
Abstract
Whether the association between metabolic syndrome (MetS) and functional disability differs depending on sex or age remains unknown. To determine the association between MetS and functional disability in older people separately by sex and age groups. A total of 11 083 participants (4407 men and 6676 women) aged 65 years or over without functional disability were enrolled. MetS was defined according to the revised NCEP ATP III guidelines. Functional disability was defined by a new certification in the long-term care insurance in Japan. Cox proportional hazards models were used to assess the risk of functional disability with adjustment for possible confounding factors. Over the mean observation period of 10.5 years, 1282 men and 2162 women experienced functional disability. For those aged 65 to 74 years, HRs (95% CIs) for functional disability in the MetS group were 1.33 (1.07-1.66) in men and 1.15 (1.000-1.32) in women. For those aged 75 years or older, there was no significant association in men or women. In subjects with a severe care need level, there was a marginal significant association in men aged 65 to 74 years. Among the MetS components that independently increased the risk of functional disability were glucose intolerance and elevated blood pressure (men and women aged 65-74 years), obesity (women aged 65-74 years), and glucose intolerance (women aged 75 years or older). MetS contributed to an increase in a high risk of future functional disability among individuals aged 65 to 74 years. In this age group, improvement of lifestyle, health promotion and interventions for MetS from middle age may prevent future functional disability.
Metabolic syndrome (MetS) is shown to be as a risk factor for cardiovascular diseases, however, it is controversial whether MetS is significantly associated with functional disability among older people. Moreover, whether the association differs depending on sex or age is unknown.
This study showed that MetS was a risk factor for future functional disability in both men and women aged 65 to 74 years. In the analysis with severe cases, a marginal significant association was found in men aged 65 to 74 years.
This community-based study shows the importance of prevention of MetS from middle age to prevent future functional disability. This study revealed a high-risk group for functional disability associated with MetS. Our finding may contribute to maintain and improving quality of life of the older people.
Introduction
According to the World Population Prospects, the population aged 65 years or older is estimated at 19.6% in more developed regions in 2021. 1 Of these, Japan has the most aged population, with 29.1% of the population aged 65 years or older in 2023. 2 With the aging of the population in Japan, the number of people who needs medical support or long-term care insurance (LTCI; the Japanese government’s official care support system for people with functional disability) has been increasing. 3 Thus, preventive measures for future development of functional disabilities are crucial to shorten the unhealthy period and improve the quality of life of older people.
Metabolic syndrome is defined by a cluster of interconnected factors that increase the risk of coronary heart disease, cardiovascular atherosclerotic diseases, and diabetes mellitus. 4 In a meta-analysis of cohort studies, MetS was shown to increase the risk of incident stroke. 5 Stroke is the most common cause of LTCI in Japan except for women aged 75 years or older. 6 However, whether MetS contributes to an increase in the risk for future development of disability has remained controversial. Two prospective studies showed that MetS contributed to a high risk of functional disability,7,8 while another study showed that MetS did not increase the risk of functional disability. 9 A study conducted in Japan showed that there was no association between Mets and LTCI certification. 10 The reason for the different results of those studies is not clear; however, sex- and generation-based differences in the association between MetS and disability were not addressed in those studies. Sex- and generation-based differences in the association between MetS and disability may have contributed to the inconsistent results of previous studies. Therefore, we should elucidate the extent to which MetS contributes to an elevated risk of the future development of functional disability separately stratified by sex and generation. This study aimed to separately determine the association between MetS and functional disability in older Japanese individuals using sex- and age-stratified groups.
Methods
Study Population
The Iwate KENpoku Cohort Study (Iwate KENCO Study) was a population-based prospective study that was conducted in rural areas of Japan from 2002 to 2005. The details of the methodology of the Iwate-KENCO Study have been described in a previous paper. 11 As the purpose of the study was to investigate the risk of initial events in apparently healthy older people, the exclusion criteria encompassed those who had already been certified for LTCI (n = 94), those with a history of cardiovascular diseases (n = 654) who were at high risk for LTCI, and those with at least one missing variable in the analysis (n = 960). 12 Of the 12 791 participants aged 65 years or older, 11 083 participants (4407 men and 6676 women) were finally included in the present analysis (Figure 1). The baseline characteristics of the study subjects and excluded participants are shown in Supplemental Table 1. The study subjects included large percentages of subjects with favorable lifestyle habits such as non-smoking and non-drinking. The prevalences of MetS and its components were not different between the groups. This non-invasive observational study was conducted in compliance with the Declaration of Helsinki and was approved by the Institutional Review Boards of Medical Ethics Committee of Iwate Medical University (approval number H13-33; latest approval date: July 25, 2022). All participants were informed of the potential risks and benefits before they provided written informed consent.

Flow chart in the study population.
Definition of MetS
MetS was defined according to the revised National Cholesterol Education Program’s Adults Treatment Panel III (NCEP ATP III) guidelines. 13 The definition includes the following 4 items: overweight (body mass index [BMI] ≥25 kg/m2), low level of high-density lipoprotein cholesterol (HDLC) (<40 mg/dl in men, <50 mg/dl in women) or on treatment, elevated blood pressure (systolic blood pressure ≥130 mmHg and/or diastolic blood pressure ≥85 mmHg or on treatment or with a history of hypertension), and glucose intolerance (glycosylated hemoglobin [HbA1c] ≥6.0 %) according to the National Health and Nutrition Survey in Japan or treatment for elevated glucose or on treatment or with a history of diabetes mellitus. 14 BMI was used as the alternative definition to abdominal circumference to determine overweight. Triglycerides and fasting glucose, which are influenced by diet, were not used because the blood samples were non-fasting blood samples. According to NCEP ATP III, we categorized participants as those who had at least 3 items of the 4 criteria (MetS group) and those who had <2 items of the 4 criteria (non-MetS group) in the present study.
Outcome Definition
The LTCI system is designed to provide care for older people who need assistance in daily living. Care services are available if individuals need support, such as support for housework, personal care and other daily activities, after becoming bedridden, demented, or otherwise. The criteria for such services are uniformly and objectively defined nationwide. 15 To receive LTCI services, older people or their caregivers need certified official care requirements. The LTCI level is assessed by an initial on-site decision with structured questionnaires, home-visit report (regarding the patient’s current physical status, mental status, and use of medical services) by trained local government officials, and a medical doctor’s opinion. The applicants are also assessed for activities of daily living (ADLs) and instrumental ADLs (IADLs). The data are entered into a computer by government officials to calculate the applicant’s standardized scores for the 7 dimensions of physical and mental status and to estimate the time taken for each of the 9 categories of care (grooming/bathing, eating, using the toilet, transferring, assistance with IADLs, behavioral problems, rehabilitation, and medical services).16,17 There are 7 levels of long-term care certificates: support levels 1 and 2 (people with a requirement of daily assistance) and care need levels 1 (least disabled) to 5 (most disabled). 3 In this study, LTCI data (date of certification, levels of support/need for care) were provided by each municipality and wide-area government based on an agreement on data use. 18
The outcome was functional disability defined as being newly certified by the LTCI system during the observation period. The primary endpoint was any level of support and care needed in LTCI. We also examined whether MetS contributes to more severe needs for nursing care, and the second endpoint (severe functional disability) was care need level 2 or higher. Care need level 2 indicates difficulty in performing personal care tasks or in keeping a standing position and walking. 19
Data Collection
Supplemental Table 2 presents the data collection process used in this study. The survey items used in this study were obtained from the municipal annual health check-up and a self-reported questionnaire of the baseline survey conducted concurrently. From the health check-up data, we used anthropometry, blood pressure, blood samples (HbA1c, HDLC), medical history, smoking status, and drinking status from a medical interview. From the self-report questionnaire, we used information on marital status, the number of people living together, employment, duration of education, exercise habits, and sleep duration. Although these variables have not been validated, they have been widely used in several large epidemiological studies in Japan. All questions were developed with reference to previous studies.20,21 LTCI data (date of certification and levels of support/need for care) were provided by the municipality with prior consent. Detailed methods have been described in a previous paper. 18
Statistical Analyses
Multivariable-adjusted hazard ratios (HRs) of incident functional disability in the MetS group were estimated using the non-MetS group as a reference, separately according to sex and age (65-74 years; 75 years or older). Confounding social risk factors (single, living alone, no job, educational status, smoking status, drinking status, exercise habits, and sleep duration) were adjusted for. Additionally, we estimated multivariable-adjusted HRs of severe functional disability in the same way. The assumption of proportional hazard was verified using log-log survival curves. Interactions between sex-and age-stratified groups and MetS were properly checked. In sub-group analyses, we evaluated the linear relationships between functional disability and MetS components (per an increment of component). To confirm whether each component of MetS (overweight, low HDLC, elevated blood pressure, and glucose intolerance) contributes to an increased risk of functional disability, we estimated multivariate-adjusted HRs for functional disability. We also performed Cox regression analysis after excluding incident cases of stroke during the observation period to reconfirm whether MetS contributes to functional disability even after excluding stroke, which is one of the common causes of LTCI certification. All p-values were 2-tailed, and a P value < .05 was regarded as statistically significant. All statistical analyses were conducted using IBM SPSS statistics 25.
Results
The total observation period was 113 643 person-years and the mean (standard deviation) observation period was 10.5 (2.4) years. A total of 1,282 men and 2162 women were certified for LTCI during the observation period.
Table 1 shows the baseline characteristics of the participants with MetS and those without MetS. Of the 11 083 participants, 461 men (10.5%) and 1237 women (18.5%) had MetS. Men with MetS included larger percentages of subjects with no job and non-drinkers. Although women with MetS included larger percentages of subjects with no job, a short period of education and long sleep duration than those in women without MetS, there were no significant differences between the 2 groups in the percentages of subjects with smoking, drinking, and exercise habits. Among the participants with MetS, the order of frequencies of MetS components was elevated blood pressure, overweight, glucose intolerance, and low HDLC in men, and the order was elevated blood pressure, overweight, low HDLC, and glucose intolerance in women.
Baseline Characteristics According to Metabolic Syndrome.

Note. Continuous variables: calculated by t test and expressed as mean (standard deviation). Categorical variables: calculated by chi-square test and expressed as proportion (%).
MetS = metabolic syndrome; HDLC = high-density lipoprotein cholesterol.
Figures 2 and 3 show multivariate-adjusted HRs and their 95% confidential intervals (CIs) of functional disability (whole care need level and severe care need level of LTCI certification) in the MetS group overall and in stratified age groups separately by sex. In age-stratified analyses, MetS significantly increased the risks of functional disability in both men and women aged 65 to 74 years, but it did not contribute to an increased risk of functional disability in either men or women aged 75 years or older. Interactions between MetS and sex or age group were not observed (P > .175). After excluding deaths within 3 years of registration, MetS still contributed to an increased risk in both men and women aged 65 to 74 years (data are not shown). In severe cases using care need level ≥2 as the endpoint, a marginal significant association (P = .079) was found in men aged 65 to 74 years. On the other hand, MetS significantly decreased the risk of severe functional disability in women aged 75 years or older.

Hazard ratios for functional disability according to metabolic syndrome by age group (men). MetS = metabolic syndrome; LTCI = long-term care insurance; HR = hazard ratio; CI = confidential interval. Analyzed by Cox proportional hazards model adjusted for age, single, living alone, no job, educational years, smoking status, drinking status, exercise habit, and sleeping duration.

Hazard ratios for functional disability according to metabolic syndrome by age group (women).
Table 2 demonstrates the multivariate-adjusted HRs (95% CIs) for functional disability according to the number of MetS components stratified by sex and age groups. The risk of functional disability was significantly increased with an increment of MetS components in both sexes aged 65 to 74 years. Table 3 presents the multivariate-adjusted HRs (95% CIs) for functional disability according to MetS components stratified by sex and age groups. Each MetS component independently increased the risk of functional disability in particular groups: glucose intolerance and elevated blood pressure independently increased the risk in men and women aged 65 to 74 years, overweight independently increased the risk in women aged 65 to 74 years, and glucose intolerance independently increased the risk in women aged 75 years or older. Similar results were obtained after introducing each component of MetS simultaneously (data are not shown). Analysis excluding incident cases of stroke during the follow-up period demonstrated that the risk of functional disability was significantly high (1.34 [1.03-1.73]) in men with MetS who were aged 65 to 74 years. In contrast, no association was identified in men aged 75 years or older or in women with MetS. Among the stroke-excluded men aged 65 to 74 years, the HRs (95% CI) between MetS components and risk of disability were 1.41 (1.14-1.74) for glucose intolerance and 1.11 (0.91-1.34) for elevated blood pressure.
Hazard Ratios for Functional Disability According to the Number of Metabolic Syndrome Components by Sex and Age-Groups.

Note. Analyzed by Cox proportional hazards model adjusted for age, single, living alone, no job, educational years, smoking status, drinking status, exercise habits, and sleeping duration. P for trend:linear relationship according to the number of metabolic syndrome components (per component increase).
HR = hazard ratios; CI = confidential interval; LTCI = long-term care insurance.
Hazard Ratios for Functional Disability According to Metabolic Syndrome Components by Sex and Age-Groups.
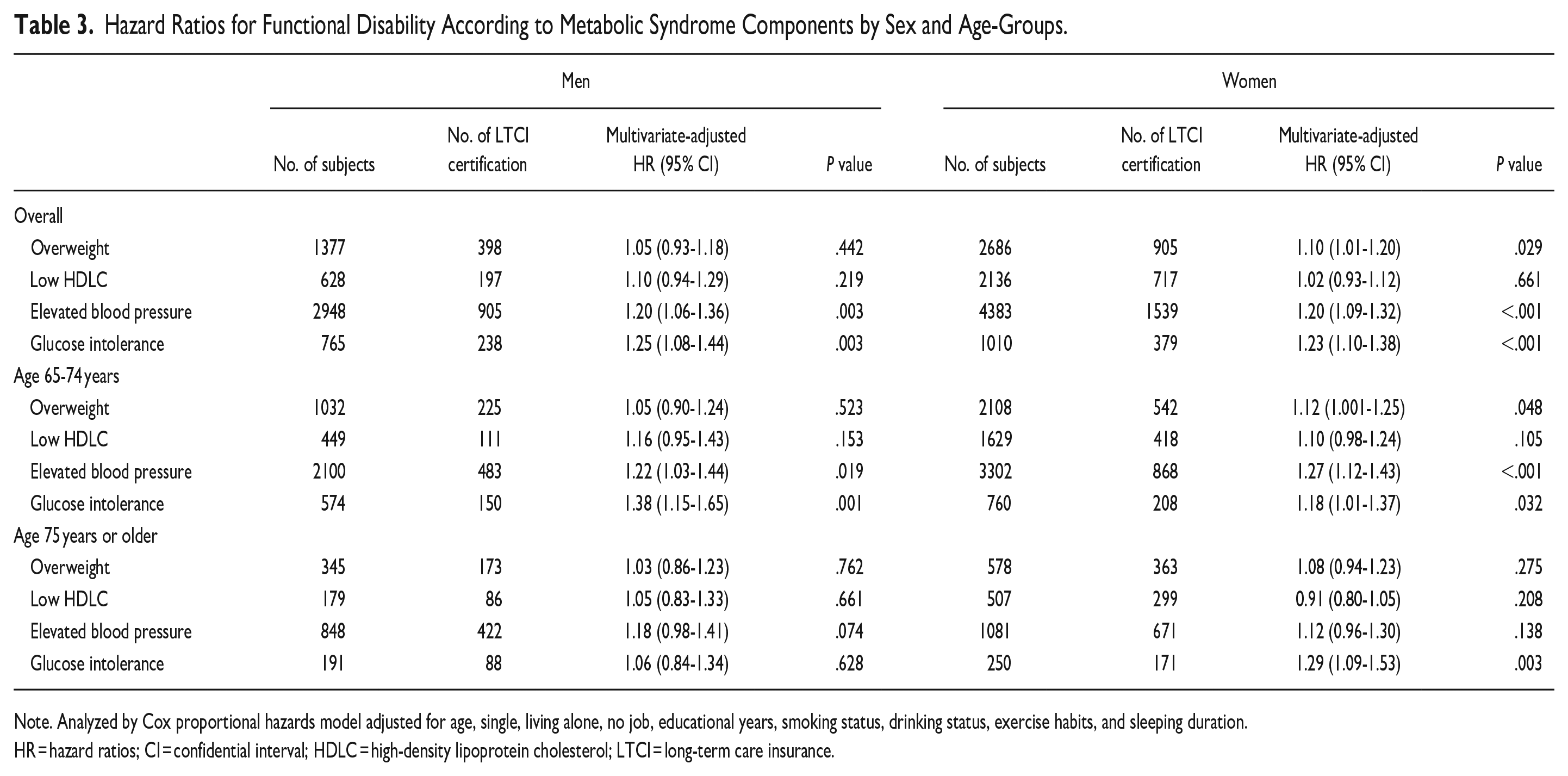
Note. Analyzed by Cox proportional hazards model adjusted for age, single, living alone, no job, educational years, smoking status, drinking status, exercise habits, and sleeping duration.
HR = hazard ratios; CI = confidential interval; HDLC = high-density lipoprotein cholesterol; LTCI = long-term care insurance.
Discussion
We demonstrated that MetS was significantly associated with new LTCI certification in both men and women aged 65 to 74 years; however, there was no significant association in either men or women aged 75 years or older. Similar results were obtained even after excluding deaths within 3 years of registration. Our findings suggested that MetS contributes to an increased risk for functional disability in Japanese people aged 65 to 74 years.
Our study revealed sex-specific and age-specific associations between MetS and functional disability. To the best of knowledge, there has been no studies on the association between MetS and functional disability in a study population stratified by sex and age. Penninx et al 22 examined the sex-specific association between MetS and mobility limitation using 4.5-year follow-up data for 2920 community residents aged 70 to 79 years without mobility limitation at the baseline survey. They showed a stronger association between MetS and functional disability in women than in men. The adjusted relative risks (95% CI) were 1.30 (1.09-1.57) in men and 1.57 (1.36-1.82) in women. In contrast, our results showed a stronger association in men than in women, although there was no interactive effect by sex. In the Penninx study, the age range of the participants was narrower than that in our study, and the study had a relatively small sample size. Furthermore, the outcome was defined as mobility limitation, which differs from the LTCI. Differences in the population analyzed and in the definition of functional disability may have caused differences in the results according to sex. In Japan, Kitamura et al examined the age-specific association between MetS and functional disability in older people aged 65 years or older similar to our study. They demonstrated that MetS was not associated with LCTI certification in participants aged 65 to 74 years or in those aged 75 years or older. 10 They employed the Japanese MetS criteria with the requirement of abdominal obesity. A major difference in the NCEP III criteria might have influenced the differences in the results of our study. Additionally, multivariate analysis was not performed separately according to sex. Further studies on the sex- and age-specific associations between MetS and functional disabilities are needed. Our additional analysis excluding stroke patients during the follow-up period showed that MetS contributed to an increased risk of functional disability in men aged 65 to 74 years. That result is consistent with the results of the study by Penninx et al 22 Previous studies have shown that MetS was associated with sarcopenia, knee osteoarthritis, and cognitive decline.23 -26 Therefore, MetS may have influenced the development of functional disability attributable to factors other than stroke in men aged 65 to 74 in our study. In contrast, in women aged 65 to 74 years, MetS did not contribute to the increased risk of functional disability in analysis excluding stroke patients during the follow-up period. The onset of stroke may have been a factor in LTCI certification in women aged 65 to 74 years. Conversely, in women aged 75 years and older, MetS was demonstrated to be a protective factor for severe functional disability in our study. Women aged 75 years or older might have avoided the risk of functional disability until later in life, possibly due to a more favorable lifestyle compared to that of men, as indicated by our cohort. Additionally, the contribution of MetS to functional disability may vary with age. Previous reports have demonstrated that the impact of risk factors for cardiovascular disease generally declines with aging.27,28 Similarly, the impact of MetS on functional disability may have diminished in women aged 75 years or older in our study. Given that these studies did not examine sex, further studies on sex-specific changes in cardiovascular risk contribution over time among older adults are needed.
Our study showed that the risk of functional disability was increased as the number of MetS components increased in both sexes overall and aged 65 to 74 years. Previous studies showed that more severe MetS, as indicated by the number of MetS components, predicts future functional disability.7,22,29 The results of those studies are similar to the results of our study. However, it is not possible to discuss the differences by sex or age since analysis in previous studies was not conducted separately for sex and age. Among the components of MetS, elevated blood pressure and glucose intolerance were particularly associated with an increased risk of functional disability. Hypertension and glucose intolerance have been reported to be risk factors for physical disability.30,31 In addition, overweight was significantly associated with functional disability among women aged 65 to 74 years. The results of a previous study revealed that there were significant gender and BMI interaction effects among older adults and that women with obesity were most functionally impaired. 32 Overweight may be an important factor for functional disability for older women. Since we did not have information the underlying causes of LTCI certification, we cannot further address the mechanism of the association between MetS and functional disability. Further studies on the pathway of MetS to functional disability in older people are needed. However, our findings highlight the importance of further research on ongoing lifestyle improvements and health-promoting behaviors in middle age.
There are 3 limitations in the present study. First, our study showed that MetS contributed to future functional disability in an apparently healthy population without cardiovascular disease. Therefore, we should be cautious in extrapolating the results of our study to a population that includes individuals with cardiovascular disease. Second, the definition of MetS in this study was based on the NCEP ATP III criteria. In this study, BMI was used instead of abdominal circumference, HbA1c was used instead of fasting blood glucose to determine glucose intolerance, and triglycerides were excluded from the criteria. A previous study conducted in Japan showed that different MetS criteria had different abilities to predict the risk of cardiovascular diseases. 33 Different MetS criteria may therefore have different abilities to predict functional disability, and attention should be paid when comparing the results of this study with results obtained using other criteria. Finally, the variables utilized in our study were not individually validated for reliability. However, the lifestyle habits and demographic data analyzed in our study are widely employed in epidemiology, and we referenced previous studies. Therefore, the absence of individual validation does not pose a concern.
Conclusion
In conclusion, MetS increased the risk for future functional disability in both men and women aged 65 to 74 years in an apparently healthy population. Improvement of life style and prevention of MetS are needed to decrease the risk of functional disability in late life.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580241273103 – Supplemental material for Sex- and Age-Specific Associations Between Metabolic Syndrome and Future Functional Disability in the Japanese Older Population
Supplemental material, sj-pdf-1-inq-10.1177_00469580241273103 for Sex- and Age-Specific Associations Between Metabolic Syndrome and Future Functional Disability in the Japanese Older Population by Naomi Takahashi, Megumi Tsubota-Utsugi, Shuko Takahashi, Yuki Yonekura, Masaki Ohsawa, Toru Kuribayashi, Toshiyuki Onoda, Nobuyuki Takanashi, Kiyomi Sakata, Takehiko Yamada, Kuniaki Ogasawara, Shinichi Omama, Fumitaka Tanaka, Koichi Asahi, Yasushi Ishigaki, Ryo Itabashi, Hiroaki Itamochi, Fumiaki Takahashi, Akira Okayama and Kozo Tanno in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580241273103 – Supplemental material for Sex- and Age-Specific Associations Between Metabolic Syndrome and Future Functional Disability in the Japanese Older Population
Supplemental material, sj-pdf-2-inq-10.1177_00469580241273103 for Sex- and Age-Specific Associations Between Metabolic Syndrome and Future Functional Disability in the Japanese Older Population by Naomi Takahashi, Megumi Tsubota-Utsugi, Shuko Takahashi, Yuki Yonekura, Masaki Ohsawa, Toru Kuribayashi, Toshiyuki Onoda, Nobuyuki Takanashi, Kiyomi Sakata, Takehiko Yamada, Kuniaki Ogasawara, Shinichi Omama, Fumitaka Tanaka, Koichi Asahi, Yasushi Ishigaki, Ryo Itabashi, Hiroaki Itamochi, Fumiaki Takahashi, Akira Okayama and Kozo Tanno in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors would like to thank the participants of this study, the staff of Iwate Health Service Association and the staff in all municipalities (Iwate Prefecture, Ninohe City, Ichinohe Town, Karumai Town, Kunohe Village, Yamada Town, Miyako City, Iwaizumi Town, Tanohata Village, Kuji City, Fudai Village, Noda Village and Hirono Town).
Author Contributions
Conceptualization, K.T. and A.O.; methodology, Na.T., M.T.-U., and S.T.; formal analysis, Na.T., M.T.-U., and S.T.; investigation, K.T., Y.Y., T.K., S.O., T.O., M.O., F. Tan., and T.Y.; data curation, T.O.; writing-original draft preparation, Na.T.; writing, review, and editing, M.T.-U., S.T., Y.Y., M.O., T.O., No.T., K.S., T.Y., K.O., S.O., F. Tan., K.A., Y.I., R.I., H.I., F.Tak., A.O. and K.T.; project administration, A.O. and K.T.; funding acquisition, K.T., A.O., K.O., and K.S. All authors have read and agreed to the published version of the manuscript.
Data Availability
As they are sensitive in nature and are maintained based on agreement with the study participants, this study’s data and materials are not available to other researchers to reproduce the results or replicate the procedure.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.T-U., K.T., Y.Y., and A.O received a research grant from Eli Lilly Japan K.K. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results. None of the other authors declares a conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from Japan Arteriosclerosis Prevention Fund; a grant-in-aid for Scientific Research (C) from the Japan Society for the Promotion of Science (JSPS KAKENHI Grant Numbers JP17K09126 and JP21K10477); and a grant-in-aid from the Ministry of Health, Labor and Welfare, Health and Labor Sciences research grants, Japan (H23-Junkankitou [Seishuu]-Ippan-005; H26-Junkankitou [Seisaku]-Ippan-001; H29-Junkankitou-Ippan-003;20FA1002 and 23FA1006); and Eli Lilly Japan K.K.
Ethical Approval
This study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Medical Ethics Committee of Iwate Medical University (approval number. H13-33; latest approval date: July 25, 2022).
Consent
All participants were informed of the potential risks and benefits before providing written informed consent.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.