
Abstract
South Western Sydney (SWS) is one of the fastest growing regions in the state of New South Wales (Australia). Much of the population live in local government areas (LGAs) with levels of disadvantage higher than the state average, with a predominance of non-communicable and chronic diseases that are typically associated with age-related and behavioural factors. This necessitates the management of social determinants of health through the integrated provision of primary and social care. The SWS Local Health District and Primary Health Network is exploring the potential of community health alliances (CHAs) as an innovative approach to support the provision of integrated health services. CHAs are a population health approach for addressing health challenges faced by people who share a common area of residence, sociocultural characteristic or health need, and are characterised by a shared mission, shared resource needs and acquiring/developing necessary organisational knowledge and skills. We explore how CHAs operate as social enterprises that utilise digital health and citizen engagement to deliver integrated people-centred health services (IPCHS) by conducting two case studies of CHAs operating in SWS: in Wollondilly and Fairfield LGAs. Using this approach, we aim to unpack the conceptual convergence that enables social enterprises to utilise digital health interventions and citizen engagement strategies to co-produce IPCHS with a view to developing theory and a framework for engaging digital citizens in integrated primary health care via social enterprise.
Keywords
Introduction
Community health alliances (CHAs) are a population health approach for addressing the challenges faced by people who are united by a common area of residence, sociocultural characteristic or health need, and are generally characterised by a shared mission, shared resource needs and the task of acquiring/developing necessary organisational knowledge and skills. 1 In South Western Sydney (SWS), CHAs are being explored as an innovative approach to support the provision of integrated health services. 2 The SWS Local Health District (LHD) is among the most diverse regions in the Greater Sydney metropolitan area. Around 44% of inhabitants were born overseas, and 51% speak a language other than English at home, while 21% are children aged 0–14 years. 3 In terms of population density, the region includes urban, suburban and peri-urban areas. The SWSLHD is also the setting of the SWS Primary Health Network (PHN) and is divided into local government areas (LGA). The region is undergoing a period of unprecedented growth and is one the fastest-growing regions in New South Wales, with 33% growth predicted from 2016 to 2031. Much of the population live in LGAs with levels of disadvantage higher than the state average, with a predominance of non-communicable and chronic diseases that are typically associated with age-related and behavioural factors which necessitate integrated primary and social care.
Social enterprises can utilise digital health interventions and citizen engagement strategies to integrate health services. Building on the foundational work of Liaw et al. which highlighted the convergence of global eHealth, social business and citizen engagement 4 and its potential for addressing the production of integrated people-centred health services (IPCHS), 5 we will explore how CHAs in SWS operate as social enterprises to enable care integration within their LGA. This will be used to develop theory about how CHAs work, with a view towards developing a framework for their monitoring and evaluation.
A conceptual framework: foundation for inquiry
The redevelopment of primary-care systems that is required for meeting future health and care delivery needs holds considerable promise for (a) employment generation driving economic growth, (b) improving social protection and cohesion and (c) promoting technological innovation and integration, all while improving health outcomes through health-care provision. 6 However, realising this promise requires health services that are financially sustainable and promote equitable economic growth, responsive and accountable to the populations they serve and technologically enabled to maximise access and affordability to the socio-economically disadvantaged. To address these issues, the 2016 High-Level Commission on Health Employment and Economic Growth recommended three promising sectoral innovations: (a) social enterprises as ‘a private-sector, socially-oriented solution to serve the unserved’; (b) ‘digital technologies’ in health, including ‘electronic health (e-health), mobile health (m-health)’ and ‘electronic … information systems’; and (c) engaging citizens and communities in implementing these. 7
Digital health is ‘the field of knowledge and practice associated with any aspect of adopting digital technologies to improve health, from inception to operation’. 8 It includes ‘eHealth’ as well as developing computing sciences, such as big data and artificial intelligence, among others.9,10 As a market-based innovation for addressing social issues, 11 a ‘social enterprise’ is a business entity that aims to fulfil a social and/or environmental mission while being financially sustainable. 12 Citizen engagement is a ‘two-way interaction between citizens and governments or the private sector, with the objective of improving development outcomes’. 13 Considering the global need and demand for health and care services, social enterprises that utilise digital technology and citizen engagement hold promise for accelerating global progress towards IPCHS for universal health coverage and sustainable development goals (Figure 1).4–7,14–16

Digital health, social enterprise and citizen engagement in integrated people-centred health services (IPCHS) for achieving universal health coverage and sustainable development goals.
Literature review and framework synthesis
A review of literature was performed to synthesise a preliminary conceptual framework on the utilisation of digital health, social enterprise and citizen engagement in the co-production of IPCHS (Table 1). Drawing from applications of the critical realist approach in organisational research, 17 framework elements are categorised as either context, intervention, mechanism or outcome. 18 Outcomes emerge as result of the interaction between contexts (comprising ecosystems and actors), 18 interventions (comprising structures and interventions) 19 and mechanisms, which are hidden ‘underlying entities, processes, or structures which … generate outcomes of interest’. 20 A more detailed explanation of this framework will be provided elsewhere. The information that will be sought in this study pertains directly to the elements and dimensions outlined in this conceptual framework.
Preliminary framework on the utilisation of digital health, social enterprise and citizen engagement in the co-production of IPCHS.
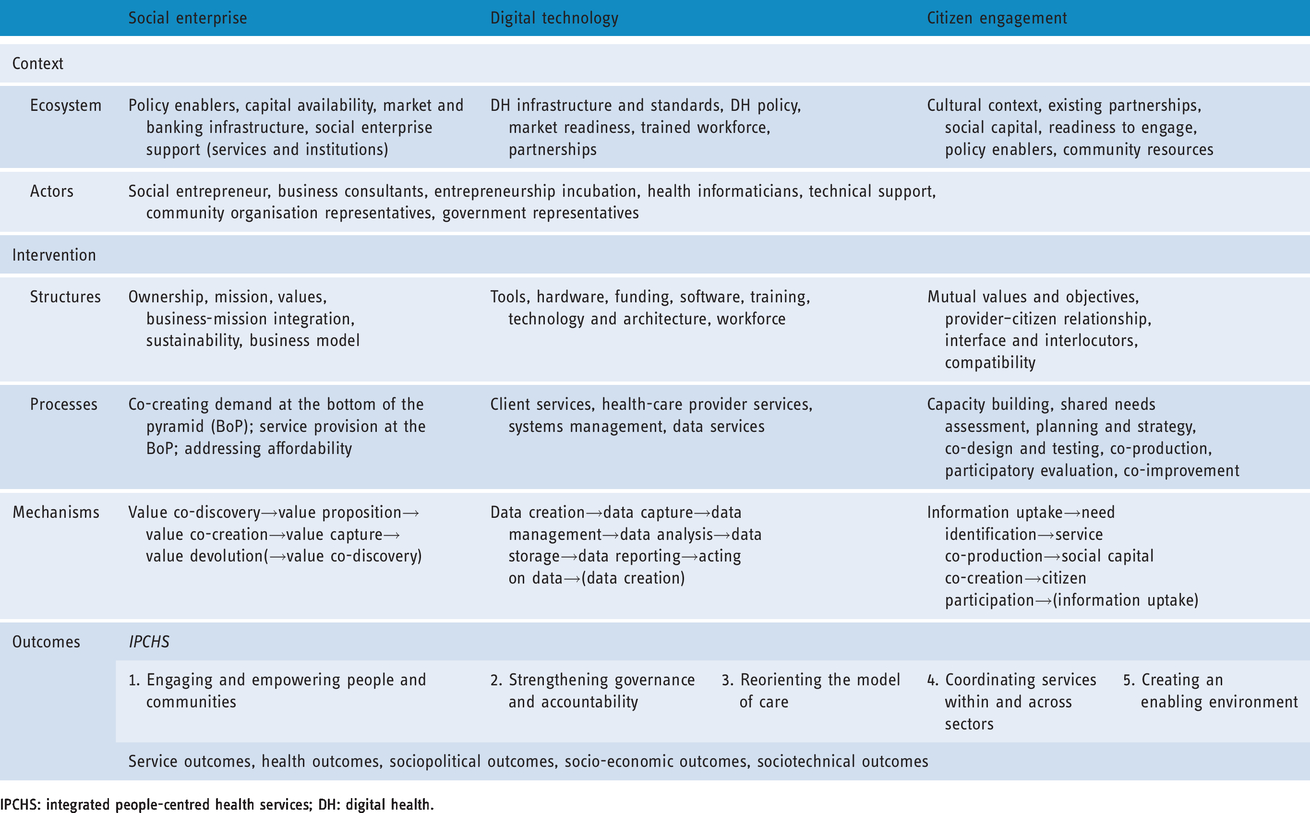
IPCHS: integrated people-centred health services; DH: digital health.
Objectives
We aim to: (a) investigate how CHAs operate as social enterprises that utilise digital health and citizen engagement to co-produce IPCHS; and (b) test a conceptual framework on the utilisation of digital health, social enterprise and citizen engagement in the co-production of IPCHS.
Research design and methods
To address these objectives, we will employ a case-study design involving both quantitative and qualitative data to investigate the elements and dimensions described in the conceptual framework (Table 1). To test this framework, we will explore how CHAs operate as social enterprises that utilise digital health tools and citizen engagement approaches to support the delivery of IPCHS. We will base our inquiry on the critical realist philosophical stance as applied in organisational case-study research. 21
Defining the CHA as a case
For the purpose of this case study, we define the case as a CHA. CHAs are a population health approach for addressing the challenges faced by people who are united by a common area of residence, sociocultural characteristic or health need, and are generally characterised by a shared mission, shared resource needs and the task of acquiring/developing necessary organisational knowledge and skills. 1 CHAs can vary in their degree of organisational formality, ranging from an informal inter-organisational collaboration, a contractual agreement shared governance structure, to a single-firm consolidation involving shared ownership. 1 For this case study, a CHA will comprise a single organisational entity. 1
Selection of CHAs for case study
We used a ‘distribution-based’ case-selection strategy (for small-n analyses), allowing for the selection of (a) a typical case and (b) a diverse case. 22 In keeping with pragmatist recommendations, access to the cases of interest was a consideration in case selection as well.23,24 In keeping with the realist approach, two cases were purposively selected for diversity in order to enable insights to be generated through a cross-case comparison. We will study two CHAs operating in different LGAs under the SWSPHN: the Wollondilly Health Alliance (WHA) and the Fairfield City Health Alliance (FCHA). As part of the ongoing health-system development for integrated care services, the WHA was born out of an ongoing collaboration between the SWSPHN, the SWSLHD and the Wollondilly Shire Council. 25 Similarly, the FCHA involved the SWSLHD, SWSPHN and Fairfield City Local Council. 26
The social, economic, cultural and political background of Wollondilly and Fairfield differ considerably from each other. While the Fairfield LGA is a predominantly urban/suburban setting, the Wollondilly LGA is much less densely populated as a peri-urban setting. In 2016, the Fairfield LGA was the most disadvantaged in the Sydney metropolitan region, and the fourth most disadvantaged in the state. Within SWS, Fairfield has the highest proportion of residents who speak a language other than English at home (71%), the most common of which were Arabic, Vietnamese or Cantonese. 27 Relatively, Wollondilly LGA is considerably more socio-economically privileged, as illustrated by data from several metrics in the SWSPHN Needs Assessment 2019–2022 (Table 2). 27 Comparing CHAs in different settings (each with different health needs, cultural diversity, etc., as illustrated above) can provide valuable insights into the variable context (ecosystem and actors), interventions (structures and processes) and mechanisms that produce the CHAs’ outcomes (i.e. IPCHS).
Population characteristics of Fairfield and Wollondilly (adapted from SWSPHN Needs Assessment 2019–2022).
LGA: local government area; SWS: South Western Sydney
Data-collection methods
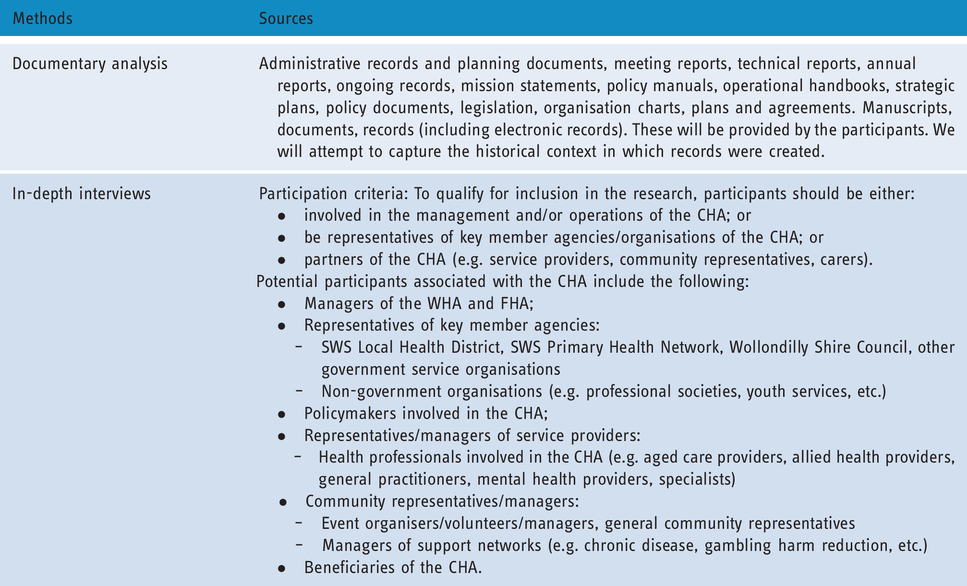
The study will involve a variety of different data-collection methods to facilitate the triangulation of approaches, data and methods at the stage of analysis. Data collection will aim to collect information that may provide support for rival/alternative theories about how the intervention of interest may work. Data-collection methods will include documentary analysis of archival records, and semi-structured in-depth interviews (Table 3). We will standardise data collection across the two case studies using an interview guide (see Appendix 1) that we developed based on the preliminary conceptual framework (Table 1). We will involve a diverse range of stakeholders and documents to build a comprehensive and coherent understanding of the context, interventions, mechanisms and outcomes involved by iteratively clarifying doubts and elucidating missing information. 28
Data-collection methods and sources.

Strategy for identification and invitation of participants
CHA managers will be the first participants to be recruited and interviewed. Subsequent participants will be identified based using a snowball sampling (referral sampling) approach from contacts/references provided by CHA managers based on their respective association with the CHA. Contact with potential participants will be established via CHA managers’ introductions, and subsequently by email containing all necessary information (see Appendix 2). The researcher will then visit each participant in person, explain the study in detail, answer questions and obtain each participant’s informed consent. Participants will be provided with information sheets detailing the nature of the participation, the kind of information they will be required to provide and the rights of participants (in accordance with the Declaration of Helsinki), including their right to withdraw their participation at any time without damaging their relationship with any participating institutions (see Appendix 3). Any questions that potential participants may have will be addressed prior to obtaining consent. Written informed consent will be sought in the form of a signed consent form. Upon consent, the researcher will be offered the option to have the interview conducted immediately or to set a convenient future date, time and place for conducting the interview.
Participant recruitment
We will recruit approximately 10–15 participants, although the true number will be determined based on achieving information saturation during iterative cycles of data collection and analysis. Data collection will continue until data saturation has been achieved. 29 Participants will not be expected to incur any out-of-pocket expenses, as the student researcher will travel to meet them at the time and place of their choice. Hence, no reimbursement or incentive (financial or otherwise) will be provided to participants for their participation in the study.
Methods for recording and storing data during collection
Research data and materials will be retained for five years after the date of publication. We do not intend to reuse or share the data for a secondary research purpose. In terms of archival records, electronic documents will be saved in PDF format, and physical documents will be scanned and saved in image formats (e.g. JPEG, PNG) and, if possible, subsequently formatted into text format for coding. Diagrams will be coded as image files. With regard to semi-structured in-depth interviews, these will be audio recorded (MP4 format) using an electronic recording device, and the recording files will be securely saved and de-identified, transcribed and coded. Printed data will be stored in locked filing cabinets at UNSW, and electronic data (including audio tapes) will be stored in password-protected networked computers to ensure confidentiality. The participants will be de-identified during data collection by assigning codes.
Data analysis
Collected data (both quantitative and qualitative) will be analysed using NVivo v12. The student researcher who will conduct the interviews will also perform the analysis. Senior researchers will review, critique and validate the analysis and results. Both within-case and cross-case analysis will be performed. For inductive coding, this grounded approach will remain close to the data, so as to be ‘driven to theory’. 30 For deductive coding, we will employ a ‘framework approach’ to analyse the data, 31 using a deductive structured approach to coding based on the conceptual framework outlined earlier (Table 1). Analysis of the case studies will focus on identifying the CIMO configurations described in the framework and will apply principles of analytical generalisation to attribute causation to the outcomes of interest. 23
Within-case analysis
Within-case analysis will:
Determine the outcomes achieved by the CHA from the perspective of key stakeholders involved; Identify the CHA interventions by which these outcomes are produced; Identify the structures and processes involved in implementing the CHA interventions; Determine the mechanisms by which interventions produce outcomes; Characterise the context (ecosystems and actors) within which interventions are enacted; and Identify the facilitators and barriers to producing the outcomes of interest.
Cross-case analysis
Cross-case analysis will:
Explore differences, similarities and trends/patterns in context, structure, interventions, processes, mechanisms and outcomes between/across different CHAs; and Develop and discuss explanations for cross-case comparisons, considering existing theory.
Dissemination of results
The participants will be de-identified during data collection by assigning codes, and the results will be written up in a way that no participant or practice can be identified following dissemination. Case studies will be reported in accordance with established guidelines for the reporting of observational studies (e.g. STROBE Statement) 32 and organisational case studies in health research. 33 Where possible causal relationships between systems components will be illustrated using systems maps. 34 The findings will then be presented at scientific conferences and submitted for publication in peer-reviewed journals. A plain-language summary of findings will be sent to the patients and participating health-care professionals. Publications will be shared with the participants.
Supplemental Material
sj-pdf-1-dhj-10.1177_2055207620930118 - Supplemental material for Community health alliances as social enterprises that digitally engage citizens and integrate services: A case study in Southwestern Sydney (protocol)
Supplemental material, sj-pdf-1-dhj-10.1177_2055207620930118 for Community health alliances as social enterprises that digitally engage citizens and integrate services: A case study in Southwestern Sydney (protocol) by Myron Anthony Godinho, Md Mahfuz Ashraf, Padmanesan Narasimhan and Siaw-Teng Liaw in Digital Health
Supplemental Material
sj-pdf-2-dhj-10.1177_2055207620930118 - Supplemental material for Community health alliances as social enterprises that digitally engage citizens and integrate services: A case study in Southwestern Sydney (protocol)
Supplemental material, sj-pdf-2-dhj-10.1177_2055207620930118 for Community health alliances as social enterprises that digitally engage citizens and integrate services: A case study in Southwestern Sydney (protocol) by Myron Anthony Godinho, Md Mahfuz Ashraf, Padmanesan Narasimhan and Siaw-Teng Liaw in Digital Health
Supplemental Material
sj-pdf-3-dhj-10.1177_2055207620930118 - Supplemental material for Community health alliances as social enterprises that digitally engage citizens and integrate services: A case study in Southwestern Sydney (protocol)
Supplemental material, sj-pdf-3-dhj-10.1177_2055207620930118 for Community health alliances as social enterprises that digitally engage citizens and integrate services: A case study in Southwestern Sydney (protocol) by Myron Anthony Godinho, Md Mahfuz Ashraf, Padmanesan Narasimhan and Siaw-Teng Liaw in Digital Health
Footnotes
Contributorship
M.A.G. conceptualised the work, drafted and revised it critically for important intellectual content and approved the final version to be published. M.M.A. conceptualised the work, drafted and revised it critically for important intellectual content and approved the final version to be published. P.N. conceptualised the work, drafted and revised it critically for important intellectual content and approved the final version to be published. S.T.L. conceptualised the work, drafted and revised it critically for important intellectual content and approved the final version to be published.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical and scientific approval was provided by the SWS Local Health District Human Research Ethics Committee (HREC), as part of an amendment to ‘the ePBRN research and development program’ (2019/ETH04410). This was then endorsed by the UNSW HREC Executive (HREC/16/LPOOL/83).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Guarantor
ST Liaw.
Peer review
This manuscript was reviewed by reviewers who have chosen to remain anonymous.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.