
Abstract
The Age-Friendly Health System (AFHS) movement has spread widely in recent years, with nearly 5000 healthcare organizations across the country recognized as Age-Friendly. Despite this broad recognition, there is little focus on how AFHS are implemented and the impact of implementation. The objectives of this study were to describe the strategies employed to support AFHS implementation in outpatient settings and to identify the measures used to evaluate implementation and effectiveness. We conducted a systematic review of literature from multiple databases spanning 2015 to March 2024, identified eligible studies using predefined inclusion/exclusion criteria, and extracted key data (eg, study design, study population, implementation strategies, outcomes/measures). We identified ten eligible studies from primary care clinics (N = 8), convenient care clinics (N = 1) and a cancer center (N = 1). The studies employed over 65 implementation strategies and 98 outcomes or measures. The vast majority of measures mapped to components of the 4Ms (Mobility, Mentation, Medication, What Matters), with up to ten measures per M category. Five of ten studies had reporting discrepancies and four did not fully define outcomes. The ten included studies serve as clear examples for the need for more evidence to support AFHS implementation in outpatient settings. Existing research lacks strategy specification and standardization of measures. We present gaps and opportunities to advance from AFHS “recognition” to impact.
Introduction
The Age-Friendly Health System (AFHS) movement has undergone rapid growth since merging with the 4Ms Framework less than 10 years ago. 1 As of August 2024, nearly 5000 health care organizations across the United States have been recognized as Age-Friendly. 2 AFHS is an initiative of The John A. Hartford Foundation and the Institute for Healthcare Improvement (IHI), in partnership with the American Hospital Association (AHA) and the Catholic Health Association of the United States (CHA). The 4Ms Framework—Mobility, Mentation, Medications, What Matters—provides the structure for this practice transformation. Although evidence supports each M individually, 3 integration of all 4Ms in AFHS as a set potentially enables synergy between practice improvement across the Ms. Questions remain around the recommended frequency of 4M assessment (eg, annually vs matched to health status change) and target population (eg, all older adults vs specific high-risk groups), presenting avenues for future research.
When considering how to optimize AFHS implementation, attention to implementation strategies can standardize efforts and encourage sharing of best practices. Implementation strategies are the actions taken to enhance adoption, implementation, and sustainability of evidence-based interventions. 4 Example strategies are changing recording systems, conducting educational meetings, or accessing new funding. IHI provides care worksheets and case studies to support AFHS implementation and connects participants in Action Communities to develop site-specific implementation plans. IHI’s broad approach focusing on bringing AFHS to all older adults contrasts with efforts of the VA Safer Aging through Geriatrics-Informed Evidence-Based Practices (SAGE) trial, which targets high-risk older adults and prioritizes intervention fidelity over reach. 5 A challenge of AFHS expansion is the huge diversity in organization characteristics—ranging from small physician groups to large integrated health systems. Early adopters of AFHS were primarily hospital systems, and the majority of investigations of AFHS implementation strategies have focused on inpatient settings.6,7 As AFHS is increasingly adopted by outpatient providers and expands to non-Geriatric care settings, knowledge of the diversity and use of implementation strategies is needed to quickly move to impact.
The impact of AFHS implementation is assessed through measures and outcomes. This includes process measures (eg, what percentage of patients were screened for depression—aligned with Mentation), sometimes referred to as implementation outcomes. If the intervention specifies that all older adults should be screened for depression, the frequency of screening is an implementation outcome (fidelity to the intervention). Impact may reflect health service use, such as the rate of hospitalization among those with multiple health concerns. Impact is also assessed through patient-centered outcomes (eg, ability to mobilize around home independently). Outcomes and measures must document both whether the intervention was delivered as intended and the impact of the intervention on patient health and service use.
Among the largest sites employing AFHS, integrated health systems are common (eg, Veterans Health Administration, CVS, Kaiser Permanente). While committing to age-friendly care is an important first step, the ultimate goal of age-friendly care is to determine appropriate strategies to overcome challenges and improve outcomes. To address the need for comprehensive assessment of AFHS implementation in outpatient settings, we conducted a systematic review of the literature. The objectives of this manuscript are to describe which strategies have been employed to support AFHS implementation in outpatient settings and to identify the measures used to evaluate intervention implementation and effectiveness.
Methods
Protocol
The Evidence Synthesis Program at the VA Providence Health Care System used established systematic review methodologies to evaluate the strategies and associated measures of AFHS implementation in outpatient settings. In this report, we focus on describing the implementation strategies and measures used by these studies. The systematic review was registered in PROSPERO (CRD42024547851).
Data Sources and Searches
We searched Medline (via PubMed), EMBASE, CINAHL, Cochrane and clinicaltrials.gov (http://clinicaltrials.gov) from 2015 to March 28, 2024 using Medical Subject Headings and free text terms for age-friendly healthcare, ‘What Matters’, Medication, Mentation and Mobility (see Supplemental Appendix A for complete search strategies). Additional citations were identified from hand-searching relevant systematic and non-systematic reviews.
Study Selection
Study eligibility criteria are listed in Supplemental Appendix B. We included randomized controlled trials (RCTs), non-randomized comparative studies (NRCS), single group, and statistical process control studies. Case studies or case series, qualitative studies, and protocols without empirical data were excluded. Eligible studies evaluated or described strategies to implement an AFHS model, defined as addressing and acting on each of the “4Ms.” We excluded studies using non-AFHS models or strategies focusing on supporting other models of care, models not implementing all 4Ms, interventions for students/trainees who were not offering unsupervised patient care, and educational interventions only assessing changes in knowledge or attitudes but that did not assess implementation. Outpatient care settings included primary care clinics, convenient care clinics, non-urgent care walk-in clinics, or dental settings. Studies that took place in urgent care clinics, emergency departments, post-acute care settings, long-term care settings, surgical centers, transitional care settings, or non-clinical community-based settings were excluded. Finally, AFHS implementation studies included adults aged 65 and older, and/or the providers or staff that serve these individuals. For this manuscript, we did not include conference abstracts due to the limited reporting on strategy details in the majority of those identified.
Screening and Data Extraction
The research team ran one pilot round of 100 citations, where all team members screened the title and abstract of the same citations, and conflicts were resolved as a group. After the pilot round, all citations were independently double screened by the research team and conflicts were resolved by group discussion. We extracted data using Systematic Review Data Repository (SRDR+) (https://srdrplus.ahrq.gov/projects/5433). We evaluated whether the article was free of discrepancies and adequately defined patient eligibility criteria, interventions, and outcomes assessed (Supplemental Appendix C).
Data Synthesis and Analysis
We used Waltz et al’s 8 nine clusters of strategies (derived from the original strategies of the Expert Recommendations for Implementing Change [ERIC] project 9 ) to categorize the implementation strategies employed in each study. The first stage of the ERIC project used a modified Delphi process to identify 73 distinct implementation strategies. Waltz et al 8 examined the relationship between these strategies and identified nine strategy clusters, which we leverage to categorize strategies in this paper. The nine strategy types include “adapt and tailor to context,” “engage consumers,” and “change infrastructure” (examples of each type provided in Table 1).
Waltz Clusters with Example Implementation Strategies (ERIC).

Results
Literature Search
After removal of duplicates, 1537 unique records were screened, 59 studies met criteria for full-text review and 10 studies were eligible and included. Reasons for exclusion at the full-text level included: conference abstract or articles that did not have extractable data (N = 19), no implementation of 4Ms model or only reporting pre-implementation data (N = 12), wrong setting (N = 7), duplicates (N = 6), education-only outcomes (N = 2), protocol without results (N = 1), or other reason (N = 2) (Figure 1).
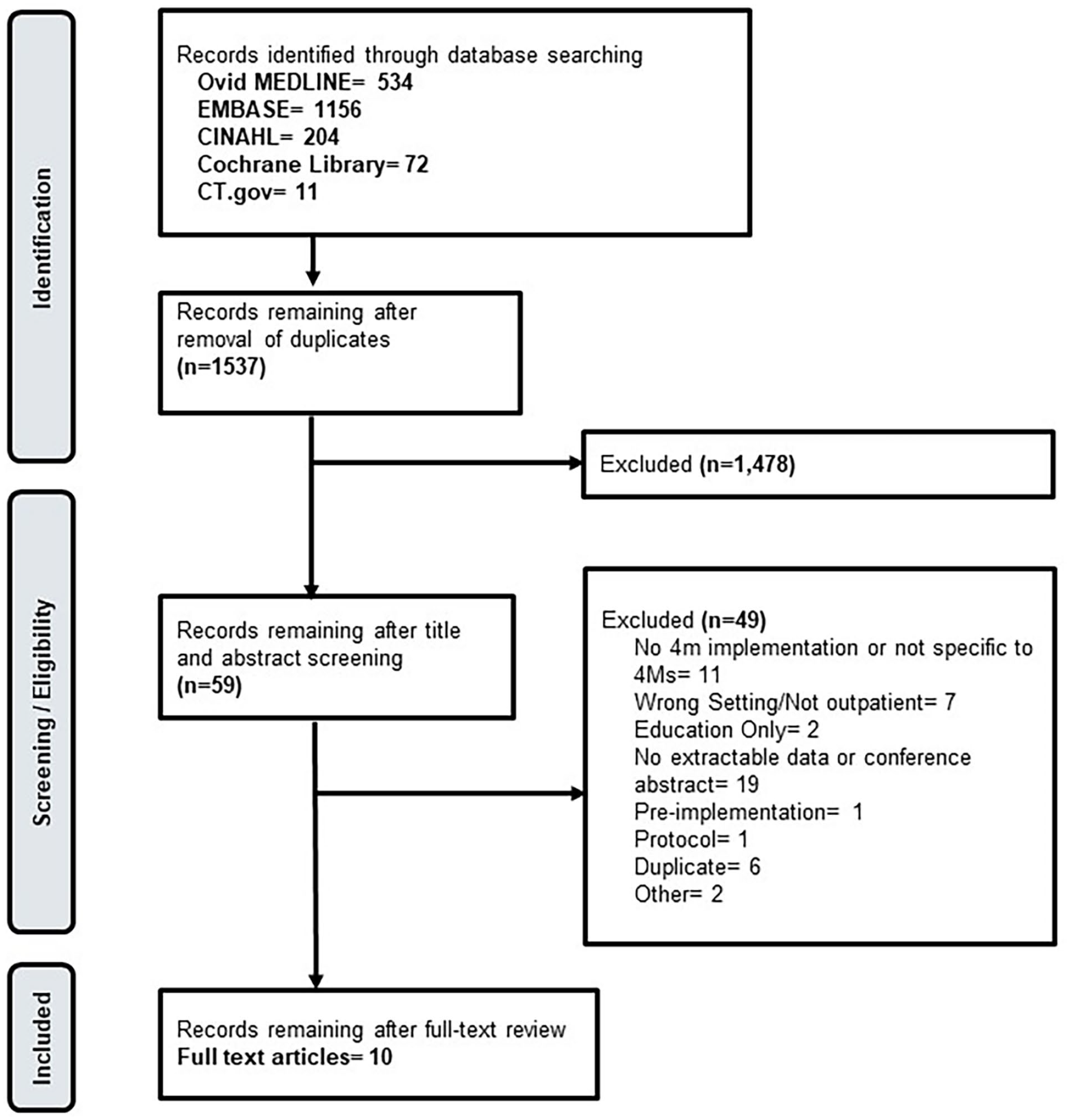
Literature flow diagram.
Study and Participant Characteristics
All ten studies were conducted in the United States and were non-randomized comparative studies (N = 1) 10 or single group studies (N = 9).11 -19 The unit of reporting (“participants”) included patients (N = 10 studies),10 -19 providers (N = 5 studies),11,13,15,16,20 and healthcare facilities (N = 3 studies).10,18,19 Eight studies were conducted within primary care or ambulatory care settings, one study was conducted in a cancer center, one was conducted in convenient care clinics (MinuteClinics). The number of participants per study varied from few (eg, eleven healthcare providers) to more than 300 000 patients in multi-facility studies. The included studies were conducted between 2015 and 2023. Few studies reported racial/ethnicity data for participants (Table 2).
Study Details.

Note. AI = American Indian; NH/PI = Native Hawaiian/Pacific Islander; NR = Not reported; NRCS = Nonrandomized comparative study.
Study compared results at three pilot sites to 18 sites after they implemented strategies at a later date. Because all 21 sites implemented the same strategies we reported this as a single group pre-post study.
Pre-post or multiple time point comparisons.
Patients seen from three pilot sites and 18 comparison sites.
Practice that specializes in the case of older adults with medical, medication, and psychosocial needs during the study period.
Rural Primary Health Care.
Providers completed the orientation introducing 4Ms care.
Study compared a site that incorporated a templated note as part of their electric health record to a site that implemented AFHS but did not use a templated note. Because the overall strategies and 4Ms assessments were different between sites, we reported this as a single group study.
Who received training.
Of participants provided feedback by completing the knowledge survey (N = 16).
Within an academic health system.
Geriatrics, Internal Medicine, three family medicine clinics.
Study Clarity
Using criteria set by the review team, five of ten studies had discrepancies or lacked clarity in reporting, and four did not fully define outcomes. Eligibility criteria was unclear in three of ten studies. All ten studies adequately described the intervention of the 4Ms of AFHS (Supplemental Appendix Table C).
Implementation Support Strategies
The ten included studies employed over 65 implementation strategies, aligning with all nine of the Waltz strategy clusters (Table 3). Two studies15,17 described two different sets of strategies, so were considered separately in this table. One study 10 included 20 different strategies in the initial phase of the study but later used two groups of strategies (PDSA and Virtual Clinics). Because the specific strategies included within these later two were incompletely described, we included the initial 20 strategies when examining Waltz clusters. All strategies identified in the included articles employed more than one of the Waltz clusters (mean 4.5, range 3-7). The most commonly used strategy clusters were to support clinicians (N = 11), change infrastructure (N = 9), or train and educate shareholders (N = 8). Other strategy categories identified included use evaluative and iterative strategies (N = 7), engage consumers (N = 6), develop shareholder interrelationships (N = 6), adapt and tailor to context (N = 4), provide interactive assistance (N = 2), and utilize financial strategies (N = 1).
Strategies by Waltz Categories. “X” Indicates Waltz cluster associated with identified strategies.

Strategies to support clinicians included providing reminders about the 4Ms and sharing 4Ms clinical data to support decision making. Change infrastructure included implementation of a templated note into the electronic medical record, revisions to the intake packet, and creating electronic message boards. Strategies to train and educate shareholders included training on the 4Ms or infrastructure changes, development of educational support materials, or peer consultations. Use of evaluative and iterative strategies included Plan-Do-Study-Act, utilizing data dashboards and other forms of performance feedback and tracking, and ongoing process evaluation. To engage consumers, studies developed recruitment processes for annual wellness visits or developed pocket cards about the 4Ms to engage patients as active participants in their care. Strategies to develop shareholder interrelationships included the development of interprofessional teams. Strategies to adapt and tailor to context included use of data experts or tailoring strategies. Project facilitation was employed to provide interactive assistance. To utilize financial strategies, one study incorporated financial incentives for completion of the 4Ms. The strategies used in each study, along with the Waltz categorizations associated with each strategy, can be found in Table 3.
AFHS Outcomes and Measures
A total of 98 outcomes or measures were assessed by the ten studies. The large majority of outcomes could be mapped to individual Ms (Figure 2; Supplemental Appendix Table D). Figure 2 shows the variety of ways each M was measured across studies. What Matters was assessed with five different outcomes, with “Advance care planning (ACP) on file or discussed” or “Asked ‘what matters’” used in all ten studies to fulfill this M. Medication was predominantly assessed through “review and reconciliation” (N = 5) and identification of high risk medications (N = 4). Mobility showed the greatest variability in reported outcomes, with 10 different outcomes used to measure completion of this M. The most common measures were “fall risk assessed” (N = 5) and “timed up and go (TUG) test” (N = 3) or referral to physical therapy (N = 3). Mentation was frequently assessed through cognitive screening (N = 8) or depression screening (N = 5) but was also associated with five less commonly used outcomes (eg, referred to social work, hypertension control). Three studies included composite measures for completion of all 4Ms. One study included measures not clearly aligning with particular Ms (FRAIL—Fatigue, Resistance, Ambulation, Illness, Loss of weight—a five-component scale for frailty; SNAQ—Simplified Nutrition Appetite Questionnaire—assessing appetite loss and risk for weight loss).

4Ms outcomes.
Discussion
After conducting a systematic review, we identified and analyzed ten peer reviewed studies of implementation of AFHS in outpatient settings. These studies described over 65 strategies used with implementation and 98 measures and outcomes. Clinically, these studies provide a foundation for teams and health systems looking to become AFHS, but these studies are likely insufficient to meet the needs of all potential implementation sites. Strategies employed were inadequately specified to allow for replication in other settings. Outcomes were variable in how they were used to describe impact at the level of individual Ms and lacked the broad scope needed to more comprehensively assess impact of AFHS implementation. As such, there is ample opportunity for current and future AFHS to measure and describe their experience with implementation of AFHS. Studying implementation of AFHS is critical to addressing the challenges of reproducibility and reliability that invariably arise with multicomponent studies in large complex systems.
The ten studies in our review included a wide range of characteristics and implementation strategies, with most studies including four different types of implementation strategies. By categorizing the strategies according to established clusters, we were able to show which are more commonly used (eg, supporting clinicians) and which were rarely used (eg, providing interactive assistance). Categorizing and assessing the frequency of strategy use by cluster provides an immediate visualization of opportunities for future implementation. Within the “change infrastructure” strategy cluster, many studies employed electronic health record templates to facilitate AFHS implementation. This represents a more feasible strategy than, for example, altering incentive structures, which falls within the “utilize financial strategies” cluster and was employed by just one study. Through accumulation of outcomes data around both cost and quality of care associated with AFHS transformation, health systems may be able to leverage strategies with even broader impact.
None of the studies explicitly specified strategies to determine the effect on intervention fidelity or other outcomes. This specification on the use of strategies is necessary to analyze the effects of strategies on outcomes. Many of the outcomes assessed by the ten studies aligned with individual “M” measures included in the IHI care plan worksheet, 21 the completion of which is required for level one AFHS recognition. We also noted significant variability in the measures used to fulfill each M (eg, ten measures to assess Mobility). Acknowledging the complexity of health systems and individual care settings, the AFHS movement would benefit from standardized measures to determine AFHS impact and allow for comparable analyses across settings and populations. Such standardization will require significant resources and organizational capacity.
A major goal of the AFHS movement is dissemination beyond Geriatric specialty settings, where 4Ms assessment is more established, and into other health care fields such as primary care, surgery, and acute care. Among the ten studies included in our outpatient review, seven were in non-Geriatric specialty primary care settings,10 -12,14,16,17,19 an encouraging finding as the AFHS movement progresses. Six of these seven studies received support from Geriatrics Workforce Enhancement Programs (GWEPs), HRSA funded programs that educate and train the healthcare workforce caring for older adults.11,12,14,16,17,19 Five of the seven primary care studies implemented AFHS in Annual Wellness Visits (AWVs),11,12,14,17,19 prevention-focused visits that align well with 4M assessment. Though none of the ten studies explicitly discussed the optimal frequency for 4M assessment, AWV integration mirrors the IHI’s call for annual 4M assessment. Two studies in Geriatric specialty settings integrated 4Ms at intake,13,18 and just one study utilized 4Ms in risk stratification in weekly high-risk rounds, 13 with the nine other studies broadly applying 4Ms to all older adults. Two primary care studies mapped the 4Ms to Center for Medicare and Medicaid Services (CMS) Merit-based Incentive Payment System (MIPS) measures, leveraging pre-existing data collection and incentive structures to drive AFHS transformation.16,19
While several studies assessed the rates of completion of all 4Ms, few studies included global measures of AFHS implementation. Global measures assess the impact of all 4Ms and include quality of life, home days, and patient or caregiver experience. 22 Home time, which uses administrative data to subtract days spent in a hospital or nursing home, has been increasingly employed as an outcome to support patients’ desires to age in place. 23 Quality of life is not routinely assessed in outpatient care and patient and caregiver experience if often narrowly assessed through satisfaction. 22 Global measures of AFHS implementation could mirror existing efforts to support the Quintuple Aim: (1) patient/caregiver experience, (2) population health, (3) reducing costs, (4) care team well-being, (5) health equity. 24 The Quintuple Aim, an expansion of the previous Triple Aim and Quadruple Aim, seeks to provide a more equitable, effective, and holistic approach to healthcare. A minority of studies in our review included outcomes related to patient/caregiver experience and none included measures related to the other four Aims.
Strengths and Limitations
There are several strengths and limitations to the current review. We included rigorous search and screening methods for study identification, and only included studies describing IHI-based AFHS models. This evidence base is quickly evolving; since completion of our citation search in March 2024, several additional studies of AFHS implementation are planned 25 or have been published.26,27 For study inclusion, we required that studies implement a strategy to support the AFHS model and measure outcomes beyond educational improvements. This excluded a number of studies that examined outcomes related to AFHS implementation but only for educational improvements. Further, some implementation strategies and their accompanying outcomes were not fully described in all studies, which may have led to inaccurate or incomplete categorization of these strategies and outcomes. Because we required that studies implement all 4Ms as part of their intervention, it is possible that we may have excluded studies that report on strategies used to implement individual component Ms of the 4Ms AFHS.
Conclusion
The AFHS movement has rapidly gained momentum, with nearly 5000 sites recognized. As regulations and incentives increase participation, AFHS transformation requires strategic guidance about implementation that is built from the scientific literature and the pragmatic experience of current AFHS. The ten peer reviewed studies serve as clear examples for the need for more evidence to support AFHS implementation in outpatient settings. Studies used multiple strategies, tailoring implementation to the resources and strengths of the individual healthcare organization or setting. Most studies focused on measures aligning with individual Ms, which while important for AFHS recognition, provide limited insight into the impact of AFHS transformation on global measures. We also highlight the need to standardize measures to support reliable and accurate comparisons of AFHS implementation across diverse settings. As the AFHS transformation continues to take hold throughout the United States, this review presents the strategy and outcome opportunities for clinicians and researchers to advance from AFHS “recognition” to impact.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251318244 – Supplemental material for Strategies and Outcomes of Age-Friendly Health System Implementation in Outpatient Settings: A Systematic Review
Supplemental material, sj-docx-1-inq-10.1177_00469580251318244 for Strategies and Outcomes of Age-Friendly Health System Implementation in Outpatient Settings: A Systematic Review by Rebecca J. Howe, Katherine Rieke, Thomas Bayer, Htun Ja Mai, Jennifer L. Sullivan, Jane A. Driver, Taylor Rickard, Thomas A. Trikalinos, James Rudolph, Ellen McCreedy and Eric Jutkowitz in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors are grateful to Gaelen Adam, PhD, MLIS and Becky Baltich Nelson, MLS, MS, for assistance with search strategy development, Cheryl R. Banick, MLIS for text retrieval, and Anayah Sanders and Andrea Schwartz, MD, MPH, AGSF for their contributions to this project.
Disclaimer
This manuscript was prepared by the Evidence Synthesis Program Center located at the VA Providence Health Care System, directed by Eric Jutkowitz, PhD and James Rudolph, MD and funded by the Department of Veterans Affairs, Veterans Health Administration, Health Services Research and Development. The findings and conclusions in this document are those of the author(s) who are responsible for its contents and do not necessarily represent the views of the Department of Veterans Affairs or the United States government. Therefore, no statement in this article should be construed as an official position of the Department of Veterans Affairs.
Data Availability Statement
The data generated and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Health Services Research & Development, Department of Veterans Affairs, ESP 22-116.
Ethical Approval and Informed Consent Statements
There are no human participants in this article and informed consent is not required.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.