
Abstract
The increasing elderly population has led to a rise in the demand for long-term care services, prompting the adoption of long-term care insurance (LTCI) as a crucial solution. Since 2012, China has been conducting a pilot LTCI program, gradually expanding its coverage. Utilizing the survey data from China Health and Retirement Longitudinal Study (2011-2018), we employ the difference-in-differences method to examine the health effects of LTCI. We find that LTCI significantly decreases the probability of outpatient visit by 7.1 percentage points, the number of outpatient visits by 0.208 times, and outpatient expenditure by 65.8%. Additionally, LTCI improves self-reported health and life satisfaction, and reduces the probability of smoking. LTCI results in health benefits, particularly notable for individuals with more than 2 chronic diseases, lower household consumption, females aged over 62, or those enrolled in more generous programs.
With the rapid aging of the population, long-term care (LTC) services are in urgent need for people with chronic diseases or disabilities. In response, the introduction of long-term care insurance (LTCI) has been seen as one means of tackling this challenge.
This study utilizes the difference-in-differences method to examine the impact of LTCI on healthcare utilization, health outcomes, and health behaviors, building upon prior research. Furthermore, we investigate the diverse health effects of LTCI across different policy frameworks in China.
Our study provides policy references for introducing LTCI in both urban and rural regions to address issues of the rapid aging population in developing countries.
Introduction
With the rapid aging of the population, long-term care (LTC) services are in urgent need for people with chronic diseases or disabilities. 1 Compared to other countries, China faces bigger challenges. 2 In 2018, the number of people aged 60 years and older reached 17.90%; about 11.90% of the Chinese population was aged 65 years and older. Additionally, the disabled and semi-disabled population in China at the end of 2020 is 42.5 million, accounting for 17% of the elderly who are in urgent need of LTC. The increasing population aging and the surge in the number of disabled elderly have posed a series of challenges to society, firstly, the rising cost of medical care, 3 secondly, the heavy burden of family care, 4 and finally, the difficulty in ensuring the quality of life of the disabled elderly in their old age. 5 How to cope with the above challenges and help healthy aging has become a common focus of attention in various countries.
In response, the introduction of long-term care insurance (LTCI) has been seen as 1 means of tackling this challenge.6 -8 For instance, countries with an aging population, such as the United States, Germany, the Netherlands, Japan, Korea, and Israel have established LTCI to meet the LTC needs of older people with disabilities.6,9 -11 In addition to enabling frail older people to live a dignified life, LTCI also brings many potential benefits, including reducing improper use of acute medical services, helping families avoid high medical expenses, and freeing women to bear multiple social functions. 12
Up to now, previous studies have examined the effects of LTCI on healthcare utilization and health outcomes in different counties. However, the results of these studies are mixed. Specifically, some studies show that the services provided by LTCI can reduce healthcare utilization, such as preventing frail older people from being admitted to the hospital.7,8,12 -15 Among these, Costa-Font et al 14 find robust evidence of reducing inpatient admissions in Spain. Rapp et al 16 show that patients with Alzheimer’s disease experience a significant decrease in the lower rate of emergency care in France. Lei et al 17 examine the impact of LTCI on the well-being of older adults and their families using data from the Chinese Longitudinal Healthy Longevity Survey. The results show that LTCI reduces the unmet care needs, informal care intensity, care expenditures, and out-of-pocket medical expenditures of older adults while being more sufficient to improve their health outcomes, and this study provides useful insights for this paper.
On the contrary, other literature finds that the introduction of LTCI is positively correlated with the increased care needs of beneficiaries, 18 thus increasing healthcare utilization. It has also been documented that LTCI affects informal care and thus improves beneficiaries’ quality of life and spousal caregivers’ well-being.19,20 On the other hand, LTCI improves the health outcomes of beneficiaries by providing professional care and disease management.14,21 -24 Therefore, the impact of LTCI on healthcare utilization and health outcomes is still mixed and needs further analysis.
This paper has made some contributions to the previous literature in the following ways. First, by exploiting a quasi-experiment of introducing LTCI in China, this study uses the difference-in-differences method to examine the impact of LTCI on healthcare utilization and health outcomes, which contributes to previous studies on LTCI. Second, we further investigate the impact of LTCI on health behaviors, while the previous studies concentrated on healthcare utilization and health outcomes may underestimate the beneficial effects of LTCI. Third, we examine the heterogeneous effects of LTCI on healthcare utilization, health outcomes, and health behaviors by the LTCI policy designs in China. Finally, our findings provide policy implications for introducing LTCI in both urban and rural regions to address issues of the rapid aging population in developing countries.
The rest of this paper is structured as follows. Sections 2 and 3 present the institutional setting and literature review. Section 4 describes the data. Section 5 outlines the estimation strategy. Section 6 reports empirical results, including preliminary empirical results, parallel trend tests, and heterogeneous analysis. Sections 7 and 8 provide the discussion and conclusion.
Institutional Background
China has been establishing the LTCI pilot for frail older people since 2012. 25 More specifically, Qingdao became the first city to implement LTCI in China, taking the lead in launching a pilot program in urban areas in July 2012 and expanding the system to rural areas in 2015. 26 In June 2016, the General Office of China’s Ministry of Human Resources and Social Security issued guidance and determined to carry out pilots in 15 pilot cities (Qiqihar, Chengde, Nantong, Suzhou, Ningbo, Anqing, Jingmen, Guangzhou, Chengdu, Shihezi, Shangrao, Shanghai, Chongqing, Qingdao, and Changchun). 17 On September 16, 2020, the National Healthcare Security Administration and Ministry of Finance of the People’s Republic of China issued guidance on expanding the LTCI system pilot, adding 14 extra pilot cities. So far, there are more than 49 pilot cities for LTCI in China.
LTCI in China provides 3 types of service benefits: home care, institutional care, and hospital care. 1 More specifically, home care and institutional care mainly contain 42 specific services, divided into 2 categories: primary life care and common clinical care, such as head and face cleaning and grooming, bathing, assistance with feeding/water, excretion and incontinence care, self-care training, nasal feeding, and stoma care. Also, hospital care is carried out under medical treatment items, medical service facilities, and medication used by medical insurance.
Literature Review
Previous literature documents that LTCI has a dual effect on healthcare utilization, including a substitution effect and an income effect. The substitution effect refers to the fact that LTCI provides professional medical services to older people with disabilities, which reduces the demand for healthcare such as intensive care units, thus reducing the overall utilization.6,8,27,28 Instead, the income effect means that LTCI provides a higher percentage of compensation for disabled older people, which reduces the care burden. The previously suppressed demand for healthcare will translate into increased utilization due to an income effect, while the savings in medical care costs will indirectly boost income, further stimulating demand for healthcare services.22,29 Thus, the impact of LTCI on healthcare utilization depends on the relative strength of the substitution effect and income effect, which is subject to empirical analyses. In this context, we try to fill the gap and analyze whether and how LTCI affects healthcare utilization from multiple dimensions.
In addition, previous studies show that LTCI effectively improves the health outcomes of disabled people to some extent. Stabile et al 30 find that publicly financed home care in Canada significantly increases self-reported health. Sohn et al 31 find that LTCI in South Korea significantly reduces the mortality rate. Lei et al 17 and Tian et al 32 find that LTCI in China, for older people with baseline need for care, increases the likelihood of reporting good health.
Moreover, several common behavioral risk factors are found to be associated with health problems and the potential increase in healthcare utilization, including smoking, drinking, and obesity. 33 Specifically, alcohol and tobacco intake have been identified as significant public health burden that contributes to several diseases as well as increased mortality.34,35 Research has shown that primary care providers’ efforts to influence patients’ personal health behaviors can promote health behaviors that lead to better coping with symptoms, adherence to treatment regimens, and engagement in the prevention of future illnesses. 36 For example, primary care providers rely on “information power” (information about health and disease) and “expert power” (professional credentials) to persuade patients to change their behavior. 37 Similarly, long-term care providers are able to improve health behaviors to some extent. Based on the literature, we hypothesize that:
H1: LTCI leads to the improvement of health outcomes and health behaviors.
Moreover, previous studies show that there exists a heterogeneous effect of LTCI on healthcare utilization and health outcomes across different groups by gender, age, income, and living arrangement.1,17,31 For example, as for age issue, Feng et al 1 find that LTCI has a greater negative effect on inpatient care utilization for people over 80 years old. Also, Lei et al 17 find that LTCI matters more for those with lower income, residing in communities with social services, or covered by more generous programs.
Furthermore, previous studies find that the effects of LTCI vary by the LTCI policy designs.17,38 In China, there are 2 main categories of target people who are eligible for LTCI benefits: moderately and severely disabled people. The severely disabled are defined as “persons who have been bedridden for more than six months, have lost the ability to take care of himself/herself, and are adopted by most cities.” 38 Based on the severely disabled, some cities have expanded the recipients, such as Guangzhou, Shanghai, and Suzhou to include people with moderate disability in the scope of treatment recipients. 17 Xiao et al 38 find that caregivers in LTCI pilot cities with both severe and moderate disabilities provide more labor supply than in cities with only severe disabilities. Lei et al 17 find that the introduction of LTCI has a bigger effect on healthcare utilization and health outcomes for those people eligible for both moderate and severe disability. On top of that, studies show that the effects of LTCI vary by reimbursement ceiling. Lei et al 17 find that compared with a low reimbursement ceiling, LTCI significantly decreases the care expense and medical expenses, increases the likelihood of self-reported good health, and reduces depression in pilot cities with high reimbursement ceiling. Based on the literature, we hypothesize that:
H2: The effect of LTCI in China vary across different demographic characteristics and policy designs.
Data
The data used in this paper is from the China Health and Retirement Longitudinal Study (CHARLS), which is conducted by the National of School Development at Peking University. Similar to the US Health and Retirement Survey, the English Longitudinal Study of Aging (ELSA), and the Survey of Health, Aging and Retirement in Europe (SHARE), the CHARLS is a biennial survey, designed to collect a nationally representative sample of urban and rural residents aged 45 years and older. 39 There were 17 706 respondents, covering about 10 000 households in 150 counties/districts and 450 villages/resident committees in the 2011 baseline national wave of the CHARLS. Besides, the CHARLS provides multiple dimensions of health information, including individual-level healthcare utilization, health outcomes, and health behaviors information.
This paper uses the 2011, 2013, 2015, and 2018 waves of CHARLS. The primary coverage of LTCI is for beneficiaries who participate in the Urban Employees Basic Medical Insurance (UEBMI), and some cities have extended the coverage to other residents. For the sake of consistency, we draw on data on individuals who participate in the UEBMI. According to the CHARLS report, Chinese people aged 50 to 54, 55 to 59, 60 to 64, 65 to 69, 70 to 74, and 75 and above have difficulties in the Activity of Daily Living Scale (ADL), which is 7.5%, 13.2%, 19.3%, 26.8%, 33.1%, and 45.9% higher than the 45 to 49 age group, respectively. In addition, most people with LTC service needs have underlying medical conditions. Therefore, to improve the representativeness of the survey sample, we restrict the sample to those aged 50 years or older and suffering from at least 1 chronic disease. Moreover, as key contact provinces of LTCI, Shandong province, and Jilin province have more discretionary to decide the scope and timing of the LTCI pilot, which may produce self-selection bias. Thus, we exclude Shandong province and Jilin province, and the rest treatment group is the 11 pilot cities, including Qiqihar, Chengde, Suzhou, Ningbo, Anqing, Jingmen, Guangzhou, Chengdu, Shangrao, Shanghai, and Chongqing in China. Then, we exclude some observations when our key dependent variables are missing. Eventually, we obtain 5208 person-year observations.
Outcome Variables
Dependent variables in this study consist of healthcare utilization, health outcomes, and health behaviors. Healthcare utilization contains outpatient care and inpatient care. Outpatient care includes the probability of outpatient visit, number of outpatient visits, and outpatient expenditure in the last month preceding the survey date. Inpatient care comprises the probability of inpatient admission, the number of inpatient admissions, length of stay (LOS), and inpatient expenditure in the past year preceding the survey date.
Health outcomes include self-reported health, life satisfaction, and depression. Among these, self-reported health includes 5 answers: “very poor,” “poor,” “fair,” “good,” and “very good,” which are assigned values from 1 to 5. As a comprehensive evaluation index, self-reported health can reflect the individual’s judgment on the severity of existing diseases and undiagnosed health problems with symptoms and is considered an important health evaluation index. 40
In addition, this paper adds life satisfaction, a comprehensive indicator that is essential for measuring the well-being of the elderly, with values ranging from 1 to 5. Existing literature shows that the life satisfaction of the elderly and the main indicators of physical and mental health, including cognitive ability, mental health, and health behavior, are significantly positively correlated. 41
The measure of mental health is the degree of depression of the respondent, which is calculated based on the response of the simplified self-rating depression scale (CES-D10). The CES-D10 scale has high reliability and validity. 42 Depression is the sum of the 10 questions from the standard depressive scale. The scales for each of the 10 items are adjusted so that the anchors are 0 to 3, rather than 1 to 4. 43 Depression ranges from 0 to 30, indicating that the higher the score, the higher the depression degree, and the worse mental health.44-46
Moreover, we consider the effects of LTCI on health behaviors. CHARLS provides detailed information on a set of health behaviors. This paper chooses the following indicators related to LTCI, including the probability of drinking, daily drinking, and smoking. The probability of drinking refers to whether or not alcohol is currently consumed. The probability of smoking means whether or not currently smoking.
Explanatory Variable
The key explanatory variable LTCI indicates whether the LTCI pilot has been implemented where the individual currently lives. The coefficients measure the average impact of LTCI on the individual healthcare utilization, health outcomes, and health behaviors.
Control Variables
To account for possible confounding factors, we include individual-level characters and city-level characters. Specifically, individual-level covariates consist of an individual’s age and its square, gender, years of schooling, marital status, living in rural areas, number of chronic diseases, and household size. Additionally, this paper uses household consumption per capita as a measure of overall household economic status. 47 Besides, the implementation of LTCI in China is at a pilot stage, and the criteria for rating disability levels are not yet uniform. At present, only a few cities such as Shanghai and Suzhou have developed their assessment criteria, while the majority of the remaining regions determine the level of disability based on the ADL. Therefore, we control the ADL in the following model, expressed as the presence or absence of ADL difficulties. In addition, we further control self-reported health when analyzing the effects of LTCI on healthcare utilization. As for city-level covariates, we control the population size, GDP per capita, public spending per capita, the share of the secondary industry in GDP, and the share of the tertiary industry in GDP. More detailed definitions of variables and summary statistics are displayed in Appendix Table A.1 and Table A.2.
Methods
In this section, we exploit the quasi-experiment of introducing LTCI in China and the difference-in-differences method to examine the health effects of LTCI. Specifically, the treatment group is the 11 pilot cities (Qiqihar, Chengde, Suzhou, Ningbo, Anqing, Jingmen, Guangzhou, Chengdu, Shangrao, Shanghai, and Chongqing) in China. In contrast, the control group is the other cities that have not implemented LTCI. Thus, the treatment effect can be estimated as follows:

Where the dependent variable
Besides, following Huang and Zhang, 48 we draw some city-specific economic indexes over the calendar years to examine whether the trend of dependent variables would be parallel between the LTCI pilot cities and control cities. Specifically, Panel A in Appendix Figure A.1 plots the pattern for GDP per capita. Results show that the time trends over the calendar years are parallel between the LTCI pilot cities and control cities. Also, the F-statistic and corresponding P-values for the economic indexes’ parallel trends indicate that there are no significant nonparallel trends. Moreover, other economic indexes have similar nonparallel trends, including the population size, government spending per capita, the share of the primary industry in GDP, the share of the tertiary industry in GDP, and the number of hospital beds.
Furthermore, this paper uses the event study approach to test the validity of the parallel trend hypothesis with the following equation (2):

Where the LTCI dummy variables, the “D’s,” equal zero, except as follows: D(−j) equals one for the city c (where individual i currently lives) in the jth year before LTCI, while D(+j) equals one for the city c in the jth year after LTCI. Then, we exclude the second year before LTCI as the reference group, thus estimating the effect of LTCI on healthcare utilization, health outcomes, and health behaviors relative to the second year before LTCI. CHARLS conducts the survey every two years. Due to the time limitations of the survey, the actual time periods we used in the regression analysis are –6, –4, –2,1. The

The parallel trend tests of healthcare utilization.
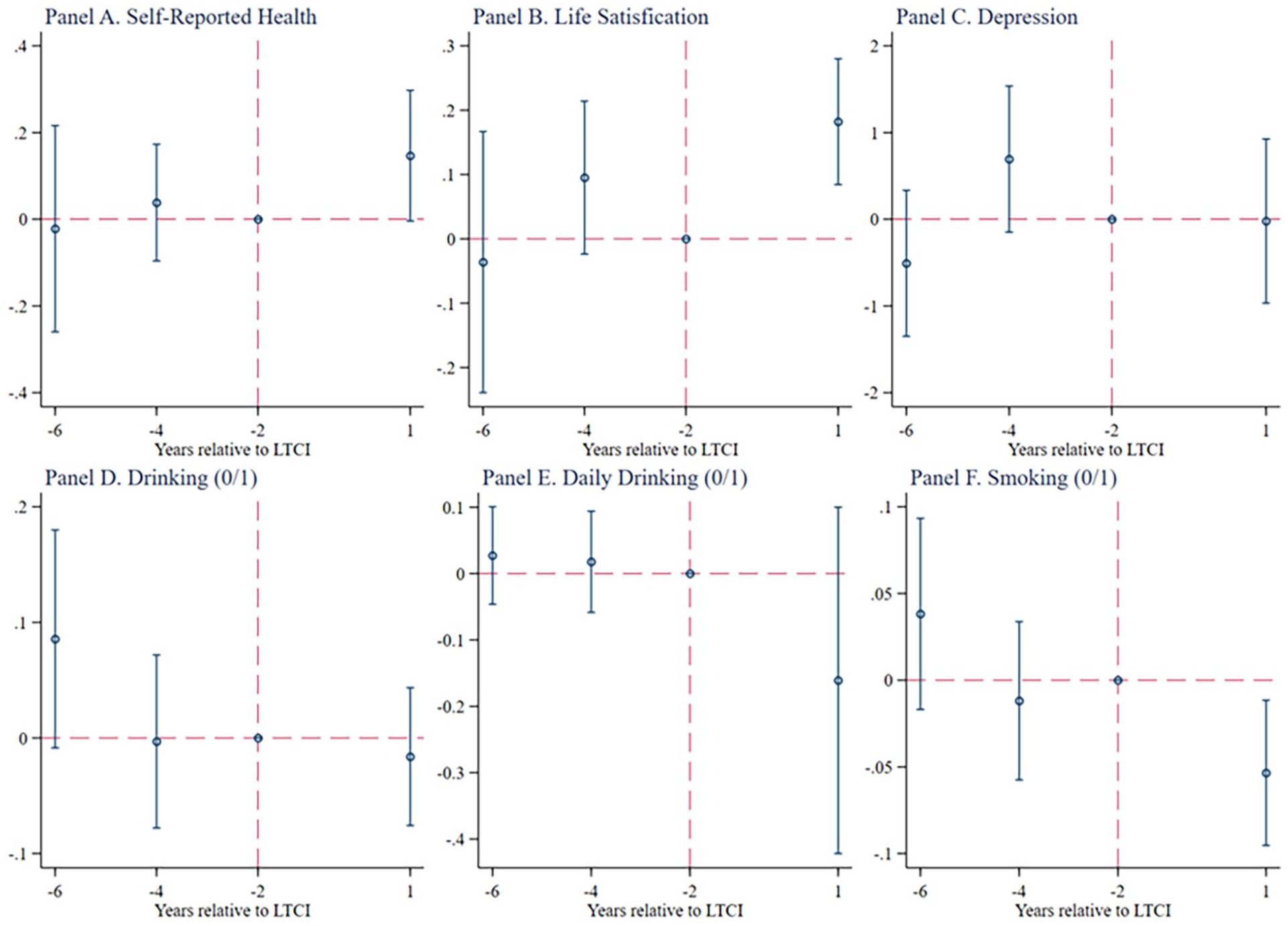
The parallel trend tests of health outcomes and health behaviors.
Results
Baseline Results
Healthcare utilization
In this section, we investigate the impact of LTCI on outpatient and inpatient care utilization. The first 3 columns in Table 1 focus on LTCI’s effects on outpatient care. Our results suggest that LTCI decreases the probability of outpatient visit by 7.1 percentage points, which is significant at the 5% level. Furthermore, LTCI significantly decreases the number of outpatient visits by almost 0.208 times and outpatient expenditure by around 65.8%. These results align with the findings of Ma et al. 49
The effects of LTCI on individual healthcare utilization: outpatient care and inpatient care.

Note. (1) Individual-level covariates include age and its square, gender, years of schooling, marital status, living in rural areas, number of chronic diseases, self-reported health, ADL difficulty, household size, and household consumption per capita; City-level characteristics include population size, GDP per capita, public spending per capita, the share of the secondary industry in GDP, and the share of the tertiary industry in GDP. (2) Year fixed effects and individual fixed effects are controlled. (3) Standard errors clustered at the city level are reported in parentheses.
Outpatient (0/1) = outpatient visit (0/1); Outpatient (#) = number of outpatient visit; Inpatient (0/1) = inpatient admission (0/1); Inpatient (#) = number of inpatient admissions; LOS = length of stay.
P < 1%. **P < 5%. *P < 10%.
The subsequent four columns in Table 1 explore LTCI’s influence on inpatient care. Our analysis reveals no significant impact on inpatient care utilization. This contrasts with Feng et al 1 which demonstrates that LTCI significantly reduces the LOS, inpatient expenditures, and health insurance expenditures in tertiary hospitals by 41.0%, 17.7%, and 11.4%, respectively. The discrepancy may stem from differences in sample demographics. Feng et al 1 focused on individuals over 60 years old covered by Urban Employees Basic Medical Insurance (UEBMI) and Urban and Rural Residents Basic Medical Insurance (URRBMI), while our study includes only individuals over 50 years old covered by UEBMI.
Health outcomes and health behaviors
In Table 2, we investigate the impact of LTCI on health outcomes and health behaviors. The columns 1 and 2 show that LTCI significantly increases the self-reported health by 0.14 scores and life satisfaction by 0.163 scores. In column 3, LTCI reduces depression by 0.117 scores, although the coefficient is statistically insignificant. In addition, we use 10 and above as a cutoff point for high depressive symptoms.42,46,50 The results, as shown in Appendix Table A.3, show that LTCI reduces the risk of high depression but is not statistically significant, which is consistent with the results in column 3. Furthermore, LTCI leads to a non-significant decrease in the probability of drinking and daily drinking by 3.2 and 17.1 percentage points, respectively, in columns 4 and 5. In column 6, LTCI significantly reduces the probability of smoking by 4.4 percentage points. The above results validate Hypothesis 1, that LTCI improves health outcomes and health behaviors.
The effects of LTCI on individual health outcomes and health behaviors.

Note. (1) Individual-level covariates include age, age square, gender, years of schooling, marital status, living in rural areas, number of chronic diseases, ADL difficulty, household size, and household consumption per capita; City-level characteristics include population size, GDP per capita, public spending per capita, the share of the secondary industry in GDP, and the share of the tertiary industry in GDP. (2) Year fixed effects and individual fixed effects are controlled. (3) Standard errors clustered at the city level are reported in parentheses. (4) *** P < 1%. **P < 5%. *P < 10%.
Parallel Trend Tests
Next, this paper uses the event study method to examine the parallel trend assumption of LTCI on healthcare utilization, health outcomes, and health behaviors. Specifically, Figure 1 reports the results of parallel trend tests for healthcare utilization. As shown in Figure 1, the coefficients of LTCI dummy variables are insignificantly different from zero for all years before implementing LTCI, with no trends in healthcare utilization before LTCI. Moreover, note that the probability of outpatient visits, number of outpatient visits, and outpatient expenditure fall immediately in the first year after LTCI.
In addition, Figure 2 reports the results of parallel trend tests for health outcomes and health behaviors. Results show that all the coefficients of
Overall, the parallel trend hypothesis holds in estimating the effects of LTCI on healthcare utilization, health outcomes, and health behaviors.
Robustness Checks
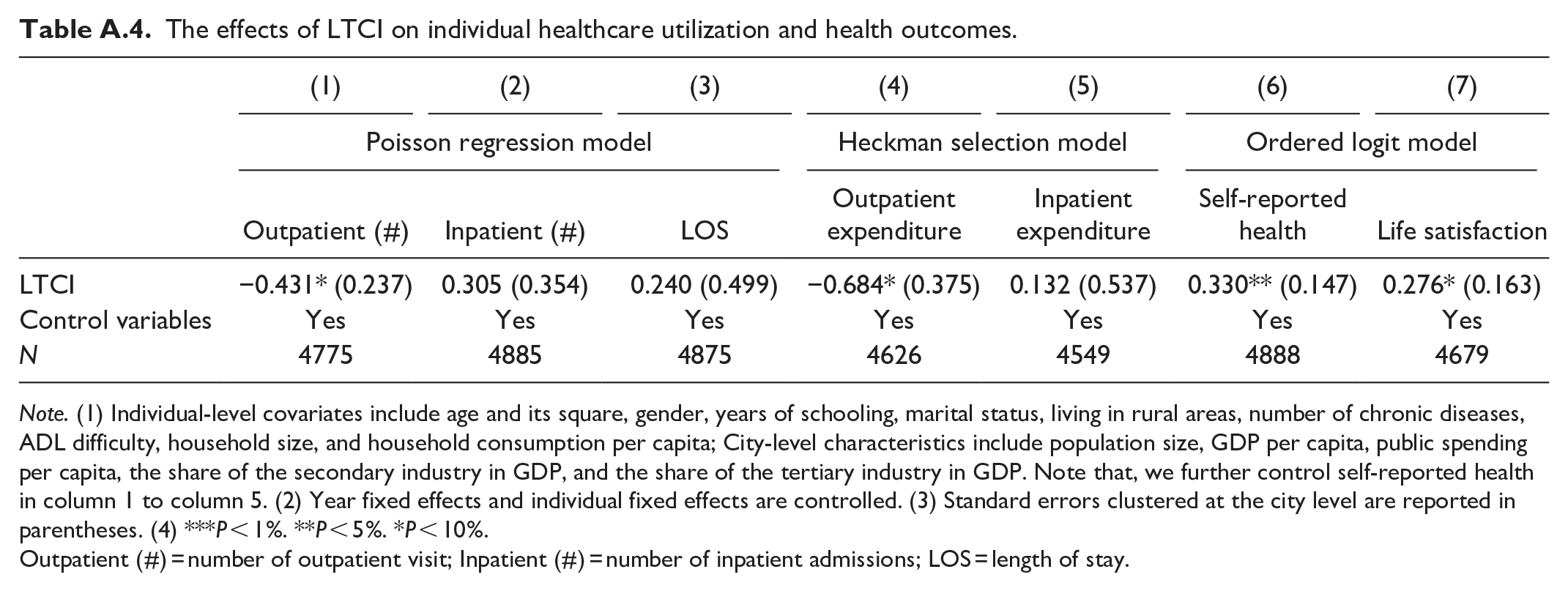
According to the distribution of the dependent variables, we use the Poisson regression model, Heckman selection model, and Ordered logit model for robustness checks. Specifically, the number of outpatient visits, number of inpatient admissions, and LOS are count data that take values of non-negative integers. In this regard, we adopt the Poisson Regression Model for estimation. The results are shown in columns 1 to 3 of Appendix Table A.4, where LTCI significantly reduces the number of outpatient visits and has no significant effect on the number of inpatient admissions and LOS, similar to the results in columns 2, 5, and 6 of Table 1.
In addition, when respondents do not receive outpatient or inpatient care, the outpatient and inpatient expenditures are zero. In this way, there may be self-selection of the sample and subsequent selection bias. To correct for potential selection bias, we use the Heckman selection model to re-estimate. As shown in columns 4 to 5 of Appendix Table A.4, the results show that LTCI significantly decreases outpatient expenditure and has no significant effect on inpatient expenditure, which is consistent with the results in columns 3 and 7 of Table 1.
Moreover, self-reported health and life satisfaction are ranked data that take values from 1 to 5. Considering the distribution of the ranked data, we use the Ordered Logit Model for re-estimation. As shown in columns 6 and 7 of Appendix Table A.4, LTCI significantly increases self-reported health and life satisfaction, which is similar to the results in columns 1 and 2 of Table 2.
Heterogeneous Analysis
In this section, we conduct the heterogeneous analysis from 2 perspectives: heterogeneity of individual characteristics and LTCI policy designs. The sample is segmented by gender, age (above or below the median), household consumption per capita, number of chronic diseases, eligible group, and reimbursement ceiling. Detailed results are presented in Appendix Figure A.2, Panels A to F.
More specifically, Panel A shows that compared with males, LTCI significantly decreases outpatient care utilization for females, including a lower number of outpatient visits and outpatient expenditure. Besides, after LTCI, the female has better health behaviors than the male. This is indicated by a lower probability of drinking. Panel B indicates that after LTCI, the people younger than 62 years have higher inpatient care utilization, while those older than 62 years have higher self-reported health. Panel C presents that LTCI significantly decreases the outpatient care utilization and the probability of daily drinking for people below consumption of 15189.63 Chinese Yuan. Similarly, Panel D illustrates that for people with more than 2 chronic diseases, LTCI significantly reduces outpatient care utilization, including a lower probability of outpatient visit, number of outpatient visits, and outpatient expenditure. Also, people with more than 2 chronic diseases have higher life satisfaction and better health behaviors, including a lower probability of daily drinking and smoking. Panel E shows that LTCI in pilot cities covering both severely and moderately disabled individuals decreases outpatient care utilization, increases life satisfaction, and reduces the probability of daily drinking. Conversely, pilot cities covering only severely disabled individuals see an increase in inpatient expenditure and the probability of daily drinking after LTCI. Panel F demonstrates that compared to cities with low coverage, LTCI in cities with high coverage reduces outpatient care utilization, improves self-reported health and life satisfaction, and decreases the probability of daily drinking.
The results depicted in Appendix Figure A.2 indicate a more pronounced reduction in outpatient care utilization and a more significant improvement in health behaviors among individuals with more than 2 chronic diseases, females aged over 62 years, household consumption per capita below the median, and those with higher reimbursement ceilings eligible for both moderate and severe disabled. These findings confirm hypothesis 2, suggesting that the effect of LTCI in China vary across different demographic characteristics and policy designs.
Discussion
The findings above show that the LTCI significantly decreases the probability of outpatient visit by 7.1 percentage points, reduces the number of outpatient visits by 0.208 times, and lowers the outpatient expenditure by 65.8%, while inpatient care utilization has no discernible change. Similarly, Chen and Ning 51 find that LTCI in China significantly reduces the number of outpatient visits by 0.322 times. Ma et al 49 find that LTCI significantly decreases outpatient visits by 0.14 times per month.
Moreover, LTCI significantly improves self-reported health and life satisfaction. Also, LTCI results in a healthier lifestyle, including a significant decline in the probability of smoking by 4.4 percentage points and a modest decrease in the probability of drinking and daily drinking, supporting Hypothesis 1. Previous studies also support these findings.1,17,30 Lei et al 17 find that LTCI significantly increases the likelihood of self-reported good health by 29%. Similarly, Stabile et al 30 find that publicly financed home care in Canada has a significant increase in self-reported health.
Additionally, our study further investigates the heterogeneous effects of LTCI by individual characters and policy designs. Results show that LTCI has more benefits for individuals with more than 2 chronic diseases, lower household consumption, females older than 62 years, and those with higher reimbursement ceilings eligible for both moderate and severe disabled in terms of healthcare utilization, health outcomes, and health behaviors, supporting Hypothesis 2. These results are consistent with Lei et al. 17
We recognize this study has several limitations. First, due to the absence of CHARLS data for 2011, 2013, 2015, and 2018 on issues related to the implementation of LTCI, we are unable to identify beneficiaries who have access to LTCI accurately. Thus, the estimation results in this paper belong to intent-to-treat effects. Previous studies suggest that public programs can indirectly affect the ineligible group in the same region.17,48,52 Therefore, the true effects of LTCI may be underestimated. Also, we lack information on individuals who applied for LTCI but did not receive the benefits. If we had information on this group, we would compare the outcomes of participants who are entitled to LTCI (the treatment group) with those who have applied but do not meet the criteria. In this regard, we identify respondents based on whether or not they lived in a city that had implemented a pilot LTCI. Second, due to the data limitation, we are not able to examine the long-term impact of LTCI.
Conclusion
The aging population and increased life expectancy in China pose significant challenges in meeting the long-term care needs of the elderly. To address this, the Chinese government initiated long-term care insurance (LTCI) pilots since 2012. This study utilizes quasi-experimental data from the LTCI pilots to demonstrate that LTCI substantially reduces outpatient care utilization, improves self-reported health and life satisfaction, and decreases smoking rates. These health benefits are most notable in individuals with multiple chronic conditions, lower household consumption, females above 62 years old, and those enrolled in more comprehensive LTCI programs.
Our research has significant policy implications, emphasizing the necessity of enhancing LTCI in China and other developing countries. Policymakers are encouraged to expand LTCI pilot programs, establish a sustainable and skilled workforce, provide high-quality LTC services, and cultivate an elder-friendly environment. Additionally, it is crucial to extend LTCI coverage to all beneficiaries of basic public medical insurance to address the urban-rural healthcare gap and promote social equity.
Footnotes
Appendix
The effects of LTCI on individual healthcare utilization and health outcomes.
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | |
|---|---|---|---|---|---|---|---|
| Poisson regression model | Heckman selection model | Ordered logit model | |||||
| Outpatient (#) | Inpatient (#) | LOS | Outpatient expenditure | Inpatient expenditure | Self-reported health | Life satisfaction | |
| LTCI | −0.431* (0.237) | 0.305 (0.354) | 0.240 (0.499) | −0.684* (0.375) | 0.132 (0.537) | 0.330** (0.147) | 0.276* (0.163) |
| Control variables | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| N | 4775 | 4885 | 4875 | 4626 | 4549 | 4888 | 4679 |
Note. (1) Individual-level covariates include age and its square, gender, years of schooling, marital status, living in rural areas, number of chronic diseases, ADL difficulty, household size, and household consumption per capita; City-level characteristics include population size, GDP per capita, public spending per capita, the share of the secondary industry in GDP, and the share of the tertiary industry in GDP. Note that, we further control self-reported health in column 1 to column 5. (2) Year fixed effects and individual fixed effects are controlled. (3) Standard errors clustered at the city level are reported in parentheses. (4) *** P < 1%. **P < 5%. *P < 10%.
Outpatient (#) = number of outpatient visit; Inpatient (#) = number of inpatient admissions; LOS = length of stay.
Contribution List
QH: Methodology, Formal analysis, Original draft, Software, Reviewing & Editing. SW: Formal analysis, Original draft, Reviewing & Editing. LC: Visualization, Reviewing & Editing. YZ: Conceptualization, Supervision, Resources, Reviewing & Editing. All authors have read and approved the final manuscript.
Data Availability Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chinese Academy of Social Sciences (Grant No. 2025QNZX021).
Ethical Statement
The CHARLS data used in this study were approved by the Biomedical Ethics Committee of Peking University, approval number: IRB00001052-11015.