
Abstract
Outpatient clinic access for patients diagnosed with non-emergent ocular conditions has been shown to decrease patient load in the Emergency Department (ED)/Urgent Care and improve patient satisfaction with care. We sought to quantify referral completion rates and ED/Urgent Care visit durations at a pediatric tertiary care center and analyze how demographic factors may influence these quality indicators. We discuss an overarching strategy to improve access to subspecialty care through a same-day access program. We retrospectively reviewed ED/Urgent Care patient encounters from 2019 to 2024. Patients diagnosed with conjunctivitis, vision loss, corneal abrasion, or iritis referred for follow-up care were included in this report. Visit duration in the ED/Urgent Care, referral completion rates, and patient demographics were analyzed. Seven hundred six patient encounters met the initial inclusion criteria. The average visit duration in the ED/Urgent Care per month was 3.36 hours (median, 3.45; IQR, 2.84-3.81), the average proportion of incomplete referrals per month was 21.9% (median, 20%; IQR, 10.6%-30%), and average proportion of ED/Urgent Care visits over 4 hours per month was 33.1% (median, 33.3%; IQR, 21.3%-43.5%). Demographic subgroup analysis (n = 411) revealed a relationship between age, insurance status, zip code, and race with completed referral rates and visit duration in the ED/Urgent Care. Our results indicate long visit durations in the ED/Urgent Care and a large proportion of incomplete referrals for patients with non-emergent ocular issues. A same-day access program could streamline access to subspecialty care by moving patients directly to the ophthalmology department from the ED/Urgent Care.
Keywords
Introduction
Parents are increasingly searching for convenient and timely access to healthcare for their children. Ophthalmologists, similar to other pediatric subspecialists, are typically busy practitioners with clinic schedules that are not amenable to adding additional patients on the same day. For patients seeking ophthalmic care, the dichotomy between the patient’s desire to be seen urgently and the physician’s inability to manage urgent issues easily in the clinic has led to an increase in Emergency Department (ED) and Urgent Care visits. 1 Patients seen by ED/Urgent Care personnel are treated by practitioners who are not subspecialty trained and have little expertise in ophthalmology. Channa et al 2 suggest that around half of patients seen for an ocular-related concern did not warrant hospitalization, and patients were instead referred for outpatient follow-up care.
For patients with non-emergent conditions that do not warrant an immediate ophthalmology consult, completing a referred ophthalmology appointment ensures appropriate diagnosis and management of an ocular condition. 3 Some literature suggests that patients who complete a follow-up appointment are less likely to revisit the ED for the same condition.3,4 In addition, patients seen in the ED wait an increased amount of time to see a doctor, pay increased fees, and generally have lower patient satisfaction with treatment provided.1,5 Despite the importance of adequate follow-up care, studies show that 25%-63% of patients do not complete their referred ophthalmology appointment from the ED.2,3,6,7
Referral completion rates and visit durations are key for increasing patient satisfaction, decreasing repeat admissions to the emergency department, and improving access to subspecialty care.1,5,8 This issue is especially pertinent in pediatric populations, where delays in care or mismanagement of ocular conditions can have long-term implications due to early childhood ocular development. 9 Patient demographic variables are another key factor for understanding referral completion rates and ED/Urgent Care visit durations. Pediatric patients from underserved or minority communities may face unique barriers, such as transportation difficulties or limited healthcare literacy.10,11 Identifying demographic disparities can help administrators and clinicians develop targeted interventions to improve access to subspecialty care. Limited research has been done to quantify these problems in pediatric populations, especially for ophthalmic diagnoses. 12
Accordingly, we sought to quantify referral completion rates and ED/Urgent Care visit durations at a pediatric tertiary care center and analyze how demographic factors may influence these quality indicators. After doing so, we aim to justify the adoption of a same-day access program, which could help redirect patients from the ED/Urgent Care to the outpatient ophthalmology clinic. We discuss the merits of this strategy in decreasing wait time to see a subspecialist, reducing the overall cost of medical care, and improving patient satisfaction.
Methods
This study was conducted in accordance with the principles of the Declaration of Helsinki, and this quality improvement project initiative was reviewed and determined to not meet the criteria for Human Subjects Research by Nationwide Children’s Hospital. We undertook a 5-year, single-institution retrospective chart review of all ED/Urgent Care visits for patients seen at our main facility during the hours of 8 AM and 3 PM for non-emergent ocular issues. These hours were chosen for direct comparability to our outpatient clinic’s hours of operation. Our main campus ED accepts patients from birth to 21 years old and is open 24/7 for appointments. The ED sees around 200 patients a day and has 46 patient beds. The Urgent Care department sees patients from 8 am to 10 pm daily. They see around 45 patients a day and have 18 beds. Both departments do not regularly staff subspecialty providers, such as ophthalmologists, but rather consult them frequently for emergent, vision-threatening concerns.
For patients who may have less severe symptoms, ED/Urgent Care providers may choose to schedule a referred appointment to the outpatient ophthalmology clinic for definitive care. The outpatient eye clinic typically sees 60-80 patients daily and employs pediatric ophthalmic subspecialists. Additionally, our institution contracts with a private outpatient ophthalmology clinic, which may accept patients recently seen at the ED/Urgent Care department. While these patients are not specifically referred there, they may opt to schedule an appointment at the private clinic as a follow-up.
From June 2019 to April 2024, patients diagnosed with conjunctivitis, vision loss, corneal abrasion, or iritis who were referred to the outpatient eye clinic were included in this report. These diagnoses have been reported as the most frequent, non-emergent ocular conditions presenting to the ED. 2 Quality indicators were defined as average visit duration in the ED/Urgent Care, the proportion of patients who waited over 4 hours, the number of patients referred to ophthalmology, and the rate at which these patients completed their referred ophthalmology appointment.
Any ED/Urgent Care follow-up appointments from the ED/Urgent Care made with the outpatient eye clinic or the contracted private ophthalmology office were considered referrals. Patients who no-showed or canceled their referred appointment were considered to be “Incomplete,” while patients who completed their appointment were considered “Completed.” Patients who were not referred to our outpatient ophthalmology clinic or contracted private office were excluded from this report. Visit duration was defined as the length of time a patient spent at the ED or Urgent Care from checking in to checking out.
A subanalysis was performed to assess the relationship between patient demographics, visit duration in the ED/Urgent Care department, and referred appointment status. Only patients who met the initial inclusion criteria and had demographic information available were included in the subanalysis (n = 411). Patients who denied any demographic questions were not included. According to Seaberg et al, 13 insurance status, lack of a primary care provider, language or immigration status, and socioeconomic status can influence rates of ED usage. For this study, age, sex, race, ethnicity, primary language, zip code, and insurance status were analyzed.
Some demographics were simplified for clarity and sample size considerations. “Latino/Hispanic/Unspecified,” “Latino/Hispanic/White,” and “Latino/Hispanic/Black” were grouped as “Latino/Hispanic” in the race category. “African” and “Black or African American” were grouped as “Black or African American” in the race category. “African,” “Asian,” “Hispanic,” and “Other” were grouped as “Other” for ethnicity to accommodate a small sample size. Insurance status was stratified as public insurance (such as Medicaid or Medicare), private insurance, or not insured. This information was determined at the time of the patient encounter.
Zip codes were grouped according to the CDC’s 2022 Social Vulnerability Index for Socioeconomic Status. 14 This index was used to group zip codes based on relative risk for poverty, lack of access to transportation, crowded housing, and additional community-level stressors. Those living in a Medium-High SVI zip code are more at risk than those living in a Low SVI zip code. Visit duration was grouped as either “High” or “Low,” with a “High” visit duration containing any appointment that took longer than 4 hours and a “Low” visit duration containing any appointment shorter than 4 hours. The outpatient eye clinic has a maximum appointment time of 3 hours; therefore, visit duration in the ED/Urgent Care was grouped for clearer analysis and comparability to the outpatient clinic.
Lastly, we examined ED/Urgent care revisits, which were defined as any additional ED/Urgent care encounters for the initial presenting ophthalmic condition that occurred within 3 months after the date of the initial ED/Urgent care encounter. Revisits that occurred more than 3 months after the initial ED/Urgent Care encounter were considered separate encounters.
Statistical Analysis
We reported the median, mean, and average for visit duration, proportion of incomplete referrals, and proportion of visits over 4 hours long. A chi-square test for association was used for univariate analysis. 15 Logistic regression modeling assessed the association between referral completion rates and various patient demographic factors and visit duration and various patient demographic factors. Unadjusted odds ratios (UOR) were reported for univariate analysis. P-values of ≤ .2 in the univariate analysis were entered in a multivariate logistic regression model, and backward elimination was carried out. Test significance was determined at α = .05, and adjusted odds ratios (AOR) were reported for multivariate analysis. A sample size analysis was conducted for the multivariate model with an anticipated effect size of 0.15, a desired statistical power of 0.8, 4 model predictors, and significance determined at α = .05. This determined a minimum required sample size of 84 encounters. All statistical analyses were conducted in R 3.6.0 (R Foundation for Statistical Computing) and Jamovi.16,17
Results
A total of 706 patient encounters met the initial inclusion criteria, and their charts were reviewed. The average total visit time for patients with non-emergent ocular conditions per month was 3.36 hours. The median proportion of patients whose total ED visit time was more than 4 hours to be seen was 33.3% (See Table 1). In all cases, patients were given a follow-up appointment with ophthalmology. On average, each month, 21.9% of patients either canceled or did not show up for their referred ophthalmology appointment. Over the 5-year-period, 32 patients continued to return to the ED/Urgent Care department (68 unique appointments) for treatment of the same condition despite having a referred ophthalmology appointment. This group of patients had an average incomplete referred appointment status of 25.0% and an average visit duration of 2.41 hours.
Referred Appointment Status and ED/Urgent Care Visit Duration Per Month.

Of the 706 patient encounters that met the initial inclusion criteria, 411 had demographic data available and were included in the demographic subanalysis. In this subanalysis, there were 235 males and 176 females with ages ranging from newborn to 20 years old (See Table 2). The majority of patients were white (43.3%) or Black or African American (34.5%). The majority of patients spoke English (84.9%). A total of 258 (62.8%) of patients had private insurance, while 135 (32.8%) held public insurance. Most patients were also from a Medium-High SVI zip code (72.7%).
Characteristics of Non-Life-Threatening Ocular Diagnosis in a Pediatric Emergency/Urgent Care Department.

Note. Patient demographic counts for secondary inclusion critera (n = 411) and chi-square analysis.
p < .05. **p < .01.
No statistically significant differences were found concerning sex, language, and ethnicity with visit duration and referral completion rates (See Table 2). There were significant differences for race, zip code, and insurance type with visit duration at the ED/Urgent Care (See Table 3). Black or African American patients were 60.4% less likely to have a “Low” visit duration (<4 hours) than their white counterparts (UOR = 0.396; 95% CI, 0.241-0.651; p < 0.001). Patients were 44.5% less likely to have a “low” visit duration if they lived in a Medium-High SVI zip code compared to a Low SVI zip code (UOR = 0.555; 95% CI, 0.336-0.917; p = 0.022). Insurance status also outlined a relationship with visit duration, indicating that patients with public health insurance were 49.5% less likely to have a “Low” visit duration than those on private health insurance (UOR = 0.505; 95% CI, 0.328-0.779; p = 0.002).
Odds Ratios for Visit Duration and Referred Appointment Status Associated with Patient Demographic Factors.

Note. Significance of demographic variables on visit duration and completed referred appointments. OR= Odds Ratio, CI = Confidence Interval.
*p < .05. **p < .01.
Only zip code and insurance status yielded a significant relationship with referred appointment status. Patients living in a Medium-High SVI zip code were more likely to have completed their referred ophthalmology appointment than those living in Low SVI zip codes (UOR = 4.390, 95% CI, 1.706-11.292; p = .002). Additionally, patients with public health insurance were more likely to complete their referred ophthalmology appointment than those on private health insurance (UOR = 2.218; 95% CI, 1.202-4.049; p = .011).
Multivariate Analysis
Sex, language, and ethnicity were not significantly associated with visit duration and referral completion rates, were below the threshold range, and therefore excluded from the multivariate analysis. Age and race, although not statistically significant for referred appointment status, were retained in the multivariate regression model as a priori.
For visit duration, race, and age were found to be statistically significant upon multivariate analysis (See Table 3). Patients who identified as Black or African American were 53.8% less likely to have a “low” visit duration than white patients (AOR = 0.462; 95% CI, 0.260-0.824, p = .009). Upon analysis, age was also found to be significant, with every additional year of age, the odds of a “Low” visit duration increase by almost 5% (AOR = 1.048, 95% CI, 1.005-1.094, p = .030). When looking at referred appointment completion rates, the only significant relationship on multivariate analysis was zip code, with those living in Medium-High SVI zip codes being more likely to complete their referred ophthalmology appointment than those living in Low SVI zip codes (AOR = 3.726; 95% CI, 1.423-9.757, p = 0.007). The AUC for both models was 0.66.
Discussion
We evaluated visit durations, referred appointment completion rates, and the relationship between these quality indicators and patient demographic factors. For this study, an association was found between age, race, zip code SVI, and insurance status on referral completion rates and visit duration in the Emergency and Urgent Care department. Furthermore, we identified that one-third of patients had long visit durations at the ED/Urgent Care and around a quarter of all patients reviewed did not complete their referred ophthalmology appointment. While patients had non-emergent conditions, meaning they did not warrant an immediate ophthalmology consult, they were still ultimately referred to an ophthalmologist for definitive care and treatment. For physicians and clinical practices, understanding how to increase completed referred appointments and decrease visit duration in the hospital has been shown to lead to better patient satisfaction and health outcomes by ensuring timely care and reducing delays in diagnosis and treatment.18,19
During this study, only 32 patients returned to the ED/Urgent Care department more than once for treatment of the same condition despite having an ophthalmology follow-up appointment. These patients often had shorter wait times and had comparable referred appointment completion rates to the larger cohort. This subset of patients was therefore viewed as outliers and were not analyzed as a specific cohort.
Appointment Visit Durations
Due to the availability and objectivity of the measure, appointment visit durations have been used as a quality indicator for many projects focusing on patient satisfaction and healthcare delivery improvement.5,20 In the ED/Urgent Care Department, long visit durations can lead to overcrowding, which contributes to greater physician burnout, worse patient satisfaction, and greater costs to the healthcare system as a whole.1,21,22 Overall, we found that patients presenting to the ED for non-emergent conditions have considerable visit durations and about a third of patients have visits that are more than 4 hours. Typically, an outpatient appointment at the ophthalmology clinic takes up to 3 hours for a complete, dilated eye exam and less than 2 hours for a follow-up, non-dilated exam. This identifies a problem for patients, as they wait longer for less definitive care, wasting time, money, and resources.
Additionally, our results indicate a relationship between patient demographic factors and longer ED/Urgent care visit durations, which may help hospital organizers identify patients most at risk for longer visits. For example, when controlling for other covariates, age may play a role in ED/Urgent Care visit durations. We discovered that for every year older, patients were more likely to have shorter visit durations. For younger patients and newborns, it may be more difficult for non-specialized clinicians to perform a thorough eye exam, which may extend visit times. This pattern of findings extends beyond age, as we also observed a relationship between race and visit duration in the ED/Urgent Care department, a topic with mixed support in the existing literature.20,23 -25
We found that patients who identified as Black or African American were more likely to have longer visit durations compared to white patients, even while controlling for other covariates. The discrepancy in the literature may be due to the variables analyzed, our focus on a pediatric population, and the lack of knowledge on the direct mechanism for how race plays a role in patient encounters. Implicit bias has been discussed as a potential factor contributing to disparities in quality of care, decision-making, and treatment recommendations. As discussed in Ghosh et al, 24 failure in proper communication due to implicit bias may result in exacerbated visit durations and increasing distrust between patient and provider. Implicit bias is difficult to measure directly, however, and further research into this area of physician-patient interaction is needed to fully understand the issue.
We also determined that patients with public health insurance were more likely to have a longer visit duration in the hospital than patients with private insurance, which is consistent with previous literature.20,23 Previous literature has described how patients with public health insurance may face more barriers to care, including resource allocation, administrative burden, and more chronic or advanced conditions than those with private health insurance.1,20 Upon multivariate analysis, insurance status did not indicate a significant relationship with appointment visit duration. The longer ED/Urgent Care visits observed among public insurance patients may reflect systemic inefficiencies that disproportionately impact lower-income populations, which may not be easily controlled for upon logistic regression. Future research should seek to understand how addressing differences in insurance status could improve equity, reduce resource strain, and enhance patient outcomes.
Another factor that could contribute to healthcare inequity is geographical location. We determined that patients living in a Medium-High SVI zip code are more likely to have a longer visit duration, which has been indicated in previous literature where lower socioeconomic living may be associated with an increase in visit duration.25,26 Nguyen et al 27 suggests that although many hospital systems are in urban areas with low socioeconomic status (SES), the patients living in these areas may face more challenges when trying to receive care. For patients coming from Medium-High SVI zip codes, providers may need to address more than the original ophthalmic concern. For example, there is a growing body of research suggesting that integrating social care into healthcare may improve overall health outcomes for patients.28,29 However, when addressing multiple concerns at an appointment, physicians may feel overwhelmed, lack sufficient time, and be unaware of concrete actions they can take to address patient concerns.30,31 Therefore, patients from Medium-High SVI areas may experience longer ED/Urgent Care visits due to medical complexity and face systemic inequities that exacerbate these durations. This suggests a need for further research to replicate these findings in diverse populations and geographical locations to better understand the underlying factors contributing to this problem.
Referred Appointment Completion
Our study contributes to continued research indicating a relationship between patient demographic factors and referred appointment completion rates. Our total proportion of completed referred appointments (75.4%) is comparable to some previous research3,32 but much higher than others.6,7,33 Unlike previous literature,27,34 we determined that patients with public health insurance were more likely to complete their referred appointments than those with private health insurance. This may be due to patients with private health insurance seeking care at other private ophthalmology offices that could not be accounted for in this study, which may create a falsely elevated number of patients with private health insurance not completing referred appointments. Other research has indicated that those relying on Medicaid or who are uninsured may face challenges returning for appointments because of out-of-pocket costs, inflexible schedules, and unexpected expenses.27,34 These findings highlight the complex interplay between insurance type and healthcare access, emphasizing the importance of addressing systemic factors influencing follow-up care patterns.
Like longer visit durations, geographical location may also play a role in identifying patients who have high-risk factors for missing appointments. We found that patients with Medium-High SVI zip codes were more likely to complete their referred ophthalmology appointment. Our hospital is located in the center of a larger urban area, which is classified as a Medium-High SVI zip code. The majority of the suburbs in the area are classified as a Low SVI zip code. As such, patients who have to drive longer distances for their referred appointment may opt to see a provider closer to home or may be more likely to miss their appointment. Other literature has indicated a relationship between rural vs. urban location on healthcare accessibility, with patients in rural areas often having to travel much longer distances to receive care, which may increase their likelihood of not completing their referred appointment.34,35 However, this geographical dichotomy ignores challenges in healthcare accessibility across urban landscapes.
Nguyen et al 27 notes that neighborhoods with lower SES indicators experience significant transportation, financial, and time constraints contributing to decreased appointment show rates. These challenges are particularly pronounced in areas where access to healthcare is limited, and patients may struggle with logistical barriers such as unreliable public transportation or, for parents of pediatric patients, allocating time off from work and school. Some research has suggested that by focusing on specific patient cohorts with low SES, hospital organizers may be able to identify patients who are the most at risk for missing their appointments and develop interventions to reduce the disparity.35,36 When controlling for multiple covariates, only the SVI zip code continued to show a relationship with appointment completion rates, highlighting it as a potential factor for identifying high-risk patients. Some researchers have developed predictive models to identify patients who are at risk for a high rate of incomplete referred appointments. 35 Further development of these predictive models may help clinical administrators use a data-driven approach to mitigate the impact of incomplete appointments and support patients with high-risk factors.
Same Day Access Program
To combat long visit durations for ED/Urgent Care appointments and the rate of incomplete referrals, we suggest streamlining patients from the ED/Urgent Care department to the outpatient eye clinic. A same-day access program has been shown to improve patient wait times for treatment, improve referral completion rates, and save them the cost of an ED visit.1,37 Longer visit durations, referral completion rates, and costly ED visits have previously been identified as indicators for lower patient satisfaction with subspecialty care.1,13,38 Telemedicine appointments have been suggested as a method to improve referred appointment show rates and patient satisfaction with treatment. 18 However, this presents a unique challenge in ophthalmology due to the need for specialized equipment, limitations in visual acuity testing, and the need to physically interact with the ocular area.
We believe these results support the need for a same-day access to ophthalmology program. Same-day access to ophthalmology programs have been developed and described in the adult literature.1,37 A same-day access program would allow patients to receive immediate specialty care for their ocular condition by directly sending them to our outpatient eye clinic, which is in the same building as the ED/Urgent Care departments. For patients who have moderate ophthalmic concerns that warrant referral to a subspecialist but who are not in life-threatening condition, a same-day access program would allow them to see a subspecialist sooner and reduce the cost of an emergency visit. Additionally, by seeing a subspecialist the same day, patients would be getting definitive care sooner and be better established for follow-up appointments. Appointment visit durations may also decrease because patients would be worked into the outpatient appointment times instead of waiting in a potentially overcrowded ED/Urgent Care. Healthcare delivery may be improved by decreased crowding in the ED/Urgent Care from non-emergent patients. These types of programs have not been developed in the pediatric setting. We are currently implementing a system to facilitate same-day ophthalmology access in our hospital.
This system requires a well-defined protocol with established criteria to evaluate a patient with a vision complaint. We have suggested a protocol that the emergency triage nurse can use to facilitate this decision-making process (Figure 1). Future research will be conducted by monitoring the rate of correctly triaged patients, total service time, and referred appointment show rates. Our goal is to work toward improved access to ophthalmology and definitive subspecialty care for patients presenting to the emergency room with non-emergent ocular issues.
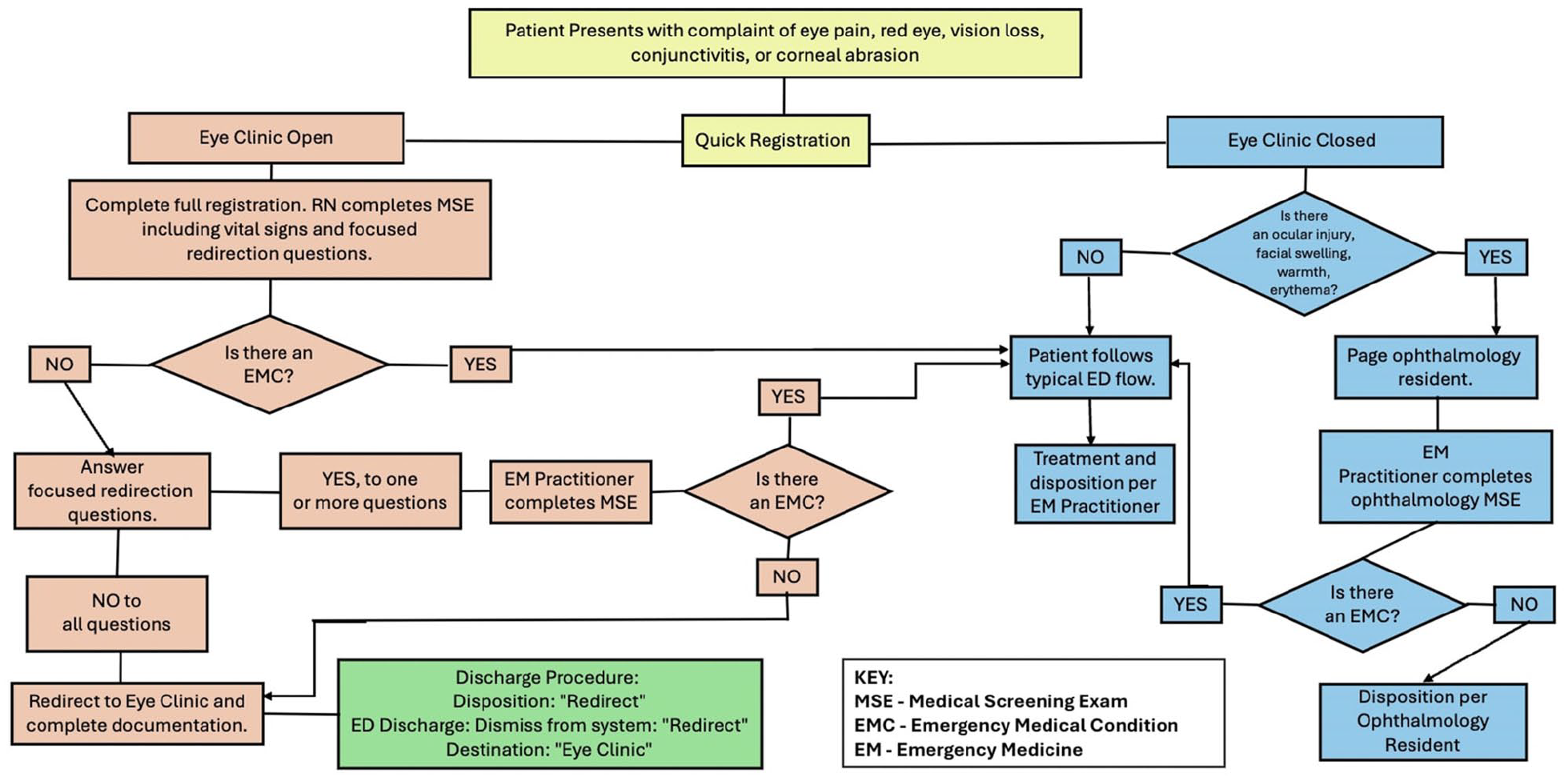
Direct access to the eye clinic. Proposed screening for triage nurses in the ED and urgent care department.
Limitations
A few limitations of this study minimize the generalizability of the results. First, the duration of each visit was determined by taking the difference between admission and discharge times, which does not distinguish between wait time and treatment time. Additionally, while repeat admits were minimal (n = 32 patients, n = 68 unique encounters), they were not excluded in the report and may artificially inflate or deflate patient demographic information. Although this report analyzed multiple patient demographic variables, we did not include all possible indicators for long visit duration and incomplete referrals. For example, Otto et al 39 have suggested that the day of the week may impact a patient’s visit duration in the ED, with particularly high-use days of the week increasing wait times.
Both multivariate models for visit duration and referred appointment status showed moderate discriminative ability with an AUC of 0.66, indicating that it can distinguish between the classes 66% of the time. While this is better than random chance, it suggests that further improvements are needed for predictive accuracy. The model fit may be hindered by a class imbalance, such as the relatively low number of patients (n = 411) with incomplete referrals (18.2%) that had demographic information available to analyze. This may reduce the generalizability of our models.
Some studies have developed more robust regression models to identify the relationship between patient demographics and appointment show rates, 27 which may inform future research. Our analysis was confined to the demographic variables available within a retrospective chart review, limiting statistical testing.
Conclusions
As more patients utilize the Urgent Care and ED for subspecialty care, direct access to ophthalmology for definitive evaluation and treatment is a growing issue. Our study finds long visit durations in the ED/Urgent Care department and high rates of incomplete referrals for outpatient ophthalmology care in pediatric populations. Additionally, our study identifies a relationship between some patient demographic factors and quality indicators for patient satisfaction. A same-day access program that fast-tracks a patient from the ED/Urgent Care to the outpatient eye clinic will decrease patient visit durations, costs from emergency visits, and improve subspecialty access. Further study into the benefits of a same-day access program in pediatric populations is needed to analyze the potential benefits and costs of such a program.
Footnotes
Author Contributions
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations/Consent
The quality improvement project initiative was reviewed and determined to not meet the criteria for Human Subjects Research by Nationwide Children’s Hospital IRB. This project does not satisfy the definition of “research” under The US Department of Health and Human Services code 45 CFR 46.102(d). Therefore, there is no requirement under these regulations for such activities to undergo review by an IRB, or for these activities to be conducted with provider or patient informed consent.