
Abstract
The Chronic Care Model (CCM) is a framework that supports the proactive, planned, coordinated and patient-centered care of chronic diseases. The Patient Assessment of Chronic Illness Care (PACIC) scale is a valuable tool for evaluating patients’ perspectives on chronic care delivery based on the CCM. Few studies have examined its application in China. This study assesses hypertension care in Chinese patients and explores how PACIC scores relate to patient compliance. A cross-sectional study was conducted in Hangzhou, China, from June to August 2021, including 253 hypertensive patients from 5 county hospitals and 13 primary healthcare centers. The study used the PACIC scale to assess hypertension care delivery and the Compliance of Hypertensive Patients scale (CHPS) to measure patient compliance. Multiple linear regression analyses were used to explore the relationship between demographic characteristics and the total and domain scores of PACIC, as well as the association between CHPS and the domain scores of PACIC. The mean value of overall the PACIC score was 3.12 (out of 5). Problem solving/contextual domain had the highest average score for each item, while follow up/coordination domain had the lowest. Patient activation had negative effects on intention (β = −.18, P < .05), attitude (β = −.21, P < .05), responsibility (β = −.17, P < .05), and the total score of CHPS (β = −.24, P < .01). Delivery system design/decision support was negatively associated with lifestyle (β = −.21, P < .05) and the total score of CHPS (β = −.26, P < .01). Hypertensive patients perceived that they sometimes received hypertension care consistent with the CCM in Chinese primary healthcare settings. A higher level of PACIC score was beneficial for improving hypertensive patient compliance.
The Patient Assessment of Chronic Illness Care (PACIC)scale assesses patients’ views on chronic care delivery based on the Chronic Care Model(CCM).
This study evaluates the current situation of hypertension care delivery based on the CCM and explores the association between PACIC scores and patients’ compliance with hypertension.
Hypertensive patients in Chinese primary healthcare settings believed they received some care consistent with the CCM. Higher PACIC scores helped improve patient compliance.
Introduction
Chronic disease is a crucial global public health problem, and hypertension is a highly prevalent chronic condition.1,2 China faces the challenge of hypertension care. According to Chinese Residents’ Nutrition and Chronic Disease Status Report (2020), approximately 27.5% of residents had hypertension. 3 It is concerning that hypertensive patients do not always receive optimal care. The rate of taking prescribed antihypertensive medications among hypertensive adults was only 34.6%, and 12.0% had achieved control in China, 4 which was lower than rates in Western countries like Canada (72.0% taking medication, 58.3% control) and the USA (88.2% taking medication, 43.7% control).5 -9 Current hypertension care is often fragmented and event-driven. For instance, there is suboptimal communication and coordination among the multiple healthcare professionals usually involved in a primary care setting. 10 The historical focus on acute care has meant that healthcare delivery did not prioritize improving patients’ self-management skills. 11 Therefore, the continuity and coordination of hypertension care should be improved.10,12
Delivering high-quality chronic care requires significant system changes beyond just adding new features to the existing acute-focused system. 11 The Chronic Care Model(CCM) aims to improve care delivery by shifting practices from reactive to proactive, patient-centered care through multidisciplinary team collaboration and planned interactions.13,14 Hypertension care is a key part of China’s National Basic Public Health Service Programs, combining clinical and public health services in primary healthcare settings. 10 It follows Chinese guidelines for monitoring blood pressure, managing medication, promoting healthy lifestyles, and providing follow-up care through multidisciplinary teams. Furthermore, the Chinese government has implemented a national policy, called Long Term Planning for Chronic Disease Prevention in China (2017-2025), to improve chronic care by integrating patient-related, professionally-directed, and organizational interventions in the primary healthcare system. Hypertension care in China has evolved with links to the CCM. 15 The Patient Assessment of Chronic Illness Care (PACIC) is a widely used tool for evaluating the alignment of chronic care with the CCM from the patient’s perspective, with good reliability and validity across different cultures.16 -22 The PACIC score can help evaluate patients’ experiences of chronic care delivery, supporting quality improvement efforts in healthcare organizations. 23 However, few studies evaluate the delivery of hypertension care on this scale in primary care settings in China and make cross-culture comparisons. 24 Hence, it is meaningful to evaluate the current status of PACIC in China and to provide strategies to improve the quality of chronic care.
PACIC level might be affected by the gender, age, education, monthly income, years of chronic diseases, and the number of disease conditions.25 -32 However, these factors might vary due to cultural differences. For example, in Singapore, a study among diabetes patients found that having a younger age was positively associated with PACIC scores, while there was no significant difference in education level, gender, and number of chronic diseases. 32 In contrast, another study among Turkish patients with chronic diseases found that having a younger age and a higher education level was negatively associated with PACIC scores. 29
The PACIC has the potential as a quality improvement tool and patient-centered metric. Nonetheless, its effectiveness would be improved by showing its correlation with other quality measures such as patient compliance and quality of life. 33 Evidence suggests that PACIC scores were related to quality of life.34,35 Patient compliance is a broad concept. Patient compliance involves patients wanting to change their lifestyle, working closely with healthcare professionals, making treatment decisions together, and adhering to medication. 36 Non-compliance can lead to inadequate blood pressure control and is a notable issue in chronic care.37,38 Previous research has linked the total or domain scores of PACIC with improved medication adherence and compliance with self-management behaviors among diabetes patients.39 -42 However, more research is needed for other chronic conditions. 31 In addition, limited evidence has examined the relationship between the domain scores of PACIC and a broad array of compliance, such as intention of care compliance and responsibility compliance. Therefore, it is essential to explore the relationship between the domain scores of PACIC and the above aspects of compliance for patients with hypertension.
The current study: (1) evaluated the current PACIC scores of Chinese patients with hypertension, (2) explored the factors that influence PACIC scores, and (3) investigated the relationships between PACIC and patients’ compliance with hypertension. We hypothesized that the PACIC scores were positively related to almost all the hypertensive patients’ compliance.
Methods
Study Design and Settings
A cross-sectional study was conducted from July to August 2021 in Hangzhou City, Zhejiang Province. We selected 3 districts representing the medical group’s poor, fair, and good construction levels. Each district had 2 or 3 medical groups, and each medical group had one county hospital and several community health service centers. One or 2 medical groups were selected from each district, and 2 or 3 community health centers from central and non-central areas were chosen from each medical group. A total of thirteen community health service centers were chosen as investigation sites. Potential participants were approached while waiting for their appointments in the outpatient clinic. The trained interviewers administered self-designed questionnaires after obtaining oral consent from the participants. Criteria for selecting the participants were as follows: (1) over the age of 18, (2) a diagnosis of hypertension or taking an anti-hypertensive drug, (3) using primary health service over the past 6 months, (4) willing to participate in the study, (5) without serious complications. The exclusion criteria were: (1) not being a local resident, (2) not having lived in the area for more than half a year, and (3) inability to communicate in Chinese. To confirm associations, it is recommended to have at least 10 events per analyzed variable.43,44 In our linear regression model, there were 15 predictor variables, including dummy variables, necessitating a sample size of 167 after accounting for a 10% estimation of invalid questionnaires. A total of 265 questionnaires were distributed, and 253 valid questionnaires were returned, resulting in a 95.47% response rate.
Measurements
The PACIC scale, developed by Glasgow et al. was designed to measure the patient assessment of care for chronic conditions according to the CCM. It assesses the behavior of healthcare professionals and practice teams from the perspective of patients. 16 This scale is comprised of 20 items, covering 5 domains: (1) patient activation (3 items, eg., “asked to talk about any problems with my medication history or their effects”), (2) delivery system design/decision support (3 items, eg., “shown the way I took care of my illness influenced my condition”), (3) goal setting/tailoring (5 items, eg., “helped to set specific goals to improve my eating or exercise”), (4) problem solving/contextual (4 items, eg., “asked to how my chronic illness affects my life”), (5) follow up/coordination (5 items, eg., “encouraged to take part in programs in the community that could help me recover from the disease”). Participants were required to rate on a 5-point Likert scale, ranging from 1 (almost never) to 5 (almost always). Total scores range from 20 to 100, with higher scores indicating a more frequent occurrence of the pertinent aspect of chronic care and a better perception of chronic care delivery. 20 The Chinese version of the PACIC scale has been validated in multiple places within several provinces of China. For example, a study in Anhui province among 3434 hypertensive patients suggested good internal reliability (Cronbach’s alpha = .88). 24 More information on PACIC is shown in the Supplemental File.
The Compliance of Hypertensive Patients scale (CHPS) developed by Lahdenperä et al. is one of the most commonly used instruments to evaluate hypertension compliance. 45 In our study, the compliance of patients with hypertension was measured by the Chinese version of the CHPS. 46 To be specific, this scale comprises 13 items across 5 domains: Intention (4 items), Lifestyle (3 items), Attitude (3 items), Responsibility (2 items), and Smoking (1 item). Responses are rated on a 4-point Likert-type scale from 1 (good compliance) to 4 (poor compliance). Total scores range from 13 to 52, where a lower score indicates a higher-level compliance. This version of the CHPS has been used in other Chinese research and found to be reliable in measuring hypertension compliance.46,47 The Cronbach’s alpha was .80 in our study. More information on the CHPS is shown in the Supplemental File.
A self-designed questionnaire was produced to collect demographic characteristics, which include the gender, age, education level, monthly income, years of hypertension, and number of chronic diseases (see Supplemental File for more details).
Statistical Analysis
Data were entered through EpiData 3.1 (The Epidata Association, Odense, Denmark) and analyzed using SPSS 26.0 (SPSS Inc., Chicago, IL, USA). Firstly, descriptive analyses were performed for socio-demographics. Categorical data were listed as frequency and percentage, while continuous data were shown as mean and standard deviation (SD). Secondly, a multiple linear regression was used to analyze the association between demographic characteristics, domain and the total scores of PACIC. Another multiple linear regression was conducted to explore the association between CHPS and the domain scores of PACIC after controlling socio-demographics (the Enter method was used in the multiple linear regression model). As the total and domain scores of PACIC and CHPS were not normally distributed, the data were submitted to the Z-score transformation before entering into the analysis. Multicollinearity was assessed by checking the variance inflation factor (VIF) in a multiple regression model. Variance inflation factors below 5 in our model indicated a low risk of multicollinearity. 48 Model explanatory power was evaluated with R2. The significant level of all the regressions was set at P < .05.
Results
Sample Characteristics
A total of 253 patients with hypertension were eligible. The social-demographic characteristics are shown in Table 1. The mean age of the participants was 65.28 ± 11.80 years, 56.13% were male, 62.10% had a primary education or below, and 63.05% of the participants’ monthly income was less than 3000 RMB. Among the participants, 47.04% had been diagnosed with hypertension for more than 7 years, and 49.80% had co-morbidity diseases.
Demographic Characteristics of the Participants (n, %).

Missing data < 3%.
Scores on the PACIC Scale
In our study, Cronbach’s alpha for the PACIC scale was .89. Scores on the PACIC scale are shown in Table 2. The total score for PACIC was 62.49 (13.25), and the mean value of the overall PACIC score was 3.12 (0.66). The domain scores on the PACIC scale were as follows: patient activation was 10.43 (2.68), delivery system design/decision support was 9.78 (2.30), goal setting/tailoring was 15.00 (3.79), problem solving/contextual was 14.03 (3.45), and follow up/coordination was 13.12 (4.55). The problem solving/contextual domain had the highest average score for each item (3.51 (0.86)), while the follow up/coordination domain had the lowest average score for each item (2.62 (0.91)).
The Total and Domain Scores of the PACIC Scale.

The Influence of Socio-Demographic Characteristics on PACIC Scores
The association between socio-demographic characteristics and PACIC scores was analyzed by multiple linear regression and shown in Table 3. The PACIC scores were positively associated with age (β = .34, P < .001), having a middle school education level (β = .16, P < .05, Ref: primary and below), and having a high school and above education level (β = .28, P < .01, Ref: primary and below), and were negatively associated with more than 3 chronic conditions (β = −.20, P < .01, Ref: one chronic condition). For domain scores, delivery system design/decision support was positively associated with age (β = .33, P < .001), having a middle school education level (β = .21, P < .01, Ref: primary and below) and having a high school and above education level (β = .37, P < .001, Ref: primary and below), and was negatively associated with more than 3 chronic conditions (β = −.24, P < .01, Ref: one chronic condition). Goal setting/tailoring was positively associated with age (β = .34, P < .001), having a middle school education level (β = .15, P < .05, Ref: primary and below) and having a high school and above education level (β = .28, P < .01, Ref: primary and below), and was negatively associated with a monthly income of 3001 to 5000 RMB (β = −.15, P < .05; Ref: less than 3000 RMB), and more than 3 chronic conditions (β = −.19, P < .01, Ref: one chronic condition). Problem solving/contextual was positively associated with age (β = .30, P < .01), having a middle school education level (β = .16, P < .05, Ref: primary and below) and having a high school and above education level (β = .26, P < .01, Ref: primary and below), and was negatively associated with more than 3 chronic conditions (β = −.15, P < .05, Ref: one chronic condition). Follow up/coordination was positively associated with age (β = .19, P < .05).
Liner Regression of Patient Characteristics on the Total and Domain Scores of PACIC Scale (Standardized β Value).
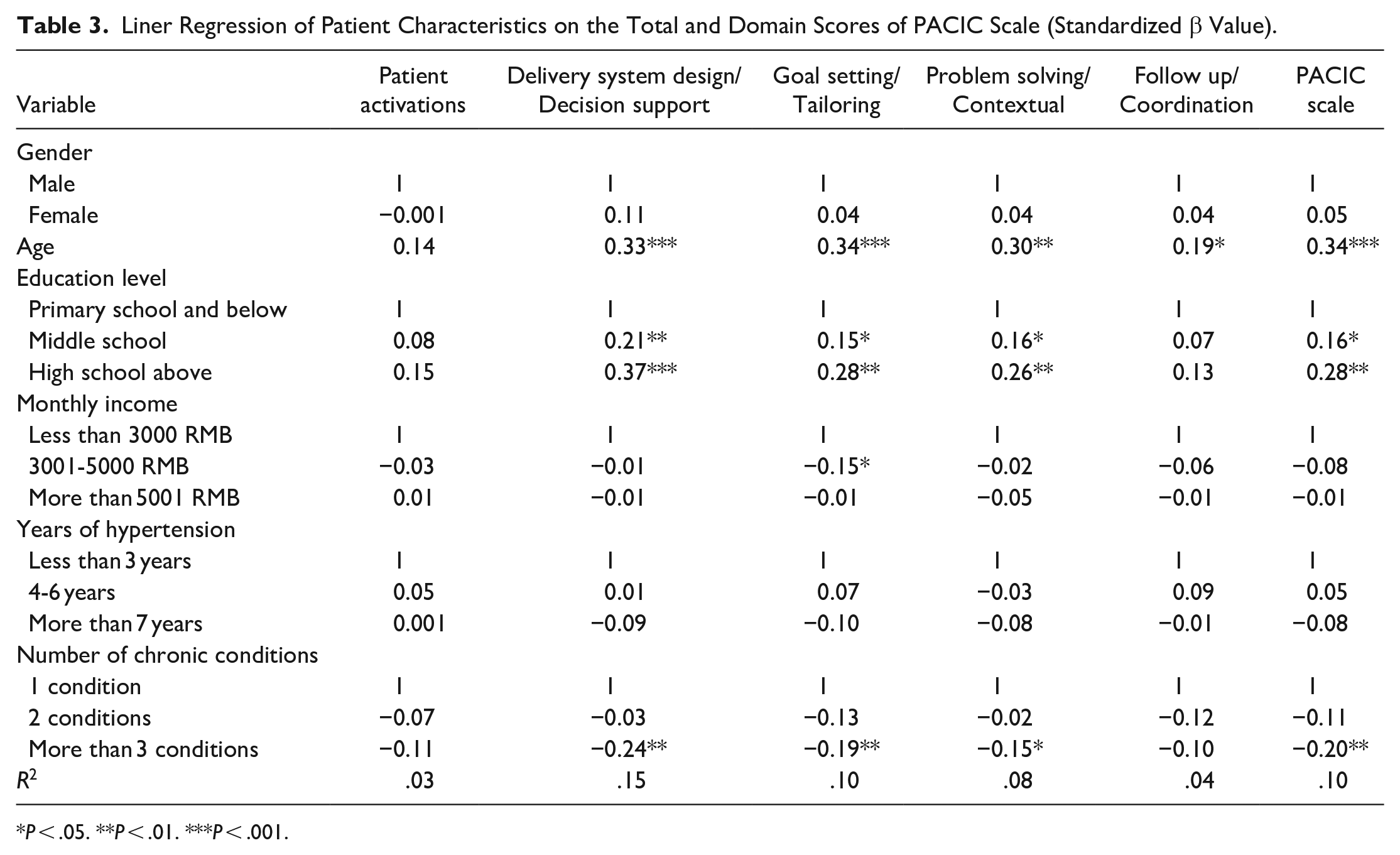
P < .05. **P < .01. ***P < .001.
The Influence of PACIC Scores on CHPS Scores
The associations between the PACIC scores and CHPS scores are presented in Table 4. After adjusting for gender, age, education level, monthly income, years of hypertension, and number of chronic conditions, patient activation had negative effects on intention (β = −.18, P < .05), attitude (β = −.21, P < .05), responsibility (β = −.17, P < .05) and the total score of CHPS (β = −.24, P < .01). Delivery system design/decision support was negatively associated with lifestyle (β = −.21, P < .05) and the total score of CHPS (β = −.26, P < .01). Goal setting/tailoring was positively associated with smoking (β = .29, P < .01).
Liner Regression of Domain Scores of PACIC on Total and Domain Scores of CHPS (Standardized β Value).

Adjusted for gender, age, education level, monthly income, years of hypertension, and number of chronic conditions.
P < .05. **P < .01.
Discussion
This study assessed the current situation of hypertension care based on the PACIC scale in China and first explored the relationship between PACIC scores and broader hypertension compliance. The CCM is promoted as a care template for the chronically ill to improve care. 13 The total score on PACIC among hypertensive patients in our study was 62.49 (13.25), and the mean value of the overall PACIC score was 3.12 (0.66), indicating that hypertensive patients perceived that they sometimes received hypertension care consistent with the CCM in primary healthcare settings. 32 A PACIC survey score of 3.5 or higher was indicative of high concordance with the CCM, as demonstrated in previous research. 49 However, our findings showed that the elements of the CCM have not yet been fully implemented in primary healthcare settings. Compared with previous literature, the mean value of the overall PACIC score among patients with common chronic diseases was slightly lower than in some high-income countries.32,50 That might be because Chinese primary healthcare providers and patients had sufficient awareness of hypertension prevention and control due to the late launch of the hypertension prevention and control system in China. 51
Among the 5 subscales of PACIC, problem solving/contextual and patient activation elements of the CCM had higher scores, indicating a strong relationship between hypertensive patients and their healthcare professionals in sharing treatment decisions in hypertension care. This finding was not consistent with other literature, which suggested that the delivery system design/support decision element of CCM, related to health promotion and self-management, was their highest subscale.19,23,50,52 One potential explanation was that Chinese primary healthcare providers might prioritize providing treatment services for hypertensive patients over conducting health education, possibly due to the medical-oriented nature of their performance evaluations. 12 Another explanation was that Chinese primary healthcare providers had lower health education capacity than those in Western countries.53,54,55 However, other elements, such as goal setting and follow up, had lower scores, similar to the results from other countries.19,29,32,55
Findings from the current study suggested that factors influencing the PACIC scores included age, education level, and number of chronic conditions. Patients in older age groups demonstrated significantly higher scores in nearly all domains and total PACIC scores compared to their younger age groups, consistent with some studies,26,29,56 but not with other studies.30 -32 Patients with higher educational levels were positively associated with nearly all domains and total PACIC scores, similar to some other studies.28,57 This might be attributed to the likelihood that individuals with higher levels of education had greater health literacy and comprehension abilities during medical consultations. 57 The number of chronic conditions in our sample was negatively associated with nearly all domains and total PACIC scores, consistent with some studies,28,58 but contrary to Western studies.59,60 This might be because hypertensive patients with other chronic diseases might have higher expectations for more comprehensive care services from primary healthcare providers than those with only hypertension. However, primary healthcare providers struggled to cope with patients with multiple chronic conditions in China.11,61 Our finding of no significant association between the domain and total PACIC scores and gender is consistent with the findings of some studies,23,29,32,62 but not in a Danish study where the total PACIC score was higher in males than females. 30 Various socioeconomic factors and differences in healthcare systems could influence these differences. Future research on healthcare quality should consider patient ratings of care received alongside data on care provided, as this could provide a more comprehensive understanding of healthcare delivery.
Previous studies have shown that the PACIC scores were associated with some aspects of compliance.41,42,63 We also found similar results in our research. The patient activation element of the CCM was negatively associated with almost all compliance domains, indicating that a higher patient activation score was beneficial for promoting compliant behavior in hypertension.56,64 Effective communications between hypertensive patients and their primary healthcare providers about treatment plans positively influenced patients’ attitudes and self-efficacy, ultimately leading to improved compliance.65,66 Furthermore, the delivery system/support decision element of the CCM was an important influencing factor in lifestyle and total hypertension compliance, consistent with studies.40,67 That could be because primary healthcare providers inform hypertensive patients about effective prevention strategies for chronic lifestyle-related diseases and assist them in understanding how health-related behaviors impact chronic disease risk factors. This could enhance patients’ appreciation of the importance of lifestyle changes and potentially improve their overall compliance. 68
There were some limitations in our study. Firstly, considering our study population consisted predominantly of older patients with hypertension and lower educational status, we had to consider the possibility that the questionnaire might not have been clear enough for some participants to understand. Secondly, our study was conducted among Chinese patients with hypertension from only one city in Zhejiang province. This geographical limitation could affect the generalizability of the findings. Thirdly, our study did not assess inter-rater reliability among the interviewers, which might impact the strength of our results. Future research should use statistical measures like Cohen’s Kappa or intraclass correlation coefficient (ICC) to confirm data consistency.
Conclusions
The Chinese government has been developing strategies based on the CCM to improve chronic care, but the elements of the CCM have not yet been fully implemented in primary healthcare settings. Our findings showed that there was a lack of setting specific goals and arranging follow-ups for hypertensive patients. This required a well-collaborative multidisciplinary team with the general practitioner as the core and other healthcare professionals such as nurses, nutritionists, and pharmacists as members to provide integrated services for hypertensive patients. We demonstrated that the care for patients with multiple chronic conditions was insufficient in primary healthcare settings, so healthcare managers and policymakers should focus on capacity of the primary healthcare settings. We provided evidence to the primary healthcare professionals that their efforts in building good communication with patients to share treatment decisions could improve compliance with hypertension. It is essential for primary healthcare professionals to train their communication skills. Furthermore, to enhance patient compliance, it is recommended that primary healthcare professionals increase the frequency of health education and explain the link between health behaviors and disease outcomes.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241277445 – Supplemental material for Patient Assessment of Chronic Illness Care (PACIC) and Its Influence on Patient Compliance With Hypertension: A Cross-Sectional Study
Supplemental material, sj-docx-1-inq-10.1177_00469580241277445 for Patient Assessment of Chronic Illness Care (PACIC) and Its Influence on Patient Compliance With Hypertension: A Cross-Sectional Study by Chi Zhou, Fang Tan, Si Hong Lai, Jing Chun Chen, Chao Yi Chen, Gao Feng Zhang and Yin Dong in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We thank all the patients who participated in this study.
Author’s Note
Si Hong Lai is also affiliated to School of Medical Imaging, Hangzhou Medical College, Hangzhou, Zhejiang, China.
Jing Chun Chen is also affiliated to School of Health Medicine, Guangzhou Huashang College, Guangzhou, Guangdong, China.
Abbreviations
PACIC Patient Assessment of Chronic Illness Care
CHPS Compliance of Hypertensive Patients scale
SD Standard Deviation
CCM Chronic Care Model
VIF Variance Inflation Factor
ICC Intraclass Correlation Coefficient
Data Availability Statement
The data can be requested from the corresponding author. All materials used for the purpose of this study are available at the request of the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the MOE (Ministry of Education in China) Project of Humanities and Social Sciences (No: 22YJCZH262), the National Natural Science Foundation of China (No: 72274050), and the 2023 Social Development Science and Technology Program Project of Yuhuan City (No: 202307).
Ethical Considerations
This study was approved by the Ethics Committee of Hangzhou Normal University (No. 2019065, 2022-1118).
Consent to Participate
All study methods were performed in accordance with relevant guidelines and regulations. Before enrollment, each participant was required to provide verbal informed consent.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.