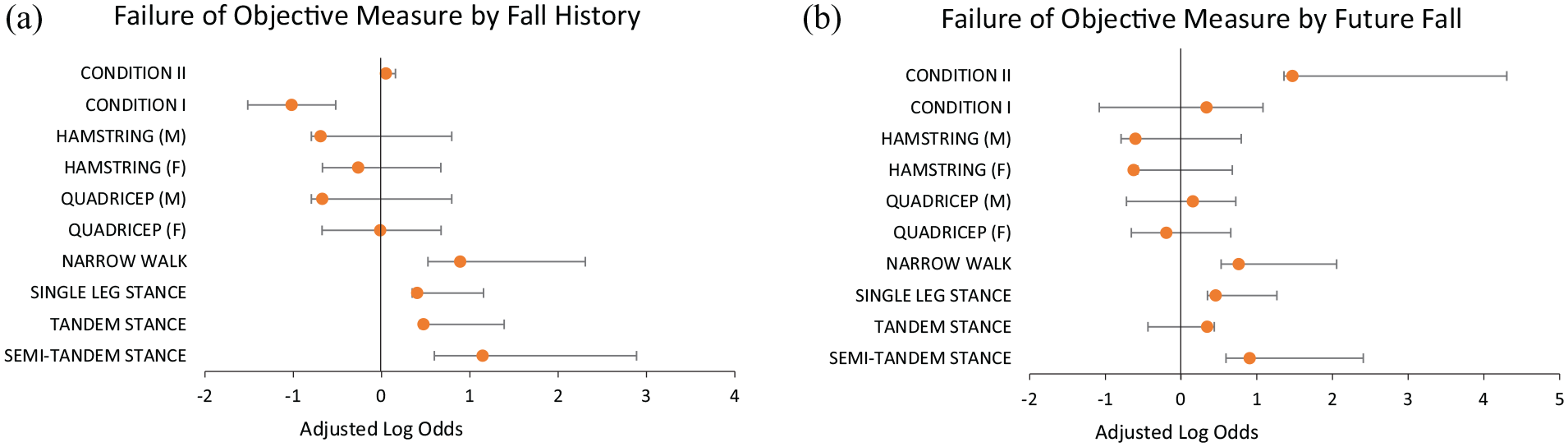
(a) History of falls: objective measures and self reported falls obtained at index visit. (b) Future falls: objective measures taken at index visit and self-reported falls obtained at subsequent visit, approximately 2.5 years post testing. Persons performing in the first quartile during muscle strength testing were considered “weak.” All other tests used a pass or fail grading system. (M): Male; (F): Female.
Longitudinal Associations
Table 2b compares the results of the objective measures obtained at the index visit and reported falls conveyed at the subsequent visit, which is described as a future fall. Over 25% of participants reported 1 or more falls at their follow-up visit, of which three quarters passed most tests at the index visit, with the exception of the SLS which had a much lower pass rate of 55.5%.
Table 3b summarizes the association between objective balance performance and future fall prevalence. In adjusted logistic regression models, persons who failed the STS, SLS, NW, and condition II had, respectively, 2.48 (95% CI 1.37, 4.49), 1.58 (95% CI 1.12, 2.24), 2.15 (95% CI 1.27, 3.64) and 4.36 (1.12, 16.97) times the odds of having a future fall than persons who successfully performed these assessments. Figure 1b illustrates the adjusted logistic regression results in log odds.
Discussion
In this cohort of community dwelling 60- to 96-year-olds, 25% reported falls within the past 12 months, which aligns with the U.S. national average of reported falls by older adults. 44 Failing the STS, SLS, or NW tests was associated with experiencing a fall within the preceding year as well as sustaining a future fall. The mCTSIB condition II had the highest association with a future fall. Interestingly, despite previous literature reporting an association between muscle strength and falling, in this study, having weak leg strength was not associated with falling as the proportion of participants who did not experience a fall was consistently higher in the weak group as compared to persons who reported a fall.27,42,45
The test with the strongest association with future falls, the mCTSIB condition II, would benefit from continued research as it was not associated with a history of falls in this study, however, previous research has observed a relationship between failing condition II and a history of self-reported falls. 46 Balance is maintained by 3 systems (vision, vestibular, and somatosensory). The primary system used depends on situational and/or environmental conditions. By testing balance exclusively with eyes open, we likely miss key information on balance deficiencies. Condition II of the mCTSIB requires the participant to stand with their feet together with eyes closed which eliminates use of vision for stabilization, decreases mechanical support (since feet are together) and demands integration of somatosensation with vestibular signals to maintain an upright and balanced position. 47 Studies have identified the pass rate for persons performing condition II as generally high overall, with normative scores averaging over 90% in both young and older adults, which may indicate that persons who fail this test are at a higher risk for falls.48,49 In this study, participants who self-reported having a problem with their balance when their eyes were closed had nearly twice the odds of falling as persons who denied having balance concerns with their eyes closed.
Although this study used body worn sensors to quantify sway during the mCTSIB, the traditional Clinical Test of Sensory Interaction in Balance does not use sensors and relies on tester capability to observe sway which is scored on a 1 to 4 grid (minimal, mild, and moderate sway, and fall). 39 We mimicked this grid system while scoring the mCTSIB to be more applicable to clinical practice. Those unable to perform the test or determined to have moderate sway should be considered a fall risk.
Conceivably, the experience of a memorable fall and the apparent downward trajectory of standing balance post fall may precipitate a concern for falling. This is consistent with the observation that persons reporting 1 or more falls were 3.36 (95% CIa 1.85, 6.10) times more likely to express a fear of falling, relative to persons without a recent fall. These findings align with previous work demonstrating that both the fear of falling and self-perceived balance concerns tend to perpetuate if not accelerate instability largely through avoidance-related disuse, or by adopting postural strategies that jeopardize balance control.50,51,52 Previous research has demonstrated that balance and balance confidence can be improved with formal balance training interventions,53-56 suggesting that primary prevention may decrease fall occurrence.
The primary study limitation is that this population largely consists of well-functioning older adults as demonstrated by the average pass rate of 83.7% across all objective measures. Participants selected for this research met the criteria of community dwelling individuals aged 60 years and older who were able to follow test instructions. Persons who required use of an assistive device were not administered balance testing, which eliminates testing for persons with obvious balance concerns. In addition, objective measures were performed in a controlled environment and may not sufficiently represent external balance challenges experienced in daily life. This study relied on self-report of falls which is subject to recall bias and may underestimate the occurrence of non-injurious falls.
An important study strength is investigation of both past and future reported falls, to evaluate the relationship between several objective balance-related assessments as metrics of fall risk. Current clinical fall prevention guidelines recommend physicians obtain a fall history annually, with an assessment warranted if a fall has occurred.16,57 With falls as the leading cause of injury-related death among adults aged 65 and older on the rise from 55.3 per 100 000 older adults in 2012 to 78.0 per 100 000 older adults in 2021, 58 we can no longer afford to be reactive to a fall history. Fall risk emerges from age-related pathologies and as such is not consistent with normative aging. 59 Healthcare professionals should educate their patients that falls are multifactorial and occur because of an internal or external influence that can be improved or modified. Balance testing and fall prevention education should be performed at every primary care appointment to detect a deficit or decline. Using any 1 of the standing balance tests (STS, SLS), NW or condition II of the mCTSIB as a quick objective measure to predict future falls in a primary care setting, combined with referral to the appropriate intervention allows us to be proactive. Reducing falls by using these tests as a predictor tool in primary care has not been previously examined and would benefit from further research.
Conclusion
Older adult fall incidence in the U.S. has been on the rise. Current fall prevention guidelines are largely reactive to an existing balance deficit as there has yet to be momentum toward proactive prevention of an initial fall. This study evaluated several objective assessments to identify their predictive validity for future falls in older adults and found that persons who failed the semi-tandem, full tandem, single leg stance, narrow walk, and condition II had, respectively, 2.59 (95% CI 1.51, 4.46), 1.57 (95% CI 1.06, 2.33), 1.54 (95% CI 1.15, 2.06), 2.21 (95% CI 1.37, 3.58), and 3.56 (95% CI 1.01, 12.57) times the odds of a future fall than persons who did not fail these tests. It is possible that early detection of a decline in status by proactively testing balance could be more beneficial in the prevention of falls.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251337269 – Supplemental material for Narrow Walk, Condition II, Semi-Tandem, Tandem, and Single Leg Stance Test Failure Could Predict Falls in Older Adults
Supplemental material, sj-docx-1-inq-10.1177_00469580251337269 for Narrow Walk, Condition II, Semi-Tandem, Tandem, and Single Leg Stance Test Failure Could Predict Falls in Older Adults by Colleen Brown, Marina Oktapodas Feiler, Eric R Anson and Eleanor M Simonsick in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Consent to Participate
Written informed consent was provided by all participants. Research was approved by the Institutional Review Board of the Intramural Research Program of the NIH.
Consent for Publication
Not applicable.
NIH Intramural IRB Protocol Number
03-AG-0325
Author Contributions
Colleen Brown designed the research study, collected, analyzed, and interpreted the data, and wrote the manuscript. Eleanor Simonsick assisted in the collection, interpretation of data, and manuscript revision. Marina Feiler provided critical feedback throughout the manuscript process. Eric Anson provided expertise on the mCTSIB protocol performed at the NIA as well as contributed feedback on manuscript revisions.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported and funded by the Intramural Research Program of the National Institute on Aging. Abstract was previously submitted to the Geriatric Society of America and accepted for presentation via poster at the GSA conference on November 8, 2023.
We certify that this work is novel of recent clinical research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Researchers can apply to use BLSA data through the National Institute on Aging’s database. Home | National Institute on Aging: Baltimore Longitudinal Study of Aging (nih.gov)
Supplemental Material
Supplemental material for this article is available online.