
Abstract
Growing long-term care (LTC) needs represent a major challenge for our aging societies. Understanding how utilization patterns of different types of care are influenced by LTC policies or changes in the population composition such as age patterns or health can provide helpful insight on how to adequately prepare for this situation. To this aim, this paper explores how individuals choose between different forms of LTC. We exploit variation between countries as well as between individuals within countries using data from the Survey of Health, Ageing, and Retirement in Europe (SHARE). Using nonlinear decomposition techniques, we break down the difference in utilization rates between countries into differences based on observed sociodemographic and need-related characteristics and differences in the impacts of these characteristics, which allows us to identify the drivers behind differences in the formal-informal care mix. Our results show that a substantial fraction of the observed country differences can be explained by differences in impacts. We argue that this is a result of the different incentives provided by the different LTC systems.
Keywords
The choice between formal and informal long-term care services is primarily influenced by age, impairments, cultural norms with respect to informal care, and the availability of family carers and nursing home beds.
We compare different long-term care systems in Europe to assess whether sociodemographic and need-related characteristics impact individuals’ care choices differently in different institutional settings.
By setting different incentives for formal and informal care, long-term care systems can influence the mix between formal and informal care use as well as the absolute share of either form of care use.
Introduction
By 2050, the share of the population aged 80 and older is expected to double across OECD countries. 1 In line with this general trend, social demand for long-term care (LTC) is expected to grow considerably. Meeting the increasing demand by supplying and financing adequate LTC services poses a serious challenge to aging societies and LTC systems. Today, average public and private spending on LTC accounts for as much as 1.5% of gross domestic product (GDP) across OECD countries. This share is projected to double or even triple by 2050. 1 To prepare for this development, it is crucial to understand the determinants of LTC. Although cross-country differences in LTC use are well documented,1,2 the underlying reasons are not fully understood. Better knowledge of these determinants allows the prediction of future costs and shortages in the supply of formal and/or informal care. The existing literature on the determinants of LTC use finds that, eg, age, impairments, cultural norms with respect to informal care, or the availability of family carer and nursing home beds are important to explain the demand for specific LTC services.3-8 Hence, a different distribution of these socioeconomic characteristics and of country-specific preferences is likely to result in diverging LTC use between countries. Besides, the available mix of different LTC options may influence a person’s LTC choice because different forms of LTC are associated with different costs. While some countries with strong public institutions have put a strong emphasis on the support of formal care, many other countries prioritize family care instead, which is often seen as the least expensive form of care at least from a budgetary point of view. As a result, both the absolute amount of care use and the distribution between formal and informal LTC differ substantially between countries. In a study which highlights the importance of such institutional differences, de Meijer et al 9 find that recent trends in the choice of different forms of LTC in the Netherlands can almost entirely be explained by changes in the Dutch LTC system. Similarly, Bakx et al 10 and Alders et al 11 show that system characteristics result in a different mix of formal and informal care in Germany and the Netherlands. For policy makers, it is therefore of special importance to understand the role of institutional designs such as the LTC insurance (LTCI) system on different types of LTC, especially because in terms of welfare cost, the cost of informal care and nursing home care can be similar. 12
A related strand of the literature estimates the effects of LTC policy changes on care utilization. For example, Hoerger et al 13 find that increased Medicaid subsidies in the United States make disabled parents more likely to live independently than with their children, Karlsberg Schaffer 14 finds that the introduction of free personal care in Scotland led to an increased supply of informal care, and Løken et al 15 find a significant negative impact of a formal care expansion on the work absences of informal carers in Norway. They interpret their results as evidence on the substitution between formal and informal care at home. Likewise, Bonsang 16 and Bolin et al 17 provide evidence that informal and formal care are substitutes rather than complements analyzing several European countries, which is an important condition for policy reforms aiming to strengthen 1 of the 2 options to be effective. Besides, the finding that informal and formal care are substitutes rather than complements has important implications for informal carers. When formal care options exist, informal caregiving becomes a choice rather than an obligation, but when no formal care options exist, the pressure to provide informal care increases. Hence, the availability of formal care option allows for specialization effects, while caregiving out of necessity might lead to potential negative consequences for carers’ health.18-21
Understanding the extent to which observed cross-country differences in LTC use are based on need versus institutional differences or preferences is the aim of this paper. We extend the analysis of Bakx et al 10 and analyze the determinants of the LTC choice in 4 European countries. Each country represents a different LTC setting, which provides us with a comprehensive picture of the incentives put in place by the different LTC systems. Our estimation strategy exploits the variation between countries and between individuals within countries to disentangle the determinants of LTC use analyzing data from the Survey of Health, Ageing, and Retirement in Europe (SHARE).22,23 Using novel nonlinear decomposition techniques, we break down the difference in utilization rates between countries into differences based on observed socioeconomic, demographic, and need-related characteristics and differences in the impacts of these characteristics. This allows us to identify the drivers behind differences in the formal-informal care mix. We focus on individuals aged 65 and older to capture those with a high probability of LTC needs and concentrate on 4 countries within the European Union, which are chosen as representatives of different philosophies in the organization of LTC. Most importantly, LTC systems differ with regard to the availability of services and generosity. Moreover, systems can set different priorities for informal or formal care options, which are arguably a reflection of the cultural norms in the country’s population (see, for example, Kraus et al 24 for a typology of European care systems). We focus on countries with a strong informal or ambulatory care sector because (1) most existing incentives put in place aim to promote these types of care and (2) information on nursing home care is limited in our data. We choose Germany as an example of a mixed system with both formal and informal care support but a relatively strong cultural preference for informal care. France is similar to Germany but has more generous eligibility rules, puts a stronger emphasis on formal care at home, and cultural norms in favor of informal care are weaker. Spain is chosen as a Southern European economy with traditionally strong family ties and consequently a large share of informal care, but a recently growing formal care sector. Finally, the Czech Republic is an Eastern European country with relatively low LTC benefits, a fragmented care delivery system, and a very strong norm for informal care.
Our results show that although differences in health outcomes and demographics explain some of the observed country differences in LTC use, a substantial fraction remains unexplained and is likely caused by different societal values and different features of the LTC systems. These results, hence, provide highly relevant information for policy makers aiming to reduce or promote certain care options by highlighting the relative contribution of population characteristics and system characteristics on the choice of LTC options.
The remainder of the paper is organized as follows: We briefly describe the institutional settings in Germany, Spain, France, and the Czech Republic in the “Institutional Settings” section; in the “Methods” section, we present our empirical strategy; in the “Data” section, we describe the SHARE data set and provide a descriptive analysis of differences in LTC use; in the “Results” section, we present our estimation results; the “Conclusion and Discussion” section concludes.
Institutional Settings
Although elderly care has traditionally been the responsibility of the family, the reliance on family care has become more difficult with increasing female labor supply, fewer children, and, in general, smaller family sizes. 25 As a result, countries in Europe have developed different strategies to ensure a sufficient supply of LTC. While some countries still rely heavily on informal carers and public spending for LTC is low, others have put an emphasis on the support of formal care to reduce the burden for family members, resulting in a North-South gradient (see, for example, Börsch-Supan et al, 26 Haberkern and Szydlik, 27 Kraus et al, 24 and Rodrigues et al 28 for further information). The Scandinavian countries as well as the Netherland and Switzerland have relatively generous LTC systems and formal care options are widely available. 27 Informal caregiving is, hence, rather a choice than an obligation. Contrary, public spending and, hence, the availability of formal care options are much lower in Southern and Eastern European countries. Countries that lay in the middle regionally, such as Belgium or France, also are intermediate cases with respect to their LTC systems. While LTCI in these countries does not offer the same level of support as in Scandinavian countries, formal care plays a larger role than in Southern or Eastern Europe. 27 For a more detailed look at the countries in our study, Table 1 provides an overview of their LTCI systems, cultural norms regarding family care, and LTC resources. One notable difference lies in support options for family carers. Flexible work arrangements or leave regulations make it easier for informal carers to combine work and care and thus are likely to increase family care. 12 Similarly, any form of monetary transfer that supports family care is likely to increase informal care use. 29 With respect to formal care, all countries in our study offer nursing home support as well as benefits in cash and in kind for care at home. Hence, each country offers incentives for both informal and formal care use at home or in nursing homes. However, eligibility rules and the generosity of the systems differ.30,31 In the following, we briefly describe the relevant aspects of the LTCI system of each country, putting a special focus on incentives set for informal and formal care. Because the market for private LTCI is relatively small in all countries,32,33 we concentrate primarily on the public LTC settings.
Comparison of LTCI systems (in 2013).
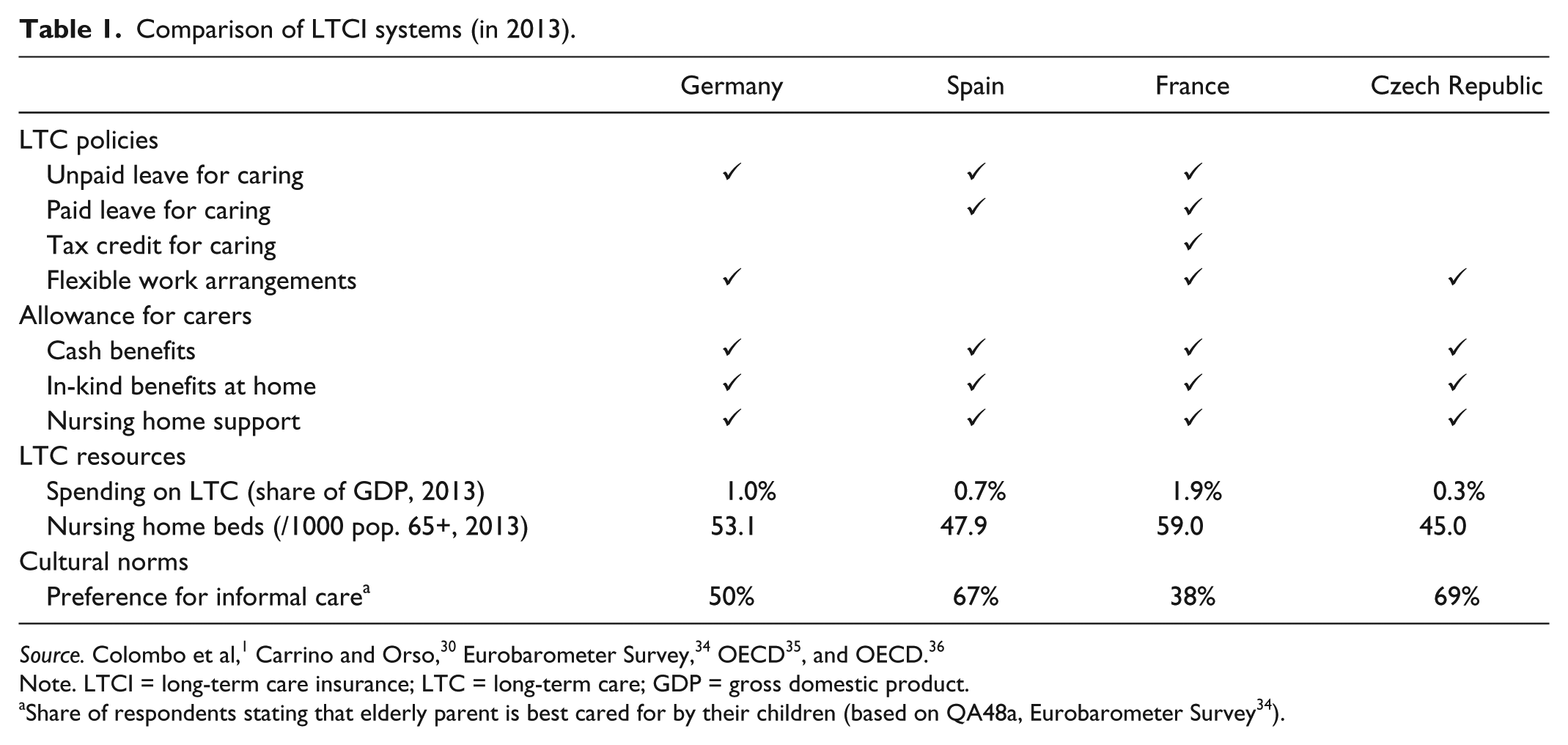
Note. LTCI = long-term care insurance; LTC = long-term care; GDP = gross domestic product.
Share of respondents stating that elderly parent is best cared for by their children (based on QA48a, Eurobarometer Survey 34 ).
Germany
Germany introduced mandatory LTCI in 1995. The LTCI aims to support and strengthen family care; hence, informal care is given precedence over formal care at home, and home care takes precedence over inpatient care. 37 This preference for informal care is also strongly mirrored by the public opinion. The insurance system provides benefits without regard to age or financial status to individuals with permanent (at least 6 months) impairments in at least 2 activities of daily living (ADL) and 1 instrumental activity of daily living (IADL), with mental disabilities being largely disregarded until recently. i Depending on the level of impairments, 3 care levels are distinguished, which are assessed by the German Health Insurance Medical Service (MDK). If a care level is established, LTCI for care at home covers informal care, which is generally provided by family members, or formal care provided by professional health care services. Informal care benefits are given as cash transfer whereas formal care is organized as an in-kind transfer. In 2015, monthly benefits in cash for informal care ranged from 244 euro (in care-level I) up to 728 euro (in care-level III). Cash benefits can also be used to reimburse informal carers. These benefits are not means-tested or earmarked, and their spending is not monitored. Benefits in kind for formal care are more generous. They range from 468 euro per month up to 1612 euro and are directly paid to an ambulatory care service. However, the benefits do not fully cover the costs of LTC; they are designed to support and complement family care but not to replace it.
For nursing home care, the LTCI pays the nursing home a fixed monthly payment ranging from 1064 euro in care-level I up to 1612 euro in care-level III. However, copayments for institutional care are high and the costs for accommodation have to be paid by the resident. Schulz 41 estimates that the LTCI covers only about 50% of the total cost of the nursing home; the difference has to be financed by the care recipient, social insurance, or close family members. Due to the high copayments and the preference of most elderly to remain in their own home, nursing home entry is often seen as a last resort. 11 Hence, while the German LTC system is a mixed system that provides benefits for informal and formal care, the high copayments, the unmonitored cash transfers, and cultural norms set strong incentives for informal care.
France
In France, dependency for LTC services is determined by the AGGIR (Autonomie Gérontologique Groupes Iso-Ressources) scale, which is based on the degree of difficulty when performing ADLs, eg, eating, dressing, or bathing. Based on this score, 6 iso-groups (GIR) of need are classified. They range from GIR1 (very dependent) to GIR6 (not dependent). Individuals who are aged 60 or older and are classified GIR1 to GIR4 are entitled to receive the main French LTC allowance, the Personalized Allowance for Autonomy (APA), created in 2001. ii Those who have mental limitations are assigned to GIR1 or GIR2; being classified into GIR4 or higher requires difficulties with at least 2 ADLs. 30 The APA is an earmarked in-kind benefit that can be used for LTC at home or for residential care. It is not means-tested but depends on the level of impairment as well as on individual income. For individuals with monthly disposable income more than 739 euro (in 2014), the amount of the benefit decreases progressively from 100% to 10% of the maximum amount. In 2014, the maximum APA amount ranged from 563 euro per month in GIR4 to 1313 euro in GIR1. 30 Usually, the benefit is paid directly to a formal care provider; it can only be paid to the care recipient if he or she provides proof of the correct use of the benefit. However, the benefit can also be used to pay a member of the family except husband or wife if he or she provides the required assistance.
If individuals live in a nursing home, they have to finance a large fraction of the care costs themselves. With estimated nursing home fees ranging from about 1300 euro to 2000 euro per month and average APA-benefits for a person in a nursing home at about 410 euro per month, over two thirds of the expenditures have to be paid for by the person in need of care or their relatives. 44 Although families play a nonnegligible role in financing and assisting LTC in France, public opinion primarily sees the state responsible for LTC provision. 44 While private contributions are similar to Germany, formal care is more accepted in France. In addition, mental limitations also qualify for benefits. We therefore expect the preference for formal care to be stronger than in Germany.
Spain
Traditionally, the provision of LTC in Spain has been a family responsibility. However, to respond to increasing female labor supply and changing family structures, the Spanish government passed an act to increase and harmonize the state’s support for LTC in 2006.45,46 Under the newly introduced System for Autonomy and the Care of Dependency (SAAD), the Spanish law distinguishes between 3 degrees of dependency (moderate, severe, and major dependency). The 3 degrees are assessed by a scoring system that takes into account a list of 11 daily activities such as eating, washing, or dressing. Individuals receive a score for each activity they need assistance with, which is further weighted by the degree of supervision required to perform the activity. 30 Moreover, within each of the 3 degrees, the system distinguishes between 2 levels depending on the person’s autonomy and on the intensity of required care. While the first level corresponds to individuals who are able to perform the activities without direct support of a third person, the second level is for individuals who need additional support. 30
Once a person is eligible for benefits, the state provides in-kind benefits consisting of, eg, home help services, personal care, day care centers, or residential care services (for a detailed list of available services, see Gutiérrez et al 45 ). Only if the in-kind benefits are not available in the community, means-tested cash benefits can be granted. In 2010, they ranged from 300 up to 833 euro per month when linked to a professional care provider and from 180 up to 520 euro per month when used for informal care within the family. 30 Even though the system prioritizes in-kind services, the necessary infrastructure is not available in many communities yet. Consequently, about 45% of the benefits are still granted in cash and informal family care is still an important pillar of the Spanish LTC mix. 45 We therefore expect the incentives for informal family care to dominate, also because cultural norms strongly favor informal care.
Czech Republic
The LTC assistance in the Czech Republic is fragmented. Instead of having a single body, responsibilities for LTC benefits are divided between the health care and social service sector. The Ministry of Health is responsible for home health care and care provided in health institutions; the Ministry of Labor and Social Affairs is responsible for other forms of home care and offers cash benefits. 47
Eligibility for cash benefits, which were introduced with the 2006 Social Service Act (Social Services Act No. 108/2006), depends on individual impairments. A list of 10 activities relating to the ADL concept is used to assess 4 dependency levels. They range from light dependency (level 1) if a person needs help in at least 3 activities up to very heavy dependency (level 4) if help in at least 9 activities is required. 30 However, the assessment of need can vary by the assessing doctor or social worker as no clear definition exists. In 2014, monthly cash allowances ranged from 29 euro in level 1 up to 438 euro in level 4 which corresponds to about 3% up to 30% in relation to average disposable income.30,48,iii The allowance is not means-tested and is designated to help pay for the provision of needed home care rather than to provide a full reimbursement of the costs. It can also be used to pay for family care or care given by other informal carers.
While informal care supported by cash benefits is the main pillar of the Czech LTC system, support for formal care is also provided. The social service sector offers support for institutional full-time elderly homes but, in general, the number of beds in nursing homes is too low to meet demand. In 2003, more than half of all applications for retirement homes had to be rejected due to insufficient capacities.47,iv Because both benefits and the number of available nursing home beds are low, we expect the incentives for informal family care to dominate, again also mirroring cultural norms.
Methods
The 4 LTC systems described above set different incentives for formal and informal care. Besides, the countries differ in other aspects such as, eg, their demographic structure and average health status. The aim of the following analysis is to determine to what extent system and population characteristics can explain differences in patterns of LTC use across countries. v Our empirical strategy follows a 2-stage approach. First, we estimate multinomial logit models to explain care use in each country separately. The considered care choices are no care, only informal care, and formal care (alone or in addition to informal care). Second, we use nonlinear decomposition techniques to break down the differences in LTC utilization, which can be interpreted similarly to linear Blinder-Oaxaca decomposition results.50,51
In general, the multinomial logit results provide a first impression of how coefficients differ between countries. However, because differences in care use result not only from differences in coefficients but also from different distributions of the independent variables, we use a novel extension of the Blinder-Oaxaca decomposition method for nonlinear models proposed by Yun. 52 Analogue to the linear Blinder-Oaxaca decomposition, the decomposition uses an auxiliary equation based on the characteristics of a base country and the estimated coefficients of the other countries. Under the assumptions that LTC use is determined by the same functional form in all countries under study and overlapping support, the decomposition breaks down the difference in utilization rates between countries into differences based on observed characteristics (endowment effect) and differences in the impacts of these characteristics (coefficient effect). 53
For nonlinear models, Yun 52 proposes to calculate the decomposition at first moments. As it is not possible to calculate conditional expectations in multinomial models, 54 we follow Bakx et al 10 and treat the choice probabilities estimated in the multinomial logit model as binary choices. That is, we decompose the probability for each care choice separately, which provides us with decomposition results for informal and formal care separately. We use the estimated choice probabilities from the multinomial logit to calculate differences in country means as follows:
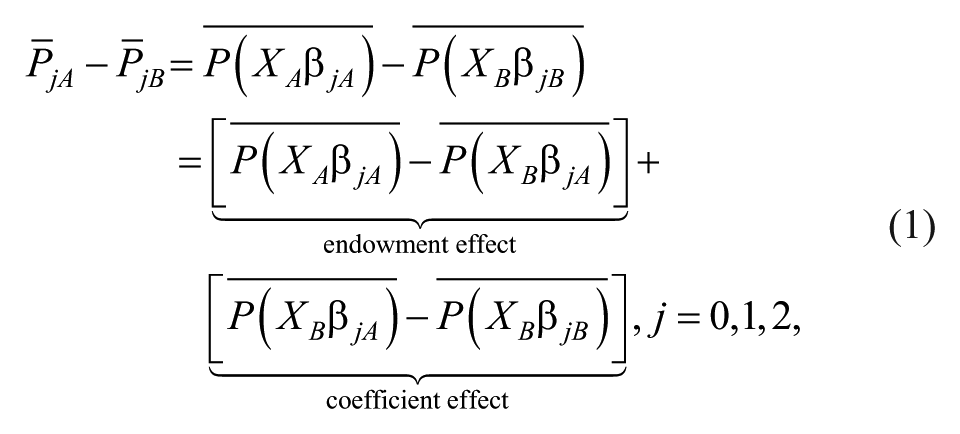
where
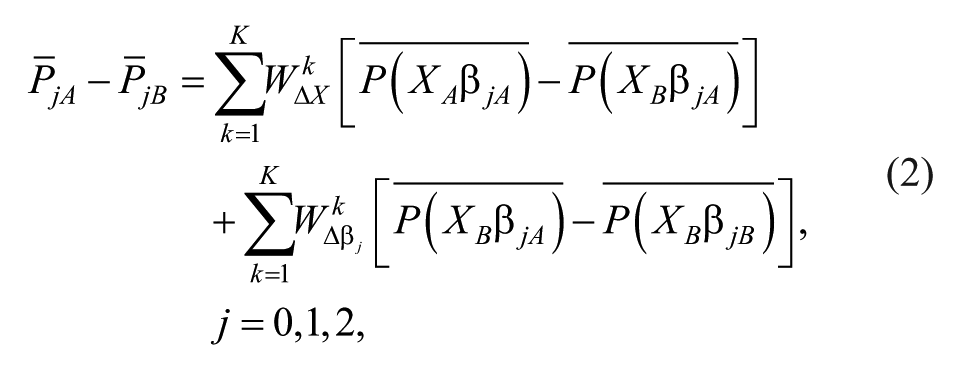
where K denotes the number of independent variables. Note that as long as


where, per definition,
A widely known problem with detailed decomposition techniques is the separation of the intercept from coefficients of sets of dummy variables. Usually, in a regression framework, identification can be achieved by restricting one of the coefficients of the dummy variables to zero (the reference group). However, Oaxaca and Ransom 56 showed that the detailed decomposition might not be invariant to the choice of the reference group. We therefore follow Yun 57 and normalize the contribution of differences in coefficients of dummy variables. vi
Data
We use data from the fifth wave of the SHARE collected in 2013, which targets persons 50+ years of age (or spouses/partners of a person 50+ years of age), who do not live either abroad or in institutions such as prisons and hospitals during the entire fieldwork period and speak (one of) the official language(s) of the country.58,59 Individuals living in institution for the elderly are included in the target population but may be underrepresented due to sampling difficulties. The SHARE is the first data set to include information on health, socioeconomic status (SES), and the demographic situation of the elderly at a pan-European level, which provides the unique opportunity to study the effect of institutional differences. Data are collected using a computer-assisted personal interviewing technique (CAPI). Sample selection varies across countries from simple random selection of households to multistage designs due to varying institutional conditions regarding sampling. 60 We limit the sample to individuals aged 65 or older as LTC needs increase steeply with age and, hence, the need for LTC is higher for older age groups. After further deleting observations with missing information—about 6.5% of the original sample—our sample includes 11511 individuals. vii
Summary statistics are presented in Table 2 separately by country. Informal care is defined as regular help with personal care such as washing, getting out of bed, or dressing by someone living in the same household or from outside the household during the last 12 months. For help received within the same household, only daily or almost daily care during at least 3 months is classified as informal care to exclude short spells of help during a short-term sickness. Formal care includes any professional or paid services a person receives in his or her own home (ambulant formal care) to help with a physical, mental, emotional, or memory problem as well as any overnight stay in a nursing home or residential care facility during the last 12 months. Ambulant formal care comprises help with personal care (eg, getting in and out of bed, dressing, bathing, and showering), domestic tasks (eg, cleaning, ironing, cooking), services such as meals-on-wheels, and other activities such as filling a drug dispenser. Only formal care is relatively rare. Equivalent to Bakx et al, 10 we combine the options formal care and informal care use to have a sufficient number of observations in each country and care option. The definition of informal care is restricted to personal care, as domestic tasks are often shared between household members and do not necessarily represent care activities. If a household receives informal care but the care recipient is not identified because of multiple disabled household members, all observations from this household are dropped. Thereby, we lose about 5% of the original sample. No care use makes up the largest group in all countries. The share ranges from 63% (Czech Republic) to 75% (Germany). In the Czech Republic, the second largest group are individuals who receive informal care only, while in Germany, Spain, and France, this is the smallest group. The SHARE does not provide information about care intensity and all results will therefore be relevant on the extensive margin only.
Descriptive Statistics.
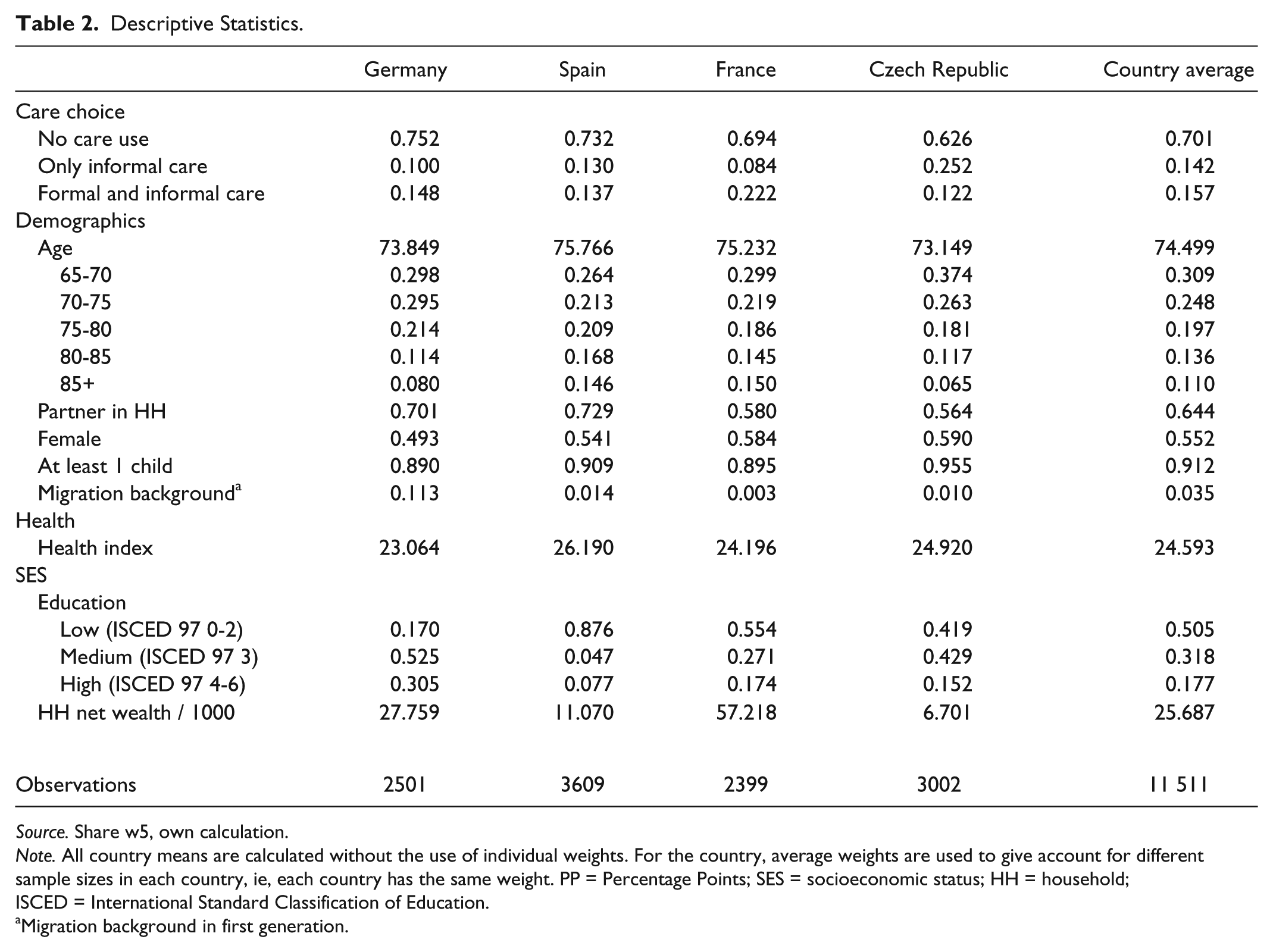
Source. Share w5, own calculation.
Note. All country means are calculated without the use of individual weights. For the country, average weights are used to give account for different sample sizes in each country, ie, each country has the same weight. PP = Percentage Points; SES = socioeconomic status; HH = household; ISCED = International Standard Classification of Education.
Migration background in first generation.
As explanatory variables, we include demographic characteristics such as age, whether the person lives with a partner, and whether he or she has children. Health information is summarized by a health index, which combines information on chronic conditions and health problems diagnosed by a doctor, self-assessed health, depression (measured by the EURO depression scale ranging from 0 [not depressed] to 12 [depressed]), the number of limitations with ADL and with IADL, mobility limitations, cognitive ability, and whether the respondent has had at least 1 hospital stay in the 12 months prior to the interview using principal components analysis. We use the method proposed by Kolenikov and Angeles 62 based on polychoric and polyserial correlations, which is suited for the inclusion of binary and ordinal variables. Results are shown in Table A3 in the appendix. Descriptive statistics of the variables used to construct the index are reported in Table A2 in the appendix. By including both subjective and objective measures of health, the health index provides a measure of multiple aspects of health. Besides, as it includes measures of physical and mental health, it allows for an easy interpretation of the influence of general health on care choice. The index is standardized to range from 0 (the best possible health outcome) to 100 (the worst possible health outcome). On average, elderly individuals in Germany are the healthiest, whereas those in Spain are the sickest. Furthermore, SES is included, which is captured by the education level and household net wealth. Household net wealth has been adjusted for household size by dividing by the square root of the number of household members. In the logit estimation and the decomposition, we use indicators for being above/below the country-specific wealth median. The explanatory variables serve as indicators for the need for care and for the availability of informal care. Moreover, the education level and household wealth provide information about how easily a person can navigate the LTC system and the affordability of copayments for formal care (see, for example, Feinstein, 63 for an overview of the relationship between SES and health).
Results
Results of the first-step multinomial logit regression are largely as expected and in line with previous findings.4,10 A poor health status, ie, a higher health index, increases the probability to receive care. The older the individual, the higher the probability that he or she relies on formal care services. Furthermore, in France and Spain, women have a significantly higher probability of receiving formal care and a lower probability of receiving informal care than men. Detailed results can be found in Table A1 in the appendix.
In the following, the cross-country differences are analyzed further using decomposition methods. In each decomposition, a weighted average of all countries is used as the reference—the group B in equations (1) to (4). Theoretically, any country or country average could serve as the reference category. The reasons we choose an weighted average is that, by definition, it can be classified as an intermediate case concerning eligibility rules and generosity of benefits and can therefore be seen as a benchmark for other European systems that put a strong emphasis on cash benefits, in-kind benefits, or a mixture of the two. To avoid biases due to overrepresentation or underrepresentation of different countries in the comparison group, we calculate probability weights based on the sample size in each country. This ensures that each country contributes the same weight to the country average. The decomposition results are shown in Table 3. For easier interpretation, variables are grouped into demographic, health, and socioeconomic variables and only aggregate endowment and coefficient effects as well as the overall difference in care use of each country relative to the average are shown. Detailed results are shown in the appendix.
Decomposition Results.
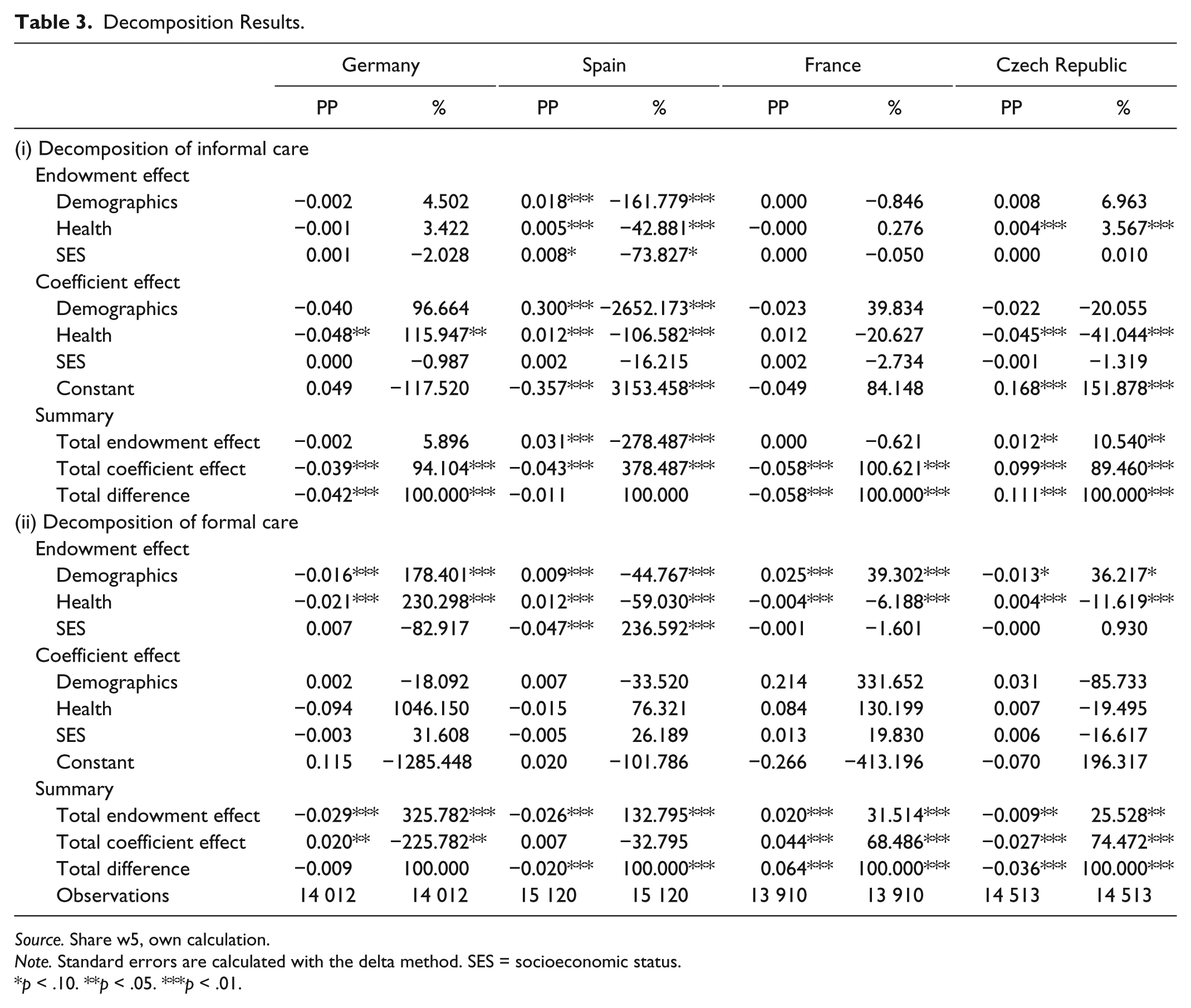
Source. Share w5, own calculation.
Note. Standard errors are calculated with the delta method. SES = socioeconomic status.
p < .10. **p < .05. ***p < .01.
In Germany the use of informal care is lower (–4.2 PP) compared with the country average. Formal care use is almost identical to the average (–0.9 PP and not significant). The difference in informal care is primarily driven by the coefficient of health, indicating that individuals with the same impairments rely on informal help less often than the country average. This is interesting because the LTCI in Germany puts an emphasis on informal care. However, the overall care use is lower as can be seen in the descriptive statistics (Table 2) and, unlike other countries, Germany also supports formal care with in kind benefits.
In Spain, elderly individuals have a 1.1 PP higher probability of receiving informal care but a 2.0 PP lower probability of receiving formal care than the average. Yet, only the latter estimate is statistically significant. Differences in the endowments alone would explain a 3.1 PP higher rate of informal care use in Spain, whereas differences in coefficients would explain a lower rate of informal care (–4.3 PP). The negative coefficient effect is driven by the constant term. Given the same health status or demographic characteristics, Spanish individuals are more likely to receive informal care than the average. With respect to formal care, the endowment and coefficient effects also point in different directions. The worse health status of Spanish elderly and differences in demographic variables alone would result in a higher rate of formal care use in Spain. However, if Spain had the same socioeconomic characteristics as the country average, formal care use would be lower, resulting in an overall negative endowment effect (–2.0 PP). The coefficient effect is positive but small in magnitude (0.7 PP) and statistically insignificant. Although informal care use is above average and formal care use is below average in Spain due to, eg, demographic differences, the direction of the coefficient effect is in line with the fact that ambulatory and inpatient professional care takes precedence over cash benefits in Spain even though they are not yet nationwide available.
The probability of French elderly to use informal care is 5.8 PP lower than the average, which seems to be entirely explained by the coefficient effect (101%). While given the same influence of the health status, French elderly are more likely to receive informal care (1.2 PP); this effect is counteracted by the influence of demographics (–2.3 PP) and by the constant (–4.9 PP), although no single term is statistically significant. In contrast, the probability to use formal care is 6.4 PP above average. While 32% of the difference can be explained by differences in endowments, the remaining 68% are driven by differences in coefficients, indicating a general lower preference for informal care and a stronger preference for formal care in France. While eligibility rules are relatively similar in France, Germany, or Spain, a major difference between the systems is their benefit schemes. Cash benefits are earmarked and monitored in France but not in the other countries. Hence, to use those benefits to pay for formal care at home is more likely in France than in the other countries where benefits can be kept as additional household income. Care must then be compensated by family care instead.
In the Czech Republic, receiving informal care is much more common compared with the country average: The difference in the probability of receiving informal care amounts to 11.1 PP. 89% of this difference can be explained by differences in coefficients, 11% by different endowments. In particular, a worse health status (0.4 PP) and demographic characteristics (0.8 PP) seem to explain the endowment effect, though only the former effect is statistically significant. Contrary to informal care, formal care use is low. Czech elderly are 3.6 PP less likely to receive formal care with differences in coefficients explaining about 74% of this difference. Although statistically insignificant, the constant is driving the coefficient effect, indicating a general low preference for formal care. As public expenditures for LTC in the Czech Republic are low, this result may be caused by barriers to access to formal LTC. It is thus likely that in the Czech Republic, family care often acts as care of last resort: Family members have to support their parent or spouse if public support is not available.
Conclusion and Discussion
In this paper, we compare differences in formal and informal care use in Germany, Spain, France, and the Czech Republic to obtain a comprehensive picture of care use and care choices in different European LTC systems. While all analyzed countries face aging populations and a growing need for LTC, care patterns differ substantially across these countries. We show that these differences might be explained to some extent by differences in population composition, ie, by the fact that some countries have a younger or healthier population. Yet, in some cases, differences in coefficients are responsible for an equal or even larger difference in care use—especially the differences in formal care seem to be driven by different coefficients. We attribute these differences to aspects of the LTC system and societal preferences. However, whether different preferences have led to different institutions or whether institutions themselves remain the driving force is still an open question. Answering this question would require longitudinal data on a macro and micro level to assess changes in individuals’ behavior to institutional changes. As changes in the institutional setting are lengthy processes, we do not separate preferences and institutions. In line with the literature, our study focuses on individual behavior treating the institutional setting as given. Our results complement findings by Bakx et al 10 and Alders et al 11 who show that differences in the German and Dutch LTC system characteristics explain a different mix of formal and informal care in these countries by extending the focus of the analysis to additional countries representing a variety of different types of care systems.
We find that informal family care is most widely used in countries that have either low support for LTC or in countries that have a strong emphasis on cash benefits that can be used as additional household income or to pay informal carers. For example, the Czech Republic, the country with the highest share of informal care in our sample, provides relatively low benefits and informal care supported by cash benefits is the main pillar of the LTC system, whereas other countries also offer in-kind benefits. Differences in informal care use between the country average and the Czech Republic are almost entirely explained by different coefficients and could be explained by different institutions. The more additional benefit schemes supporting formal care are available, the more options individuals have regarding their care decisions. Our results show that more generous in-kind benefits likely increase the demand for professional formal care services. This may explain why, eg, Germany and Spain with their mixed systems have a more similar rate of informal and formal care use compared with the Czech Republic. If, like in France that has the highest use of formal care in the sample, cash benefits are earmarked and can only be used for formal care (and not to reimburse family members), the shift from informal to formal care can be expected to be even higher. However, an increase in formal care use can only occur if such care options are available. Moreover, building up the necessary infrastructure takes time and changes in care use patterns hence happen slowly. This becomes apparent in the comparison between Germany and Spain. While in the German system, cash benefits take precedence over in-kind benefits, in Spain, in-kind benefits are the preferred option. However, Germany introduced its LTCI reform much earlier in 1995; Spain on the contrary started offering comprehensive in-kind benefits only rather recently in 2006. Consequently, in many areas of Spain, the sufficient infrastructure is not yet available and formal care use is thus still lower than in Germany.
As providing LTC services is associated with considerable public spending, understanding the drivers behind care choices is highly relevant for the design of LTC systems. Our results show that by providing different incentives, both the mix between formal and informal care use as well as the absolute share of either form of care use can be influenced. A caveat, however, remains as our results only consider the share of care use for each form or care but not its costs. While formal care is generally considered to be more expensive, this result might no longer hold if all societal costs are considered.12,64 Thus, the design of LTC systems should not only focus on reducing public spending for LTC by lowering formal care use but also aim to reduce societal costs while providing adequate care to individuals with LTC needs.
Footnotes
Acknowledgements
We thank Maryna Ivets and Adam Pilny for useful comments and discussions.
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper uses data from Survey of Health, Ageing, and Retirement in Europe (SHARE) Wave 5 release 5.0.0 (doi:10.6103/SHARE.w5.500), see Börsch-Supan et al
22
for methodological details. The SHARE data collection has been primarily funded by the European Commission through the 5th Framework Programme (project QLK6-CT-2001-00360 in the thematic programme Quality of Life), through the 6th Framework Programme (projects SHARE-I3, RII-CT-2006-062193, COMPARE, CIT5- CT-2005-028857, and SHARELIFE, SHARE-LEAP, 227822 and SHARE M4, 261982). Additional funding from the U.S. National Institute on Aging (U01 AG09740-13S2, P01 AG005842, P01 AG08291, P30 AG12815, R21 AG025169, Y1-AG4553-01, IAG BSR06-11, and OGHA 04-064) and the German Ministry of Education and Research as well as from various national sources is gratefully acknowledged (see ![]() for a full list of funding institutions, data access, and questionnaires). Furthermore, we gratefully acknowledge financial support from the European Investment Bank (EIB) under the EIB-Universities Research Action Programme. Any errors remain those of the authors. The findings, interpretations, and conclusions presented in this article are entirely those of the authors and should not be attributed in any manner to the EIB. Thorben Korfhage also gratefully acknowledges the support of a special grant (Sondertatbestand) from the German Federal Ministry for Economic Affairs and Energy and the Ministry of Innovation, Science, and Research of the State of North Rhine-Westphalia. The publication of this article was funded by the Open Access Fund of the Leibniz Association.
for a full list of funding institutions, data access, and questionnaires). Furthermore, we gratefully acknowledge financial support from the European Investment Bank (EIB) under the EIB-Universities Research Action Programme. Any errors remain those of the authors. The findings, interpretations, and conclusions presented in this article are entirely those of the authors and should not be attributed in any manner to the EIB. Thorben Korfhage also gratefully acknowledges the support of a special grant (Sondertatbestand) from the German Federal Ministry for Economic Affairs and Energy and the Ministry of Innovation, Science, and Research of the State of North Rhine-Westphalia. The publication of this article was funded by the Open Access Fund of the Leibniz Association.