
Abstract
This study explores the implementation of the Age-Friendly Health Systems (AFHS) 4Ms Framework into primary care clinics in rural Arkansas, facilitated by the AGEC and funded by The Health Resources and Services Administration’s Geriatric Workforce Enhancement Program (GWEP) grant. Implementation success is evaluated by monitoring merit-based incentive payment system (MIPS) measures and other variables, providing insight into the effectiveness of integrating AFHS and enhancing older adult care. AGEC employed implementation strategies (train-the-trainer, audit and feedback, and clinical reminders using Electronic Medical Record (EMR)), the i-PARIHS implementation framework, and the RE-AIM evaluation framework to facilitate integration of the AFHS 4Ms Framework into partnered rural federally qualified healthcare clinics (FQHC). AGEC aimed to equip the healthcare workforce through comprehensive training sessions and resource provision. Additionally, the EMR system modifications guided clinicians in aligning care with the AFHS 4Ms Framework. This multifaceted approach ensured a systematic and tailored implementation, enhancing the capacity of rural FQHCs in Arkansas to deliver Age-Friendly care. Improvements were observed in MIPS outcome measures, including increased completion of fall and depression screens, Annual Wellness Visits (AWV) and Advance Care Plans (ACP). These changes reflect a proactive impact on comprehensive care delivery for older adults. Since adopting the AFHS 4Ms Framework, these rural Arkansas FQHC clinics have significantly enhanced their older adult care, earning recognition as AFHS Clinics by the Institute for Health Improvement (IHI). Primary care practices nationwide can implement similar evidence-based approaches to improve care for the expanding older adult population in the U.S.
Keywords
We already know that the older adult population in the United States is fast-growing and that Age-Friendly Health Systems (AHFS) principles are evidence-based to improve person-centered healthcare outcomes for the older adult population.
Our research contributes significantly to the field of healthcare by addressing the pressing need for Age-Friendly care in rural primary care settings through: (1) Implementation of AFHS Framework, (2) Evidence-based models and strategies including i-PARIHS, RE-AIM and train-the-trainer, (3) Improvements in care delivery (via MIPS measures: AWVs, ACPs, falls and depression screens), and (3) Recognition and replicability via highlighting the success and impact of the implemented interventions.
Our research’s implications toward theory, practice, and policy underscore the effectiveness of integrating the AFHS 4Ms Framework into rural primary care clinics, providing actionable and tangible insights for practitioners (comprehensive training, resource provision, EMR system modifications), informing policy decisions, and contributing to efforts aimed at addressing healthcare disparities in older adults and promoting healthcare equity.
Introduction
Aging Population in the U.S. and Arkansas
The population of older adults is rising steadily as more people in the United States are living healthier, more productive, and longer lives past 65 years old, yet the number of healthcare professionals (HCP) specializing in geriatrics has not increased accordingly. 1 The U.S. population aged 65+ grew from 2010 to 2020 at the fastest rate since 1880 to 1890. 2 From 2019 to 2020, the older adult population 65+ in the U.S. increased from approximately 52.8 to 54.6 million, 3 but only 315 new Medical Geriatric Subspecialty Certificates were issued by the American Board of Medical Specialties in the same period. 4 Furthermore, people aged 65+ represented 16% of the population in 2019 and are projected to reach 21.6% by 2040. 5 In addition to the sheer lack of HCPs specializing in geriatric care, older adults often have complicated health histories that can hinder access to care and lead to increased healthcare costs. Consistent with the rest of the U.S., Arkansas’ 65+ population increased from 15% to 17% of its total population from 2010 to 2019, an increase of over 60,000. 6 Arkansas (AR) ranks 42th out of 50 states in overall health. 7 Thus, improving access to optimal, Age-Friendly practices is critical as Arkansas’ older adult population continues growing, especially in rural areas where specialized healthcare resources may be more sparse than in urban regions.
Geriatric Workforce Enhancement Programs (GWEP) and Clinical Partnership
The Health Resources and Services Administration (HRSA) funds programs to support the education of HCPs and students, connect older adults to educational programs, and empower older adults to play an active role in their healthcare decisions. HRSA funds GWEPs to improve health outcomes for older adults by developing a healthcare workforce that maximizes patient and family engagement and by integrating geriatric best practices into primary care. 8 GWEPs receive funding under Title VII and Title VIII of the Public Health Service Act. 9 The following is the journey of a GWEP located in the rural state of AR in their efforts to improve older adults’ healthcare in rural Federally Qualified Healthcare Center (FQHC) clinics.
The only GWEP in AR, the AR Geriatric Education Collaborative (AGEC), resides within The University of Arkansas for Medical Sciences in The Donald W. Reynolds Institute on Aging. AGEC partners with the largest FQHC in Arkansas, ARcare, which began as one rural clinic in 1986. Since 2022, ARcare has served over 106,990 patients and has expanded to surrounding southern states. Each year, approximately 12 000 people aged 65+ are treated at ARcare clinics. ARcare is Joint Commission on Accreditation of Healthcare Organizations (JCAHO) and Utilization Review Accreditation Committee (URAC) accredited and received awards for 2022 Covid-19 Public Health Champion, HRSA Access Enhancer 2022, and 2022 Health Disparities Reducer. ARcare employs trained providers in medications for opioid use disorder (MOUD) and diabetes self-management, connecting patients to multi-modal services and resources within their primary care clinic.
Foundations of Age-Friendly Health Systems and Applications in Primary Care
In 2017, five major U.S. health systems (Anne Arundel Medical Center, Ascension, Kaiser Permanente, Providence, and Trinity Health) joined geriatric experts in reviewing the literature for ways to reliably apply 4 essentials of geriatric healthcare, known as the “4Ms”: what Matters, critical interactions of high-risk Medications, Mentation screenings for dementia, delirium, and depression, and Mobility screenings.10,11 In late 2019, HRSA shared this initiative with GWEPs nationwide. The John A. Hartford Foundation and the Institute for Healthcare Improvement (IHI) sponsored a healthcare initiative in partnership with the American Hospital Association and Catholic Health Association of the U.S. to concertedly address the health needs of the growing aging population via a framework called “Age-Friendly Health Systems (AFHS).” Two levels of certifications from IHI were established for which clinics could apply: Level I (AFHS Participant) and Level II (Committed to Care Excellence). To receive one of these certifications, a clinical site must integrate Age-Friendly principles and the 4Ms Framework into daily practice, namely centering conversations around “What Matters?” 12 “What Matters” involves honoring the older adult’s choices, priorities and goals. Evaluating Mobility aims to ensure older adults’ safety in different environments via balance assessments and falls plans of care as needed. “Mentation” includes screenings and determining appropriate next steps for dementia, depression, and delirium. “Medication” involves the American Geriatric Society’s (AGS) Beer’s Criteria, assessing risks and benefits of prescribed and over-the-counter medicines to ensure necessity and safety, especially as to not interfere with What Matters, Mentation, or Mobility.
The reach of an AFHS surpasses primary care and permeates into the clinic’s associated community; it promotes interprofessional teamwork and practice throughout the continuum of care for older adults. 1 Creating such systems involves understanding and respecting the needs, values, and preferences of older adults and educating healthcare workers to focus on the AFHS 4Ms Framework. 1 This study describes the implementation of the AFHS 4Ms Framework in rural FQHCs in AR, funded by HRSA’s GWEP grant. We discuss early implementation success through monitoring MIPS measures and other variables and provide insights into the effectiveness of integrating AFHS practices to enhance care for older adults in rural ARcare clinics.
Methods
ARcare excels beyond many primary care practices in rural AR; however, ARcare previously lacked a specific framework for an evidence-based approach for geriatric care. As ARcare adds multimodal services (i.e., medical nutrition therapy), particularly relating to chronic conditions, providers will benefit from post-graduate training to improve older adult care across the health spectrum. Equipping the healthcare workforce with an evidence-based framework for older adult care aims at improving clinical quality, patient safety, and early identification of risks. In 2019, AGEC and ARcare began their journey implementing the AFHS 4Ms Framework through HRSA’s GWEP initiative. AGEC’s clinical aim is infusing geriatric content into rural primary care practices for optimal healthcare of older adults. To fulfill this initiative in AR, AGEC partnered with ARcare rural FQHC sites. AGEC planned to add one new ARcare clinic each calendar year of the five-year GWEP grant.
Implementation Science Framework and Strategies
AGEC utilized the multidimensional revised Integrated-Promoting Action on Research Implementation in Health Services (i-PARIHS) framework by working with ARcare providers and clinical staff to help them understand the practical nature of getting evidence into practice. 13 The i-PARIHS framework helped AGEC identify potential barriers and facilitators, and guided AGEC’s selection of implementation strategies; it specifies barriers and enablers influencing implementation outcomes. 14 The core constructs of the i-PARIHS framework are facilitation, innovation, recipients, and context, with facilitation actively assessing, aligning, and integrating the other three constructs. 15 Health Services researchers use the i-PARIHS to assess factors impacting implementation and to identify optimal interventions and implementation strategies. 16 In this study, the i-PARIHS framework guided AGEC during its implementation efforts (Table 1). AGEC used three context elements (leadership, culture, and measurement) of the i-PARIHS framework 16 and the role of facilitator element. AGEC identified no current comprehensive geriatric assessments or strategies used with geriatric patients within ARcare. Thus, AGEC used this knowledge gap as evidence within the i-PARIHS framework and operationalized AFHS guidelines via the 4Ms Framework to measure reach, effectiveness, adoption, implementation fidelity, and maintenance to ensure ongoing improvement. Next, to operationalize i-PARIHS, AGEC facilitated AFHS trainings with ARcare providers and staff, and provided continuous coaching and support through in-person (pre-COVID) and virtual communication and training (post-COVID).
Strength of Various i-PARIHS Constructs and Definitions in Partnered ARcare Clinics After Implementation of AFHS 4Ms Framework.

AGEC utilized a train-the-trainer strategy for improving evidence-based decision making in primary care. In a train-the-trainer program, practitioners and professionals are trained in a specific area while receiving instruction on how to effectively train, monitor, and supervise colleagues. 18 Research suggests this implementation strategy is effective in increasing knowledge and improving patient outcomes and clinical behavior in various healthcare environments, including geriatric medicine.18,19
Through the ARcare and AGEC partnership, AGEC coordinates monthly educational trainings to the healthcare workforce regarding healthy aging topics, including Annual Wellness Visits (AWV), Advance Care Plans (ACP), fall risk screenings, depression screens, opioid-risk evaluations, and incontinence screenings. These topics relate to a Medicare incentive system, the Merit-Based Incentive Payment Systems (MIPS). ARcare’s data team (community health worker and grants manager) generate MIPS reports for AGEC as needed for HRSA (quarterly, annually, etc.) and engages in QI-related reports. MIPS data are tracked via Practice Analytics, ARcare’s data management software, from billing codes from ARcare’s EMR system, Intergy.
A training schedule included monthly, in-person trainings, each with a geriatric or AFHS-focused topic. The partnership began with one clinic in Lonoke County in 2018. Six additional clinics joined from 2019 to 2023, from rural counties of Woodruff, Lonoke, White, Cross, and Saline. The overall implementation goal was to systematically investigate the baseline MIPS clinical data while addressing clinicians’ deficits in knowledge related to AFHS and MIPS measures. Besides train-the-trainer, AGEC also used additional implementation strategies including audit and feedback, and EMR-based clinical reminders (pop-up cues for nurses to conduct a TUG mobility test on an older adult if that patient had “2 or more falls” or “1 fall with injury” since their last visit. Descriptive data was collected from ARcare’s FQHC healthcare leadership team (providers, nurses, MAs, grant managers, and EMR nurse informaticist) via qualitative testimonials, virtual meetings, and workflow mapping in EMR during a 12-month period; this data helped identify facilitators, potential barriers, and other opportunities for implementation while motivating clinical champions in each clinic.
AGEC provided ARcare with definitions of each MIPS measure to be tracked and reported back to HRSA. ARcare’s nurse informaticist used these definitions to build the baseline reports needed for AGEC to track clinical efficiencies in older adult care. AGEC used each clinic’s baseline MIPS data from the calendar year preceding the respective training start date. Many of ARcare’s EMR data points needed improvements—including ACPs, Fall Risk Assessment, Future Fall Risk, Hypertension Control, A1c Control, Depression Screens, and Medicare AWVs—before the data could be reliably used.
In early 2019, the second rural ARcare FQHC clinic joined the AGEC partnership; here, the older adult population was about five-times that of the first clinic. This second clinic also had a more influential footprint, which led to more community involvement, including health fairs, caregiver education, and dementia-related community classes in the local library. AGEC also trained local community fitness staff in an evidence-based neurocognitive exercise program.
Together, AGEC and ARcare’s leadership team (nurse informaticist, medical director, medical coder) made additional changes to improve documentation for falls, depression, and delirium screens in 2021. Additions included the Timed-Up-and-Go (TUG), an evidence-based test for Mobility, the PHQ-9, and Confusion-Assessment-Method (CAM) for Mentation. Improved training materials included updated EMR screenshots of evidence-based tests within the “geriatric” tab of ARcare’s EMR alongside instructions for conducting efficient older adult screenings. Following the trainings, trainees completed quality improvement (QI) projects via the Plan, Do, Study, Act (PDSA) model to implement and track changes in MIPS measures. Through 2023, five additional ARcare clinics were added, making a total of seven FQHCs. Clinical champions were designated at each site to help make the AFHS integration a success, and to ensure the AFHS 4Ms screenings were incorporated into older adults’ plans of care; champions helped coordinate training times and submitted QI projects for low-performing MIPS measures. During this time, AGEC and ARcare decided that ARcare’s EMR system needed additional customization to capture and track the remaining untracked MIPS measures: Dementia Caregiver Education and Support, Evaluation for Opioid Misuse, Urinary Incontinence (UI) Assessment in females, and High-Risk Medication Reviews. Thus, check boxes for customized high-risk medication reviews, the Opioid Risk Tool (ORT), detailed UI screening questions, and dementia/caregiver education tools were built into ARcare’s EMR, allowing for the tracking and reporting of all relevant MIPS measures.
Implementation Evaluation
AGEC felt it was important to keep morale/culture strong as to not insult the intelligence or practice of any clinician, especially because while the label of “AFHS 4Ms Framework” was new to the clinics, many of its elements (ie, depression screenings) were not. With the heavy assistance of ARcare’s EMR data analyst and nurse informaticist, AGEC and ARcare created a series of reports to capture EMR data of MIPS measures, and created an ongoing auditing and feedback system. AGEC used the facilitation element to support and encourage habitual clinical practice changes when caring for older adults. Consistent with existing literature, AGEC evaluated implementation success using the Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) framework. Additionally, the RE-AIM Framework guided MIPS baseline data collection and continuous re-evaluation. 11 The RE-AIM framework helped assess implementation of AFHS by informing logic models used to operationalize implementation success. 11 Furthermore, this study considers training attendance, testimonials from healthcare providers, QI projects (via PDSA), and changes to MIPS measures (screening efficiencies) to reflect implementation success. AGEC’s structured approach of operationalizing the i-PARIHS framework and evaluating with the RE-AIM framework allowed rural ARcare primary care sites to effectively implement and sustain AFHS practices tailored to the needs and contexts of older adults in their communities.
Of note, prior to implementation of AFHS 4Ms Framework, two partnered sites were already exposed to MIPS measures during previous AGEC trainings. To reduce confusion while increasing cohesion, AGEC designed an educational algorithm (Figure 1) linking MIPS measures to AFHS, guiding clinicians to easily relate these principles.
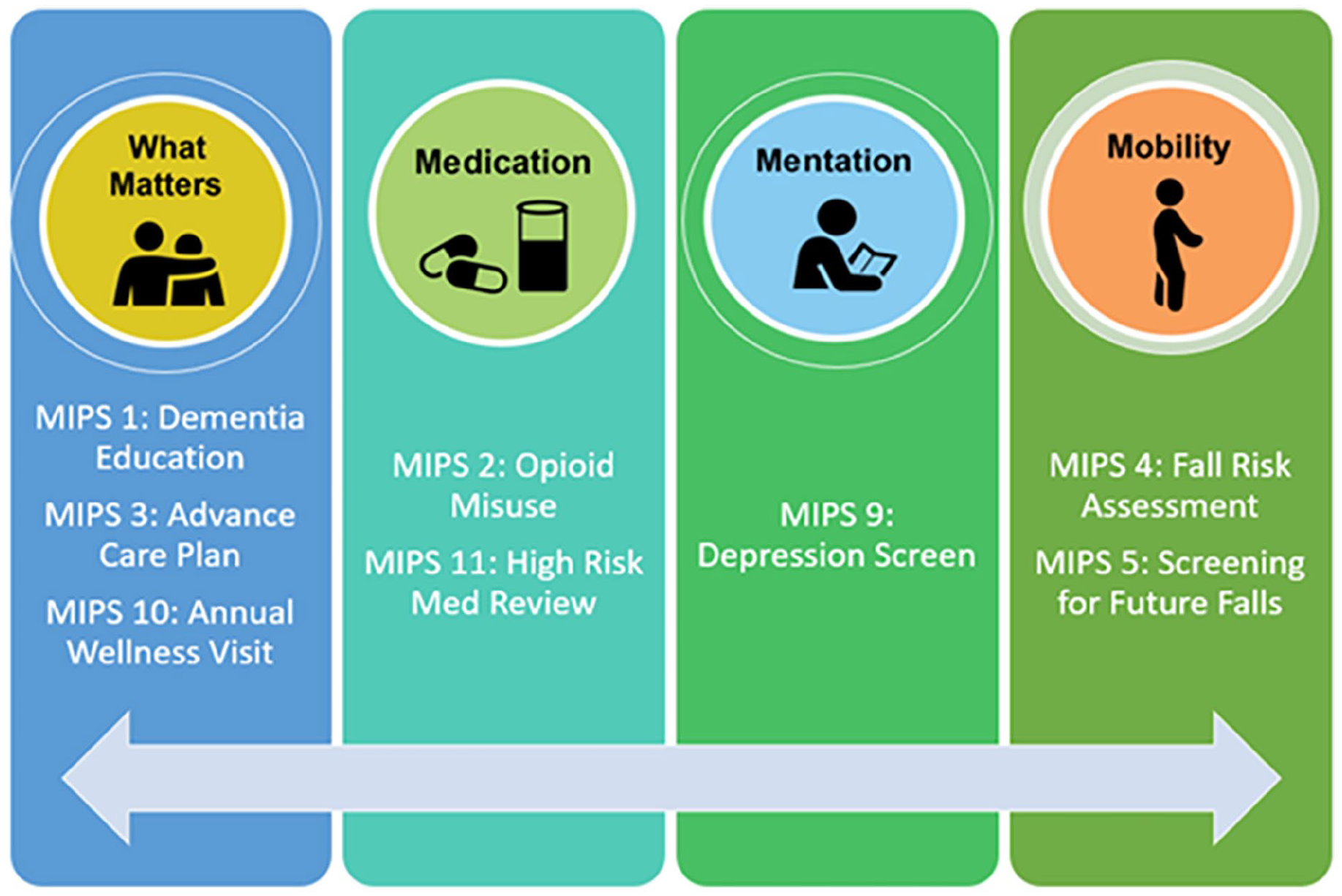
AGEC’s AFHS 4Ms and MIPS educational algorithm.
At the center of AFHS 4Ms Framework is what Matters; AGEC encouraged clinicians to ask older adults the “What Matters most?” question as often as possible but, at minimum, during AWVs, as this would allow older adults to discuss priorities like staying mentally sharp, avoiding falls, establishing caregivers via ACPs, and staying independent. By asking this simple question, clinicians were taught to seamlessly transition into conducting MIPS screens, such as depression and fall screens, when appropriate. AGEC created and utilized infographics as visual references for QI projects as seen in Figure 2. Older adults were commonly missing or canceling their Annual Wellness Visits (AWV); to further address QI and patient adherence, AGEC and ARcare co-designed an informative, patient-facing tri-fold educating older adults on the importance and purpose of AWVs (Figure 3).

Infographic used by AGEC to support clinician implementation of AFHS 4Ms “Mentation” and MIPS measure improvement per QI project.

Trifold used by ARcare-AGEC partnership as a QI project to improve AWVs.
Trainings educated clinicians that these powerful AFHS 4Ms conversations were a gateway to improving older adults’ healthcare while improving their clinic’s MIPS measures. For example, in line with the “what Matters” facet of AFHS, ARcare’s EMR was updated to include MIPS 1 (Dementia Caregiver Education and Support). To further connect ARcare’s healthcare workforce with the newly added EMR system updates, AGEC trained all clinical and non-clinical staff on dementia concepts adapted from Dementia-Friendly AmericaR, communication tips for families and caregivers of persons with dementia, and tips for comprehensible signage in the clinics to help reduce patient confusion.
During the process of providing updated trainings to ARcare staff, the COVID-19 pandemic crippled Arkansas beginning in March 2020. However, AGEC quickly pivoted to virtual education, which also helped simultaneously reach HCPs in multiple clinics during a singular telehealth training. To assist with the transition of training platforms, in 2020 AGEC received additional support from HRSA’s CARES/COVID-19 Relief funding. These funds helped improve older adults’ access to telemedicine services via telehealth software; telehealth kits were provided to older adults needing glucometers, blood pressure monitors, thermometers, and/or weight scales. Thanks to remote patient monitoring (RPM) services for these devices, older adults’ health data were electronically received and reviewed by ARcare’s RPM nurses. AGEC also utilized relief funds to help expand a variety of online programs for older adults on social media platforms, including virtual Tai-Chi for ARcare’s older adults to stay mentally and physically active during the pandemic, and “AGECaring Friends,” a monthly newsletter printed and delivered alongside Meals on Wheels programs in Central Arkansas.
Each year, ARcare’s partnership with AGEC involved monthly trainings for new clinical staff on MIPS and AFHS principles, while staff from existing clinics attended quarterly updates. New employees were encouraged to join any training to familiarize themselves with the AGEC partnership, MIPS, and AFHS. In early 2023, AGEC employed a train-the-trainer strategy where an ARcare educator, trained by the AGEC clinical coordinator, led successful integration of the AFHS 4Ms framework in partnered ARcare clinics and now conducts most virtual trainings.
Results
The RE-AIM implementation science framework was particularly useful when training ARcare clinics in the evidence-based strategy of AFHS. Specifically, Reach was utilized alongside the AGEC strategic workplan goals of partnering with one new ARcare clinic per year (except during COVID when this was tripled). Effectiveness and Adoption of the RE-AIM framework guided assessment of changes in clinical practice following trainings and patient outcomes, as measured by MIPS performed with older adults; barriers and facilitators were discussed by AGEC and the ARcare trainer and staff throughout AFHS trainings as necessary. The Implementation and Maintenance elements of RE-AIM assisted AGEC and its partnered ARcare clinics in reassessing the fidelity and quality of the training curriculum, particularly focusing on sustainability of AFHS. AFHS sustainability was further supported under AGEC’s recent GWEP funding from HRSA (2024 to 2029) , which includes an online training toolbox available via AGEC’s website. RE-AIM implementation success was evident in measures of training efficiencies, qualitative testimonials, 1:1 meetings with satisfied providers, and various successful QI projects (PDSA).In summary, the ARcare HCP workforce excelled in their awareness, screenings, referrals, and efforts—they continue to reach for their goal to improve healthcare for all older adults they treat. Table 2 shows major improvements in MIPS measures made since implementation of the AFHS 4Ms Framework. Finally, formal recognitions from IHI proved successful implementation. Two ARcare clinics received Level II recognition in February 2021 and four received the same in February 2024; one clinic earned Level I certification in February 2024. Additionally, AGEC’s partnership with its home academic institution’s Longevity Clinic led to Level I Age-Friendly certification in summer 2021.
MIPS Measures Improvements in Partnered Healthcare Clinics from 2020 to 2023 After AFHS Training.

Highlights include the range of improvements of 26% to 40% in completion of ACP, 44% to 91% increase in fall risk assessments, 23% increase in the completion of depression screens, and 79% increase in dementia-caregiver education and support following the initiation of AFHS training.
The i-PARIHS and RE-AIM implementation frameworks in combination with the implementation strategies (train-the-trainer, audit and feedback, and clinical reminders in the EMR) provided a comprehensive approach to guide implementation of the AFHS 4Ms Framework in partnered rural ARcare clinics. The healthcare participants’ testimonials and informative meetings during the pre-implementation and implementation phases of the AFHS 4Ms Framework revealed important insights in the choice to revise AGEC’s implementation plan with the addition of the train-the-trainer strategy. Inclusion of this supplemental strategy allowed AGEC to evaluate the implementation outcomes of adoption and penetration through ARcare clinics, which proved internal ARcare employee-led AFHS 4Ms trainings to be successful! Having an internal trainer with ARcare as their primary Age-Friendly champion enhanced learning opportunities for all healthcare staff. Her rich, internal knowledge of the EMR system allowed her to provide accurate and efficient click-by-click instructions of where to locate the required MIPS screening tools and tests for older adult care. Her involvement was crucial in helping clinical staff stay up-to-date with their AGEC trainings. The train-the-trainer strategy also helped enhance buy-in from HCPs and helped increase attendance of required trainings. Additionally, the RE-AIM framework guided meaningful components into the development of AGEC’s AFHS and MIPS algorithm (Figure 1). Through AGEC’s implementation and training in geriatric principles and the AFHS 4Ms Framework, the AGEC-ARcare partnership increased older adult screenings and improved the knowledge base of ARcare’s HCPs who care for the older adult population.
Discussion
Although there is still room for improvement in the MIPS measures, great strides are noted, and the training process is working! AGEC has identified several key factors that helped make these rural practices successful in their Age-Friendly journey, namely the support of ARcare’s leadership in numerous aspects of the grant’s initiatives: staff training time, EMR system changes, community collaborative support, compliance with tracking MIPS data, and application submissions for IHI certification. The EMR system changes were especially critical and led clinical staff to track and improve their performance of older adult screenings. Overall, this partnership promoted the achievement of implementation goals through facilitating innovation, evident in improved MIPS data and qualitative testimonials.
Implementation Barriers and Limitations
AGEC realized that monthly training attendance was inconsistent—even low at times—especially when three newly partnered ARcare clinics joined simultaneously during the COVID-19 pandemic. In qualitative testimonials, many primary care providers highlighted the difficulty of managing walk-in patients during lunch hours, especially when AGEC trainings were scheduled, amidst the pandemic peak. AGEC understood the daily clinical workflow also often did not allow staff to stay attuned to their emails, where training reminders and telehealth links were found. To overcome this hurdle, AGEC made advance phone calls to each clinic, sometimes both a day prior and on the scheduled training day, to remind all HCPs to attend. Low attendance could have also stemmed from HCPs unfamiliarity with AGEC’s clinical coordinator (i.e., an “external” email address). Three clinicians reported in their qualitative testimonial they “felt the 4Ms trainings were more efficient when facilitated internally from their internal provider training [via ‘train-the-trainer’ model]… because EMR examples were shared.” Another barrier AGEC identified was communication issues between ARcare and AGEC during the onboarding of new clinics. One provider’s feedback highlighted that “We’re not told by management that we’re included in new grants like this one, and we’re not paid any extra to do all these ‘extra’ things—they’re just added to our workload on top of all the other patient care and documentation we’re required to do.”
AGEC learned that a critical aspect of assisting clinical staff in implementing practice changes was the integration of screening prompts in the EMR system; these led to more consistent outcome measurements (MIPS) and significant improvements in fall and depression screens, AWVs, and ACPs. Because of their dedication and accomplishments, the ARcare system is ready to expand this AFHS initiative to additional clinics in 2025. While MIPS measures are a static representation of older adults’ healthcare, AGEC, HRSA, and over 40 other GWEPs continuously evaluate the ongoing need to more efficiently and accurately measure training outcomes.
In summary, AGEC’s successes came with setbacks and delays, including the COVID-19 pandemic, and stumbling blocks in the EMR system. However, AGEC discovered new ways to accomplish goals, learning many lessons along the way. One lesson included maximizing virtual trainings and using them as helpful instruments to simultaneously train multiple rural clinics. AGEC adapted to the constant HCP turnover and continuously offered 1:1 or small group trainings to new staff. AGEC acknowledged the critical role of ARcare’s administration in accepting the principles of the AFHS 4Ms Framework, supporting necessary trainings and allocating staff time for them. AGEC will continue strategizing with staff and discuss ways to optimize AFHS. We also plan to further integrate AFHS into community-education endeavors, empowering community members to better serve as their own advocates in AFHS. Doing so encourages informed conversations and decisions between patients and their HCPs. With future GWEP funding, AGEC will create and disseminate two surveys. First is a provider-facing, self-evaluation survey, serving as a tool further evaluating implementation outcomes (ie, fidelity and sustainability), and service outcomes (ie, effectiveness, efficiency, and timeliness). Second is a patient satisfaction survey proving ARcare and AGEC with a realistic, meaningful look into patient’s perceptions of the utility of the AFHS 4Ms Framework.
Overall, implementing the AFHS 4Ms Framework in primary care clinics shows promise in improving older adult healthcare and outcomes, evident in EMR and MIPS measures. The i-PARIHS and RE-AIM implementation frameworks, and the train-the-trainer strategy helped facilitate comprehensive and successful implementation of AFHS 4Ms Framework. Sustainability of AFHS is challenging with continuous turnover of FQHC staff. For other states to be effective with AFHS implementation, AGEC suggests using the RE-AIM implementation science framework, followed by train-the-trainer implementation science strategy with an internal trainer, helping inform about staff changes, ensuring consistent delivery of AFHS principles, and contributing positively to sustainability efforts.
Footnotes
Acknowledgements
We acknowledge our partnered FQHC’s data tools: Intergy Electronic Medical Record (EMR) system and Practice Analytics (PA) data software; these data are not readily accessible by other researchers. However, study materials can be made available to other researchers for replication purposes upon request.
Data Availability Statement
The data that support the findings of this study will be made available from the corresponding author (LTM), upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Health Resources and Services Administration’s Geriatric Workforce Enhancement Program (U1QHP28723 to R.M.). “Research reported in this publication was supported in part by the National Center For Advancing Translational Sciences of the National Institutes of Health under award number U54 TR001629. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.”
Ethical Statement
We affirm that this manuscript submitted to the Journal of Healthcare Organization, Provision, and Financing adheres to the highest ethical standards, ensuring the integrity, transparency, and originality of our research findings.
Informed Consent/Patient Consent
Not applicable for this study. Only deidentified (clinical-level) data was utilized; no identifiable patient or provider-level data was used.
Trial Registration Number/Date
Not applicable for this study. Only deidentified data was utilized; (no patient or provider identified data).
Other Journal Specific Statements as Applicable
Not applicable.