
Abstract
PHC should be accessible to the entire population, regardless of their economic or social class and geographical location. The PHC system in Saudi Arabia provides most curative and preventive health services through many centers. This study aims to estimate the percentage of PHC utilization and determine the factors associated with the utilization of PHCCs in Riyadh, Saudi Arabia. A quantitative cross-sectional design was used for community-based PHCs and employer-based PHCs in Riyadh. The study sample consisted of 306 patients and community members attending primary health clinics at National Guard Health Affairs (NGHA) and Ministry of Health (MOH). Data were collected using a self-administered questionnaire adopted from the Agency for Healthcare Research and Quality. Data analysis was conducted using SPSS. Descriptive and inferential statistics were used to achieve the aim of the study. In our study, we found that 53.9% (95% CI = 48.34%, 59.51%) utilized PHCs. Furthermore, females were more likely to utilize PHCs with OR = 1.675 and 95% CI = (1.029, 2.727). Healthcare managers and policymakers should focus their efforts on providing desirable services, consequently changing public opinion about healthcare services, and increasing their satisfaction with existing services.
Keywords
The concept of healthcare utilization refers to individuals seeking medical attention for a variety of purposes, such as preventing and treating health issues, encouraging the maintenance of health and well-being, or learning more about their current state of health and prognosis. PHC covers essential medical services that are grounded in evidence-based medicine and widely accepted methodologies.
Using PHC facilities was more common among female patients than male patients, suggesting a greater association between genders. No significant association was found between PHC center use and any of the demographic characteristics such as age, employment status, income, or education level.
Although females utilize healthcare services more than males, healthcare administrators and policymakers should focus on enhancing care services to encourage greater utilization among both genders.
Introduction
The World Health Organization (WHO) defines primary health care (PHC) as initial health care delivered using scientific and practical methods and techniques that are justifiable, accessible and cost-effective for the country and society at any stage of development. 1 The concept healthcare utilization refers to individuals seek medical attention for a variety of purposes, such as preventing and treating health issues, encouraging the maintenance of health and wellbeing, or learning more about their current state of health and prognosis. PHC covers essential medical services that are grounded on evidence-based medicine and widely accepted methodologies. It is easily available to individuals and families through their active engagement, and the cost is designed to ensure it remains affordable for both the general population and society. 2 Additionally, it is recommended to maintain communication with the healthcare system at a basic level. When it comes to a country’s health system, primary healthcare (PHC) plays a crucial role in keeping the population’s health at an acceptable level.3,4
Primary healthcare is sometimes referred to as a mindset, a movement, a philosophy, a way of working, an attitude to healthcare, or a set of fundamentals. However, pursuing it at the national level means that societies focus on health services at the national level rather than building large tertiary hospitals that exclusively serve residents of financially secure urban areas. It also means that healthcare provider education will be present at this level without focusing on high-cost medical technologies and interventions that are only accessible to relatively limited populations. WHO emphasizes that PHC is acceptable, affordable, accessible, and appropriate and is delivered through partnerships between local communities and the national health system. The primary duty for prioritizing health needs and implementing appropriate primary healthcare services lies mostly with communities. The primary healthcare (PHC) services include preventative interventions, health promotion efforts, and both curative and rehabilitative treatment that are self-administered by people. 2
Theoretical Background
Healthcare services-provided on primary health care centers (PHCCs)—mainly involve educating the public about prevalent health issues and preventative and control measures, as well as enhancing food supplies and promoting effective nutrition. Additionally, these services include maternal and pediatric healthcare, which includes family planning, vaccination against prevalent infectious diseases, and management of epidemic outbreaks. They additionally ensure sure that these facilities provide effective medications and supplies. 5
Modern primary healthcare encompasses a multi-professional team, proactive and reactive care, population and individual focus, the social and cultural context of illness, the patient’s centrality in their own care, an advocacy role, multiple service models, and multiple interfaces. 6 Regardless, we think that “Primary care is first-contact care, delivered by generalists, dependent (increasingly) on teamwork, which is accessible (both geographically and culturally), comprehensive (interested in old as well as new problems), coordinated, population-based (there is responsibility for ‘the list’ as well as the individual patient), and activated by patient choice.” 6
Literature Review
The state of many PHC facilities not only poses a threat to society but also affects the utilization rate of PHC facilities. A study conducted in southwestern Nigeria revealed that less than half (42.50%) of the study participants used PHC services. 7 The high expense of healthcare services is a major issue for individuals living in Nigeria, even when healthcare facilities provide specific services and exemptions for things like routine vaccinations and prenatal care. The differences in facility types between urban and rural regions affects the utilization of health services. In comparison to their rural equivalents, high-quality facilities in cities are more likely to be used all day, every day since they provide a wider range of services. Other barriers that affect the use of PHC services are due to social, economic, mental, demographic, or geographical challenges. 5 Studies have shown that approximately 75%-85% of patients require initial treatment and management within 1 year, referral with medical. Referral to healthcare professionals is only required just in 10%-12% of patients, and referral to advanced levels or further treatment and management is essential only required in 5% of patients. 8 Access to primary healthcare services basic medical care is essential for maintaining good health. Current research illustrates how variations in the utilization of primary healthcare (PHC) services are influenced by socioeconomic factors that affect individuals within the country. Services are utilized at a greater rate by patients with higher incomes than by those with lower incomes, according to studies revealed an association between financial stability and having accessibility to primary healthcare services among high-income persons.9,10
Niyas et al 8 conducted a cross-sectional study to elucidate the utilization of primary healthcare services and health seeking behavior in Iranian families using samples from three phases in 2016-2017. The data were gathered by the administration of a questionnaire. The results indicated a statistically significant association between the probability of service use and the quality of service used, and factors such as education level, age, insurance type, income level, residence, and referral system type. Additional factors influence the use of primary healthcare (PHC) services for counseling such as nutrition, mental health, counseling for risky behaviors, care for the elderly, and medical management of hypertension and diabetes.
The research highlights the need of enhancing the quality of PHC services and implementing policies to promote the use of PHC and referral systems. 8 Truppa et al 2 conducted a randomized home study to determine whether the International Committee of the Red Cross (ICRC) program effectively engages the most disadvantaged populations, to investigate the primary health needs identified in the ICRCS-supported facilities located in metropolitan areas, and to identify the obstacles encountered when attempting to access healthcare services. According to the findings of the research, the most vulnerable citizens were identified in facilities that received assistance from the International Committee of the Red Cross. Additionally, reproductive and sexual health concerns (28.6%) and noncommunicable diseases (40.6%) were the most frequent reasons for seeking care. According to the findings of the population survey, substantial disparities exist in the use of health services between childbearing-age women and their children. Consequently, innovative approaches are required to resolve financial obstacles that exist at both the facility and individual user levels. 2
In Saudi Arabia, basic, secondary, and tertiary health services are provided by the Ministry of Health (MOH). Primary healthcare facilities offer a wide range of medical treatments, encompassing preventive, promotional, and curative care. General hospitals are directed to patients needing a higher level of treatment (secondary level of care), whereas tertiary level of care refers to patients requiring much more advanced levels of care. Fast urbanization and socioeconomic transformation in Saudi Arabia in the last several decades have raised the need for high-quality healthcare services among the population. This highlights the critical need for solid tools for evaluating primary healthcare. 11
Despite abundant global research on the factors influencing the utilization of primary healthcare (PHC) services, recent data on the Saudi Arabian context remains scarce. In addition, there is a discrepancy in the results of studies conducted in Saudi Arabia. For instance, existing studies, such as the study of Alfaqeeh et al 12 found that there is a significant association between primary healthcare utilization and gender and age, whereas the study of Alsubaie et al 13 found no such association. Thus, there is a critical need for recent research that investigates the utilization of PHC services in Saudi Arabia and the associated factors related to the utilization. Increasing utilization prevent and treat health issues and maintaining of health and wellbeing, Therefore, this study aimed to evaluate the utilization of PHC services in Saudi Arabia and identify the factors that are associated with utilization.
Methods
Study Sample and Data Collection
This research utilized a cross-sectional design, and was conducted at Primary Health Centers (PHCs) in Riyadh, Saudi Arabia from May 13, 2020, to January 2021. The study period was chosen because this period covers different circumstances and seasons, including multiple holiday seasons, which can be important for assessing behaviors in different situations. In 2021, the total number of Primary Health Centers (PHCs) in Riyadh was 436. Their usual working hours go from 8:00 am to 6:00 pm, with certain locations offering longer and 24/7 shifts. All individuals aged 18 and older who visited PHCs in Riyadh represented the target population for this research. Patients with mental health issues and/or those under the age of 18 were excluded, along with those who declined to participate in the research. Participated PHCCs were from the Ministry of Health and National Guard Health Affairs. Based on the Cochrane equation (https://www.myrelab.com/learn/sample-size), the sample size should be at least 385 individuals to be representative to the study population. Using a consecutive sampling method and despite the several reminders and extension of the data collection period, only 306 individuals (response rate = 79.5%) completed the survey. The data were gathered using a self-administered valid questionnaire obtained from the Consumer Assessment of Healthcare Providers and Systems Clinician and Groups (CG-CAHPS) survey.14,15 The questionnaire was distributed among participants via an online hyperlink. The survey includes demographic data as independent variables, such as age, gender, employment status, income, and level of education. Furthermore, the survey investigates the utilization of primary healthcare services (the dependent variable), with a specific focus on visits to primary healthcare centers within the last 6 months. Ethical approval was obtained from the King Abdullah International Medical Research Center (KAIMRC) Institutional review board (IRB) on May 13, 2020 (Ref, No, IRB/0756/20). Informed consent was obtained from all participants.
Statistical Analysis
The researchers analyzed the data using the Statistical Package for the Social Sciences (SPSS, IBM version 24) to accomplish the study’s objectives. The demographic data were managed as categorical variables; these data include gender, age, employment status, income, and education level. Categorical variables were summarized using frequencies, and percentages. Association of utilization with demographic factors was established by the Pearson’s chi-square test. Additionally, the intensity of the association between utilization and potential factors was evaluated using a binary logistic regression to calculate the odds ratio. Statistical significance was set at P-value < .05.
Results
A final sample size of 306 participants was secured, with a response rate of about 79.5%. Overall, 51.6% of the study participants were female. Most of the study participants were in the 30-39 age group. The number of participants regarding this age group was 90 individuals, and their percentage was 29.4%. Almost 60.1% of participants were employed, participant who are unemployed were 114 (37.3), and 8 (2.6%) retired. Among the study participants, 16.3% had an income ranged between 3000 and 5000, and 47.1% had an income 5000-15 000. Regarding the educational level of the participants, 26.1% have a primary school degree or less, 23.2% have a middle school degree, and 19.9% have a bachelor’s degree (Table 1).
Number and Percentage of Demographic Characteristics of Study Participants.
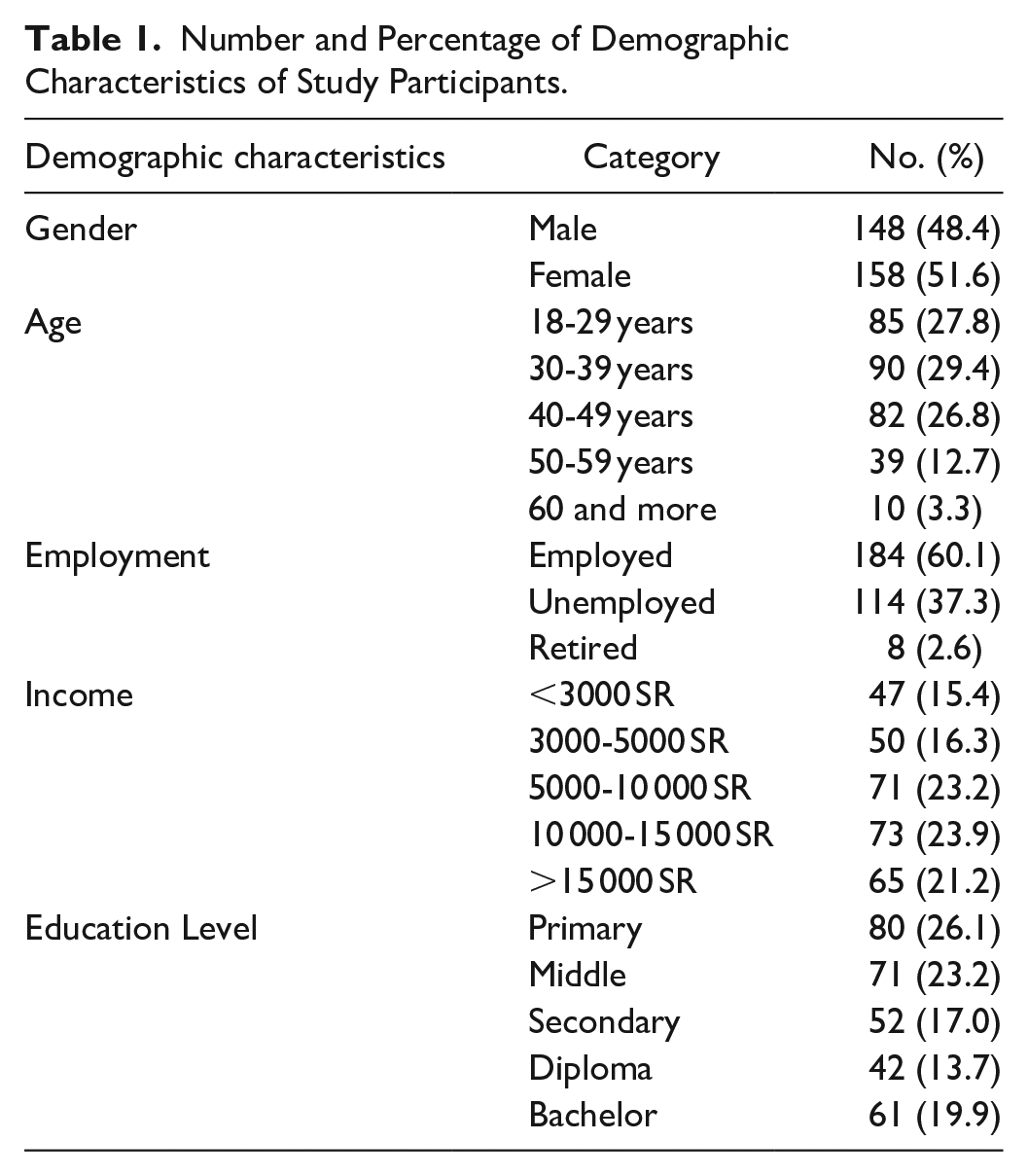
Table 2 shows that 165 (53.9%) of the participants had used PHC centers in the last 6 months, while 141 (46.1%) of the participants had not used PHC centers.
Frequency and Percent of People Utilized PHC Centers During the Last 6 Months.

Table 3 shows that there is a significant association between the gender of the patient and the use of a specialized health center (P = .035). Conversely, no significant association was found between the age of the participants and their use of a specialized health center (P = .681). Furthermore, no significant association was found between the employment of the participants and their use of a specialized health center (.288). Similarly, no significant association was found between the participants’ income and their use of a specialized health center (P = .987). Finally, no significant association was found between the education level of the participants and their use of a specialized health center (.685).
Association Between Participants’ Utilization of PHC Centers and Demographic Characteristics.
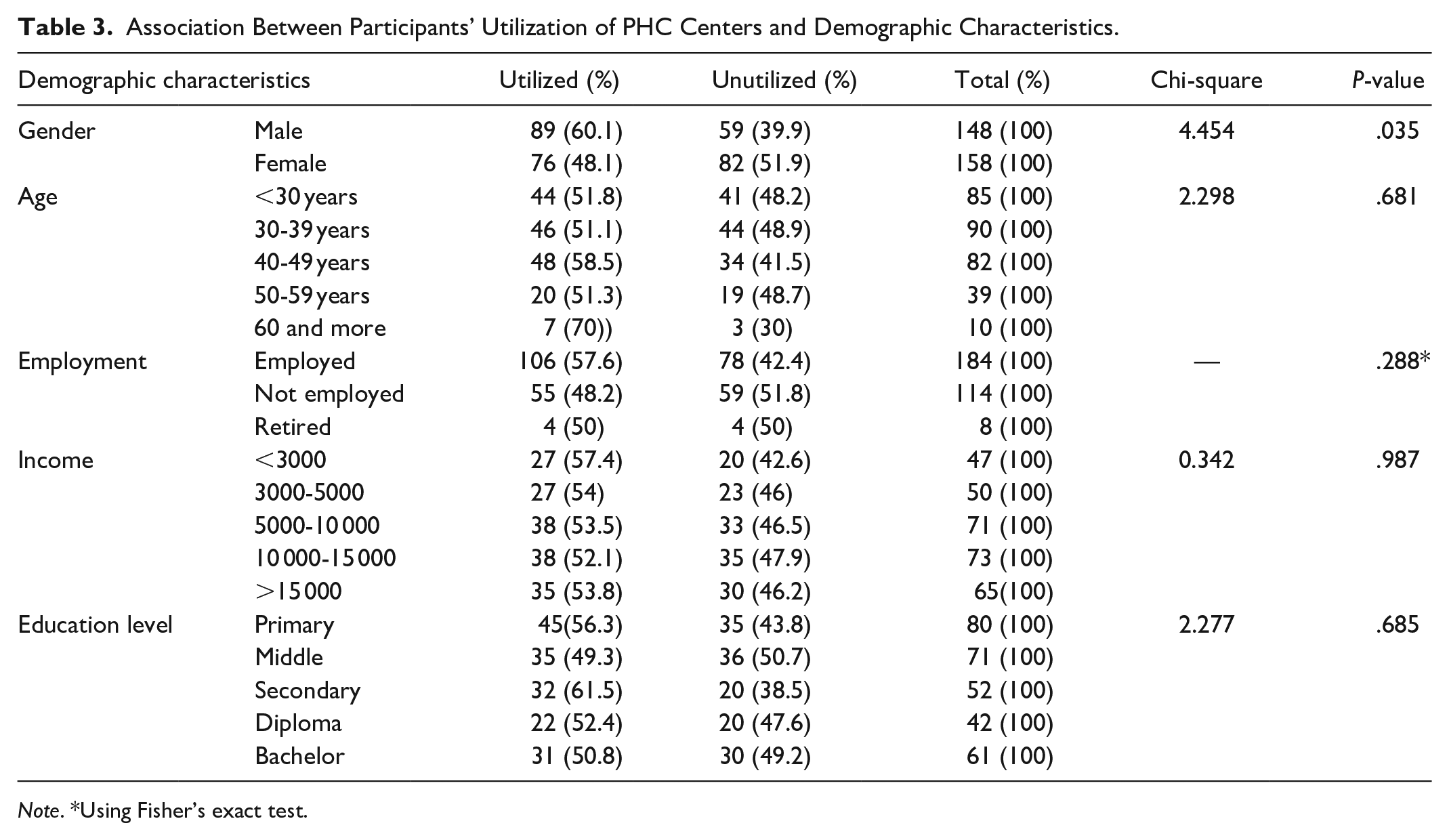
Note. *Using Fisher’s exact test.
Table 4 shows that female participants are 67.5% (95% CI = 1.029-2.727, P = .038) more likely to use PHC services than male participants. The odds ratio was 1.675.
Odds Ratio of Gender Regarding Utilize PHC Services.

Discussion
The objective of this research was to examine the utilization of PHC services and determine the factors that are linked to the use of primary healthcare facilities in Riyadh, Saudi Arabia. Overall, 53.9% of participants utilized PHC services (95% CI = (48.34%, 59.51%)). This result is consistent with a study conducted by Alonge. 16 Using PHC facilities was more common among female patients than male patients, suggesting a greater association between genders. No significant association was found between PHC center use and any of the demographic characteristics such as age, employment status, income, or education level.
Almost half of the respondents had received treatment at PHCs in the study location, while 46.1% of the respondents had not used PCH services. This surpasses the 30.7% found among 481 residents in Al-Madinah, Saudi Arabia. 17 In a study examining PHC utilization in Turkey, 30% of individuals were found to use PHC centers. In addition, a study in Nigeria found that only 7.5% utilized PHC services.
In general, the usage rate of PHC facilities is low, which could indicate that patients are not monitoring their health status frequently and are therefore at risk. All Saudi citizens have access to free health services provided by the Saudi Ministry of Health; however, utilization of PHC services remains low, most likely due to patients’ perceptions of service quality and satisfaction.
Although 90% of medical visits can be treated by the primary care provider, most people do not consider PHC centers as their first choice to receive healthcare services. 18 One study found that 72.3% of the respondents prefer to visit Emergency Department (ED) rather than PHC to address their medical issues. 19
People’s attitude towards family medicine and primary care needs to be reconsidered. Access to the availability of medical supplies and equipment greatly influences patient care quality and use of PHC. A poor state of infrastructure could also have a negative impact on the use of PHC. This is in line with a study by Aldhamadi and Alzahrani 19 and a study by Al Janabi 10 where participants expressed dissatisfaction with the state of the facilities and equipment. The major pillars of PHC system include appropriate technology that can be adapted to local needs and community participation; patients would prefer to participate in various preventive activities led by PHC centers. 18 Shifting the focus from purely curative health services to preventive and promotive health-care services would promote the well-being of all. Patients are willing to engage with the public and improve their health literacy. 20 Availability of medication is also considered one of the primary indicators of patient satisfaction with PHC. 21
The utilization of PHC centers was found to be significantly influenced by gender, with females being more likely than males to utilize PHC services. This result aligns with the findings of Asamrew et al, 22 who found that females were more satisfied and utilized healthcare facilities more frequently than males. Alghamdi et al 17 observed an association between gender and the use of PHC centers. Disparities in the utilization of PHCCs services by gender may be attributable to maternal health need.
Healthcare use was higher among married women than among single women, mostly because of reproductive and maternal health concerns. 23 In Gabrani et al 24 study found that the use PHC services is more prevalent among elderly and married people. This may be attributed to two factors: increased utilization of PHC centers by women because of a greater morbidity burden and treatment delays, both of which could potentially be influenced by gender. 25 Women are more likely to contract and experience a more severe form of numerous infectious diseases compared to males. Factors such as biological variations and socially determined roles contribute to this. 26 The societal role of women as caregivers for their families might leave them more at risk for illness and less likely to seek treatment when they need it.
In our study, no significant association was found between age, employment, income, educational level, and utilization of PHC centers (P > .05). This finding is inconsistent with other studies which found that age, education, and income were statistically significantly associated with utilization PHC services utilization.8,27 A study demonstrates that individuals with health insurance utilized PHC services less frequently. Comparing low-income individuals with high-income ones, the former is more likely to use PHC services.
There was significant link found between the level of education of the participants and their use of PHC. Similar results were found in study of Prayogi et al. 27 The absence of association may be attributed to the comparable manner in which respondents sought medical care, regardless of their level of education. 17 Nonetheless, prior research conducted in Saudi Arabia found that PHC services offered by the Ministry of Health (MOH) are more often used by individuals with lower levels of education than by those with higher levels of education.
Limitations of the Study
While this study offers insight into some factors that influence the utilization of PHCs, there are a few limitations to this study that should be articulated:
Time constraints prevented further research beyond Riyadh.
In addition, the results have limited generalizability due to the COVID-19 situation which may affect the utilization of PHC.
Furthermore, the sample size was smaller than the desired one, this affected the precision of the confidence interval by approximately 0.006 (Actual − Desired = 0.0558 − 0.05). In other words, our confidence interval is a bit wider that desired.
Moreover, a potential recall bias should be acknowledged, since we focused on visits to primary healthcare centers within the last 6 months.
Finally, since the data were collected using online platform, the older age group might be underrepresented.
Conclusion
The study concluded that more than half of participants utilize the PHC services, and the dominant factor associated with the use of healthcare services at the PHCC is patients’ gender. This raises the possibility that gender influences healthcare-seeking behavior. Other factors such as age, employment status, income, and education level were not associated with the utilization of healthcare center. This result emphasizes the necessity of specialized interventions to promote access to and use of basic healthcare services by addressing gender-specific barriers and facilitators. To investigate the underlying causes of these gender disparities in healthcare usage. It is highly recommended to conduct educational events for various community members to raise their awareness on utilization of PHC services.
Healthcare administrators and policymakers in the healthcare system need to focus their skills on providing the desired care services to change public opinion about these services and increase satisfaction with existing services. Policymakers should also find solutions to problems related to healthcare services in primary healthcare centers, such as ensuring that patients receive adequate information about primary healthcare services. These can create an incentive for patients to regularly check their health status. Further investigation should be conducted to explore additional variables that might impact the utilization of primary healthcare services. It is possible to obtain more information from patients regarding the quality of services and information they receive from healthcare providers through qualitative or quantitative research studies.
Footnotes
Acknowledgements
We would like to express sincere gratitude to Almaarefa University, Riyadh, Saudi Arabia, for their scientific support of this research. We would like to express sincere gratitude to King Saud bin Abdulaziz University for Health Sciences, for their scientific support. We would like to express sincere gratitude to King Abdullah International Medical Research Center, for their scientific support. We would like to express sincere gratitude to the Office of Research at King Saud bin Abdulaziz University for Health Sciences and in particular Reem Alamr has assisted us with editing and proofreading this research paper.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the King Abdullah International Medical Research Center (KAIMRC) Institutional review board (IRB) on May 13, 2020 (Ref, No, IRB/0756/20). Informed consent was obtained from all participants.