
Abstract
To estimate the technical efficiency of health systems toward achieving universal health coverage (UHC) in 191 countries. We applied an output-oriented data envelopment analysis approach to estimate the technical efficiency of the health systems, including the UHC index (a summary measure that captures both service coverage and financial protection) as the output variable and per capita health expenditure, doctors, nurses, and hospital bed density as input variables. We used a Tobit simple-censored regression with bootstrap analysis to observe the socioeconomic and environmental factors associated with efficiency estimates. The global UHC index improved from the 2019 estimates, ranged from 48.4 (Somalia) to 94.8 (Canada), with a mean of 76.9 (std. dev.: ±12.0). Approximately 78.5% (150 of 191) of the studied countries were inefficient (ϕ < 1.0) with respect to using health system resources toward achieving UHC. By improving health system efficiency, low-income, lower-middle-income, upper-middle-income, and high-income countries can improve their UHC indices by 4.6%, 5.5%, 6.8%, and 4.1%, respectively, by using their current resource levels. The percentage of health expenditure spent on primary health care (PHC), governance quality, and the passage of UHC legislation significantly influenced efficiency estimates. Our findings suggests health systems inefficiency toward achieving UHC persists across countries, regardless of their income classifications and WHO regions, as well as indicating that using current level of resources, most countries could boost their progress toward UHC by improving their health system efficiency by increasing investments in PHC, improving health system governance, and where applicable, enacting/implementing UHC legislation.
Maximizing the efficiency of healthcare resources is critical to advancing toward UHC and SDGs for health.
Our study indicates that, while the global UHC index has improved (compared with the 2019 estimates), a vast majority of health systems are inefficient in terms of using their healthcare resources toward achieving UHC. In addition, improving investments in PHC, health system governance, and enacting UHC legislation significantly boosted health system efficiency toward UHC.
It is imperative that policymakers prioritize the enactment and implementation of UHC laws and actively work to raise PHC expenditure. Equally important is effective governance at the local, national, and global levels to enhance health system efficiency in pursuit of UHC objectives.
Introduction
Universal Health Coverage (UHC) is defined as the desired outcome for health systems, where all individuals in need of healthcare services, including promotion, prevention, treatment, rehabilitation, and palliative care, receive them without experiencing excessive financial hardship. 1 Good health is essential for human capital and economic growth. This enables children to attend school and allows adults to participate in the workforce. Financing healthcare services, therefore, is not an expenditure, but an investment in human capital. 2 UHC plays a central role in achieving Sustainable Development Goals (SDG), as health is a prerequisite for sustainable development, an outcome of it, and an indicator of progress in all three dimensions of sustainability.1,3 High-quality health systems that offer universal access protect individuals from illnesses, promote economic growth, combat poverty by maintaining population health, and contribute to social cohesion by ensuring the availability of healthcare services when needed. 4
Health systems refer to a combination of actors, institutions, and resources involved in the financing, regulation, and delivery of activities primarily aimed at improving or preserving health.5,6 These systems bring together labor and capital resources in a production process to generate various healthcare services, including medical, surgical, nursing, dental, pharmaceutical, physiotherapy, counseling, and palliative care, all of which contribute to enhancing health. 7 While the ultimate goal of healthcare services is to bring about a marginal improvement in health status, it can be challenging to measure it accurately in most datasets.6,7 Therefore, intermediate outcomes, such as the number of surgical procedures, antenatal visits, childhood vaccine doses, and similar indicators, have often become the primary focus of research. Health systems demonstrate varying levels of performance, even when they have similar income classifications, education standards, and healthcare expenditures. This divergence in performance affects their ability to achieve critical health objectives.5,8 According to the World Health Organization (WHO), health systems worldwide lose a significant portion of their resources, estimated at 20% to 40%, owing to various forms of inefficiency. 5 For most countries, particularly low- and middle-income countries (LMICs), continuing on this path will not be sufficient to achieve the UHC goal by 2030. 8
Midpoint on the way to 2030, monitoring the progress of health systems toward achieving UHC has become increasingly vital.9,10 The efficiency of health systems is evaluated based on their ability to reach intermediate outcomes and ultimate goals, while making the best use of available resources. These assessments are crucial for shaping and implementing healthcare reforms. 5 Consequently, our objective was to determine the extent to which health systems have achieved UHC, assess the technical efficiency of health systems in striving to achieve the UHC objective, and analyze the factors contributing to differences in efficiency levels. Initially, we used the Joint World Bank and WHO Framework for Monitoring UHC to calculate the UHC index for each of the 191 countries. 11 Subsequently, we employed data envelopment analysis (DEA), a non-parametric method for measuring the efficiency of decision-making units using multiple input-to-output configuration, to estimate the technical efficiency of the health systems.12,13 DEA was chosen because of its widespread use in production frontier analyses, its ability to work with various inputs and outputs, and because it does not require specific functional form assumptions.14,15 Our study findings could potentially facilitate the tracking of health system efficiency trends, improvements over time, and countries’ progress toward achieving UHC.
Methods
Study Design
This was a multi-country, cross-sectional analysis using population-based, national-level data. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, together with Dufault and Klar’s recommendations, were used to ensure appropriate reporting of our study’s design, conduct, and findings.16,17
Study Variables
UHC is generally considered to have 2 key dimensions: service coverage, which ensures that everyone, regardless of their ability to pay, receives the necessary healthcare services; and financial protection, which prevents individuals from experiencing financial hardship due to seeking necessary care.18,19 The UHC index captures and measures both dimensions of the UHC concept to facilitate the tracking of progress, comparison between countries, and guide policy decisions along both dimensions.18,20 Given that policymakers are concerned with both UHC dimensions, service coverage (SC) and financial protection (FP), and are likely willing to make trade-offs between them, the UHC index represents a geometric mean of indicators for these 2 UHC dimensions, presenting an overall score ranging from 0 to 100, with higher scores indicating better performance.18,20,21 Numerous studies have used the UHC index as a target or benchmark to evaluate the efficiency of healthcare systems.5,22-27
Service coverage (SC): refers to “the average coverage of essential services based on tracer interventions that include reproductive, maternal, newborn and child health, infectious diseases, non-communicable diseases and service capacity and access, among the general and the most disadvantaged population.” 28 The index is presented on a unitless scale ranging from 0 to 100, and its calculation involves taking the geometric mean of 14 tracer indicators related to health-service coverage. These indicators are categorized into 4 components: reproductive, maternal, newborn, and child health; infectious diseases; non-communicable diseases; and service capacity and access. 28
Financial Protection (FP): We meticulously adhered to the joint World Bank and WHO Framework, incorporating 2 key measures of out-of-pocket (OOP) health expenditure: catastrophic OOP healthcare spending, defined as surpassing a specific percentage of a household’s total consumption, and impoverishing OOP healthcare spending, signifying that OOP costs push a household below the poverty threshold. 11 While the latter directly tackles the issue of OOP expenses leading to hardship and poverty, catastrophic expenses do not necessarily result in poverty but instead indicate exposure to financial risk. We selected thresholds of 10% of total household consumption for catastrophic health expenditure (CATA) and an international poverty level of $1.90 per day for impoverishing OOP healthcare expenditure (IMPOV).
Health system inputs: We incorporated indicators that capture the inputs associated with healthcare production, including healthcare workforce, capital, and infrastructure. Specifically, we included the average current health expenditure (CHE) per capita, adjusted for purchasing power parity (PPP) over the last 5 years (2016-2020), and the density of physicians, nurses, and hospital beds. We opted for the average CHE per capita, as it provides a more comprehensive assessment, accounting for the time delay that exists in the cause-and-effect relationship between healthcare spending or investments and the generation of intermediate outputs and health outcomes. 29
Other indicators/variables: We incorporated 11 indicators to capture the economic, social, and environmental factors that could influence health systems’ capacity to produce healthcare services. These include: (1) per capita gross domestic product (GDP); (2) government health expenditure as a percentage of CHE (referred to as GOVT); (3) out-of-pocket expenditure as a percentage of CHE (referred to as OOP); (4) external health funding as a percentage of CHE, specifically donor or international aid contributions (referred to as EXT); (5) primary health care (PHC) spending as a percentage of CHE; (6) current health expenditure as a percentage of GDP; (7) the existence of UHC legislation; (8) governance quality encompassing dimensions such as control of corruption, government effectiveness, political stability, absence of violence/terrorism, regulatory quality, rule of law, and voice and accountability; (9) Gini coefficient; (10) educational attainment measured by mean years of schooling; and (11) urbanization. We included CHE as a percentage of GDP to underscore the significance of the health sector within the broader economy, highlighting the societal prioritization of healthcare in monetary terms compared to other sectors. The OOP per capita was included to signify both individuals’ health-spending capacity and their active engagement with healthcare services, reflecting the effective utilization of such services. GDP per capita served as an indicator of income relative to population size, with the rationale being that higher incomes facilitate individuals’ access to healthcare services and enable nations to invest in advanced healthcare technologies. 30 In this context, the term “governance pertains to a country’s performance across various governance dimensions: control of corruption, government effectiveness, political stability, absence of violence/terrorism, regulatory quality, rule of law, and voice and accountability. 31 We employ this as a proxy to evaluate the effectiveness of the health system’s governance. Furthermore, we integrated the mean years of schooling as a gage of educational achievement, hypothesizing that a higher average number of years of schooling would have a positive influence on healthcare accessibility. 30 Finally, the inclusion of urbanization as an indicator considered its role in facilitating access to healthcare services and its reflection on the proportion of the population with access to basic living conditions. 32
Data Sources
We examined 3 distinct sets of variables for each country: (1) direct inputs of the health system, (2) health system output, which in this study are indicators for estimating the UHC index, and (3) contextual factors affecting the efficiency of the health system. Thus, we used the WHO’s Global Health Observatory (GHO) and World Bank’s Health Equity and Financial Protection Indicators data for the components of the UHC index.28,33 Data for the main UHC dimensions were derived from various surveys conducted in different years, and 2021 was chosen as the index year. When 2021 data were not available, we used estimates from the nearest preceding or subsequent year following recommended practices.
19
. Additionally, we gathered data on 4 key health system inputs, including current health spending per capita, physician density, nurses’ and midwives’ density, and hospital bed density, from the GHO.
28
For a list of data sources for the other variables, refer to
For countries in which data were missing from institutional databases, we adopted a 2-stage approach to address these gaps. In the first stage, we prioritized data from nationally representative surveys over hospital-based and administrative data, using information on catastrophic health expenditure and impoverishing health spending from peer-reviewed studies.10,11 Further details are provided in
Statistical Analysis
We conducted our analyses in 2 phases. First, we compute the UHC index for each country. Second, we apply a conventional economic analysis framework to assess efficiency by employing a 2-step procedure. During the initial step, we assessed the health system efficiency by considering both health system inputs and outputs. Second, we employ econometric models to elucidate the factors influencing this efficiency.
Estimating UHC index
Based on previous studies,18,20,21 we aggregated the two dimensions of UHC (SC and FP) into an overall summary index. To achieve this, we transformed the FP indicators (CATA and IMPOV) into complements that quantified the portion of the population that did not encounter catastrophic expenses or impoverishment. The FP index was then calculated as the geometric mean of these complements, each given an equal weight. This choice of geometric mean, as opposed to the arithmetic mean, was deliberate and aimed to introduce a penalty for countries that excelled significantly in one indicator or dimension but performed poorly in the other. 20

We then computed the UHC index by aggregating the SC index with the FP index in equation (1). We assigned equal weights to both dimensions because policymakers are willing to trade off one for the other.

Data envelopment analysis (DEA)
DEA is a non-parametric data-driven linear programing technique used to compute efficiency scores for each DMU in a dataset.12,13 Technically efficient DMUs achieve a score of 1.0 or 100%, whereas inefficient DMUs achieve efficiency scores of less than 1.0 or less than 100%. Notably, DEA assesses the efficiency of a DMU relative to the best practices observed within the dataset, allowing us to benchmark health systems globally in our analysis. DEA has found extensive application in evaluating the efficiency of hospitals and health systems across various regions, including Africa,22,35 Asia,24,25 Europe,36,37 and Latin America and the Caribbeans (LAC). 29
While DEA can operate under a constant return to scale (CRS) model, assuming that an increase in inputs results in a proportionate increase in outputs, this model may not be suitable for our analysis. Many health systems function at suboptimal scales because of factors such as imperfect competition, government regulations, and public sector bureaucracy.12,22 Therefore, the variable return to scale (VRS) model, which accounts for the possibility of inputs leading to proportionate increases or decreases in output, is more appropriate. This choice aligns with the nature of health service production, which typically exhibits an increasingly concave relationship with health expenditure.13,22 We also adopted an output-oriented model, which seeks to maximize the output, represented by the UHC index, while keeping the health system inputs constant. This approach aligns with the policy objective of increasing the UHC levels. 1 Furthermore, using an input-oriented model with restricted inputs would be inappropriate, especially for health systems in LMICs, where there is often a deficiency in healthcare resources, such as healthcare workers, funding, and equipment. 2
Therefore, using the VRS output-oriented DEA approach, we estimated the efficiency of health systems as follows:

Subject to constraints:




Where Yrj the amount of output r from country j, Xij the amount of input i to country j, Or the weight given to output r, Vi the weight given to input i, n the number of countries, s the number of outputs, m the number of inputs, O0 > 0 defines increasing returns to scale, O0 = 0 defines constant return to scale (CRS), and O0 < 0 defines decreasing returns to scale. Technical efficiency scores, denoted as ϕ, are defined within a range of 0.00 to 1.00. An efficiency score of 1.00 signifies that the production process within the DMU operates at maximum efficiency. Conversely, if the score is less than 1.00, the production process is considered inefficient. In addition to our global analysis, we also explored health systems’ efficiency by WHO regions (African Region (AFR), Region of the Americas (AMR), Eastern Mediterranean Region (EMR), European Region (EUR), South-East Asian Region (SEAR), and Western Pacific Region (WPR)), income classification (low, lower-middle, upper-middle, and high), and economic groups.
We performed Kruskal-Wallis H tests to assess the potential association between the efficiency estimates and health system characteristics: dominant mode of financing healthcare services (state, private, and external), income classification (low-income, lower-middle-income, upper-middle-income, and high-income), WHO region (AFR, AMR, EMR, EUR, SEAR, and WPR), and Mann-Whitney U test for the passage of UHC legislation (Yes and No).
We also performed a Tobit regression analysis to assess the association between DEA efficiency estimates and the following potential health system efficiency determinants: economic status, health financing, governance quality, economic inequality, education, and urbanization. Due to the high correlation between the health financing options (GOV, OOP, and EXT) and governance quality indicators, we conducted an exploratory factor analysis using the iterated principal factor method to identify the most representative indicators for inclusion in our models. For health financing options, we discovered that one factor could effectively explain more than two-thirds of the variance in these indicators, leading us to select a single representative indicator for inclusion in our models (see
We specified our final Tobit regression model as follows:

where ϕ denotes the technical efficiency scores, i represents the ith country, GDP is GDP per capita, CHE signifies CHE as a percentage of GDP, OOP denotes the OOP expenditure as a percentage of CHE, PHC is primary health care expenditure as a percentage of the CHE, GEFF is government effectiveness (governance quality), ROL is the rule of law (governance quality), LEG is the passage of UHC legislation (Yes/No), GINI is the Gini coefficient, EDU is the mean years of schooling, URB is urbanization, and εi is the stochastic error term. We also included our initial DEA estimates in a Simar and Wilson smoothed bootstrap analysis to estimate the robust efficiency score and identify factors associated with these estimates. 14 We conducted sensitivity analyses to assess the robustness of this model using different combinations of input and output variables, excluding efficient health systems, health systems in selected economic groups, and health systems with imputed data. 34 We compared the efficiency scores using Pearson’s correlation coefficients. We conducted all statistical analyses using Stata MP 18.0 (StataCorp LLC®) and considered an α (alpha) of 0.05 as the cut-off for statistical significance.
Results
Overall, our analysis included 191 national health systems responsible for 99.6% of the global population. 38 The overall UHC index ranges from a minimum of 48.4 (Somalia) to 94.8 (Canada) with a global mean, median, and standard deviation of 76.9, 80.3, and 12.0 respectively. Figure 1 illustrates the significant differences in the distribution of UHC indices based on WHO region (Figure 1a) and income classification (Figure 1b). Countries in the WHO African region have the lowest UHC index, whereas countries in the WHO European region have the highest. Figure 1b shows a steady increase in the UHC index based on income classification, with low-income countries having the lowest UHC indices and high-income countries having the highest. Figure 2 shows the positive exponential relationship between the average CHE per capita (2016-2020) and UHC index. Initially, small increases in health expenditure yield large changes in UHC, but as the levels of health expenditure rise, the marginal improvement in the UHC index diminishes. The average CHE elasticity was estimated to be + 0.05377, indicating that, if the average CHE per capita increased by 1%, the UHC index increased by 0.054%. Table 1 show the descriptive results for the input and contextual indicators. The global average CHE per capita was $1103, with significant differences between countries based on the WHO regions.
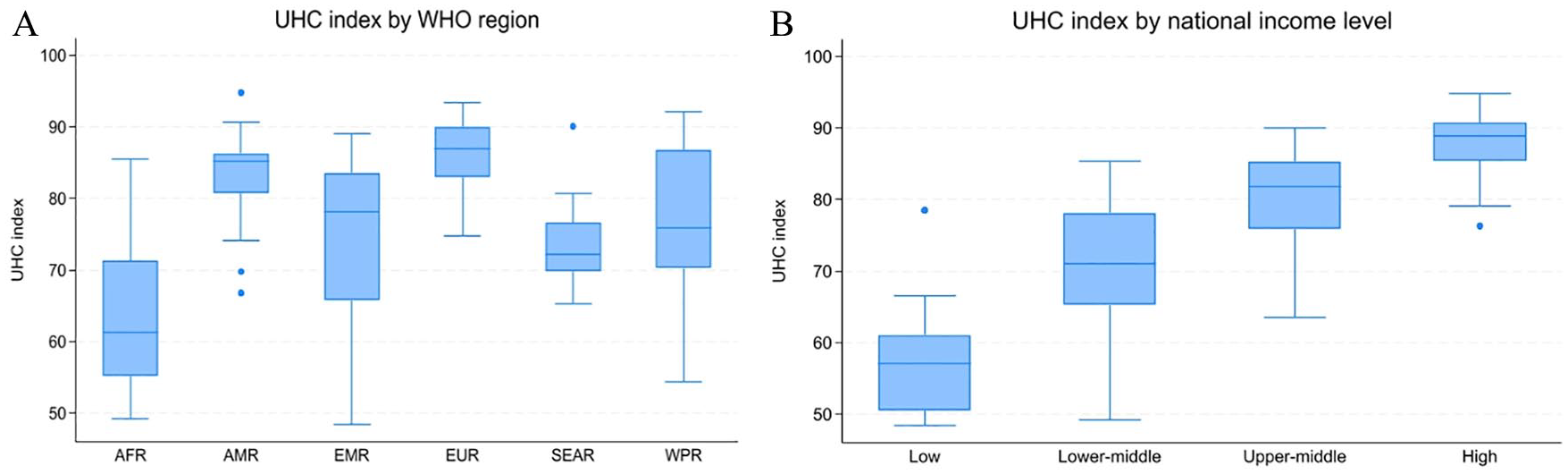
UHC index by WHO regions (A) and income classifications (B).

Relationship between mean current health expenditure per capita (2016-2020) and UHC index in 2021.
Descriptive Statistics of Input, Output, and Contextual/Environmental Indicators/Variables by WHO Regions.

Note. AFR = WHO African region; AMR = WHO Americas region; CHE = current health expenditure; EMR = WHO Eastern Mediterranean region; EUR = WHO European region; GDP = gross domestic product; OOP = out-of-pocket; PHC = primary health care; SEAR = WHO South-East Region; UHC = universal health coverage; USD = United States dollars; WPR = WHO Western Pacific region.
Per 10 000 of the population.
# As a percentage of the current health expenditure (CHE).
Our DEA suggests that the global average health system performance toward achieving UHC, given the available health system inputs (CHE per capita, doctors, nurses, and beds), was 94.7% – Table 2. This suggests that the current global UHC index can be boosted by a mean of 5.32% with the same level of health-system inputs. The countries with the most efficient health systems toward this goal given their health system inputs are Niger, Madagascar, and Sierra Leone, while the least efficient are Libya, Angola, and Nigeria. Overall, 174 health systems had decreasing returns to scale performance, 12 had constant returns to scale, and 5 had increasing returns to scale (
Technical Efficiency Estimates from 2-Stage Output-Oriented DEA.

The State of Palestine (West Bank and Gaza) was not included in our analysis.
The Sahrawi Arab Democratic Republic is not included in our analysis.
The European Union (EU) is not included as a single block in this analysis.
Note. ASEAN = The Association of Southeast Asian Nations; AU = The African Union; BRICS = Brazil, Russia, India, China, and South Africa; CARICOM = The Caribbean Community; ECO = The Economic Cooperation Organization; EU = The European Union; G7 = Group of 7; G20 = Group of 20; OECD = The Organization for Economic Cooperation and Development; SCO = Shanghai Cooperation Organization; SD = Standard deviation; SELA = Sistema Económico Latinoamericano y del Caribe (Latin American and the Caribbean Economic System.
Table 3 shows the results of the final bootstrapped regression model used to evaluate the impact of economic status, health financing, governance quality, economic inequality, education, and urbanization on health system efficiency. Three of the 10 variables used in the final model–PHC expenditure as a percentage of CHE, government effectiveness (governance quality indicator), and passage of any UHC legislation–were statistically significant (P < .05). PHC expenditure as a percentage of CHE was statistically significant and positively contributed to the efficiency of the health systems. A one-percentage-point increase in PHC expenditure as a share of CHE was associated with a 0.999% increase in health systems’ efficiency toward achieving UHC. Government effectiveness and the passage of any UHC legislation both improved the efficiency of health systems’ efficiency toward achieving UHC. A unit increase in government effectiveness improves health system efficiency toward achieving the UHC goal by 0.932%. Unsurprisingly, the passage of UHC legislation is positively associated with health system efficiency. A stronger rule of law was associated with higher performance of the health system in the country, although this was only statistically significant at the 10.0% significance level. However, economic status, CHE as a share of GDP, government health expenditure as a share of CHE, and urbanization were not significantly associated with the health systems’ efficiency toward achieving UHC.
Determinants of the Health Systems Technical Efficiency Based on Simar & Wilson Smoothed Bootstrap Analysis of Shephard Bias-Corrected Inefficiency Estimates.
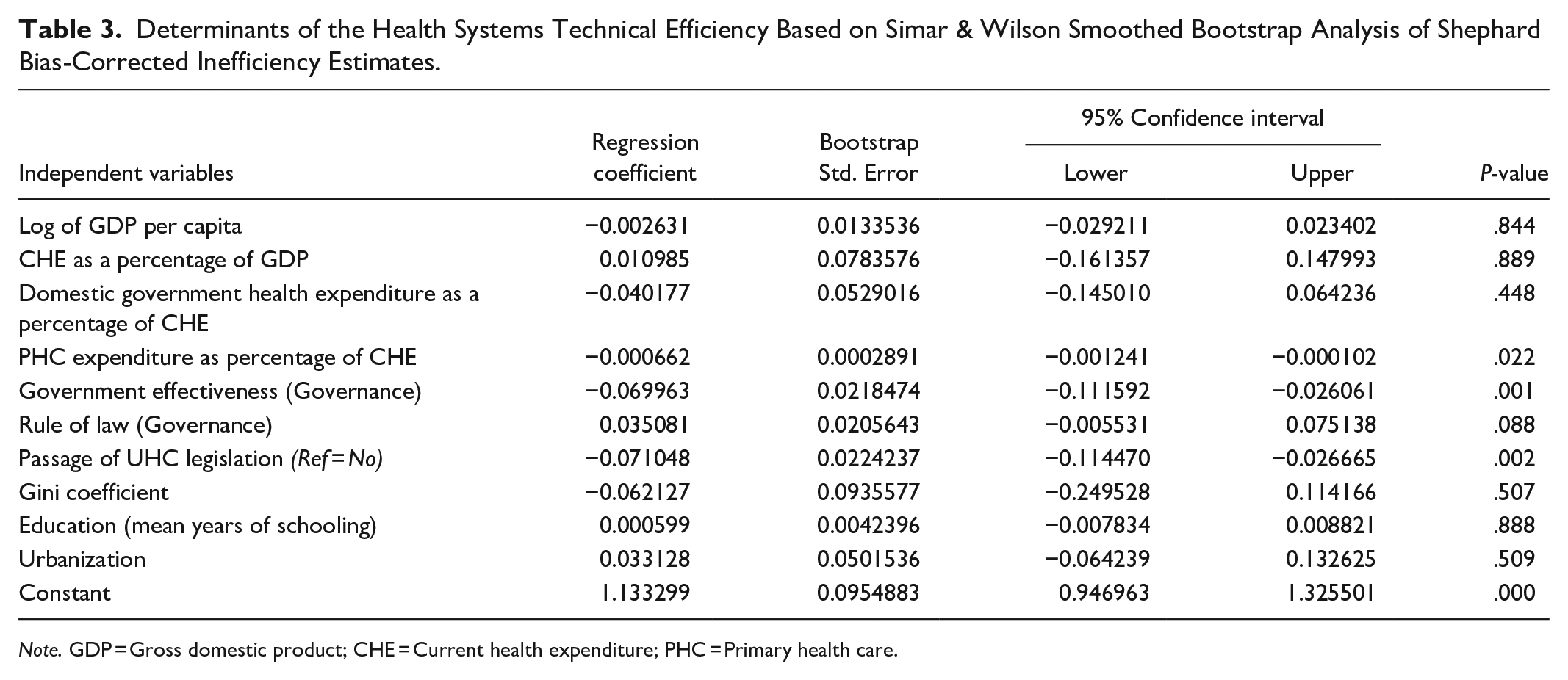
Note. GDP = Gross domestic product; CHE = Current health expenditure; PHC = Primary health care.
Restricting the DEA analyses to only countries within each income classification yielded efficiency estimates that were significantly correlated with estimates from the global model (Pearson correlation coefficient ranged from .696-.944)
Discussion
This study evaluates the technical efficiency of health systems toward achieving the UHC goal midway to 2030 and provides the most recent and comprehensive estimates of global, regional, and national health-system efficiency toward this goal. Despite the widespread scarcity of healthcare resources in most countries, only one in 5 health systems are efficiently using these scarce healthcare resources toward achieving UHC, and there are sizable differences in efficiency scores across global regions and income classifications. In addition, most countries (93.7%) have scale inefficiency, suggesting a need for interventions to improve the productivity of health systems in the run-up to 2030. Also, favorable macro-fiscal policies are required to raising finance for the health sector development.39,40 In addition, the share of current health expenditure spent on PHC, governance quality, and the passage of UHC legislation were all significantly associated with health system efficiency toward UHC. Surprisingly, the share of GDP spent on health, the economic status of the county (GDP per capita), and education were not significantly associated with efficiency.
Our study shows that increasing investment in PHC improves the efficiency of health systems toward achieving their UHC goals. This observation holds because the aims of the UHC largely overlap with those of the PHC. While UHC aims to guarantee access to needed healthcare services to all people who need them without undue financial hardship, PHC addresses the health needs of all patients at the community level by integrating curative and preventive healthcare services. PHC is one of the 3 main tiers of health system infrastructure in most countries, and the tier closest to the very people that UHC aims to extend high-quality affordable healthcare services to – the poor, vulnerable, and marginalized. Furthermore, PHC facilities such as health posts, primary health centers, community health centers, dispensaries, and subcentres are accessible to everyone in the community and are the first point of contact between most patients and the health system. Indeed, PHC, as a means, paves the way for achieving UHC, as a goal.41,42 Studies from Caribbean, Asian, and sub-Saharan African countries demonstrate that investments in PHC significantly improve health service delivery toward UHC.18,41-44
Our study demonstrates a significant association between governance factors and health-system efficiency. Health systems are increasingly decentralized structures, engaging diverse, heterogeneous, complex, and dynamic networks of actors for generating resources, delivering services, and financing care. 45 The importance of health system governance as a significant determinant of health system performance and achievement of health-specific goals, including UHC, is increasingly recognized. 46 Governance is broadly construed as “the rules that distribute roles and responsibilities among societal actors and shape the interactions among them.” 47 With the appropriate use of standards, incentives, performance information, and accountability, good health system governance significantly boosts efficiency.48,49 Our analysis suggests that compared to high-income countries, governance remains a huge challenge in low-income countries, where weak accountability, incentives, and regulatory systems within public institutions foster inefficiency, corruption, and waste. Corruption diminishes the performance of any system, and ultimately leads to zero output. 48 Indeed, health system governance is the key change-maker for UHC at the local, national, and global levels and is fundamental for improving the efficiency, resilience, and responsiveness of health systems. 49
Our study also demonstrated a significant relationship between the passage of UHC legislation and health system efficiency. Health laws are used to formalize commitment to goals, such as UHC and creating a drive for action. 50 By establishing UHC as a desired goal within the legal framework of a country, UHC legislation codifies the prevailing political momentum into actionable policies that direct the interaction between different health system actors to deliver healthcare services more efficiently. 50 Enacting UHC legislation requires broad discussion across political divides on the concept and practicalities of UHC, arriving at a consensus on the package of care that is acceptable to all gender and age groups, fair and affordable to everyone, and feasible for the country, and codifying all these into law. 51 Although our initial bivariate assessment (Mann-Whitney U test) of the association between UHC legislation and health system efficiency was not statistically significant, our multivariate regression analysis (after including other variables including governance factors) showed a completely different association. This suggests that enacting UHC legislation is a necessary but insufficient determinant of health system efficiency; that is, enacting UHC legislation alone does not alter health system efficiency toward UHC unless it is matched with strong political and health system governance. 51
Strengths and Limitations
While our study represents a comprehensive assessment of the potential efficiency of health systems toward achieving UHC, given resource constraints, our findings should be understood considering a few limitations. First, in a multi-country assessment, such as ours, data availability is a major challenge. Despite our use of few simple and undemanding indicators, many countries, including several high-income technologically advanced countries, lack complete data on key UHC indicators and health expenditure indicators. Despite employing an advanced statistical approach to remedy this, data challenges remain, as imputed data are unlikely to be as accurate as locally collected data. Second, in comparing the relative efficiency of health systems, our assessment did not include any indicator of the quality of healthcare services – an important goal of UHC and a critical indicator on which health system performance should be assessed. Regrettably, there are currently no universally applicable indicators suitable for use in multicountry studies assessing health system efficiency. Third, our simplified assessment of health system efficiency, focusing on the conversion of healthcare resources into valued outputs, overlooks the various structural and organizational factors that significantly influence service delivery. For instance, our evaluation did not account for prior investments in infrastructure, such as transportation networks, power grids, and Internet access, as well as technological capabilities. While it is not feasible to encompass these complex factors in our assessment, it is important to interpret our findings in the context of this omission.
Policy Implications
Notwithstanding these limitations, our study offers valuable insights into policy discussions and health-system reforms. Overall, there appears to be substantial room for efficiency improvement in health systems in most countries, especially in sub-Saharan Africa and Southeast Asia. These potential efficiency improvements are important not only from the standpoint of public sector accountability, given that a substantial portion of health system funding comes from the public sector, but also because they can contribute to progress toward UHC. National, subnational, and sector-specific assessments of health system efficiency serve as valuable tools that policymakers can use to identify inefficiencies, allocate resources more effectively, and implement critical reforms within the healthcare system. Moreover, the inclusion of countries with various income classifications and WHO regions in the list of efficient nations implies that any country, regardless of its economic status or geographical region, can develop an efficient health system. The strong association between PHC expenditure and health system efficiency toward UHC suggests that the UHC goal might only be achieved at significantly earmarked levels of PHC expenditure. This implies that policymakers must make a conscious effort to increase PHC expenditures to ensure attainment of the UHC goal. Likewise, to achieve UHC by 2030, all countries must commit to actionable steps to strengthen health systems by improving health system governance and passing universal healthcare legislation. Important lessons from Costa Rica and South Korea suggest that incremental implementation may be more realistic for LMICs. 50 Lastly, continued efforts to improve technical efficiency need to be undertaken alongside advocacy efforts to increase investment in health. Given the low-level health expenditures in Africa, the eastern Mediterranean, and Southeast Asia, efficiency gains alone will be insufficient to attain UHC.39,40 Consequently, a dual strategy that combines improved efficiency with increased healthcare investment is essential for realizing UHC goals.
Conclusion
Despite some improvement in the global UHC index compared to the 2019 estimates, it remains suboptimal, with stark disparities among countries, WHO regions, and income classifications. Our study suggests that a significant majority of health systems are inefficient, regardless of their income classification or WHO regions. More importantly, this study highlights those improving investments in PHC significantly boosts health systems’ efficiency toward toward achieving UHC. In addition, effective governance at the local, national, and global levels coupled with a concerted enactment and implementation of UHC legislation are necessary measures to enhance health systems’ efficiency toward UHC.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241235759 – Supplemental material for Evaluating health systems’ efficiency towards universal health coverage: A data envelopment analysis
Supplemental material, sj-docx-1-inq-10.1177_00469580241235759 for Evaluating health systems’ efficiency towards universal health coverage: A data envelopment analysis by Paul Eze, Chidumebi Judith Idemili and Lucky Osaheni Lawani in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We thank Professor Joel E. Segel (Penn State University) for his helpful comments and suggestions.
Authors’ Contributions
Data Availability Statement
The datasets analyzed in this study are publicly available from the sources mentioned in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval for this study was not required as this study retrieved and synthesized publicly available data.
Consent to Participate
Not applicable
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.