
Abstract
We described disruptions in cancer-related healthcare appointments and perceived quality of healthcare during the COVID-19 pandemic and identified predictors, including socioeconomic factors, of perceived quality of healthcare among cancer survivors. In this cross-sectional study, we used 2021 Health Information National Trends Survey-Surveillance, Epidemiology, and End Results data from Iowa, Greater Bay Area (California), and New Mexico cancer registries. Among cancer survivors who visited a healthcare provider in the past 12-months (N = 1130), we reported weighted prevalence of disruptions in (cancelled and/or changed to telehealth) routine cancer screening, disruptions in cancer treatment or follow-up, and perceived quality of healthcare, by registry. Using logistic regression, we identified predictors associated with perceived quality of healthcare, adjusting for sex and age. Among cancer survivors with scheduled appointments, 25.0% (Iowa) to 39.6% (California) reported disrupted cancer screening and 16.6% (Iowa) to 33.9% (California) reported disrupted treatment or follow-up related to their cancer diagnosis. 12.5% (Iowa) to 22.5% (New Mexico) of survivors perceived suboptimal quality of healthcare. Survivors with disrupted cancer screening, lower education and income, longer wait times for results, did not spend enough time with their doctor, and did not receive assistance with health uncertainty had increased odds of perceiving suboptimal quality of healthcare (odds ratio range = 2.64-19.31). Disruptions in cancer screening, lower socioeconomic status, and negative patient experiences were associated with poorer perceived quality of healthcare. Continued efforts are needed to address existing disparities to ensure equitable access to quality of healthcare post-pandemic.
Highlights
● During the early stages of the COVID-19 pandemic, over a quarter of cancer survivors who had a routine cancer screening/preventative care appointment scheduled experienced a disruption in their appointment.
● Nearly a fifth of cancer survivors who had a cancer follow-up or treatment appointment related to their cancer diagnosis scheduled experienced a disruption in their appointment.
● Cancer survivors who experienced disruptions in cancer screening appointments, had lower education and income, and had negative patient experiences had increased odds of perceiving suboptimal quality of healthcare, but associations varied by geographic region.
● Continued screening for second primary malignancies among cancer survivors during and post-pandemic should be priortizied to ensure timely care and improved quality of health care.
Introduction
By January 2022, there were 18 million cancer survivors in the United States, many of whom were newly diagnosed during the COVID-19 pandemic. 1 During the onset of the COVID-19-omicron variant surge (Fall-Winter 2021), adults in the United States who were undergoing cancer treatment had higher death rates than the general population. 2 The pandemic substantially altered cancer healthcare delivery, particularly resulting in severe underutilization of non-emergency care, such as routine cancer screenings.3,4 Further, the COVID-19 pandemic resulted in disruptions in cancer diagnoses, treatment, and follow-up care for surveillance and management of long-term and later effects of cancer and its treatment.3,4 Factors contributing to changes in cancer healthcare delivery included the issuance of stay-at-home orders, professional recommendations to pause or suspend routine screening tests, and resource prioritization toward the pandemic.5 -8 These measures, aimed at mitigating COVID-19 spread, may have impeded access to critical, timely, and quality healthcare services for cancer survivors. Continued cancer screening and follow-up for cancer survivors is crucial given the long-term risks for treatment-related adverse health effects, such as the development of primary second cancers.9 -11
In response to the pandemic, healthcare systems swiftly pivoted to telehealth, representing a paradigmatic shift in healthcare delivery, potentially influencing cancer care, patient engagement, and perceived quality of healthcare.12,13 Perceived quality of healthcare can directly impact patient outcomes and overall health management, particularly among cancer survivors experiencing health disparities.14,15 Thus, evaluating factors associated with perceived quality of healthcare could provide opportunities to improve patient satisfaction and engagement and in turn improve health outcomes. Prior studies have noted that patient-provider interactions, including perceived empathy by the provider, provider communication, time spent with the doctor, and number of healthcare visits substantially impacted patient perceptions of healthcare quality.15 -17 Further, individuals with lower socioeconomic status experience greater barriers in access to healthcare, more negative patient-provider interactions, and have poorer perceptions of quality of healthcare.18,19
Even before the pandemic, disparities in quality of healthcare were well-documented in the United States healthcare system. Studies have shown that socioeconomic factors such as income, race, and age influenced the quality of care delivered. 20 Additionally, geographic and structural barriers, such as limited access to radiotherapy facilities, have been associated with poorer cancer outcomes, particularly in rural and underserved regions. 21 These systemic inequities in quality of healthcare highlight the importance of identifying vulnerable populations who are particularly at risk due to their need for continuous and specialized care, such as cancer survivors.
Poor perceived quality of healthcare among cancer survivors can negatively impact their engagement with healthcare systems, adherence to treatment plans, and overall health outcomes. To better understand the COVID-19 pandemic’s impact on healthcare delivery among cancer survivors, we: (1) described disruptions in routine cancer screening/preventative care appointments and cancer treatment or follow-up appointments; (2) described perceived quality of healthcare; and (3) identified characteristics associated with perceiving suboptimal quality of healthcare.
Methods
Data Source and Study Population
In this cross-sectional study, we used de-identified data from the Health Information National Trends Survey-Surveillance, Epidemiology, and End Results (HINTS-SEER) study (conducted from January to July 2021), which sampled cancer survivors from Iowa, the San Francisco-Oakland Greater Bay Area (California), and New Mexico cancer registries (N = 1234). 22 The parent HINTS survey is a nationally representative survey that monitors changes in health communication, health beliefs, and healthcare among United States adults in the general population. The HINTS-SEER survey is based on the original HINTS survey; however, because cancer survivors from only 3 cancer registries were sampled in this pilot effort, the weighted prevalence estimates from HINTS-SEER are only generalizable to their source population where the registry resides. 22 Participants for HINT-SEER were selected using a systematic sampling process based on eligibility criteria and received mailed questionnaires conducted exclusively on paper using a modified Dillman approach. 22 The survey included multiple mailings, reminder postcards, and pre-paid incentives to maximize response rates. 22 Questionnaire topics assessed cancer-related experiences, including the impact of COVID-19 on cancer care. 22
The HINTS-SEER survey, similar to its parent HINTS instrument, is not a fully validated tool as a whole. 23 However, it includes questions from validated sources, with many items undergoing cognitive testing in prior HINTS cycles to ensure the validity of core items and constructs. 23 New questions, particularly those added for the SEER-specific portion, such as those addressing COVID-19 impacts and cancer treatment experiences, were pre-tested or designed following established survey design principles, though they did not all undergo cognitive testing due to time constraints.
As noted by the HINTS-SEER methodology report, each cancer registry had their own institutional review board approvals and consenting procedures. 22 In each cancer registry, all cancer survivors in the study provided consent to participate, but the procedures to obtain consent varied by registry, which resulted in varying response rates by registry. Participants of the New Mexico Tumor registry required passive consent but had the highest consent rate (60.1%), while participants in the Iowa Cancer Registry required active consent prior to receiving the survey and had the lowest consent rate (7.5%). 22 Participants in the Greater Bay Area Cancer Registry required active consent but received the consent form with the survey mailing (consent rate = 24.2%). 22
Prior to receiving the HINTS-SEER data, which is a restricted-use dataset, the authors obtained the necessary approvals by the HINTS review board. Additional information on the HINTS-SEER survey design and methodology are found elsewhere. 22 Inclusion criteria for our study were cancer survivors who visited a healthcare provider in the past 12 months regardless of cancer type, which resulted in 1130 (91.6% of 1234) cancer survivors in our analytic population. Cancer survivors who did not visit a healthcare provider in the past 12 months were excluded because the question regarding perceived quality of healthcare asked participants to reflect on their healthcare within the past 12 months. Therefore, we aimed to only examine participants who actually visited a healthcare provider within that time frame. Our study followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines. 24
Primary Variables
Disruptions in routine cancer screening/preventative care appointments was assessed by the question, “Has the COVID-19 pandemic affected any of your appointments for routine cancer screening or preventative care?” (Supplemental Table 1). Disruptions in cancer treatment or follow-up medical appointments related to the participant’s cancer diagnosis was assessed by the question, “Has the COVID-19 pandemic affected either your cancer treatment or any follow-up medical appointments related to your cancer?.” For both disruption questions, appointments were considered “disrupted” if the participant indicated that their appointments were either cancelled, changed to telehealth, or had a combination of multiple situations. Perceived quality of care was assessed using a 5-point Likert scale question, “Overall, how would you rate the quality of healthcare you received in the past 12 months?”.
Statistical Analysis
Per the HINTS-SEER analytic guidelines, analyses were stratified by state due to differences in procedures to obtain consent and varying response rates by registry. Individual-level sampling weights provided by HINTS-SEER were used to calculate population point estimates that are generalizable to the registry population from which the individual was drawn from, and 50 replicate weights were applied using the jackknife method to calculate proper standard errors, as described in the HINTS-SEER data analysis recommendation documentation. 22
We reported weighted prevalence and corresponding 95% confidence intervals (95% CIs) of disruptions in (cancelled and/or changed to telehealth) routine cancer screening/preventative care appointments; disruptions in cancer treatment or follow-up medical appointments related to the participant’s cancer diagnosis; and perceived quality of healthcare, by registry. The weighted prevalence of disruptions in care were only calculated among cancer survivors who had each appointment type scheduled. Across the 3 registries, 32.2% to 38.0% of survivors did not have a cancer screening or preventative care appointment scheduled during the past 12 months, and 47.9% to 51.0% of survivors did not have a cancer treatment or follow-up medical appointment related to their cancer diagnosis scheduled during the past 12 months (Supplemental Table 2). As an exploratory analysis, we also reported these metrics by years since diagnosis but could not cross-stratify with registry due to limited sample size. We also described additional care perceptions, such as having enough time spent with doctors, receiving assistance with health uncertainty, and having discussions with healthcare providers about COVID-19 complications due to cancer history.
Using multivariable logistic regression, we examined characteristics associated with perceiving suboptimal (less than very good) quality of healthcare, including disruptions in cancer-related appointments; sex; age group; education level; household income; primary insurance status; time since cancer diagnosis; time since last treatment; perceived enough time spent with the doctor; perceived receipt of assistance with health uncertainty; having discussions with healthcare providers among COVD-19 complications due to cancer history; having to bring an x-ray, MRI, or other test to the appointment; waiting for test results longer than thought reasonable; and seen or talked to a mental health professional about health. Each variable was tested as a separate model, adjusting for sex and age. Due to the nature of the 5-point Likert scale question for quality of healthcare, the “good” response was considered suboptimal because it represented the neutral response, which allowed prioritization of “very good” and “excellent” responses as optimal care in the analysis. Two-sided P < .05 were considered statistically significant. All analyses were conducted using Stata v17 (StataCorp LLC).
Results
Descriptive Characteristics
The analytic population included 1130 cancer survivors who visited a healthcare provider in the past 12 months (Iowa = 338, California = 429, New Mexico = 313; Table 1). Across the 3 registries, the most common cancer sites were breast (range = 22.1%-25.1%), prostate (range = 18.1%-24.1%), and melanoma of the skin (range = 8.8%-12.0%). The median age of cancer survivors was 70 years in Iowa and New Mexico and 73 years in California. Demographic distributions varied across registries, including by sex, age group, education level, household income, and primary insurance status. However, most survivors had Medicare insurance (either alone or in combination with another insurance) and were diagnosed >5 years prior to the survey, with roughly half being diagnosed ≥11 years prior. Over a quarter of cancer survivors visited a healthcare provider at least 5 times in the past 12 months.
Sociodemographic, Care Perceptions, and Healthcare Characteristics of Cancer Survivors Who Visited a Healthcare Provider in the Past 12 Months, HINTS-SEER 2021.
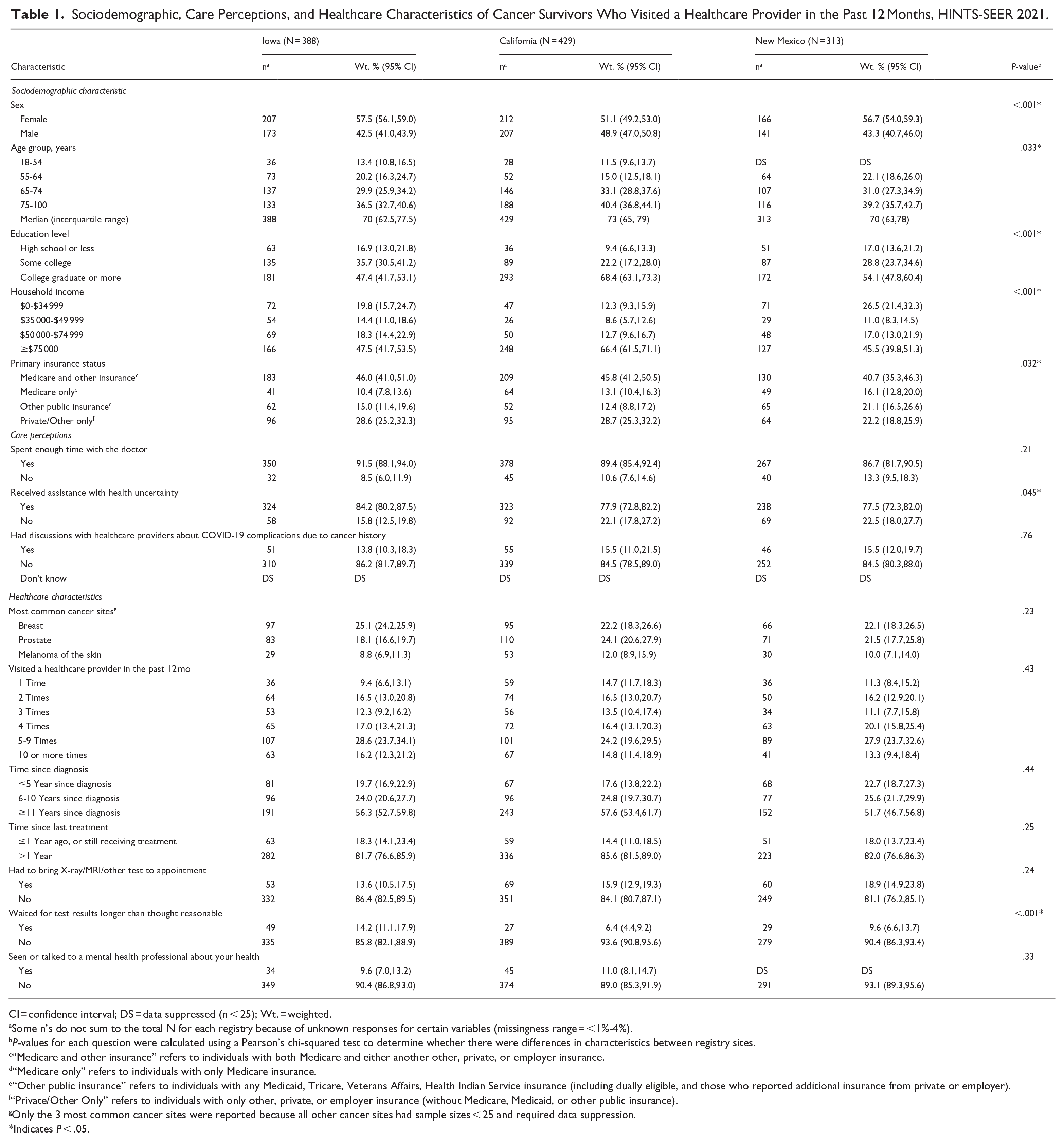
CI = confidence interval; DS = data suppressed (n < 25); Wt. = weighted.
Some n’s do not sum to the total N for each registry because of unknown responses for certain variables (missingness range = <1%-4%).
P-values for each question were calculated using a Pearson’s chi-squared test to determine whether there were differences in characteristics between registry sites.
“Medicare and other insurance” refers to individuals with both Medicare and either another other, private, or employer insurance.
“Medicare only” refers to individuals with only Medicare insurance.
“Other public insurance” refers to individuals with any Medicaid, Tricare, Veterans Affairs, Health Indian Service insurance (including dually eligible, and those who reported additional insurance from private or employer).
“Private/Other Only” refers to individuals with only other, private, or employer insurance (without Medicare, Medicaid, or other public insurance).
Only the 3 most common cancer sites were reported because all other cancer sites had sample sizes < 25 and required data suppression.
Indicates P < .05.
Disruptions in Cancer Care
Among cancer survivors who had a routine cancer screening/preventative care appointment scheduled, 25.0% (95% CI = 19.5%-31.4%; Iowa) to 39.6% (95% CI = 33.0%-46.6%; California) reported their appointments were cancelled and/or changed to telehealth (Figure 1). Among cancer survivors who had a cancer treatment or follow-up appointment related to their cancer diagnosis scheduled, 16.6% (95% CI = 11.4%-23.4%; Iowa) to 33.9% (95% CI = 25.6%-43.3%; California) reported their appointments were cancelled and/or changed to telehealth. Disruptions in appointments were similar by time since diagnosis (P > .05); however, a slightly greater proportion of survivors ≥10 years from diagnosis compared with ≤5 years reported disruptions in cancer screening/preventative care appointments (36.6% vs 27.3%) and cancer follow-up or treatment appointments (30.3% vs 24.3%; Supplemental Table 2).

Weighted prevalence of changes to cancer-related appointments during the COVID-19 pandemic by registry, HINTS-SEER 2021. Affected appointments includes canceled only, telehealth only, and multiple situations selected. Less than very good includes good/fair/poor.
Perceived Quality of Care
Approximately 90% of survivors reported spending enough time with their doctor; however, nearly 90% reported not having discussions about COVID-19 complications due to their cancer history with their provider (Table 1). Perceived suboptimal quality of healthcare ranged from 12.4% (95% CI = 9.2%-16.5%; Iowa) to 22.5% (95% CI = 17.5%-28.4%; New Mexico; Figure 1). After adjusting for age and sex, characteristics associated with perceiving suboptimal quality of healthcare included disruptions in cancer screening/preventative care appointments in New Mexico only (aOR = 2.64, 95% CI = 1.11-6.26), ≤high school versus ≥college education in California (aOR = 7.12, 95% CI = 2.74-18.45) and New Mexico (aOR = 2.64, 95% CI=1.18-5.89), household income ≤$34 999 versus ≥$75 000 in California (aOR = 3.61, 95% CI = 1.49-8.74) and New Mexico (aOR = 2.70, 95% CI = 1.15-6.36), and waiting for test results longer than thought reasonable in Iowa only (aOR = 5.17, 95% CI = 2.18-12.26; Table 2). Across all 3 registries, not spending enough time with the doctor (aOR range = 7.43-19.31) and not receiving assistance with health uncertainty (aOR range = 6.42-10.44) was associated with significantly increased odds of perceiving suboptimal quality of healthcare. In contrast, Medicare insurance was inversely associated with perceiving suboptimal quality of healthcare in California only (Medicare and another insurance versus private/other only aOR = 0.32, 95% CI = 0.11-0.98; Medicare only versus private/other only aOR = 0.29, 95% CI = 0.08-0.98).
Odds of Perceiving Suboptimal Quality of Healthcare During the COVID-19 Pandemic Among Cancer Survivors Who Visited a Healthcare Provider in the Past 12 Months by Registry Site, Adjusting for Age and Sex, HINTS-SEER 2021.

aOR = adjusted odds ratio; CI = confidence interval; DS = data suppressed (n < 25).
“Medicare and other insurance” refers to individuals with both Medicare and either another other, private, or employer insurance.
“Medicare only” refers to individuals with only Medicare insurance.
“Other public insurance” refers to individuals with any Medicaid, Tricare, Veterans Affairs, Health Indian Service insurance (including dually eligible, and those who reported additional insurance from private or employer).
“Private/Other Only” refers to individuals with only other, private, or employer insurance (without Medicare, Medicaid, or other public insurance).
Indicates P < .05.
Discussion
In this cross-sectional study, over a quarter of cancer survivors who had a routine cancer screening/preventative care appointment scheduled experienced a cancellation and/or change to telehealth for their appointment and nearly a fifth of cancer survivors who had a cancer follow-up or treatment appointment related to their cancer diagnosis scheduled experienced a cancellation and/or change to telehealth for their appointment during the early stages of the COVID-19 pandemic. Our results corroborate prior studies reporting disruptions and delays in cancer care due to pandemic-related factors among cancer survivors in the United States and globally.25 -27 Specifically, one United States-based study reported that 32% of cancer survivors who required treatment and/or other cancer-related care experienced changes, delays, or cancellations in their cancer care during the second half of 2020. 25
Our study reported that perceived suboptimal quality of healthcare ranged from 12.4% to 22.5%, and cancer survivors who experienced disruptions in cancer screening appointments, had lower education and income, and had negative patient experiences (including waiting for test results longer than thought reasonable, not spending enough time with their doctor, and not receiving assistance with health uncertainty) had increased odds of perceiving suboptimal quality of healthcare. While our study did not aim to compare across states, we note that disruptions in care, perceived quality of healthcare, and characteristics associated with perceived suboptimal quality of healthcare were not uniform across state cancer registries, possibly reflecting uneven distribution of healthcare resources and differential state-specific pandemic-related challenges.
Distinct patterns associated with the impact of COVID-19 on cancer care can be understood by examining the varying public health responses and their effects. California implemented COVID-19 response measures earlier, including stay-at-home orders, mask mandates, and restrictions on non-essential activities, 28 likely contributing to higher prevalence of changes in healthcare appointments, including increased use of telehealth services. Notably, although cancer survivors in California experienced greater changes in cancer screening/preventative care compared with survivors in Iowa (39.6% vs 25.0%), possibly due to less restrictive COVID-19 responses in Iowa (eg, relaxed state guidance on quarantine, removal of mask mandate), perceived quality of healthcare was similar in both states (14.1% and 12.4%). In contrast, cancer survivors in New Mexico also had greater changes in care compared to Iowa but had the highest prevalence of perceived suboptimal quality of healthcare, where cancer survivors who experienced disruptions in cancer screening/preventative care appointments had 2.64 times the odds of perceiving suboptimal quality of healthcare.
While telehealth may provide an alternative avenue for care, our results suggest that equitable access to telehealth technology was likely not universal, potentially exacerbating disparities in care across different regions. Specifically, in 2021, telehealth utilization was higher among adults who were women, had higher educational attainment, had health insurance, lived in the Western region of the United States, and lived in more metropolitan areas.29,30 A national study also reported that in 2021, telehealth utilization in the United States was significantly lower in Midwestern states, such as Iowa. 30 In a state-based analysis of Medicare beneficiaries in the United States, telehealth utilization varied across states during the COVID-19 pandemic, with California having the largest absolute growth in Medicare telehealth encounters from 2019 to 2020. 31 Variations in telehealth utilization across states could be related to policy differences and reimbursement factors, 31 as well as socioeconomic factors, which emphasizes the need for targeted strategies to overcome infrastructural and demographic barriers and to ensure equitable access to care nationwide.
Another possible explanation for differences in the prevalence of disruptions in care and perceived quality of healthcare across states could be differences in demographic distributions within each population. Specifically, California had a higher proportion of cancer survivors who had attained a college degree or higher and had a household income ≥$75 000 compared with Iowa and New Mexico. These sociodemographic differences could have impacted care perceptions and healthcare system satisfaction in general across states. For example, individuals with lower socioeconomic status have reported poorer perceptions of their healthcare quality, including their treatment provided, access and accessibility to care, and patient-provider interactions.18,19,32 Among patients undergoing radiation oncology, individuals with greater socioeconomic disadvantage have also reported poorer patient satisfaction, 33 further emphasizing that socioeconomic disparities play a role in patient healthcare experiences and perceptions.
Another alarming finding was that most (>80%) cancer survivors did not speak with their providers about possible COVID-19 complications due to their cancer history. Certain populations of cancer survivors may be at greater risk of health effects due to immunosuppressive treatments (eg, stem cell transplant) and cancer types (eg, blood cancers) and therefore would benefit from care discussions about potential COVID-19 complications due to their cancer history. 9 Further, disruptions in cancer screening and follow-up among cancer survivors is critical to address given the long-term risks for treatment-related adverse health effects, such as second cancers. As cancer survivors transition out of oncology care into primary care, cancer screening for second primary malignancies is critical for ensuring timely care and treatment. Implications for this study include prioritization of cancer survivors for cancer screening during and even post-pandemic (or other global disruptions or stay-at-home orders), which could be partly mitigated through telehealth services. However, the potential disparity in telehealth access (as represented by the differences in the prevalence of care disruptions across states) emphasizes the importance of addressing technological and infrastructural barriers to ensure all patients benefit from adaptable strategies, including telehealth modalities, to maintain high-quality care.
Our study was constrained by relatively small sample sizes because the HINTS-SEER study was part of a pilot project to provide a larger sample of cancer survivors for future HINTS analyses. In consequence, we were unable to examine care disruptions and quality of healthcare by cancer type. Additionally, over half of the cancer survivors in our study were at least 11 years past their cancer diagnosis, which limited the number of individuals who were actively undergoing cancer treatment to allow for more robust analyses of the COVID-19 pandemic’s impact on cancer care. We were also unable to compare results to a pre-pandemic period due to prior HINTS surveys not asking about disruptions in cancer-related appointments. Lastly, survivor bias may be present, as our study does not include individuals who passed away during the pandemic. Despite these limitations, our study is among the first to identify factors contributing to perceived quality of healthcare among cancer survivors during the COVID-19 pandemic. We also used robust statistical methods with complex sampling weights, enabling generalizability to each registry’s source populations. Additionally, unlike the original HINTS survey, which relied on a self-reported “cancer diagnosis” question, which could be subject to response bias, the strength of HINTS-SEER lies in the ability to confirm that all participants are cancer survivors, as they were sampled from population-based cancer registries.
Conclusion
Our study highlights the importance of improving timely delivery of preventative care, improving patient experiences, and providing socioeconomic support for cancer survivors experiencing health disparities, which are modifiable points of intervention. The COVID-19 pandemic contributed to major shifts in healthcare delivery across the United States, which impacted perceived quality of healthcare among cancer survivors in certain states, as supported by our findings. Although vaccination efforts have reduced COVID-19 infections, hospitalizations, and deaths, evaluating the long-term impacts of changes in cancer care delivery on perceived quality of healthcare is imperative to understand the impact of public health emergencies among cancer survivors. Continued efforts are needed to address existing disparities to ensure equitable access to quality cancer care.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251330361 – Supplemental material for Suboptimal Quality of Health Care and Associated Socioeconomic Factors Among Cancer Survivors During the COVID-19 Pandemic: A Cross-Sectional Study
Supplemental material, sj-docx-1-inq-10.1177_00469580251330361 for Suboptimal Quality of Health Care and Associated Socioeconomic Factors Among Cancer Survivors During the COVID-19 Pandemic: A Cross-Sectional Study by Erica S. Stephens, Jun Tao, Jereme Corbin, Aimée R. Kreimer, Jennifer K. McGee-Avila, Michelle Doose, Siddharth Roy, Meredith S. Shiels and Jaimie Z. Shing in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580251330361 – Supplemental material for Suboptimal Quality of Health Care and Associated Socioeconomic Factors Among Cancer Survivors During the COVID-19 Pandemic: A Cross-Sectional Study
Supplemental material, sj-docx-2-inq-10.1177_00469580251330361 for Suboptimal Quality of Health Care and Associated Socioeconomic Factors Among Cancer Survivors During the COVID-19 Pandemic: A Cross-Sectional Study by Erica S. Stephens, Jun Tao, Jereme Corbin, Aimée R. Kreimer, Jennifer K. McGee-Avila, Michelle Doose, Siddharth Roy, Meredith S. Shiels and Jaimie Z. Shing in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-3-inq-10.1177_00469580251330361 – Supplemental material for Suboptimal Quality of Health Care and Associated Socioeconomic Factors Among Cancer Survivors During the COVID-19 Pandemic: A Cross-Sectional Study
Supplemental material, sj-docx-3-inq-10.1177_00469580251330361 for Suboptimal Quality of Health Care and Associated Socioeconomic Factors Among Cancer Survivors During the COVID-19 Pandemic: A Cross-Sectional Study by Erica S. Stephens, Jun Tao, Jereme Corbin, Aimée R. Kreimer, Jennifer K. McGee-Avila, Michelle Doose, Siddharth Roy, Meredith S. Shiels and Jaimie Z. Shing in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Ethical Considerations
Each cancer registry that participated in the HINTS-SEER study had their own institutional review board approvals and consenting procedures. Prior to receiving the HINTS-SEER data, which is a restricted-use dataset, the authors obtained the necessary approvals by the HINTS review board.
Consent to Participate
Informed consent was obtained from all participants included in the study.
Author Contributions
Conceptualization and writing of the original draft were performed by Erica S. Stephens, Jereme Corbin, and Jaimie Z. Shing. Data curation, formal analysis, software, validation and visualization were performed by Erica S. Stephens, Jereme Corbin, Jun Tao, and Jaimie Z. Shing. All authors contributed to the methodology and reviewing/editing of manuscript drafts. Supervision was done by Aimée R. Kreimer, Meredith S. Shiels, and Jaimie Z. Shing. Erica S. Stephens, Jun Tao, Jereme Corbin, and Jaimie Z. Shing had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Intramural Research Program of the US National Cancer Institute at the National Institutes of Health. No sponsor had any role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Disclaimers
The opinions expressed in this article are the authors’ own and do not reflect the views of the National Cancer Institute. A related abstract for this work was presented as an oral presentation at the 2023 HINTS Data User Conference, September 2023.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.