
Abstract
Mental health literacy (MHL) has been widely explored by researchers who focus on youth mental health. However, there is little data related to the validity and reliability of the tools for the assessment of MHL constructs. The present study aimed to adapt the short version of Mental Health Literacy Questionnaire for young adults in Serbian sample and examine its psychometric properties. Translation and adaptation of items were performed using the following procedures: item are translated from English or Serbian by a bilingual translator and using a think-aloud procedure, back-translation, semantic comparison of the translation, and analysis of the translated version by the original version of the manuscript. The sample consisted of 369 participants aged 17 to 47 years, which is in accordance with the recommended number of participants needed for quantitative instrument validation studies. Confirmatory factor, internal consistency, and external validity analyses were performed. The results supported the validity of a shorter version of the questionnaire (MHLq-SVa), composed of 16 items that fit with four previously defined MHL dimensions (knowledge, beliefs, help-seeking intentions, and self-help strategies). Internal consistency, between-factor correlations, and correlations with other relevant mental health constructs further supported the adequacy of the instrument’s psychometric properties. We recommend the MHLq-SVa as valid and reliable measure for assessing MHL in young adults and encourage further exploration at more diverse and representative samples.
Mental health literacy (MHL) has been widely explored by researchers who focus on youth mental health. There is little data related to the validity and reliability of the tools for the assessment of MHL constructs. The results supported the validity of a shorter version of the MHL-YA questionnaire (MHLq-SVa), composed of 16 items that fit with four previously defined MHL dimensions (knowledge, beliefs, help-seeking intentions, and self-help strategies).
Introduction
Mental Health Literacy Questionnaire
The rapid development of scales to assess mental health literacy (MHL) across various groups and ages has made traditional methods like structured interviews and vignettes depicting individuals with mental health disorders outdated. There is now a need for tools that provide an up-to-date and comprehensive view of MHL. Previous MHL questionnaires often focused on specific mental disorders (eg, depression, schizophrenia) rather than covering the broader aspects of MHL relevant to all mental health issues. To address this gap, the Mental Health Literacy Questionnaire (MHLq) was created, reflecting contemporary MHL concepts and offering a more generalized measure.
First introduced in 2018, MHLq was developed from a pre-existing self-report assessment for evaluating MHL in adolescents aged 12–14. 1 Based on Jorm’s (2012) definition of Mental Health Literacy (MHL), the authors conducted a literature review on the components of MHL, assessed various measures for evaluating MHL, and analyzed data collected from multiple student focus groups. 2 This led to a set of items addressing different MHL components. The original version included 33 items across three subscales: first-aid skills and help-seeking, knowledge/stereotypes, and self-help strategies. After a conceptual revision incorporating erroneous beliefs/stereotypes as additional scale, a revised version with 29 items and four factors explained a higher percentage of variance (36.9%). 2 In 2022, Campos et al 3 developed a revised and shorter version of the MHLq-YA, now named the Mental Health Literacy Questionnaire-Short Version for Adults (MHLq-SVa). A shorter version is easier to administer, quicker to score, and less burdensome for participants, compared to the longer version 3 . This version was validated in student samples from six countries: China, India, Indonesia, Portugal, Thailand, and the United States. MHLq-SVa showed good psychometric properties and captured important aspects of MHL in large and diverse young adult samples. These studies contribute to the development of brief and psychometrically sound measures for assessing MHL.
Need for Validation of Mental Health Literacy Questionnaire in Serbia
Recent Serbian mental health screening revealed that the population aged between 18 and 29 years can be considered the most fragile, compared to the other populations. Similar data on young adults’ mental health issues prevalence is found in Western culture.4 -6 Despite robust data on mental health challenges among youth worldwide, scant attention has been paid to understanding the mental health landscape in less developed countries, such as Serbia. A mixed systematic review and narrative synthesis found that low levels of recognition and knowledge about mental health problems and illnesses, pervasive levels of stigma, and low confidence in professional healthcare services were dominant themes among children and young people in low-and middle-income countries. 7 To the best of our knowledge, there is only one study on mental health literacy among young people conducted in Serbia. 8 The results indicate students’ moderate ability to recognize a psychological problem, low perception of the seriousness of the problem, and detection of erroneous beliefs about possible methods of help for mental health problems. 8 Improving mental health literacy (MHL) and increasing access to mental health services are crucial for reducing the incidence of mental health disorders among young people. 9 For instance, enhancing depression literacy has been found to be particularly effective in combating depression. 10 Therefore, it can be inferred that improving MHL may be similarly effective in addressing overall mental health disorders, as it represents “half the battle” in addressing mental health issues.
Concept of Mental Health Literacy
Mental health literacy was first defined as “knowledge and beliefs about mental disorders that aid their recognition, management, or prevention”. 11 This encompassed six key domains: (1) the capacity to identify specific disorders or various forms of psychological distress, (2) understanding of risk factors and causes, (3) knowledge of self-help interventions, (4) awareness of available professional help, (5) fostering attitudes conducive to recognition and appropriate help-seeking, and (6) understanding how to access mental health information. 12 Over time, the focus shifted from assessing “mental disorder literacy” to a more critical approach emphasizing positive mental health outcomes, aligning with the evolving definition of mental health by the World Health Organization in 2019. 13 This expanded perspective includes subjective well-being, optimal functioning, and coping mechanisms, which acknowledge mental health beyond the mere dichotomy of disorders. Attributes of positive mental health literacy now encompass: (1) competence in problem solving and self-actualization, (2) personal satisfaction, (3) autonomy, (4) relatedness and interpersonal relationship skills, (5) self-control, and (6) prosocial attitude. 14 Currently, MHL is mostly defined as a multidimensional construct that unifies four factors: (1) knowledge related to the prevention of mental health problems, (2) recognition of signs and symptoms (ie, being able to identify the onset of problem development), (3) identification of available options and treatments, and (4) knowledge of tailored self-help strategies and first-help skills to support others who are developing and/or present with mental health problem.2,3,15 Recently, the authors noticed that understanding MHL as a multi-construct theory could help delineate between its broad domains: recognition, knowledge, stigma and help-seeking beliefs, and acknowledge their complexity. 16 Spiker and Hammer presented the arguments for considering MHL to be a multi-construct theory, rather than a multi-dimensional construct, for example, that by allowing mental health knowledge, erroneous beliefs/stereotypes, first aid and help-seeking skills and self-help strategies remain as independent constructs, MHL researchers properly acknowledge the well-developed literature that explicate this constructs. 17
Correlates of Mental Health Literacy
Longitudinal and cross-sectional studies have demonstrated the efficacy of school-based interventions in enhancing mental health literacy (MHL) and overall well-being, as evidenced by longitudinal studies 18 and cross-sectional investigations.19 -22 A study by Wei et al found that male and female students exhibited comparable improvements in MHL and general health outcomes, except for help-seeking behaviors. 18 Thai et al reported that Vietnamese high school students with depressive symptoms exhibited significantly lower MHL levels. Also, it was found that mental health knowledge was inversely related to public stigma, while living area, age, education level, family income, and employment status were associated with mental health knowledge and devaluation scores 21 In a sample of Norwegian adolescents, it was revealed that higher MHL levels were associated with better physical and mental health outcomes 19 while Ding et al, 20 reported that among a Chinese sample, low MHL was associated with adverse mental health outcomes, such as depression, anxiety, and poor sleep quality. Mental health problems were found to be differentially related to knowledge and help-seeking behaviors, with American college students experiencing depression exhibiting a lower recognition of depression and reduced help-seeking behaviors. 23
Relevance of Validating Mental Health Measures
Enhancing MHL and promoting anti-stigma awareness represent vital interventions conducive to the identification of mental disorders and facilitation of professional help-seeking behaviors. A crucial step toward formulating interventions tailored to specific contexts and developmental stages is to provide validated measurements that may help to measure improvements in both individual and population mental health outcomes in the future. 24 A systematic review of MHL measures for children and adolescents, 16 as well as for adults25,26revealed conceptual confusion, methodological inconsistency, and a lack of measures developed and psychometrically tested with adolescents. The most commonly assessed domains were mental illness stigma and help-seeking beliefs, with recognition and knowledge of mental illnesses being assessed more frequently than help-seeking knowledge. 16 The mental-ill health approach continues to dominate the field, with few articles assessing the knowledge of mental health promotion.
Research Objectives
The present study aimed to adapt a short version of MHLq-SVa for the Serbian population and examine internal consistency and factor structure of the questionnaire in a sample of Serbian undergraduate and high-school students. Furthermore, external validity was examined, based on correlations with related mental health constructs (mental health issues, emotional regulation, well-being, self-stigma, and self-rated mental health status).
Method
Sample
The study sample included 369 students (66.7% female), aged between 17 and 47 years (M = 20.04; SD = 3.48). Beside the age as the main criteria, every student who was willing to take part in the research and was able to fill in the questionnaire participated in the study. Sample size was determined based on the number of participants and number of items.27,28 We started from a widely accepted ratio of 10 cases per indicator variable in SEM analysis. 29 Among the population of students, 23.8% attended fourth grade of high school (medical/economic school), 73% were undergraduates, and 3.2% were postgraduates at various faculties of the University of Belgrade such as the Faculty of Special Education and Rehabilitation, Faculty of Philosophy, Law Faculty, Faculty of Mechanical Engineering, among others. All participants identified Serbian as their mother tongue, and 98% reported Serbian nationality. More than half of the undergraduates (54,9%) reported that they are not in any romantic relationship, as 47,9% of high school students. Less than one-fifth of all students are working beside studying.
Ethical Considerations
This study was reviewed and approved by the Committee for Assessment of Ethicality in Scientific Research of the Institute for Educational Research in Belgrade, Serbia (No. 163/2023).
Instruments
The sociodemographic section included self-reported questions about gender, age, nationality, and educational status (undergraduate and high school students above 18 years old).
Mental Health Literacy Questionnaire – short version for adults (MHLq-SVa). 3 The shorter version with 16 items has been provided recently based on Mental Health Literacy Questionnaire for young adults (MHLq-ya) 2 organized on a five-point Likert-type scale ranging from 1 = strongly disagree to 5 = strongly agree, following the four-factor structure: Knowledge of mental health problems (six items; eg, “A person with schizophrenia may see and hear things that nobody else sees and hears.”); Erroneous beliefs/stereotypes (3 items; eg, “Only adults have mental disorders.”); Help-seeking and first aid skills (3 items; eg, “If I had a mental disorder, I would seek for a psychiatrist’s help”); and Self-help strategies (4 items; eg, “Physical exercise contributes to a good mental health”). The erroneous beliefs/stereotypes scale was reverse-scored from higher to lower values. The MHLq-SVa is a recommended as a valid and reliable tool for assessing mental health in different cultures. 3 In the process of translation and adaptation of the MHLq-SVa questionnaire to Serbian, the recommended procedure from the instrument’s authors was strictly followed: (1) translation from English by a bilingual translator; think-aloud procedure (n = 4); back-translation by a different bilingual translator; semantic comparison of the translation (n = 4); (4) analysis of the translated version by the Portuguese research team.
Depression Anxiety Stress Scale (DASS-21 30 ; Serbian version 31 ) is a 21-item measure typically used to assess symptoms of depression, anxiety, and stress in both clinical and non-clinical settings. Participants were instructed to rate the presence of symptoms they experienced during the past 2 weeks using a 4-point response scale ranging from 0–did not apply to me at all/never to 3–applied to me very much or most of the time/always. Higher scores indicated greater depression, anxiety, and stress. The DASS-21 is a fully validated and commonly used instrument designed for the assessment of stress (eg, “I found it hard to wind down”), depressive symptoms (eg, “I felt that life was meaningless”), and anxiety (eg, “I experienced trembling [eg, in the hands]”) with good psychometric properties including strong reliability and validity. 32 The descriptive and internal consistency coefficients for all subscales are presented in Table 1.
Sample Sizes, Empirical Ranges, Means, Standard Deviations, Skewnesses, Kurtosises, and Cronbah’s Alpha Statistics: DASS21, ERQ, SSMIS-SF, SSSWB and SRMHS.
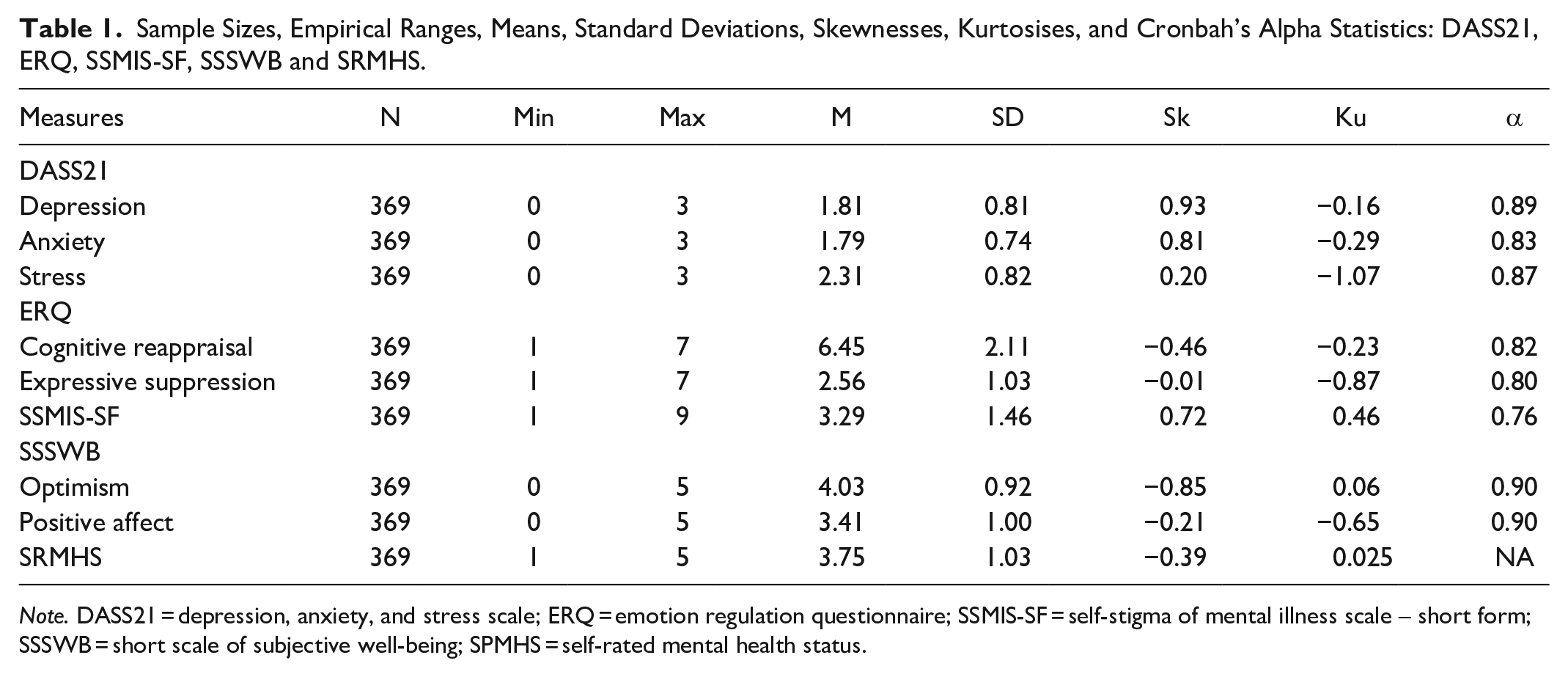
Note. DASS21 = depression, anxiety, and stress scale; ERQ = emotion regulation questionnaire; SSMIS-SF = self-stigma of mental illness scale – short form; SSSWB = short scale of subjective well-being; SPMHS = self-rated mental health status.
Emotion Regulation Questionnaire (ERQ, 33 Serbian version 34 ). The ERQ consists of 10 items capturing personal tendencies to reappraise and suppress the expression of emotions. They indicated their agreement or disagreement on a rating scale ranging from one (strongly disagree) to seven (strongly agree). The ERQ assesses two different emotion regulation strategies: Cognitive reappraisal (eg, “When I’m faced with a stressful situation, I make myself think about it in a way that helps me stay calm”), with 4 items and Expressive suppression (eg, “I keep my emotions to myself”), with 6 items. A higher score implied a higher use of strategy. The ERQ is considered to have good psychometric properties and is recommended for use in young adult populations. 35 The descriptive and internal consistency coefficients for all subscales are presented in Table 1.
Self-Stigma of Mental Illness Scale Short Form (SSMIS-SF 36 ) was used to assess personal stigma toward people with mental health issues. This scale consists of five items describing people with mental health illnesses (eg, “I think that most persons with mental health illness are unpredictable”). Participants answered on a nine-point Likert-type scale ranging from 1 (strongly disagree) to 9 (strongly agree). Higher scores indicated greater personal stigma. Research results in previous studies have demonstrated high SSMIS-SF reliability. 37 Descriptive and internal consistency coefficients are listed in Table 1.
The Short Scale of Subjective Well-being (SSSWB 38 ) was used to assess subjective well-being. The scale is consisted of 8 items, four items measuring personal experiences of positive emotions (eg, “I feel great”) and four items measuring optimistic view of life (eg, “All in all, life is beautiful”) organized on a five-point Likert-type scale ranging from 0 – strongly disagree to 5 - strongly agree. Higher scores indicated greater positive affect and optimism. The internal consistency, analyzed using Cronbach’s alpha, was found to be high. 39 The descriptive and internal consistency coefficients for all the subscales are presented in Table 1.
Self-rated mental health status was assessed using the following item: “In general, how would you rate your mental health?” The students responded on a five-point Likert-type scale, ranging from 1 (very poor) to 5 (very good). This item has been previously found to be satisfactory for use in relation to well-known mental health measures. 40 The descriptions of this item are presented in Table 1.
Procedure
Data was collected from November to December 2023. Information about the research project was provided to students and informed consent was obtained from them as well as from high school principals. All participants were required to complete an online questionnaire through the SoSci survey platform. 41 Upon completion of the questionnaire, participants were provided with a debriefing in the form of a carefully crafted text, authored by the researchers. This text encompassed topics such as the significance of mental health among young individuals, the necessity of monitoring their mental state, and the recognition of potential indicators of psychopathology. Additionally, the debriefing included referral information and suggested readings for further exploration.
Data Analysis
Descriptive statistics (mean values, standard deviation, skewness, and kurtosis) of MHLq-SVa were calculated. Based on MHLq-YA 1 study and MHLq-SVa validation studies in China, India, Indonesia, Portugal, Thailand, and the United States, 3 we conducted confirmatory factor analysis (CFA) on the original structure using the JASP software (JASP, Version, 0.17.2, University of Amsterdam, The Netherlands). We utilized the weighted least squares (WLS) estimation method for CFA analyses, which has been found to have strong convergence properties and provides accurate recovery of population parameters even when the model is large and the sample size is small. 42 Samples with a size of N ≥ 300 are likely to ensure proper convergence of the robust WLS estimator, accurate recovery of factor loadings and covariance, and other benefits. 42 Moreover, the robust WLS estimator is recommended when data are not normally distributed. 43 In line with the theoretical suggestions and previous CFA studies on diverse cultural samples, 3 we assessed the goodness of fit of models using several global indexes: Chi-square (χ2), Tucker–Lewis index (TLI), Comparative Fit Index (CFI), Root Mean Squared Error of Approximation (RMSEA), and Standardized Root Mean Square Residual (SRMR). Chi-square (χ2) tends to increase with larger sample sizes, making it less reliable. 44 Acceptable model fit is indicated by CFI and TLI values of 0.90 or higher, while values of 0.95 or higher suggest good model fit. 45 RMSEA values of 0.08 or less indicate acceptable model fit, while values of 0.05 or less indicate good model fit. RMSEA values ranging from 0.05 to 0.10 suggest fair fit, and values above 0.10 indicate poor fit. 45 Internal consistency was evaluated using Cronbach’s Alpha and the Pearson correlation among subscales, conducted through SPSS (version 29).
Results
Descriptive Statistics
In Appendices, descriptive statistical measures of all MHLq-SVa items are presented (Appendix 1) along with the scoring procedure as well as all items in Serbian language (Appendix 3). The average score for the 16 items is 4.26 (SD = 0.44); for the Knowledge of mental health problems factor 4.17 (SD = 0.57); for the Erroneous beliefs/stereotypes factor 4.56 (SD = 0.55); for the Help-seeking behavior and first aid skills 4.18 (SD = 0.98) and for the Self-help strategies factor 4.21 (SD = 0.68). All four factors are correlated with MHLq-SVa total scale (from 0.45 for Erroneous beliefs/stereotypes factor to 0.77 for Knowledge of mental health problems factor). The correlations between dimensions range between 0.17 (first with third factor) to 0.39 (first with fourth factor), except for the second with third and fourth factor. Cronbach’s Alpha values indicate reliability that can be considered as acceptable to good: for the total score (16 items) = 0.76; Factor 1, Knowledge of mental health problems (6 items) = 0.70; Factor 2, First aid skills and help-seeking behavior (3 items) = 0.82; Factor 3, Erroneous beliefs/stereotypes (3 items) = 0.55; and Factor 4, Self-help strategies (4 items) = 0.74. Factor 3 recorded the lowest reliability among the factors examined. The item intercorrelation analysis ranged between 0.29 and 0.32, and the removal of the items resulted in a decrease in Alpha value (from 0.43 to 0.46). Descriptive statistics, reliability and factor intercorrelations are presented in Table 2.
Means, Standard Deviations, Crombach’s Alpha and Pearson’s Correlations Among MHLq-SVa Dimensions and Total Score.

p < .05. **p < .01.
Confirmatory factor analysis of the MHLq-SVa. Mental Health Literacy questionnaire- Short Version for adults (MHLq-SVa), fit well to the Serbian data (χ2 (98, p < .001) = 351.60; CFI = 0.98; TLI = 0.97; RMSEA = 0.084). The standardized factor loadings ranged from 0.517 (item 11) to 0.960 (item 16). R2 values were globally good (above 0.30). The results of CFA are presented in Appendix 2.
External Validity
correlations between the MHLQ-SVa dimension and other mental health self-assessment measures are presented in Table 3. The correlation analysis supported the convergent validity of the MHLq-SVa, with relationships among constructs in the expected direction. The total score for MHLq-SVa showed significant, albeit weak, correlations with Depression, Cognitive reappraisal, Expressive suppression, Self-stigma of mental illness, Optimism, and Positive affect. Knowledge of mental health problems was positively and weakly correlated with Anxiety and Cognitive reappraisal. Erroneous beliefs/stereotypes correlate negatively with the Self-stigma of mental illness and Self-rated mental health status. The help-seeking and first-aid skills dimensions are negatively related to Depression and Expressive suppression, and positively associated with Cognitive reappraisal, Optimism, Positive affect, and Self-rated mental health status. Lastly, the Self-help dimension was negatively and weakly correlated with Depression, Anxiety, and Stress, and positively correlated with Cognitive reappraisal, Optimism, Positive affect, and Self-rated mental health status.
Correlations Between MHLq-SVa Dimensions and Total Score with DASS-21, ERQ, SSMIS-SF, SSSWB Scores and SRMHS.

Legend. KM = knowledge of mental health problems; EB = erroneous beliefs/stereotypes; HS = help-seeking and first aid skills; SH = self-help strategies; MHLq–SVa = mental health literacy questionnaire short version total score; DASS21 = depression, anxiety, and stress scale; ERQ = emotion regulation questionnaire; SSMIS-SF = self-stigma of mental illness scale – short form; SSSWB = short scale of subjective well-being; SRMHS = self-rated mental health status.
p < .05. **p < .01.
Discussion
The main objective of this study was to provide psychometric properties of the shorter version of the MHLq-YA (MHLq-SVa) in the Serbian sample. The previously obtained results for the four-factor structure of MHLq-SVa were confirmed. 3
Our study found that Serbian young adults generally possess a high level of mental health literacy. Although the result is consistent with previous multicultural assessments 3 , we expected a lower level of mental health literacy considering data about the prevalence of mental health issues among Serbian youth. 46 It’s possible that some factors, other than those we had explored might explain a high level of mental health literacy, for example, economic/political insecurity.47 -49 Mental health literacy was found to be linked with significant mental health variables in a predictable manner. Specifically, participants who reported lower mental health literacy also reported higher rates of depression, self-stigma, and emotional regulation strategies that involve lower use of cognitive reappraisal and higher use of expressive suppression strategy. Conversely, those who reported higher mental health literacy demonstrated lower self-stigma, greater optimism, and positive emotions. Interestingly, the relationship between mental health literacy and self-rated mental health status is only partially consistent in an expected way.
The study’s findings support the four-factor structure of the MHLq-SVa, aligning with the multifaceted view of MHL. 15 Data from the presented study are in line with previous research where a shortened version of MHLq-YA (MHLq-SVa) was tested with the data from six countries (US, China, Thailand, India, Indonesia, Portugal). 3 Confirmatory factor analysis demonstrated that the MHLq-SVa form has a 4-dimensional factorial structure, which indicates strong construct validity for the instrument. Internal consistency, assessed with Cronbach’s Alpha, showed acceptable to good reliability scores for four of the questionnaire’s dimensions and global score. The intercorrelations among factors and the overall MHLq-SVa score confirmed the scale’s consistency.
Factor 1: Knowledge of mental health problems
Participants who reported poor knowledge of mental health problems surprisingly perceived their mental health status to be better. This could be the consequence of a lack of education about mental health problems – if we think we know enough we believe we don’t need additional education. In collectivistic societies, as Serbian society traditionally is, people are usually relying on family, and friends support network in the case of mental health issues. 47 Our data about the unexpectedly positive relationship between knowledge of mental health problems and reporting anxiety might be explained by the high tendency of anxious people to seek information. 50 Another explanation might involve seeking information about mental health problems after noticing some negative changes in personal mental health status. The use of the internet to find mental health information among the student population is increasing, and the population with some mental health problems is using it twice as much as the general population. 51 Adaptive emotional regulation strategies are commonly found to be related to mental health literacy and other mental health outcomes as revealed in the present study. 52 Participants who use cognitive reappraisal more frequently, showed higher levels of knowledge related to mental health problems. Informing ourselves about mental health issues might be considered as an adaptive strategy in situations of increased anxiety related to mental health.
Factor 2: First aid skills and help-seeking behavior
The highest reliability is shown in help-seeking and first aid skills, similar to previous data on culturally diverse samples except Portugal. 3 Participants who reported more help-seeking and first aid skills and better self-help strategies had a more positive self-perception of their mental health status and showed lower levels of depression. It is possible that those who are better informed about help strategies are using them more frequently and therefore, their mental health benefits. It was previously shown that depressed Serbian young adults reported poorer first aid skills and less frequent help-seeking behaviors. 8 Young people are less likely to seek help if they experience depressive symptoms. 53 Low cognitive capacities (concentration difficulties, thinking speed, memory, problem-solving) along with the prevalence of the symptoms of mental health problems might interfere with low help-seeking in a way that additionally affects mood problems.53,54
Results support the significance of emotional regulation strategies for the concept of MHL, meaning that high emotional expressiveness is related to help-seeking behavior of young people. 55 Negative attitudes toward help-seeking from mental health professionals and related self-stigma are connected to the social context within a culture that has a tradition of collectivism 55 as Serbian culture still is. Social stigma is recognized as one of the main barriers to help-seeking, along with a lack of knowledge about mental health problems, poor availability of mental health services and other resources, and a lack of trust in mental health professionals. 56 Our findings indicate that individuals who reported higher levels of well-being also reported more frequent help-seeking and better first-aid skills. This is in line with previous studies, which showed a positive correlation between well-being and general help-seeking behaviors, as well as between well-being and help-seeking specifically related to suicidal ideation. 57 It is also shown that young people who perceive themselves as happier, are also more willing to seek help and have better first aid skills. 19 However, additional education about mental health and encouragement to talk about it should be part of high-school educational and college programs. Pupils and students could benefit from these changes and stigma could also be reduced.
Factor 3: Erroneous beliefs/stereotypes
The weakest reliability pertains to the erroneous beliefs/stereotypes factor, consistent with previous findings in the Chinese sample of a multicultural study. 3 Besides a small number of items (3 items), possible explanations might be the differences in the stereotype domains within erroneous beliefs/stereotypes factor (eg, item 6 “Only adults have mental disorders” differs from item 5 “Mental disorders don’t affect people’s feelings”). The correlation between erroneous beliefs/stereotypes and other mental health literacy factors is weak, except for a significant correlation between knowledge of mental health problems and the total score of MHLq-SVa, similar to what was found in the Indian sample in the multicultural study. 3 Since erroneous beliefs/stereotypes and knowledge of mental health problems were initially presented together within the same factor, the correlation between those factors in this version of the scale is expected. 1 As more students in the present study had mental health stereotypes, they more positively self-rated mental health, which might be related to some “positive illusions” 58 of Serbian youth, who are in general too optimistic about their own future. 59
Factor 4: Self-help strategies
As was the case in the USA, India, and Thailand samples, the Self-help strategies factor yielded good reliability in our sample as well. The research results support the findings from the literature regarding the lower prevalence of mental disorders in the population with high MHL.20,21,23 These results are also in line with previous studies on the relationship between mental health problems and domains of MHL. 23 More depressed Serbian young adults reported poorer self-help strategies and poorer MHLq total scores, while more stressed and anxious students had poorer self-help strategies. Developing mental health problems (depression, stress, and anxiety) worsens the recognition of the mentioned strategies as helpful. Prevalence of the symptoms of mental health problems might interfere with MHL in a way that is empowering mood problems.53,54 As noted in previous studies, 19 young people who are more optimistic about their future and perceive themselves as happier, also have self-help strategies. Serbian youth are generally more optimistic about their own future, relying on their own resources, close family and friend social networks, and taking a lot of personal responsibility in the lack of wider social and structural support. 59 However, teaching students about the recognition of mental health issues, symptoms, and adaptive self-help strategies within the educational system could improve their mental health literacy and reduce not only mental health issues but also stigma.
How good are we at assessing our MHL?
Although young adults in the present study reported a high level of MHL (at all examined dimensions), the number of those who self-rated mental health problems in the present study is not negligible. Unexpected relation between the better self-rated mental health status on the one side and poor knowledge of mental health problems and greater erroneous beliefs/stereotypes on the other side raises concerns about the accuracy of young adults’ self-assessment of their mental well-being. The discrepancy between the desired and actual quality of life may contribute to the challenges faced by Serbian youth, who prioritize material possessions yet feel limited in their ability to control their life. 60 . Encouraging a shift toward emotional problem-solving and addressing the underlying social and economic factors that influence their sense of control is crucial for promoting mental well-being among Serbian youth.
Conclusion
In order to explore MHL in different countries and different age groups, developing adequate tools is crucial. Validation of MHL instruments is also the first step toward expanding this research field in Serbia and other Balkan countries. Involving constructs other than those we did in this study for external validation may reveal stronger relationships and relevance is highly recommended. Future studies should expand exploration of psychometric properties of the MHLq-SVa within representative samples of the adult population. Our sample included only university level students and among them there were future psychologists and special educators, who are probably more familiar with mental health literacy concepts. An additional sample limitation is related to the participant’ sex - three quarters of participants were female, which disabled additional analysis and group comparisons. Data considering knowing someone with mental health problems (families/relatives/friends/themselves) were reported by participants and rely on their own assessment of disorder presence. However, those estimations are not reliable so results related to these questions should be interpreted with caution. Although Self-Stigma of Mental Illness Scale Short Form
Footnotes
Appendices
MHLq-SVa – Items in Serbian.

| 1. Fizička aktivnost doprinosi dobrom mentalnom zdravlju. |
| 2. Mentalni poremećaji ne utiču na ponašanje ljudi. |
| 3. Dobar san doprinosi dobrom mentalnom zdravlju. |
| 4. Da imam poremećaj mentalnog zdravlja potražio/la bih pomoć psihologa. |
| 5. Mentalni poremećaji ne utiču na osećanja ljudi. |
| 6. Samo odrasli imaju mentalne poremećaje. |
| 7. Promene u funkcionisanju mozga mogu dovesti do pojave mentalnih poremećaja. |
| 8. Da neko ko mi je blizak ima poremećaj mentalnog zdravlja, ohrabrio/la bih ga da poseti psihijatra. |
| 9. Balansirana ishrana doprinosi dobrom mentalnom zdravlju. |
| 10. Jedan od simptoma depresije je i gubitak interesovanja ili uživanja u većini stvari. |
| 11. Trajanje simptoma je jedan od važnih kriterijuma za dijagnostikovanje mentalnih poremećaja. |
| 12. Mentalni proremećaji utiču na misli ljudi. |
| 13. Bavljenje stvarima u kojima uživamo doprinosi dobrom mentalnom zdravlju. |
| 14. Osoba sa shizofrenijom može videti ili čuti stvari koje niko drugi ne vidi i ne čuje. |
| 15. Izuzetno stresne situacije mogu da dovedu do mentalnih poremećaja. |
| 16. Da imam poremećaj mentalnog zdravlja, potražio/la bih pomoć psihijatra. |
Correction (February 2025):
The article has been updated with the correct sample description in the Methods section
Authors Contribution
MKL: Conceptualization, Methodology, Investigation; Data Curation; Formal analysis, Writing - Original Draft, Writing - Review & Editing, Project Management; AR: Conceptualization, Methodology, Formal analysis, Writing - Review & Editing; MT: Conceptualization, Resources, Data Curation, Investigation, Writing - Review & Editing; LM: Investigation, Project Management, Resources; IM: Conceptualization, Resources, Investigation, Data Curation, Writing - Review & Editing.
Data Access Statement
The data that support the findings of this study are available on request from the corresponding author.
Missing Data Access Statement
All relevant data are within the paper and its Supporting Information files.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Ministry of Science, Technological Development and Innovation of the Republic of Serbia (Contract No. 451-03-66/2024-03/ 200018). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Ethics Statement
This study was reviewed and approved by the Committee for Assessment of Ethicality in Scientific Research of the Institute for Educational Research in Belgrade, Serbia (No. 163/2023).
Consent
Authors declare that they agree with the final version of the manuscript being submitted to INQUIRY