
Abstract
Objective
To address the growing burden of chronic disease globally, many countries have developed a national policy for primary healthcare reform. In some countries with high and very high human development index, evaluations of the implementation of these reforms have been published. To date, there has been no systematic review of these evaluations. The objectives of this review are to identify: (a) the vision for primary healthcare; (b) the features of primary healthcare reforms; and (c) evaluation findings of primary healthcare reforms.
Methods
A systematic literature review was conducted guided by the PRISMA statement. We searched for academic articles and grey literature from 1 March 2008 to 1 September 2020. Screening and data extraction were conducted by two authors. Descriptive analysis and narrative synthesis were applied.
Results
A vision for integrated primary healthcare shifting chronic disease management from specialist hospital services to primary care was found to require new organization and funding models such as collaborative primary healthcare networks and commissioning along with shared governance across health sectors. The need for general practitioner leadership and engagement to support primary healthcare reform was identified. Although there was evidence of barriers in progressing primary healthcare reform, evaluation results showed some positive outcomes, most notably shifts in services towards increased primary care access and utilization.
Discussion
A challenge in undertaking the review was the heterogeneity of articles with little consistency in how primary healthcare reform was evaluated and reported on across countries. Evaluation of national health reforms involves complex system-wide projects and is an area that needs further exploration and discussion to determine the most appropriate methodologies for collecting and analysing large-scale data with consideration for service and health outcomes.
Introduction
Globally, chronic disease and multimorbidity represent major challenges, increasing the health demand in many countries. 1 The World Health Organization (WHO) 2 reported that 15 million people aged 30–69 years old die each year from non-communicable diseases, and this number is expected to rise to an estimated 52 million by 2030. In responding to the burden of chronic disease, the WHO Global Status Report on Non-Communicable Diseases 2010 3 highlighted the importance of strengthening the health system with more emphasis on primary healthcare (PHC) as the first point of care and partnership between health services providers as key to success. Effective chronic disease management (CDM) has been linked with strong PHC characterized by good governance structures, accessibility, care coordination, continuity of care and comprehensive service delivery. 1 Hone et al. 4 indicated that countries with stronger PHC have been able to reduce mortality rates, part of which can be attributed to effective management of non-communicable diseases.
In an effort to tackle major deficits in health systems such as fragmentation, inequalities and inefficiencies, many countries have been undergoing reform of PHC including integration between primary and secondary healthcare services.5–7 CDM is a priority in these reforms shifting from predominately secondary specialist care to PHC as the principal setting for accessing and receiving healthcare.5–7 The Health Council of Canada reported that effective PHC reform will achieve enhanced continuity of care through integrated healthcare; a shift in health service provision from individuals to populations; more efficient use of qualified professional health workers leading to effective cooperation between health providers; a focus on disease prevention, and health promotion and more appropriate use of healthcare resources. 8 It has been suggested that chronic diseases and long-term health conditions are more effectively managed in countries with high or very high human development index (HDI) due to more advanced healthcare systems compared to those with low or medium HDI.9,10 Therefore, countries with high/very high HDIs may offer insights into the impact of PHC reforms on CDM. The HDI, as reported annually by the United Nations Development Programme, is a measure of a country's human development in terms of a long and healthy life expectancy, mean years of education, and gross national income per capita contributing to standards of living. 11
Conceptually, PHC is broader than primary care (PC), 12 yet, these concepts are used interchangeably leading to confusion.12,13 PC is a component of PHC referring to health services delivered to individuals closest to their communities through family doctor type services known as general practices (GPs) or family practices.12–14 More broadly, PHC, which focuses on population health, is viewed as a complex subsystem within a country's national health system. It incorporates a wide range of public health, primary and community services. 13
In strengthening PHC reform for CDM, the WHO 3 highlighted the need to evaluate progress at the national level. An evaluation of these reforms would help to determine the vision for PHC reform for the prevention and control of non-communicable chronic diseases, as well as the features of these reforms in terms of the services developed and implemented for CDM. 3 To date, a number of countries have reported on evaluations of PHC reform national policy concerning CDM. However, there has been no systematic review of these national evaluations. A review of this evidence would help to identify the vision and features of PHC reform targeting CDM, and a synthesis of evaluation findings would help to determine what works best and why. This systematic review aims to address this gap in knowledge. With a focus on countries with high or very high HDI, the objectives of this review are to identify: (a) the vision for PHC reform relating to CDM; (b) the features of PHC reforms in terms of the services developed and implemented for CDM; and (c) evaluation findings of PHC reforms for CDM.
Methods
This systematic review was guided by the PRISMA statement. 15 Consistent with the review objectives, the search process and selection criteria were guided by the following research questions: What is the vision for PHC reform relating to chronic diseases? What are the features of PHC reform relating to services developed and implemented for CDM? What are the outcomes of evaluations of national PHC reform targeting CDM?
Search strategy
We searched the academic databases CINAHL, MEDLINE and Embase to identify articles focusing on PHC reform targeting chronic diseases. We applied the terms ‘primary healthcare’, ‘primary care’ and ‘community’ since these terms are often used interchangeably in the literature. Other terms included ‘health services/system reform’ and terms relating to chronic conditions such as ‘chronic disease’/’chronic condition’/ ‘non-communicable disease’. In addition, we applied the term ‘reform’. Boolean operators (OR/AND) as well as truncation where relevant were applied. The relevant subject headings, MeSH terms and index terms were applied, respectively, to CINAHL, MEDLINE and Embase databases. The search was limited by date from 1 March 2010 to 1 September 2020 reflecting articles published since the WHO emphasized strengthening the health system through PHC in responding to the burden of chronic disease. 3 The search was also limited to articles published in the English language. A search for grey literature was conducted guided by Godwin et al. 16 Initially, three databases/websites were searched, namely OpenGrey, Grey Literature Report (up to 2017 when discontinued) and the WHO. The second search was then conducted in targeted websites of countries shown to yield a greater volume of articles retrieved from these sites and the academic databases. Websites searched were the National Health Services, Department of Health and The Kings Fund from the UK, Health Canada, Australian Government Department of Health, Ministry of Health New Zealand and the National Institute of Health, USA.
Selection criteria
Guided by our research questions stated above, we included articles on the evaluation of PHC reform in healthcare systems as part of government strategy in countries with high or very high HDI scores (i.e. index of 7–10) reported for the year(s) concerning the period of evaluation addressed and not the year of publication (sourced through http://hdrundp.org/en/countries). Articles focusing on physical chronic diseases were included since these contribute to a significant burden on health systems due to high morbidity and mortality rates. 1 Articles of any study design were included, for example, cross-sectional studies, cohort studies, surveys, case studies or qualitative evaluation studies. Additionally, the review included any type of report such as case reports, commissioned reports and narrative reviews. This review excluded articles on countries with low or medium HDI scores. Articles addressing national reform strategy and associated PHC were excluded if the focus was on an individual chronic disease rather than multiple chronic diseases since our aim was to review PHC reform regarding chronic diseases in general. Given the focus of this review on physical chronic conditions, articles on mental illness as a chronic condition were excluded. Furthermore, we excluded articles relating to clinical care provided by family doctors/GPs if not related to the broader government context of health system reform in relation to population health for CDM. Finally, any article reporting on PHC reform for years within which a country did not meet the HDI inclusion criteria was excluded, regardless of the article being published within the time limits set for this review. For example, one article retrieved was published in 2015 from China 17 but the time period of evaluating PHC reform was 2011–2013 during which time this country was classified as medium human development. 18
Screening process
All records from the search strategy were first exported to Endnote X7 and then to Covidence for screening once duplicates (n = 142) were removed. Two reviewers (MA, ES) screened the titles and abstracts of each article (n = 542) to determine if full-text review was needed. Full-text articles (n = 168) were then read to establish eligibility for inclusion. Disagreements were resolved by discussion with the other reviewers (CN, CB). The output from the search strategy and screening process is shown in Figure 1 illustrating that eight articles were included in this review. Of these, five were retrieved from academic databases,19–23 and three from grey literature sources.24–26
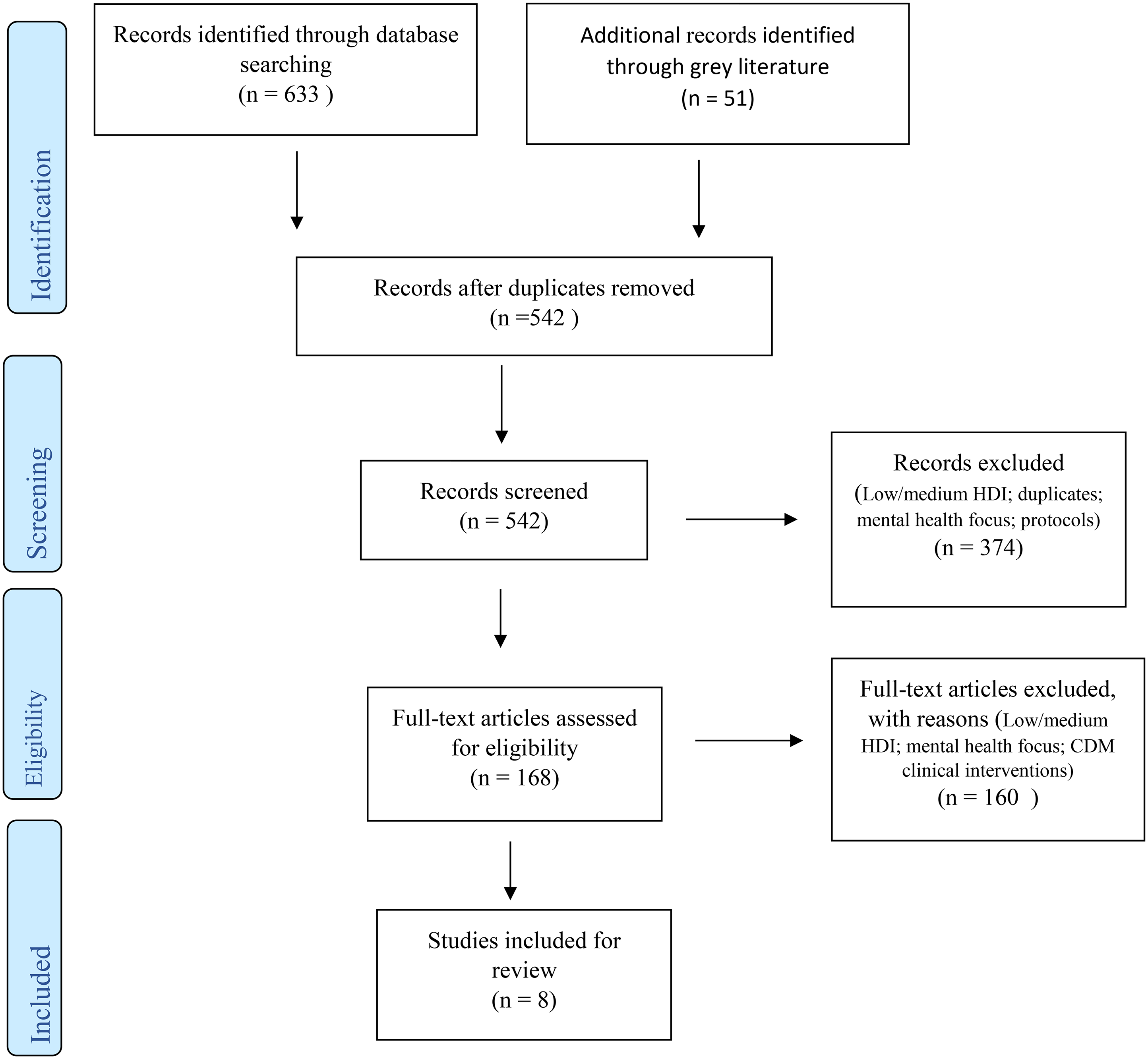
PRISMA flow chart.
Data extraction and synthesis
Data from each article were extracted into a table including author name(s), publication date, country, design, the vision for PHC reform, features of PHC reform, sources of evaluation data and the findings on outcomes (Table 1). The data were extracted by MA and cross-checked by ES including discussion between both authors to reach a consensus where differences arose. Following data extraction, a narrative synthesis of the findings was conducted structured around the objectives of the review. Although guided by the PRISMA statement, 15 a meta-analysis was not feasible due to the heterogeneity of studies included.
Data extraction table.
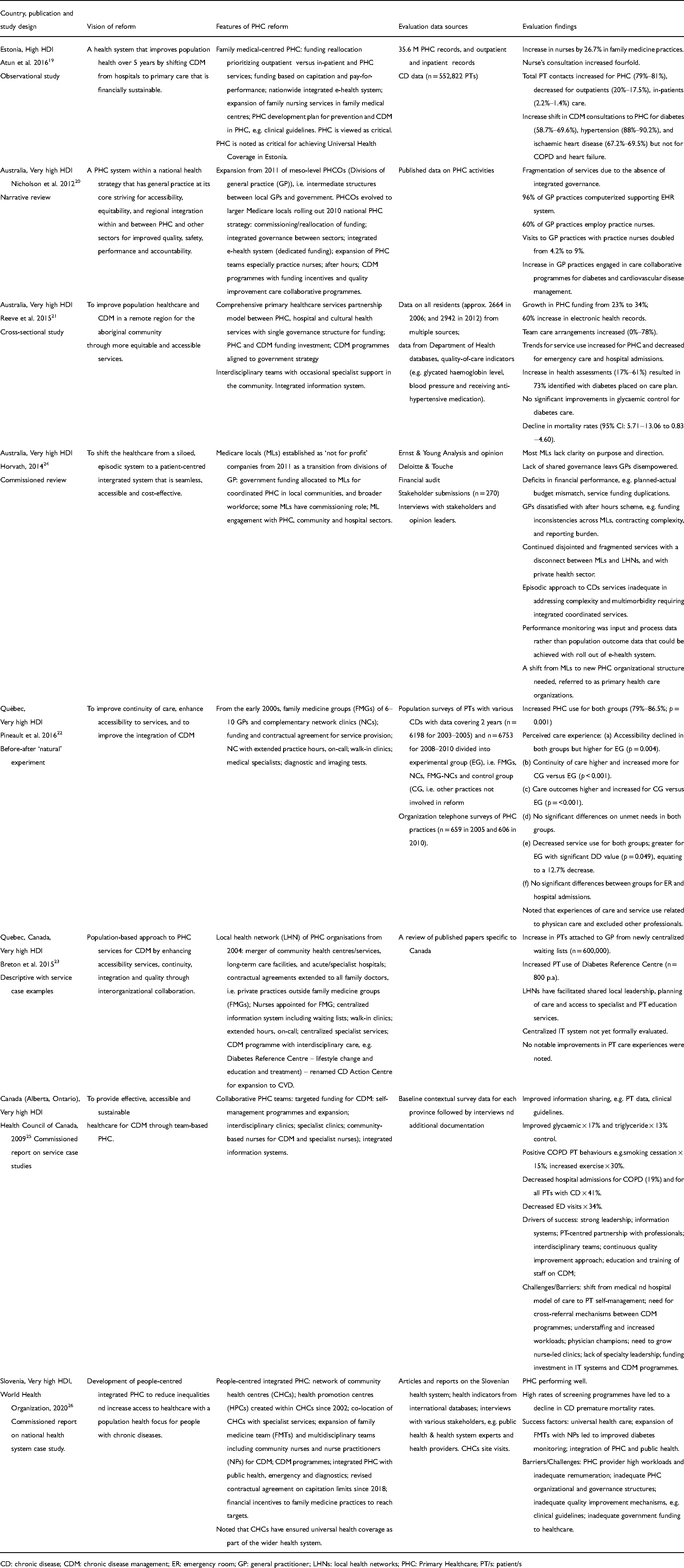
CD: chronic disease; CDM: chronic disease management; ER: emergency room; GP: general practitioner; LHNs: local health networks; PHC: Primary Healthcare; PT/s: patient/s
Quality assessment
We assessed the quality of studies19,21,22 and a narrative review 20 using relevant appraisal tools27,28 which are reported in Tables 2,3 and 4. Quality assessment was not applicable for the two case studies23,25 and the government report 24 since to date there are no published quality assessment criteria for PHC service case examples that are not reported as studies, and likewise regarding commissioned reports. Although the commissioned reports presented a case study on a national health system, 26 existing quality appraisal tools were not applicable because of a focus on clinical case–control studies27,29 rather than system level cases.
Quality assessment summary of before–after study.
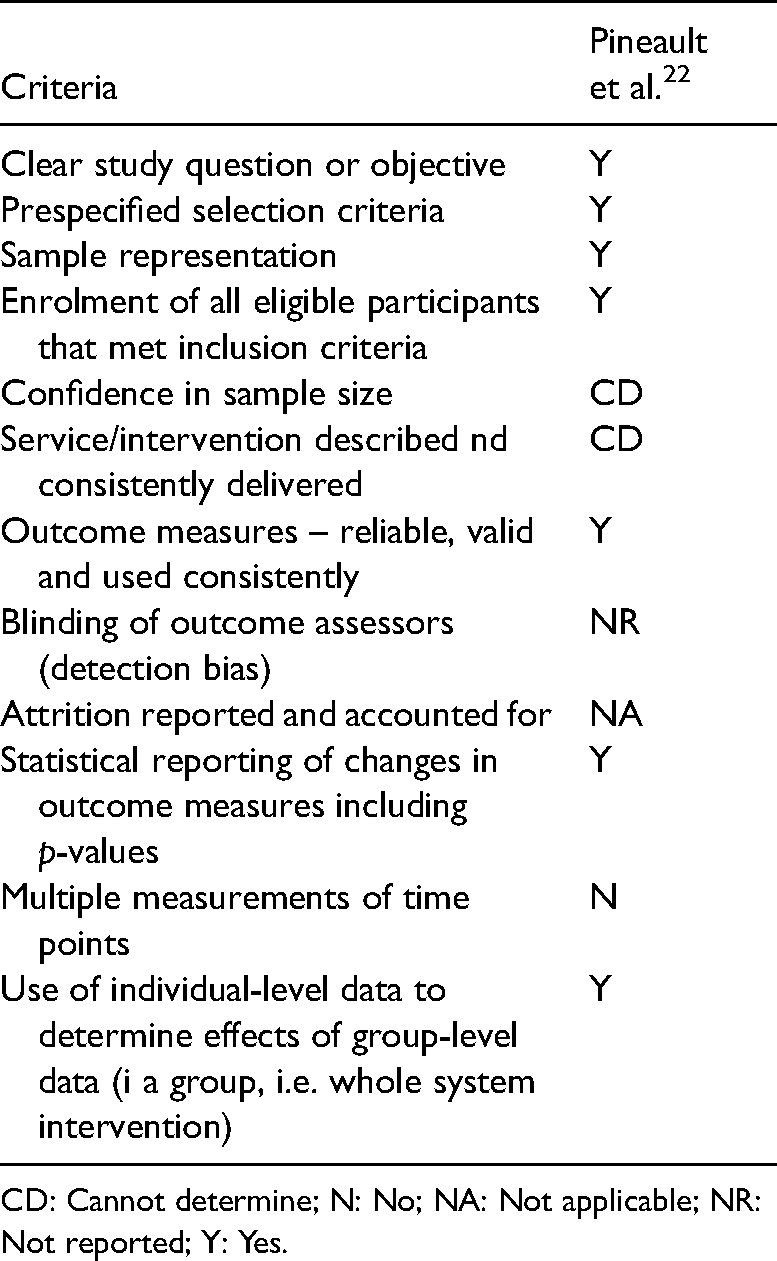
CD: Cannot determine; N: No; NA: Not applicable; NR: Not reported; Y: Yes.
Quality assessment for observational cohort and cross-sectional studies.
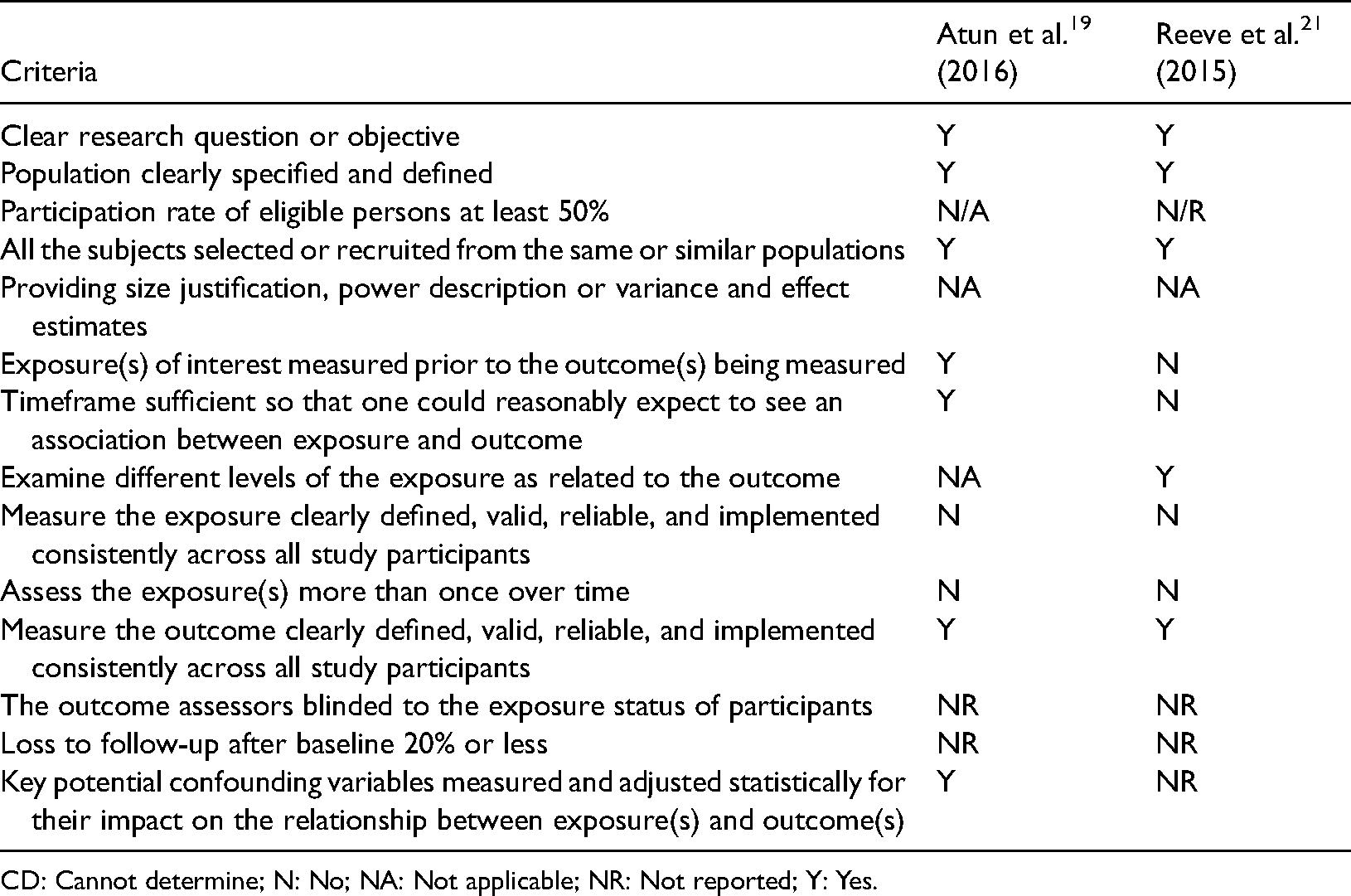
CD: Cannot determine; N: No; NA: Not applicable; NR: Not reported; Y: Yes.
Quality assessment for narrative review (Nicholson et al. 2012 20 ).
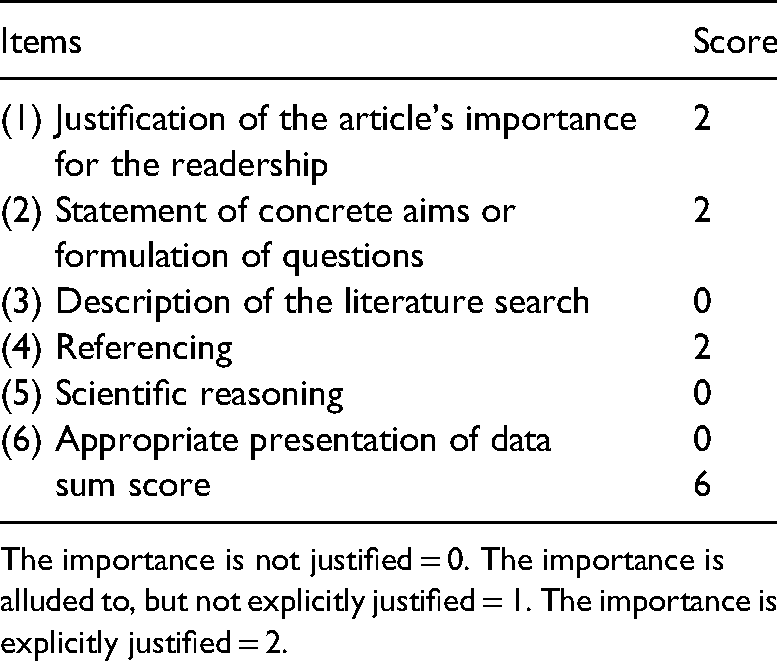
The importance is not justified = 0. The importance is alluded to, but not explicitly justified = 1. The importance is explicitly justified = 2.
The data for quality assessment were extracted by MA and cross-checked by CB. Quality assessment was discussed between all four reviewers to reach a consensus where differences arose.
Results
In total, eight articles are included in this analysis. In this section, the results are presented on PHC reforms under the following headings: characteristics of the studies/reports reviewed; the vision of PHC reform; features of PHC reform; and outcomes/impact of PHC reform.
Characteristics of articles reviewed
As presented in Table 1, of the eight articles reviewed, evaluation of PHC health system reforms were reported from four countries with high 19 or very high 21–26 HDI. The majority of articles reported on either Australia20,21,24 or Canada.22,23,25 The accounts of sampling varied across articles and for some was not explicit, therefore, making it difficult to determine the total population size of patients with chronic diseases represented in our review. Large populations sizes of patients were reported in three articles19,21,22 which ranged from almost 3000 residents from multiple sources 21 to over half a million patients sourced from health records. 19 Sampling also involved PHC activities, but the sample size was reported for Estonia only which involved over 35 million PHC records. 19 Of the eight articles reviewed, evaluations of PHC reform were conducted in three studies designed as observational cohort, 19 cross-sectional 21 and before–after study. 22 The remaining articles included a narrative review of published empirical data, 20 commission reviews 24 including service case studies and examples20,25 and a health system study. 26 Data sources for PHC reform evaluation varied across articles including PHC/service records and reports19,26 national statistical/health databases1921 or patient population records or surveys,19–22,27 interviews/surveys with various stakeholders (e.g. leaders, PHC practices),22,25,26 financial audits/reports,20,24 and published data in the literature.20,23,26 All eight articles addressed PHC within the context of multiple physical chronic conditions mostly referring to respiratory conditions,19,22,24–26 diabetes,19–26 cardiovascular19–26 and musculosletal22,25,26 conditions as a particular burden or to illustrate outcomes of PHC reform.
Quality appraisal
The before–after study 22 met most assessment criteria (Table 2). Although the sample size was large for both data collection time periods, power calculations were not reported, and so confidence in sample size could not be determined. Likewise, power calculations were not reported for the observational cohort and cross-sectional studies,19,21 results varied and details on some other criteria were not reported or could not be determined (Table 3). The quality assessment on the narrative review 20 met three of the six criteria regarding the justification of the article's importance for readership, explicit aims and supporting references for arguments made. Quality criteria not met in this review related to a description of search strategy, scientific reasoning concerning the sources (e.g. study designs) and quality of evidence and the presentation of concrete outcomes data (Table 4). Caution is needed, however, regarding the last two criteria since the SANRA scale 28 focuses on studies reporting on quantifiable clinical outcomes rather than policy literature which was included in Nicholson et al.'s review. 20 Further field testing for validity has been recommended. 28
PHC reform vision
The vision of PHC reform in relation to CDM related to improving population health through increased PHC accessibility20–26 and greater equity of services20,21,26 including affordable and financially sustainable healthcare.19,24,25 There was an emphasis on developing an integrated PHC system19–26 with reference to shifting CDM from specialist hospital-based services to PC and community health services. Healthcare reforms towards strengthening PHC were also envisioned as facilitating continuity of care for patients with chronic diseases,22–24 as well as improving quality of care.20,23
Features of PHC reform
Although countries varied in how they named the main focus of PHC reform (e.g. family medical-centred PHC, 19 local health networks (LHNs), 21 family medicine groups (FMGs)), 22 these variations reflect differences in terminology across countries rather than substantive differences between the types of reforms being implemented. Our analysis revealed that features of PHC reform across countries were more similar than different. The main features of PHC reform seen across articles reviewed related to the funding of PHC, PHC organization and infrastructure and PHC services for CDM.
Funding of PHC
All articles reviewed addressed funding implications of PHC reform.19–26 Government funding reallocation from hospital services to PHC and additional funding allocation and incentives to strengthen PHC services within the overall national health system were reported.19–26 For example, new provider payment mechanisms were introduced involving capitation and performance-related payments to motivate family doctors towards CDM in Estonia. 19 Funding through commissioning and contractual agreements with PC providers was reported for Australia,20,21 Canada22,23 and Slovenia. 26 For some countries, there was an explicit reference to targeted funding to support new initiatives such as implementation of Information Technology (IT) systems supporting data flow between sectors and access to electronic health records,20,25 expansion of PHC teams19,20,25,26 and the development and delivery of CDM programmes.19–21,23,25,26
PHC organization and infrastructure
Features of reform were found to relate to structural changes in the overall organization of PHC systems and to the implementation of infrastructural elements to support and strengthen PHC. There was evidence of health system reform evolving into new PHC organizational structures over time. For example, in Canada, Breton et al. 23 reported on the merger of community health centres, acute/specialist hospitals and long-term care facilities towards an integrated health system that provided population-based accessible services. This merger incorporated existing FMGs and LHNs. 23 The organization of PHC into networks or collaborative structures focusing on integrated and accessible services was also evident for Australia,20,21,24 and Slovenia. 24 In Slovenia, PHC was organized around a network of community health centres that were co-located with specialist services. 26 In Australia, the model of Divisions of GPs expanded to larger Medicare Locals20,24 from 2011 as part of the national PHC strategy. 20 Since the establishment of larger Medical Locals in Australia, a new model of PHC has been introduced named primary health networks (PHNs) aimed at integrating PC and public health. 30 While articles specific to evaluating PHNs within the context of CDM were not identified in our search strategy, PHNs will be raised later in the discussion section of this review. In addition, a partnership model for comprehensive PHC services was reported by Reeves et al. 21 for the aboriginal community with reference to different sectors coming together, namely PHC, community and hospital services. This partnership included a joint governance structure for the allocation of funding across the sectors. 21
The implementation of IT systems to support service integration across sectors was reported for Estonia, 19 Australia 20 and Canada. 23 A total of 265 IT systems were described as centralizing patient waiting lists 23 and facilitating the flow of patient data and information exchange between sectors and healthcare professionals. 19 There was no reference to implementing information systems for Slovenia, 26 a problem raised later when discussing the findings of the case study evaluating this country's PHC reform. Other infrastructural changes reported as part of PHC reform were expansion of multidisciplinary workforce in PHC,19–21,24–26 particularly nursing19,20,23,25,26 and service schemes such as extended or after hours,20,22,23 on-call and walk-in clinics. 23 These service schemes were introduced to improve continuity of care and increase accessibility to services. Accessibility and continuity of care was also a basis for integrating specialist services into CDM clinical care in PHC settings.21–23,25
PHC services for CDM
The findings presented above in relation to PHC organization and infrastructure provide insights into how health system reforms were intended to improve the management of chronic diseases at the point of service delivery by shifting CDM from hospital-based specialist services to patients accessing clinical care and support in the community. The descriptions of PHC reform for CDM across all countries indicated that GPs/family physicians primarily led out on and were at the core of PHC services. For example, family medicine was described as being at ‘the heart of primary health care’ in Estonia. 19 Likewise, the role of GP/family physician in Australia was described as critical to an effective PHC system that oriented healthcare away from hospital services, 24 and the expansion of PHC centres was GP led. 20 In Canada 23 and Slovenia, 26 PHC reform involved a shift towards formal enrolment of patients with family physicians in FMGs, 23 and positioning family medicine physicians as the first point of contact for services. 26
Although GPs/family physicians were noted to be at the centre of services in PHC reform, it was evident that other health professionals were seen as integral to CDM. An interdisciplinary approach involving multiple professionals for CDM was described as a feature of reform in all countries.20,25,26 apart from Estonia which referred to nurses only. 19 Nurses were specifically referred to as having a key role in CDM working in family medicine/GPs as family 19 /practice nurses,20,23 or as community nurses delivering services in community health centres.25,26 Furthermore, the provision of specialist services for CDM was reported with reference to healthcare providers having access to diagnostic services and medical specialists in PHC settings.21–23,25
There was evidence of targeted programmes developed for CDM in PHC with reference to a government strategy to address the burden of disease.19–21,25,26 Our analysis revealed that these programmes were developed for individual diseases20,21,23,25,26 with diabetes most commonly targeted first for implementing CDM in PHC.20,23,25 For example, in Quebec, Canada, a Diabetes Reference Centre to support CDM subsequently evolved to a Chronic Disease Action Centre to include patients with cardiovascular disease. 22 Some articles referred to these programmes being supported by quality improvement initiatives such as a quality bonus system to engage family doctors, 19 quality improvement care collaborations 20 and evidence-based clinical guidelines for managing individual diseases.19,20,25
Evaluation findings
For this review, we categorized the evaluation findings regarding national PHC reforms for CDM into the following broad areas: funding and financial costs; PHC organization and infrastructure; PHC service utilization; CDM programme delivery; and patient outcomes. These areas were identified by categorizing the findings reported across articles.
PHC funding and financial costs
Evaluation findings in relation to funding or associated financial costs were reported in four articles.21,25–27 Apart from one article, 21 there was evidence that funding allocation to support PHC reform was inadequate. For example, the actual budget allocated for PHC reform in Australia fell short of the planned budget. 24 The development and implementation of CDM programmes was a challenge in Slovenia and Canada due to inadequate funding,25,26 Despite the vision for the implementation of a national information system in PHC in Slovenia, this was not realized due to inadequate allocation of government funding. 26 Finally, at the level of general/family practice, funding incentives or remuneration for initiatives such as out-of-hours services were viewed unfavourably by GP/family physicians due to inconsistencies across regions, contracting complexities 24 or inadequate funding for the services provided. 26
PHC organization and infrastructure
Evaluation findings on PHC organization and infrastructure related to governance,20,21,24–26 information systems20,21,23–26 and workforce.19–21 Shared leadership at governance level was reported as a success factor in reforming PHC in Canada,23,25 whereas findings reported for Australia20,24 and Slovenia 26 were not favourable. Weak governance structures to support PHC reform in Slovenia has impeded the decision-making authority of directors of community health centres. 26 In Australia, the vision for an integrated health service between PHC and other sectors through Medicare Locals was not realized, and in the absence of shared governance, the services remained fragmented.20,24 The lack of or inadequate integrated information systems further contributed to fragmented services across some health sectors.20,24,26 Contrasting evidence was found in three articles relating to Canada23,25 and a remote region in Australia 21 which reported increased clinical information sharing and improved accessibility to services when information systems were integrated as part of PHC reform.
Although workforce expansion as a key area of reform was reported in most articles,19–21,24–26 only two articles provided data on this expansion with reference to nursing. The narrative review article from Australia which was based on published data on PHC activities reported that 60% of GPs sampled in 2009–2010 employed practice nurses. 20 In Estonia, it was reported that 27% of family medicine practices employed nurses. 19 There was some evidence from other countries to suggest that the workforce to support PHC reform for CDM was under resourced.25,26
PHC service utilization
The impact of PHC reform on service utilization of people with chronic diseases was reported in five articles19–23 with mixed results evident. The expansion of practice nurses in Australia was reported to double patient consultations to GP practices. 20 and likewise in Estonia, patient consultations to nurses in family medicine practices almost tripled. 19 A trend towards increasing PHC service use and decreasing use of hospital services was also reported.19,21,23,26 The evaluation of FMGs with complementary network clinics in Canada was reported to yield unexpected results on service use. 22 Pineault et al. 22 found that following PHC reform, there was no significant change in emergency or hospital admissions, and that accessibility to PHC services decreased. An explanation for these findings offered by the researchers was that service use and care provision was investigated in relation to physicians only and not other healthcare professionals. 22
CDM programme delivery
Outcomes reported on CDM programme delivery related to improvements in health assessment and patient monitoring.21,26 care planning21,23 and interdisciplinary collaborative approach to care.20,21 For example, an increase in health assessments seen in a partnership model between PHC and hospitals for an underserved community led to the majority of patients with diabetes being placed on care plans. 21 Breton et al. 23 also found that an interdisciplinary and intersectoral approach to delivering CDM facilitated care planning in patients with diabetes. Our analysis found little evidence of CDM programmes targeting chronic disease multimorbidity, a concern raised by Horvarth 24 who was critical of the continued episodic approach to CDM in Australia following implementation of Medicare Locals in PHC. He argued that episodic care is inadequate in addressing complex multimorbidity associated with chronic diseases.
Patient outcomes
Evidence on patient outcomes related to clinical indicators of disease status (glycaemic control and triglycerides),21,25 lifestyle behavioural changes, 25 mortality rates 26 and patient perceptions or experiences of care.22,23 Positive outcomes were reported in terms of declining mortality rates in Slovenia attributed to a heightened emphasis on health promotion and CDM. 26 Gylcaemic and triglyceride control as well lifestyle behavioural changes relating to smoking cessation and exercise were found to improve with team-based approaches to CDM. 25 Patients’ perceptions of their care experiences indicated no improvements or changes following reforms following the expansion of family medical groups and network clinics in Australia 22 (e.g. continuity of care, accessibility, unmet needs addressed) or for population-based PHC services for CDM in Canada. 23
Discussion
This systematic review was conducted to gain insight into the evidence from evaluations of PHC reforms for CDM implemented in countries with high or very high HDI. The findings indicate that between countries there were consistent motivating factors influencing PHC reform especially the need to shift away from specialist acute care for CDM. PHC reform at a population level is complex and fraught with challenges in relation to funding, governance, workforce, but a central factor is the engagement and involvement of GP/family doctors.
The vision to shift CDM away from specialist hospital services towards PHC as the first point of contact in the health system19–26 is consistent with the WHO's 2010 report urging the need to strengthen PHC systems to tackle the global burden of chronic diseases. 3 The need to strengthen PHC within national health systems of countries continues to be highlighted by the WHO 5 and other policy reports.31,32 Integrated PHC is a major focus of national health system reforms in countries such as the USA,33,34 the UK34,35 and other European countries 36 intended to reduce service fragmentation and inefficiencies,32,33,36 a focus also evident in our review.19–26
Integrated healthcare systems are complex involving interorganizational (e.g. primary and acute care; health and social services, PC networks) and interdisciplinary team collaborations to facilitate patient care coordination and continuity at the point of service delivery.37,38 Structural changes towards interorganizational collaboration were evident in our review including Medicare Locals (Australia) as new meso-level organizations linking government and frontline healthcare providers,20,24 LHNs (Canada) as mergers of community health centres, acute/specialist services and long-term facilities 23 and networks of community health centres co-located with specialist services in Slovenia. 26 PHC reform through interorganizational collaborations requires consideration for governance, funding, information and human resources as key strategies towards health system integration.34,38 Of the countries reviewed, most evidence of positive influences of these strategies was reported from Canada through LHNs 23 and collaborative PHC teams for CDM 26 such as patient enrolment with GPs through centralized waiting lists, 23 shared information/care planning23,26 and increased access to PHC for CDM including access to specialist care.23,26
Although some positive evaluations were found for Australia20,21 and Slovenia 26 such as greater GP engagement in collaborative CDM programmes 21 and increased use of PHC services for CDM,20,26 multiple barriers impeding interorganizational collaborations 38 were reported. These were a lack of shared governance and leadership,20,24,26 inadequate funding and funding inefficiencies and inequities,24,26 lack of stakeholder engagement24,26 and inadequacy of information systems to support data sharing between organizations and healthcare professionals.20,24,26 In Australia, these barriers impeded Medicare Locals in achieving integration leaving services for CDM fragmented, 24 a finding also reported about Medicare Locals concerning the broader context of health services. 29 Medical Locals have since been replaced by regional PHNs involving integration between PC and public health sector through shared goals and infrastructures, and close alignment with hospital networks. 30 In noting the multiple barriers herein, it must be acknowledged that the evidence is drawn from a small number of articles.
Integrating PC and public health is viewed as critical to shifting beyond curative and rehabilitative CDM to promotive and preventative services 30 and is more aligned to the broader concept of PHC within which PC is a component.12–14 In our review, apart from Slovenia, 26 explicit references to PHC reform involving the integration of PC and public health was lacking. A further gap concerning PHC reform for CDM relates to multimorbidity. The focus of CDM programmes on individual chronic conditions20,21,23,25,26 fails to take account of the increasing burden of multimorbidity on the health system and the challenges this presents to PHC providers working within a fragmented system with little integrated specialist support.39,40 A positive feature of PHC reform seen in our review was the expansion of multidisciplinary teams in PHC20,21,23–26 which can lead to integrated approaches to managing multimorbidity when these teams are located in the same PC practice as GPs. 39
In multistakeholder health systems, governance is viewed as an important ‘functional block’ to ensuring shared goals, policymaking and financing because of these impacts on PHC delivery and outcomes. 39 Apart from a regional partnership model from Australia involving a single governance structure and which reported increased funding allocation to PHC over time, 21 there was little evidence of shared governance found in our review. In the absence of integrated governance, funding and financing mechanisms will not be aligned to meet health service needs to the detriment of PHC delivery in general and CDM, 39 leaving healthcare providers dissatisfied with funding allocation, payment mechanisms and incentives which in turn runs the risk of PHC providers disengaging from health system reforms.24,26 The need for engagement with GPs/family physicians as a priority in reforming PHC was recommended by authors in our review.19,20,23–26 In this regard, lessons could be learned from the UK experiences of implementing Clinical Commissioning Groups involving GPs with decision-making authority concerning service provision, and flexible budgeting for service needs. 34
Strengths and limitations
A strength of this review is that a systematic approach was applied to searching, extracting, analysing and synthesizing the evidence. A challenge in undertaking the review was the heterogeneity of articles and how PHC reform was evaluated. Complex system-wide projects such as health service reforms are challenging to evaluate for researchers and this also applies to reviews of policy implementation. 41 The rigour applied to our approach helped identify the variations and consistencies across PHC reforms and the pattern of outcomes relating to the impact of these reforms. The inclusion of grey literature is a strength by providing a more balanced account of the evidence inclusive of negative findings therefore minimizing publication bias. 16 This review has some limitations. Only articles published in the English language were included, therefore, possibly missing evidence published in other languages. We included narrative reports as well as primary studies, therefore, yielding a heterogeneous selection of articles. Meta-analysis was not feasible and some articles were not eligible for quality assessment. A further limitation is that our focus was on physical chronic conditions to the exclusion of mental health conditions. The review is also limited by the exclusion of articles on single chronic conditions workforce articles that may have given additional insight into the PHC reform for chronic conditions. Given the vision for integrated PHC reform evident across countries, future reviews need to include mental health conditions and services.42,43
Conclusions
Our review showed a consistent trend in the vision for healthcare system reforms from predominately hospital-centric to PHC services towards an integrated health system for the management of populations with chronic conditions. This shift towards an integrated PHC system involving interorganizational collaboration such as network organizations is becoming an ambition of many countries worldwide. However, healthcare systems are complex. Unlike a clinical intervention which can be evaluated through a randomized controlled trial in terms of its effects on outcomes, health system reform is by far more challenging to evaluate. The breadth and scope of reform, as well as a lack of knowledge on the most appropriate methodologies, contribute to the complexities of health system evaluation. Notwithstanding these challenges, our review offers insights into the progress being made across a select number of countries including successes and barriers. It is evident that integrated PHC reform for CDM involving interorganizational collaboration requires shared governance, shared decision-making around funding and payment mechanism, multidisciplinary team expansion, and an integrated information system. GPs as clinical leads of PC practice have a key role to play in PHC governance and their engagement at this level needs to be strengthened in countries where this is weak. This finding points to the importance of policymakers engaging with GP, as key stakeholders, with consideration to their views and experiences in shaping the future direction of PHC reform for managing chronic conditions.
Supplemental Material
sj-doc-1-chi-10.1177_17423953211059143 - Supplemental material for Primary healthcare reform for chronic conditions in countries with high or very high human development index: A systematic review
Supplemental material, sj-doc-1-chi-10.1177_17423953211059143 for Primary healthcare reform for chronic conditions in countries with high or very high human development index: A systematic review by Mohammed Alyousef, Corina Naughton, Colin Bradley and Eileen Savage in Chronic Illness
Supplemental Material
sj-docx-2-chi-10.1177_17423953211059143 - Supplemental material for Primary healthcare reform for chronic conditions in countries with high or very high human development index: A systematic review
Supplemental material, sj-docx-2-chi-10.1177_17423953211059143 for Primary healthcare reform for chronic conditions in countries with high or very high human development index: A systematic review by Mohammed Alyousef, Corina Naughton, Colin Bradley and Eileen Savage in Chronic Illness
Footnotes
Acknowledgements
None.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and /or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Ethical approval was not sought or necessary because this review did not involve sampling human subjects.
Informed consent
Informed consent was not sought because there were no human subjects involved in the study and there were no issues requiring consent.
Author’s contribution
Two reviewers (MA, ES) screened the titles and abstracts of each article. Disagreements were resolved by discussion with the other reviewers (CN, CB). Quality appraisal was carried out independently by MA and ES. The data were extracted by MA and cross-checked by ES including the discussion between both authors to reach a consensus where differences arose. The synthesis was carried out by MA and reviewed by ES. All the authors contributed to the interpretation of the final findings and approved the final version of the article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.