
Abstract
Although highly related, mental illness may not fully determine perceived well-being, a distinction captured by dual-continuum models. Separating mental illness and well-being into related but separate constructs prompted investigation into potential buffers to reduce the impact of mental illness on perceived well-being. This study explored two such buffers in health literacy and psychological resilience among Australian men. Using the Ten to Men Australian Longitudinal Study on Male Health, this secondary data analysis of n = 8,408 men between 18 and 60 years of age assessed the moderating effect of three components of health literacy (feeling supported by health care providers, ability to find health information, and active engagement with health care providers) and psychological resilience on the relationship between mental illness and well-being. Mental illness symptoms were negatively associated with well-being, whereas psychological resilience, active engagement with health care, and health care provider support (β res = .65, β eng = .28, and β sup = .25) had positive significant relationships with the outcome (all p ≤ .001). Ability to find health information (p = .25) and psychological resilience (p = .43) were not significantly associated with well-being. Of the four interactions tested, health literacy relating to health care worker support was the only significant moderator between mental illness and well-being (β sup = .03). This study identified that meaningful support and understanding from health care providers for Australian men aged between 18 and 60 years may somewhat ameliorate the impact of mental illness on well-being. Further related investigation may reveal specific interventions that improve perceptions of support among men.
Introduction
While paradoxically reporting lower levels of distress (Australian Institute of Health and Welfare, 2022), Australian males are three times more likely to complete suicide than their female counterparts (Australian Bureau of Statistics, 2021). Approximately, 18% of males will experience a common mental illness annually, accumulating to 43% over their lifetime (Australian Bureau of Statistics, 2022). The magnitude of the challenge for Australian males may also be larger than reported due to males being less likely to identify indicated symptoms of mental disorders, or feel safe in reporting their mental health challenges (Affleck et al., 2018).
Unsurprisingly, the propensity to seek care through formal services, in men, remains comparatively much lower than their female counterparts, despite targeted intervention (Harris et al., 2015). Although reporting comparable levels of lifetime mental disorders, Australian men also use Medicare (socialized health care system)-subsidized mental health services at half the rate of Australian women (36 per 100 vs. 70 per 100; Australian Institute of Health and Welfare, 2023). Given similar rates of mental disorders and the proportionally lower service utilization, a better understanding of what factors may reduce the impact of mental illness on well-being for men is needed.
Well-being relates to the subjective experience of life through cognitive reflection (e.g., life satisfaction) and emotional responses (Diener et al., 2018). A conceptually nebulous area of study, subjective well-being is often defined through interrogating satisfaction across multiple life domains, as is the case with the personal well-being index (PWI) used in this study (International Wellbeing Group, 2013). We consider well-being to be a proximal outcome of mental illness and an important mediator to numerous downstream consequences. Therefore, the ability to modify the relationship between mental illness and well-being may an important avenue of investigation to reduce the impact of mental illness among Australian men.
Accordingly, we investigated whether psychological resilience (as measured by the Connor–Davison Resilience Scale [CD-RISC]; Connor & Davidson, 2003) and health literacy (as measured by three dimensions of the Health Literacy Questionnaire; Osborne et al., 2013) can mitigate the impact of mental illness on the psychological well-being of Australian men. These constructs may offer additional points of intervention for men experiencing symptoms of mental illness.
Disambiguating Mental Health and Well-Being
Increased well-being has been associated with numerous positive health and social outcomes, including for education (Murray et al., 2007), interpersonal relationships and social interactions (Moore & Diener, 2019; Ohrnberger et al., 2017), and physical health and activity (Ohrnberger et al., 2017). Traditionally, mental illness and well-being have been viewed as having an inverse relationship, as if they are opposite ends of the same continuum (Chan & Weich, 2020), or have been otherwise conflated (Jackson & Haslam, 2022). This defined mental illness by the symptoms experienced with psychopathologies (Westerhof & Keyes, 2010), and mental health as the absence of those symptoms. However, contemporary thinking on mental health and illness has disambiguated these constructs into two related but distinct constructs (Oswald et al., 2021; Westerhof & Keyes, 2010).
Whereas mental illness remains defined by symptoms of psychopathologies, mental health, or well-being, is a broad concept often defined by positive functioning (eudaemonia) and feelings of satisfaction, happiness, and engagement (hedonia; Ryan & Deci, 2001). By distinguishing between these concepts, it is therefore possible for an individual to occupy the high end of the spectrum for both mental illness and well-being, although the proportion of people meeting both of these characteristics is low and estimated at approximately 1.5% of the population (Keyes, 2007). While the shared variance between mental health and mental illness is substantial at 25% (Keyes et al., 2010), the factors associated with each also differ (Keyes et al., 2010; Westerhof & Keyes, 2010).
Both lower well-being and mental illness are associated with physical disease, health care usage, work productivity, and psychosocial functioning (Westerhof & Keyes, 2010). People with symptoms of mental illness but higher well-being exhibit better functioning than those with lower well-being (Westerhof & Keyes, 2010). This suggests that the effect of mental illness on well-being can be moderated to improve the overall functionality of those experiencing mental illness.
Potential Modifiers Between Mental Illness and Perceptions of Well-Being
Two potential moderators of mental illness on well-being include health literacy and psychological resilience. There are many ways to define health literacy, with a notable evolution of definitions over the past three decades (Smith & Ireland, 2020). Historically, health literacy has been concerned with the “cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand and use information in ways which promote and maintain good health” (Nutbeam, 1998: 29). However, more contemporary definitions have reinforced that health literacy is both an individual endeavor (i.e., focused on improving individual health behaviors; Milner et al., 2019; Waldmann et al., 2020) and a population endeavor (i.e., focused on improving population health outcomes; Smith & Ireland, 2020). Within the latter discourse, there has been a focus on improving health settings and systems to better meet the health needs of the individuals, families, and communities. This aligns with men’s health scholarship, particularly that relating to men’s help-seeking, where scholars have argued that men will seek help if provided with the right environment in which to do so (Smith et al., 2008b). This extends to men’s mental help-seeking contexts as well (Kwon et al., 2023; Seidler et al., 2017, 2020b). Importantly, improved health literacy has been reported to facilitate help-seeking among individuals with mental illness (Milner et al., 2019; Waldmann et al., 2020) and is linked with increased well-being in diverse populations (i.e., across national and socioeconomic boundaries; Kwon et al., 2023; Weishaar et al., 2019). Symptoms of mental illness have previously been associated with lower levels of health literacy in the same cohort of Australian men (Milner et al., 2019). That same study identified that higher levels of masculine norms among men was associated with lower levels of health literacy (Milner et al., 2019), offering further insight into how health literacy may be formed, bolstered, or reinforced.
While definitions of psychological resilience vary across disciplines and population groups, there is broad agreement that it relates to an ability to adapt or thrive under adverse life conditions (Sisto et al., 2019). Psychological resilience is also associated with having fewer mental illness symptoms and greater mental well-being (de Vries et al., 2021; Perlman et al., 2018). Resilience has been purported to mitigate threats to well-being through protective adaptive systems (Masten & Obradović, 2006; Yalcin-Siedentopf et al., 2021), yet men may have different stress, resilience, and coping patterns. The relationship between social support and stress, for example, has been shown to be fully mediated by resilience in men, indicating that the ability for social support to reduce perceptions of stress in men is through the development of resilience. This highlights the potential importance of resilience to the appraisal of (dis)stress in men. Resilience also acts as a buffer of well-being for men across multiple antecedents (Yalcin-Siedentopf et al., 2021) and presents as a reasonable candidate for buffering the impacts of mental illness.
Few known studies to date have explored the ability for health literacy and resilience to act as buffers between mental illness and well-being. As such, we investigated whether three components of health literacy and psychological resilience attenuated the relationship between symptoms of mental illness and well-being in Australian men (ages 18–55+ years) using the existing Ten to Men longitudinal study data source (Pirkis et al., 2016).
Method
Data
Ten To Men, a longitudinal study of men aged 10 to 55 years, was initiated by the 2010 National Male Health Policy (Australian Government Department of Health and Aged Care, 2021) in response to a recommendation to build a strong evidence base on male health to inform policies, programs, and initiatives (Australian Government Department of Health and Aged Care, 2021; Pirkis et al., 2016). Ten to Men was designed to capture a national epidemiological perspective of male health and well-being across the spectrum of health and social factors. As of 2022, three waves of data have been collected. More specifically, the aims of the Ten to Men study are to
Examine key determinants of mental health in Australian men, including social, economic, environmental and behavioral factors that affect the length and quality of life;
Address key research gaps about the health of Australian men, including health and risk behavior in life, while accounting for social, economic, and environmental changes; and
Identify policy opportunities for improving the health and well-being of Australian men and providing support for men at key life stages, particularly those at risk of poor health.
Recruitment and Sample
Recruitment to the Ten to Men study began in 2013, with the intention of obtaining a nationally representative sample of 20,000 participants who would be followed up approximately 2 to 3 years later (“Ten To Men Technical Report # 4,” 2015). We focused on n = 10,767 adult responses to Wave 2 (described further –https://tentomen.org.au/sites/default/files/ttmw2_adults.pdf (Australian Institute of Family Studies, 2021)), which was collected over a period of approximately 7 months during 2015–2016 (Bandara et al., 2021).
Variables
Outcome
The outcome variable for this analysis was well-being as measured by the PWI (International Wellbeing Group, 2013). The PWI is measured on a 0 to 10 scale across seven questions related to specific life domains, including standard of living, health, achievement, personal relationships, belonging in community, and future security. A score on a 0 to 100 scale, as is used within this study, is accomplished through a proportional conversion (International Wellbeing Group, 2013) of the 0 to 70 score inherent to the scale (i.e., seven questions, 0–10).
Main Independent Variable
The main independent variable representing symptoms of psychological illness was the Patient Health Questionnaire (PHQ-9), which can be used as a diagnostic screening tool for depression or as a linear or categorical assessment of depression severity (Kroenke et al., 2001). In this study, we employed the PHQ-9 as a linear measure of depression severity with a scale from 0 to 27 across nine items.
Moderators
Psychological resilience was measured by the short-form version of the CD-RISC 10 (Connor & Davidson, 2003), which was considered unidimensional. This version uses 10 items and has a scale range between 0 and 40.
Health literacy was measured using three domains of the Health Literacy Questionnaire (Osborne et al., 2013). These three domains were as follows: feeling understood and supported by health care providers (health literacy support), feeling able to actively engage with health care providers (health literacy engagement), and feeling able to find good health information (health literacy information). Health literacy support had four items with a 4-point response, rendering a total scale of 0 to 16. Health literacy engagement and health literacy information each had five items with a 5-point response, rendering a total scale of 0 to 25.
Controls
Control variables include age, relationship status, household income, decile of socio economic advantage—as measured by Socio-Economic Indexes for Areas (SEIFA; Australian Bureau of Statistics, 2018), employment status, level of education, psychologist attendance over the preceding 12 months, living with a disability, and a diagnosis of depression or anxiety over the lifetime. Further information of these variables is available in Table 1.
Descriptive Statistics for Included Variables

Note. PWI = personal well-being index; PHQ-9 = Patient Health Questionnaire-9.
Ethics and Informed Consent
Human ethics approval for this analysis of secondary data was received through the Human Research Ethics Committee of the Northern Territory Department of Health and Menzies School of Health Research—HREC Reference Number: 2022-4269. Implied informed consent (following explicit consent in Wave 1) was obtained during the initial data collection after providing participants with information on how the data will be used, noting, “Data from the study is used by researchers and policy makers to improve our understanding of men’s health in Australia, and to inform government policies and programs related to men’s health.”
Analysis
Only participants with complete information across the independent and outcomes variables were included in the analysis. All statistical analyses were conducted using R Statistical software (R Core Team, 2022). First-order correlations were performed between relevant variables to ensure that the pattern of associations was consistent with the expected relationships. Linear regression models were then conducted for the main analyses. A base model was first conducted, which regressed well-being onto the main independent and other variables of interest (moderating variables). This base model was conducted to establish the multivariate relationships between the independent and other variables and the outcome variable. Collinearity was assessed at this stage using variance inflation factor (VIF). Robust standard errors were produced to correct for heteroscedasticity. Following the base model, the possible moderating effects of psychological resilience and health literacy were assessed, using multiplicative interaction terms with the main independent variables.
Results
Total complete cases included in the base regression model were n = 8,408 men aged between 18 and 60 years. Correlations between variables of interest were generally in the expected direction. Mental illness symptoms had a moderate negative relationship with psychological well-being (r = –.62), whereas small to moderate positive relationships were found for both health literacy (r = .16 sup, r = .31 eng, and r = .28 info) and psychological resilience (r = .51) with the outcome (PWI). The PHQ-9 was negatively correlated with health literacy (r = –.10 sup, r = –.28 eng, and r = –.25 info) and psychological resilience (r = –.46).
The base regression models followed similar patterns to the correlations between the variables of interest. Symptoms of mental illness (PHQ-9) had a strong negative association with well-being (β = −1.38, p < .000). Health literacy information was not associated with well-being (β = .10, p = .243); however, both health literacy support and engagement were both positively associated with well-being (β sup = .25, p < .000; β eng = .28, p < .000).
Results From Linear Regression Analysis for Interactions Between Psychological Illness (PHQ-9) and Both Health Literacy and Psychological Resilience
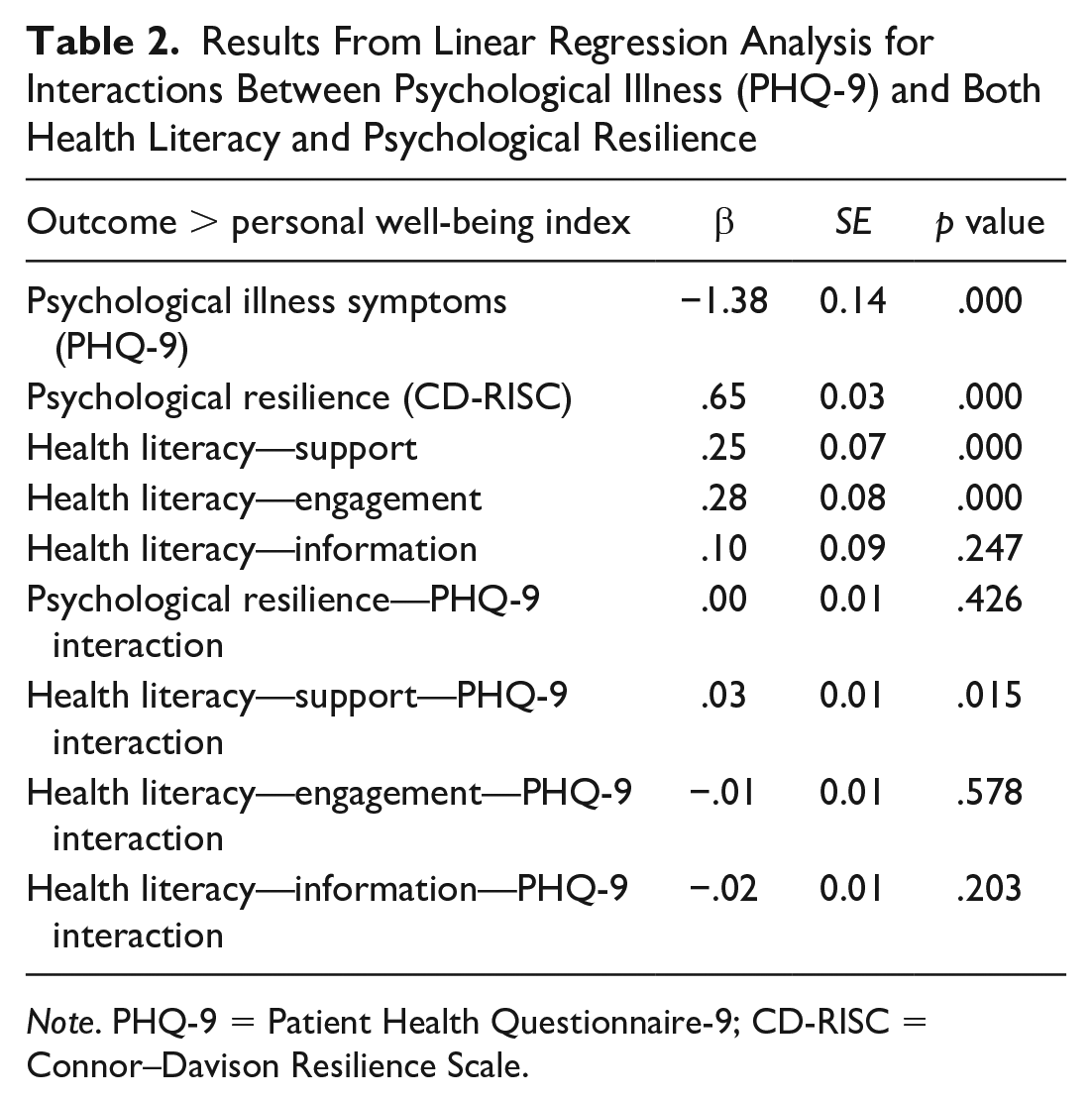
Note. PHQ-9 = Patient Health Questionnaire-9; CD-RISC = Connor–Davison Resilience Scale.
Following the base regression, a model was run to analyze the moderating effects of psychological resilience and health literacy regarding support from health care providers and engagement with health care providers (Table 2). Whereas the main effects of psychological resilience and health literacy remained statistically significant, the only significant moderator of psychological ill-health was health literacy support (β sup = .03, p = .015); in other words, the effect of mental illness on well-being was smaller among those reporting higher levels of perceived support from health care workers (Figure 1). However, the negative effect of mental illness symptoms on well-being (main effect) remained for all levels of health literacy. Figure 2 demonstrates the estimated well-being levels across the spectrum of mental illness for different levels of health literacy regarding perceived social support from health care workers.

Standardized Coefficients for Each Interaction and Main Effect

Mental Illness Symptoms and Well-Being Across Levels of Health Literacy-Support
Discussion
Consistent with previous evidence across a variety of population groups, this study suggests that both psychological resilience (Joyce et al., 2018) and health literacy (Brassington & Lomas, 2021; Brijnath et al., 2016) are relevant intervention targets for increasing well-being among Australian men between the ages of 18 and 55 years, although age-specific interventions targeting those within those ages has been recommended (Brassington & Lomas, 2021; Brijnath et al., 2016). The negative relationship between symptoms of mental illness and well-being was expected and aligns with the dual-continuum view of mental health.
Three components of health literacy and psychological resilience were proposed to moderate the relationship between mental illness and well-being. Of these, only “perceived support and understanding from health care providers” had a statistically significant, albeit small, moderating, meaning higher perceived support reduced the impact of mental illness symptoms on well-being. Notably, this association was independent of whether the participant visited a psychologist in the past 12 months, indicating relationships across various health fields may be important in moderating the impact of mental illness on well-being among Australian men.
The implications of the moderating effect of health care provider support are numerous. The mechanisms of feeling supported by a health care provider for men relate first with access and connection with the mental health care system. Well-established barriers to help-seeking in men relate to stigma, low health literacy, adherence to masculine norms, and low general awareness of symptoms (Milner et al., 2019; Mursa et al., 2022; Rice et al., 2018). This pattern of disengagement commences in adolescence and persists through adulthood (Marcell et al., 2002; Rice et al., 2018). Potential solutions that could be adopted within the broader health care system include increasing health literacy through targeted intervention, promoting progressive forms of masculinity, influencing hegemonic masculine norms, and increasing awareness of male mental health symptomatology and diagnostic indicators among health professionals (Rice et al., 2018). It is likely that these efforts will need to occur in concert as the relationship between masculinities, health literacy, and the impact on well-being is complex and it remains unclear how these factors causally affect one another.
While connecting with health services is a necessary prerequisite, feeling engaged and supported may require additional strategies (Macdonald et al., 2022). Although stigma is often a barrier to entry to health services for men, experiences during visits can also determine subsequent help-seeking behaviors (Marcell et al., 2002; Smith et al., 2008a). Seidler et al. (2020a) found that dissatisfaction with previous therapy negatively affected perceptions of effectiveness in the future, which aligns with previous evidence outlining multiple characteristics that can affect health service engagement (Scholz et al., 2022) and the client–therapist relationship, which include the following: not the right fit or approach; perceived pressure from the counselor or psychotherapist; lack of trust or uncertainty from the client, the counselor, or psychotherapist acting on assumptions about the client; uncertain expectations from the client about the session; clients not providing enough effort; and scheduling and timing problems (Richards & Bedi, 2015).
While the responsibility for addressing these characteristics may not fall wholly on the health care provider or system, improvements may be fundamental to increasing health literacy among men. This study suggests that interventions improving experiences with health care services may have an incremental impact on the ability for men to buffer the impacts of mental illness in relation to their well-being. Building the capacity of the health care systems and increasing health literacy among men are prominent objectives of the National Men’s Health Strategy (Australian Government Department of Health and Aged Care, 2021) and are supported by the findings in this study.
This study undertook a cross-sectional analysis, which is limited in the ability to draw causal inferences (Spector, 2019). The causal direction between well-being and mental illness is represented differently across publications (De Cates, 2015; Keyes et al., 2010) and it is also feasible that this relationship may be recursive. This study took the position that perceived well-being is an outcome of mental health but has not contributed to the evidence surrounding causality. Furthermore, whereas these data are drawn from a longitudinal study with three waves, the temporal separation (or lag) between measurements was more than 12 months and may not accurately reflect the timelines of cause and effect between mental illness symptoms and well-being (Spector, 2019). Sensitivity analyses among key subpopulations within Australia, namely, Aboriginal and Torres Strait Islander men, were not possible due to the limited sample size. Therefore, although the literature would suggest these findings extend to Aboriginal and Torres Strait Islander men, further empirical evidence is required to corroborate these findings.
The PWI aligns largely with the hedonic (emotional well-being) tradition of well-being measurement (Ryan & Deci, 2001). Keyes (2007) proposed a more holistic representation of well-being, which includes both hedonic and eudaemonic well-being (social and psychological well-being) that broadly reflect feelings of well-being and meaningful functioning. However, the distinction between hedonic and eudaemonic well-being may be less important, and similar satisfaction well-being measures show coverage of both forms of well-being (Kashdan et al., 2008). Finally, the data used in this study are susceptible to common biases associated with self-report data (Althubaiti, 2016) and should be considered in interpreting the results.
This study also contains several strengths. The sample is large and focuses on Australian men of varying age and their mental health, an identified priority (Australian Government Department of Health and Aged Care, 2021). This study also identified factors that may mitigate the impact on mental illness of perceived well-being among men, thus providing additional insight into effective strategies for the secondary prevention of mental illness.
Conclusion
Men who feel they receive more support and understanding from health care providers had smaller effects of mental illness on well-being. Interventions targeting interactions with health care providers may provide men with additional tools to buffer the translation of symptoms of mental illness into poorer well-being. This may extend across health fields, providing options for intervention across primary health care and allied health services. Further qualitative research is needed to uncover the characteristics of the interactions between men and their health care provider that lead to perceptions of support, which has been advocated for by scholars for decades (Johnson et al., 2012; Robertson & Williamson, 2005; Smith et al., 2008a) and is a clear objective of the National Men’s Health Strategy (Australian Government Department of Health and Aged Care, 2021).
Footnotes
Acknowledgements
The authors would like to acknowledge the Larrakia people, the people of the Kulin Nation, and Menang Noongar people whose land we live and work on.
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.