
Abstract
The global spread of severe acute respiratory syndrome coronavirus 2019 (COVID-19) has affected over 100 countries and has led to the tragic loss of life, overwhelmed health care systems and severely impacted the global economy. Specifically, individuals living with spinal cord injury (SCI) are particularly vulnerable during the COVID-19 pandemic as they often face adverse impacts on their health, emotional well-being, community participation, and life expectancy. The objective of this study was to investigate the lived experience of individuals with SCI during the COVID-19 pandemic in Ontario, Canada. An exploratory design with a qualitative descriptive approach was used to address the study objective. Nine semi-structured interviews were conducted with individuals with traumatic and non-traumatic SCI (37-69 years, C3-L5, AIS A-D, and 5-42 years post-injury). Using reflexive thematic analysis, the following themes were created: (1) Caregiver exposure to COVID-19; (2) Staying physically active in quarantine; (3) Living in social isolation; (4) Difficulty obtaining necessary medical supplies; (5) Access to health services and virtual care during COVID-19; and (6) Fighting COVID-19 misinformation. This is one of the first studies to explore the impact of COVID-19 on individuals living with SCI in Ontario. This study contributes to a greater understanding of the challenges faced by individuals living with SCI and provides insight into how to better support and respond to the specific and unique needs of individuals with SCI and their families during a national emergency or pandemic.
The spread of COVID-19 throughout the world has led to increased concerns for vulnerable populations, including individuals with SCI, as they may face adverse impacts on their health, psychological well-being, community participation, and access to necessary medical supplies and services.
Collectively, this research enhanced our understanding of the impact of COVID-19, which can provide insights into how to better support and respond to the specific and unique needs of individuals with SCI and their families during a national emergency or pandemic situation.
The findings of this study contribute to a greater understanding of the impact of COVID-19 on individuals with disabilities and physical disabilities in general and are the first step in developing an evidence-driven approach to creating an equitable, disability-inclusive pandemic response as part of a larger public health emergency plan.
Introduction
The global spread of severe acute respiratory syndrome coronavirus 2019 (COVID-19) affected over 100 countries within a few months since it was first identified. It has led to the tragic loss of life, overwhelmed healthcare systems and severely impacted the global economy. The World Health Organization designated COVID-19 a “public health emergency of international concern” and declared it a pandemic on March 11th, 2020. 1
The spread of COVID-19 worldwide has led to increased concerns for vulnerable populations, including individuals with spinal cord injury (SCI), who are often more susceptible to many physical and psychosocial health complications. 2 It is important to consider the potential effects of COVID-19 and how altered physiology after SCI may affect the presentation and management of COVID-19 symptoms. 2 The increased health risks and a shortage of personal care workers and home and community-based services have worsened a difficult situation for individuals with SCI.
Individuals with SCI are also at a heightened risk of developing complications if infected with COVID-19 due to multiple comorbidities that can pose challenges for diagnoses and increase susceptibility. 3 To expand, due to paralysis of respiratory muscles, the symptoms of cough and shortness of breath may be absent.4 -6 At the same time, autonomic complications may impair the typical fever response to infection,6,7 potentially increasing the risk of missing a COVID-19 diagnosis. 6 The inability to cough and clear respiratory secretions6,8,9 and impaired immune function4,5,10,11 are characteristic of SCI and can also increase the risk of severe COVID-19 once infected. This study aimed to explore how COVID-19 directly impacted individuals with SCI in Ontario, Canada, from May 2020 to July 2020.
Method
Study Design
A qualitative, online study design was used to address the study objective. This approach provides a deep understanding of a topic that has not been studied previously (ie, effects of a global pandemic on individuals with SCI), offers a new perspective on a particular situation and contributes to the overall understanding of lived experiences (in this case, of individuals with SCI during the COVID-19 pandemic).12 -18 Further, this approach allows a researcher to “enter the world of others and attempt to achieve a holistic rather than a reductionist understanding.”19,20 A qualitative methodology was also selected as participants were able to explain their experiences “in their own voice” and as we anticipated a small number of study participants.18,21
A semi-structured interview format was selected as the best method to answer the main and sub-research questions. Semi-structured interviews are a widely used interviewing technique in qualitative research.14,22 -24 This interview format also allowed for reciprocity16,25,26 and the opportunity for the participant to “delve deeply into social and personal matters,” which was not possible in a group setting.16,17,22,27 -29
Our objective was to achieve a nuanced, context-specific understanding of a small sample of participants who share a particular mutual experience rather than attempting to draw conclusions about the broader SCI population.30,31 By exploring the lived experiences of individuals with SCI during the COVID-19 pandemic, we hope to contribute to a greater understanding of how public health emergencies and quarantine situations affect this population and to identify potential solutions or recommendations for how policymakers and healthcare providers can better support individuals with SCI in the future.
Recruitment
Participants were recruited in May 2020 from a university-affiliated exercise facility in Southern Ontario, Canada and via several SCI Facebook groups. Participants were recruited to participate in the study if they were: (1) 18 years of age or older; (2) had experienced a traumatic (eg, motor vehicle accident, fall) or non-traumatic (disc degeneration, inflammation, cancer) SCI; (3) an incomplete or complete SCI; (4) being at least 1-year post-injury; and (5) fluent in English.
Data Collection
Once university research ethics clearance was obtained, participants were recruited using purposive sampling. Members of a University-based accessible exercise program were emailed a copy of the recruitment poster. Voluntary written informed consent was obtained from each participant before the interview. Once enrolled in the study, participants were given a pseudonym. Given the sensitive nature of the study, the contact information and resources of local crisis services and peer support programs available in the Niagara Region and contact information for Niagara Region Mental Health were also provided in case any participant expressed undue distress from the interview. Interviews ranged between 50 and 80 min in duration. All study interviews were conducted over the telephone or online via Zoom Video Communications, per the participant’s preference. 32 This approach allowed the interviews to be conducted safely in adherence with COVID-19 physical distancing restrictions and allowed participants from different regions within Ontario to participate in the study. The interviews were audio-recorded using QuickTime Player© version 10.5 (Apple, Inc., 2018), a multimedia audio recording program. Field notes were recorded by the interviewer, documenting the insights and experiences during the interview.
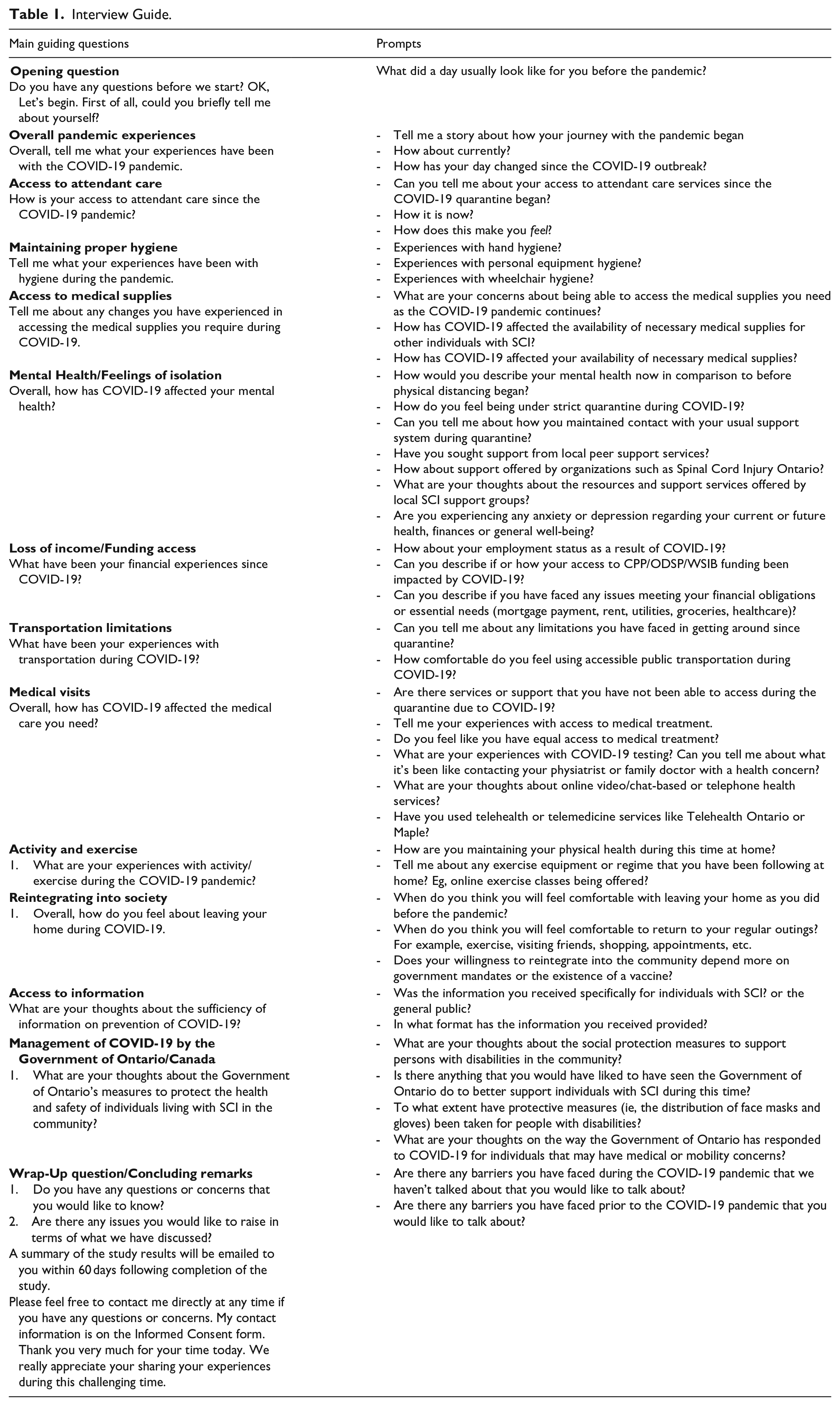
Each interview followed an in-depth, semi-structured interview guide (Table 1). All participants were asked the same predetermined, open-ended questions. The interview guide’s flexibility allowed the researchers to explore specific topics in greater detail and any important unanticipated topics.22,24,33 The interview guide was developed by the first author based on the main research question, and some additional pre-selected probing questions were created. All authors reviewed the interview guide. Some probes were developed during the interview based on the participant’s responses to questions and the semi-structured nature of the interview.22,24,34
Interview Guide.
Data Analysis
Each interview was transcribed verbatim, and the transcript was read multiple times so that the researcher could become immersed in the experiences described by each participant. The NVivo12 software package, a qualitative data analysis application (QSR International, 2018), was used to organize the transcript codes. After thoroughly reading and re-reading the interviews, codes were generated that captured ideas from all interview data. Similar codes were then collated with associated interview excerpts that supported the codes. Following this process, the codes were refined and used to generate potential themes. The codes were reviewed again to confirm that they described each theme. Then, a thematic table of the resulting themes was developed. To ensure that the thematic analysis was representative of the lived experiences described by participants, the interview transcripts, codes, and field notes were repeatedly referred to and contextualized with the findings from the rapidly emerging COVID-19 literature.
Reflexivity
The methodological guidelines provided by Braun and Clarke 35 were used to understand the approach of reflexive thematic analysis. A reflexive thematic analysis approach was used to identify, analyze, and conceptualize patterns or themes (ie, broader concepts related to the research question) within the interview data.35 -37 Reflexive thematic analysis embraces the subjective skills and research values that every researcher brings to a research study. 37 Further, it does not use a coding framework—it is open and organic, and themes are the “outcome of coding and iterative theme development.” 37 Although the reflexive thematic analysis does not have an “inbuilt theory,” 37 it is not atheoretical because researchers have personal, philosophical and theoretical assumptions that are used to inform their use of thematic analysis. A constructivist perspective (ie, reality is socially constructed by the individual in the world in which they live and work) allowed the researcher to understand the lived experiences from the “point of view of those who live it” 38 by providing quotations to illustrate the different perspectives described by research participants.
Results
Nine adults with SCI (7 male and 2 female) between the ages of 37 and 69 years (mean age of 59 years) met the inclusion criteria and completed a semi-structured interview. Detailed participant characteristics are presented in Table 2. Study participants spoke openly about their challenges and experiences during the COVID-19 pandemic. The following themes were identified following in-depth interviews with each participant: (1) caregiver exposure to COVID-19; (2) staying physically active in quarantine; (3) living with social isolation; (4) difficulty obtaining necessary medical supplies; (5) access to health services and virtual care during COVID-19; (6) fighting COVID-19 misinformation. An overview of the themes and subthemes is outlined in a thematic map in Table 3.
Participant Demographics and Clinical Characteristics.

Thematic Table.

Central Theme 1: Caregiver Exposure to COVID-19
Participant statements highlighted the role that caregivers play in their lives and how COVID-19 has changed the way they interact with their caregivers. Participants expressed concerns over whether their caregiver was exposed to or tested positive for COVID-19. The reliance on caregivers to assist with activities of daily living, coupled with an increased risk for severe complications due to COVID-19, caused anxiety in several participants. Matthew was a retired 65-year-old man living with tetraplegia, and his wife was his full-time caregiver because he did not qualify for attendant care. He described “the fear [he] lives in” if his primary caregiver, the participant’s wife, contracts COVID-19: “And now I think for me, I am truly sometimes scared because my wife is my caregiver. I don’t qualify for other caregiving. If she ever got COVID, I am screwed.” He described that he would instead put himself at risk of contracting COVID-19 by going to the grocery store rather than his wife because she would still be able to care for him:
Until then, how bad it is that I’ve often thought it would be better for me if I could manage to go and do the grocery shopping to go and do it so that she wouldn’t get COVID. But if I got it, at least she’d still be able to care for me [. . .] that says it all. That’s the fear that I live in.
Several participants who received assistance from personal support workers (PSWs) felt they were doing their part by staying home all day. However, they faced high exposure because of their PSWs coming into their homes to provide care. For instance, Mary received approximately 3 h of assistance daily from 2 different PSWs. She described the anxiety she felt thinking about the risk of her PSWs contracting COVID-19 from another client,
It’s so stressful. My PSWs see a few people every day, and they have to take the bus. It makes me so scared to think that I could get this [COVID-19] from them. . .but there’s no other option; if I didn’t have their help, I’d be screwed. If one of my PSWs becomes ill, what happens to my care then? Or if I get COVID? It’s just a lot of unknowns. . .it’s our new reality.
The participants described a “learning curve” to ensure that both themselves and their PSWs took the proper precautions. Henry had to reduce his care team from 4 PSWs to 2. He noted that because he was “more vulnerable to COVID,” he felt that he had to establish new rules that he wanted his PSWs to follow, such as spending increased time cleaning and sanitizing during each shift. During the interview, the participant noted the difference between his present care shifts compared to before the pandemic, which were relatively “brief and predictable,” and now they are much longer due to extensive cleaning measures. Similar to other participants, Henry feared the consequences if one or both of his caregivers became infected. He said,
“I have a PSW that I have scheduled to come in the morning to help me out of bed and shower me, and another at night. I honestly don’t know what I’d do if I got infected with the virus or one of my caregivers got infected.”
Further, Jason had difficulties obtaining the PSWs he required for his care. His main PSW enrolled in the Canadian Emergency Response Benefit, and another PSW left the agency that provides PSW services. He said, “I’m really short-staffed, and ParaMed, the agency that provides the PSWs. . .it’s a very difficult time to hire.” Overall, the participants’ comments reflect the importance of caregivers to their self-care and well-being, which have been disrupted due to the pandemic. For formal caregiving, this resulted in a greater reliance on family.
Central Theme 2: Staying Physically Active in Quarantine
Many participants also noted that due to the mandatory quarantine due to the COVID-19 pandemic and mobility restrictions caused by their SCI, they spent an extended period at home. Seven participants were members of a university-based exercise program, which had to close abruptly and for an undetermined amount of time when the Government of Ontario declared a province-wide state of emergency under the Emergency Management and Civil Protection Act on March 17th, 2020. The participants said they did not have adequate space or equipment to exercise in their homes. They described that they could not exercise as frequently, and participation in outdoor activities that they enjoyed before the pandemic could not be performed. Participants also missed the social interaction at their exercise facility, which affected their motivation to exercise at home. Further, a lack of adequate technology to access the online exercise classes offered by their exercise facility posed a challenge for participants.
Lack of space and equipment to exercise
Staying active at home during the pandemic was challenging. Without accessible exercise equipment that many participants used at their exercise facility, they felt unable to safely exercise in a home setting. Matthew described living in a condominium where he found it difficult to maintain an exercise regimen as both the university-based facility and the fitness facility in his building had closed:
“We do have a little fitness room here at the condo unit. But again, now I was using it. They had a treadmill and a recumbent bike that I was using, but now it’s all closed down because we can’t use it because of COVID.”
Without being able to use the equipment in the fitness room, he found it nearly impossible to exercise under quarantine:
“Well, it’s the lack of equipment. We’ve got absolutely no equipment here whatsoever. Or the money to make any equipment available to us so. You know, I mean, you know, again, you’re in. . .you’re in no man’s land. You’re caught between a rock and a hard place again.”
With the limited space for exercise in his condominium, Matthew wheels “through the halls” of the building several times a day to stay fit. He has very minimal use of his arms; however, he was able to complete some arm stretches using a portable massage table:
“We bought a portable massage table, so I do some arm stretches and that on there and keep my arms trying to. . .That’s one of the bigger issues is my arms because I got very minimal use of them. So I got to keep them stretched out.”
Laura currently lives alone, and the pandemic has made her fearful about the possibility of needing an assisted living facility if she cannot be active and exercise for an extended time:
“I’ll tell you what my biggest scare is; this is my biggest fear. But because of the pandemic, and I said to you that my mobility isn’t so bad, I like working out and stuff. I just fear that depending on how long this goes on and that if I become you know less and less mobile, that I would lose my independence and end up in a facility. I couldn’t handle that. I say that and I have to handle it, but I wouldn’t be a happy camper. That would be awful. That’s my biggest fear.”
Depending on the living environments of the participants, some found it more difficult to keep active as they usually did before the pandemic. Living in a condominium or an apartment building meant some participants did not have adequate room or equipment to stay active and felt that their mobility might worsen if lockdown measures continued.
Losing the social benefits of exercise
Participants missed the social benefits of exercising alongside individuals with similar abilities at their university-based facility. As their facility was mandated to close during the first wave of the pandemic in Ontario, participants faced a sudden change in their routine and established exercise habits. In response to this mandatory closure, the university-based facility offered online fitness classes as a way for its members to stay physically active under quarantine. Several participants did not feel motivated to stay active using online exercise classes. Laura was a 69-year-old woman who sustained an SCI 42 years ago. Laura was very social and lived alone in an apartment. Her mobility decreased recently, and while she could stand up and transfer, she could no longer walk. While Laura signed up for an online yoga class, she has found it challenging to stay motivated to exercise without the usual physical contact and company of other individuals with similar physical challenges. She said,
“And I know I know when I should be doing that [exercise]. I know. And my sister actually and her husband just started doing online yoga, and she said, ‘and this person does chair yoga too.’ Which, by the way, I finally signed up for a yoga class before all of this started. Yeah, I was all set to go. Yeah, I never started. So I did listen to this chair yoga the other day, and I listened to it. I didn’t do it, but I listened to it and to motivate myself. I work better alongside other people because when I see other people doing things and they’re as physically challenged as me.”
Adam was 58 years old and sustained an SCI from a sports accident. He used a walker or crutches at home and a wheelchair outside his home. Adam found that while he could complete some armband exercises at home, he missed the interaction with other members at the university-based exercise facility: “Like I said, the biggest thing is you know you get out and interaction.” Adam found that the quality of his exercise program was not as consistent or the same length at the gym: “I miss getting out there and doing the gym for a couple of hours every morning. I do what I can here. But it’s not the same kind of workout.” He also found it difficult to exercise at home as the “motivational assistance” he received at the facility was missing.
Accessibility in the online exercise space
Two participants faced barriers when attempting to use the online fitness classes organized by the university-based exercise facility. Chris tried to complete several of the online classes offered by the facility but found it challenging as he did not have any equipment and could only use a small phone to access the class: “It doesn’t really work for me just because a lack of equipment and I only have my little phone to look at it on, so it’s hard to see it.” Matthew also found completing the online classes challenging to access and perform the exercises. He noted,
“I’ve got no equipment and no accessibility to try and use any of them here. . .I mean, I think they’re doing a tremendous job getting that out to people who have done it and been into it, but it’s not that great for me yet.”
Physical activity played an important role in the lives of many participants. The pandemic led to a decline in their daily physical activity due to a variety of factors, including lack of space to exercise safely at home, lack of accessible exercise equipment, lack of the usual motivation they typically draw from fellow gym members and lack of suitable electronic devices to access online video workouts.
Central Theme 3: Living With Social Isolation
Social isolation was challenging for almost all participants in some way. Participants struggled with isolating themselves from their family and friends for several months. When the interviews were completed, participants were in quarantine for approximately 3 to 4 months. Laura described that while she had the support from her children to assist her, she had not left her apartment for several months and said, “. . .and I do not want to be confined. I want to be able to go out. So that’s what scares me about this going on forever because I don’t want to be even further limited than I already am.”
Mary lives alone in her own home and frequently visits friends. She also attends programs hosted by her community center. However, the sudden closure of community programs and the inability to see her friends have been challenging over the last few months. She said:
“Being extra isolated during this time is pretty tough on me, but I try to get outside each day and enjoy the sun. . .while I can. With the snow coming at some point, I know it will get even worse. I try and read a bit now and then and just keep busy a bit.”
Matthew has described social isolation as “very restrictive” and said,
“The biggest difference is that most other people can still get out and go for walks or whatever in the area. Whereas now with this, it’s made it that much more difficult for me to get out and get anything outside of the condo where we live.”
As well, Matthew moved from a freestanding home with a yard and deck to a condominium and combined with the stress of COVID-19, he described it as a “double whammy” and “all of the little things we’re making use of amenities at the condominium building were also taken away.” He described having “more down days where you just feel like, wow, you know, where are we going to go with this.”
Several participants described how they tried to enjoy life and remain connected with their friends and family under quarantine via Skype and texting. For example, Thomas discovered that he could increase his social interactions compared to before the pandemic by using a variety of social media and online platforms, including Facebook, Zoom, and text messaging,
“We’ve been texting, and you know, using Facebook and different methods like that to keep in touch. In some cases, we’ve been more in touch with some people than we ever were when we didn’t have this sickness. I’m fairly adept at technology. We use a lot of methods. You know Zoom for meetings. I’ve kept in touch with many people. I haven’t been totally isolated.”
Adam also found that he kept in touch by text messaging his support system often, “I’m texting a lot with some friends. . .I got my wife and I here too, friends and brother and stuff like that.”
Central Theme 4: Difficulty Obtaining Necessary Medical Supplies
Several participants found it challenging to obtain the necessary medical supplies (ie, for bladder and bowel care) and appropriate personal protective equipment, such as hand sanitizer and gloves. Panic-buying by the public made it difficult for 3 participants to purchase necessities from the grocery store. Mary was 47 years old with a T7 SCI and found it challenging to find the necessary supplies when the pandemic first started:
“The lineups at the grocery stores were so long that I had trouble having to wait so long outside. Then once you’re in and you see everyone is just mass panic buying. . .like what is going on here. The shelves were empty - no soaps or sanitizer or disinfectant wipes. It was crazy to see. I would’ve never expected this to happen.”
Laura used over-the-counter medication for her bowel program that was not available in Canada and had a friend purchase the medication when she was in the United States. As the Canada-United States land border was closed, she could not purchase the medication as she usually would. She says,
[. . .] Because one of the things that I use for my bowel program I get from the United States. They don’t have it here. And it’s just higher strength than they don’t have. They don’t sell it here. And so whenever my friends would go over to the United States, they just pick it up For me, it’s over the counter. But they would just pick it up. And, of course, they’re not going over. And I thought, oh, jeez, if I don’t get that, I’m in trouble.
As a result of the COVID-19 pandemic, Laura was forced to purchase the medication online at a higher price point and increased shipping costs.
Chris was 64 years old and concerned about the health consequences of contracting COVID-19 due to his age (the high-risk factor group being 65) and being immunocompromised due to his SCI. He found that he could order alcohol-based sanitizer; however, he found it a challenge to obtain alcohol-based wipes that he used for intermittent self-catheterization:
“Yes, it’s getting harder. I can’t get those alcohol wipes anymore because they don’t have them [. . .] I’m on my last box right now. I don’t know what I’m going to do after that. So, I guess I’m just going to get a bottle of alcohol if I can find one of those and just use that, but I can’t find them in Wal-Mart or anything either.”
However, one participant already had the necessary personal protective equipment and already had the necessary equipment that he would need. Henry noted that due to his compromised immune system, he was “used to making sure everything is clean and having a small, you know, like a stockpile of sanitizer.” Many participants were immunocompromised due to their SCI, so they were concerned about contracting COVID-19. They described how this altered their daily hygiene practices and access to necessary supplies, including food and medication.
Central Theme 5: Access to Health Care Services and Virtual Care During COVID-19
The COVID-19 pandemic led to the cancellation of many medical appointments at the start of the quarantine in March 2020. Participants described delays in receiving adequate healthcare for their ongoing health conditions, both related and unrelated to their SCI. At the time of the interview, participants were unsure when their previously scheduled medical appointments would begin again and how this would affect their conditions. Some participants described that their conditions had already worsened. Other participants found that telemedicine visits were beneficial in addressing some of their health concerns and allowed them to receive the required care.
Inability to receive necessary medical care
Participants had scheduled visits with general practitioners or specialists cancelled due to the COVID-19 pandemic. Participants were concerned that the backlog of appointments would make it difficult to receive the care they require when medical services reopened. Matthew’s urodynamics appointment at Toronto Rehabilitation Institute was cancelled, and he did not know when his appointment would be rescheduled:
“But, you know, my urodynamics have been cancelled, all that kind of stuff. You know that those things are important for people with SCI to be tested annually. . . When we’ve heard nothing. We got a call that it had been cancelled and that we would get a call from someone to reschedule. But from my knowledge, I don’t believe they’re even scheduling any in-clinic appointments yet at [rehabilitation center]; no better either. Even when they do that, the backlog is going to be so horrendous that who knows how long it’s going to be. . . I was scheduled in May, and that got cancelled because of COVID, but. So now who knows when it’s going to be I’m supposed to go for an appointment with [urologist] for urodynamics test with her in June, but I doubt that, you know, the way things are going that will give even go ahead with that.”
Chris was receiving physiotherapy at a local rehabilitation center after a cat bite injury on his finger. The exercise program he was receiving was helping to restore movement in his finger; however, after the services were closed due to quarantine, he found it challenging to regain movement in his finger again:
“A cat bit me on my hand this November. And it got into the tendon inside my finger, so my finger seized up, and it wouldn’t bend, and it started to really hurt. I had to go to the hospital to clean it all out so it would not get infected. Antibiotics wouldn’t work, and I got to go to therapy at [rehabilitation center]. But you know, with the pandemic, I got cut off, so the rest of the healing is up to me. So, the therapist was helping me get it back to normal, my finger to bend again, and it’s all gone now.”
As well, Chris was about to start ultrasound therapy on his finger to reduce the swelling at the rehabilitation center; however, his first appointment was when all medical appointments were cancelled at the rehabilitation hospital:
“But I was scheduled to start the ultrasound on my finger to get the swelling down. But the day that I was supposed to start, they closed. I got to get the swelling down to use the finger because it doesn’t want to bend on its own. So, the pandemic really screwed me up on that part.”
Telemedicine visits
As in-person medical appointments were cancelled at the beginning of the pandemic, physicians moved to provide telemedicine appointments with patients. Some participants found that they were able to receive some medical care during quarantine via telemedicine visits. Matthew noted:
“Yes, but we did an audio meeting like you and I are doing right now with my physiatrist there. Well, I mean, it’s OK. I mean, it’s not the same, obviously. But, you know, I’ve been fortunate [. . .] That’s what we’re doing right now instead of six months we’re every year. So we’ll see what happens in a year.”
Similarly, Adam has also found that telemedicine appointments have been able to address his health concerns adequately:
“My family doctor is doing everything online. . .like telephone, so and the other couple of doctors I did go to see when it was early on in the pandemic, but the last couple appointments have been on my phone, too, so. So, no problem. I don’t have a problem with stuff like that.”
Also, at the time of his interview, Thomas’ general practitioner did not have established telemedicine appointments, however, Thomas did not have any medical issues that had to be addressed. Still, Thomas expressed his acceptance of telemedicine by stating that he did not have “any difficulty doing this on Zoom. No, I don’t mind the technology whatsoever.” Some participants felt that their health-related issues could be treated via telemedicine visits. However, other participants thought that the cancellation of medical appointments following the COVID-19 pandemic led to a decline in their health and left them unable to get treatment for the health conditions they needed.
Central Theme 6: Reading Between the Lines: Fighting COVID-19 Misinformation
Participants felt they received contradicting advice from the different levels of government via various media sources (ie, television, online news articles and radio). Matthew felt that he received many mixed messages from the media and found that daily press conferences on the COVID-19 pandemic were not helpful and “people’s fear of the fear is far greater than they have the fear of the illness.” Matthew described the mixed messages he received:
“I think the whole issue around information on COVID is extremely disjointed. Extremely contradictory. Right from the get-go, we have received nothing but mixed messages right from, in particularly, our medical experts. Every day it changes, ahh. . .and everything is worst case scenario, worst case scenario. And again, I believe our medical people have bred way too much fear into the public. Quite frankly. There is thought there is no one source that you can go to or say that you can get a clear answer on anything. Every medical expert has their own interpretation of everything that’s going on, right from how you communicate it, and how it gets passed on to the value of gloves, masks on and on and on and on and on. There is. . .Everyone has their own opinion.”
Thomas described the messages he has heard from the media as “too much and too confusing.” He mentioned that with respect to messages about preventing the spread of COVID-19, there was “too much being researched to know what is true and proper [. . .] It’s a zoo to listen to. Who’s right, who’s wrong. Everybody’s got an answer, but nobody’s got the true answer.” Adam also described that once the pandemic began, there was a lot of contradicting information being released about masks and gloves, making it challenging to know whose advice to follow during such a serious situation. Adam noted that the information on preventing COVID-19 was “all over the place” and described:
“And so one minute. . .at the beginning, masks. . .they didn’t say you needed masks. Now they’re telling me to wear masks and everything else. So, I mean. . .So, I just I wear the mask now. Right from the beginning, I wore masks. You know, if I had to go out, my wife made a whole bunch of them. So, we have our own. Just like I said, I put your trust in the people that the educated people that are put in that position for telling you what’s going on. And I mean, that’s all you can do, right?”
Participants felt like the mixed messaging about the prevention of COVID-19 made them unsure about what practices they should be following and how seriously they should be following social distancing advice and guidelines, especially as the quarantine continues in the future.
Discussion
This study investigated the lived experience of individuals with SCI during the COVID-19 pandemic in Ontario, Canada. The COVID-19 pandemic holds additional risks for people with SCI due to physiological vulnerabilities and pre-existing challenges with physical independence and community participation. There are clear recommendations that have emerged on the needs of people with disabilities, such as SCI, during the pandemic, but few studies focused exclusively on SCI.
To better understand how the pandemic affects this particular population, it is important to learn about the lived experiences of individuals with an SCI during the pandemic. The qualitative research design of the study provided the opportunity to gain significant insights into the lived experiences of individuals living with SCI during a pandemic and having to remain under quarantine for several months. This was one of the first studies investigating the lived experience of individuals with SCI during the COVID-19 pandemic, specifically within Ontario, Canada. The pandemic affected each participant in their own way, albeit with common threads and specific factors affecting some participants more than others.
Participants with caregivers shared their concerns and fear of their caregiver contracting COVID-19. Participants with personal attendants who were responsible for assisting with activities of daily living were fearful that their attendant might be a carrier of COVID-19, thereby increasing their own risk of contracting the virus. Further, participants also described challenges in finding a new caregiver if one of their current caregivers had a positive COVID-19 diagnosis.
Participants found it challenging to stay physically active in isolation, describing several barriers, including lack of access to specialized equipment, small living spaces that were not conducive to physical activity and difficulties staying motivated to exercise. It is well-established that physical activity is critical for the health and well-being of individuals with SCI. 39 Participants noted that they were placed in a vulnerable position as they could not be physically distanced from their attendants due to the type of assistance required. Participants who had a family member act as their caregiver were also concerned. If their family member contracted COVID-19 and had to self-isolate from the participant (due to their increased vulnerability to COVID-19), they would not have the funds to hire a caregiver to assist them.
Individuals with SCI have an increased prevalence of obesity and cardiometabolic disease, potentially due to decreased muscle mass, slower metabolism and decreased levels of physical activity.40 -43 While physical activity is important for individuals with SCI to reduce the risk of obesity and cardiometabolic disease, it also plays a critical role in mitigating the impact of isolation and loneliness and maintaining a positive peer network. 39
Many participants with SCI discussed the adverse effects of the social isolation caused by quarantine during the COVID-19 pandemic. During natural disasters and public health emergencies, individuals with SCI encounter “increased barriers to mobility and maintaining physical and mental health.” 44 Emerging research has found that COVID-19 has caused elevated levels of psychological distress.45,46 Even before the pandemic, individuals with disabilities (including those with SCI) typically faced barriers to successful social relationships due to neurological impairment (ie, impaired mobility, bowel and bladder dysfunction), secondary health complications (ie, UTI and pressure injury), and environmental factors. 47
The quarantine associated with COVID-19 exacerbated this social isolation. 48 While social isolation is necessary from a public health perspective, individuals with disabilities face increasing social isolation and loneliness, which may lead to long-term health effects. 49 Previous research on the impact of natural disasters supports our finding that the mental health impact on individuals with disabilities may be exacerbated. 48
In contrast, several participants in our study also found new ways to stay connected with friends and family members using social media and other videoconferencing platforms to combat social isolation during quarantine. Several participants also decided to start or re-start hobbies to keep busy during quarantine. Dalise et al 50 conducted telephone interviews with individuals with physical disabilities living in Italy. Interestingly, participants in the study were only mildly affected by COVID-19. Compared with the non-disabled population, individuals with physical disabilities maintained good coping skills and stayed resilient throughout the quarantine. 50 One of the most important goals for those with a disability is actively engaging in normal social roles and returning to family and community life.51,52 However, several factors may lead to an increased risk of social isolation and other poor social health outcomes. For instance, secondary health conditions may negatively impact social opportunities for individuals with SCI, including neuropathic pain, pressure injuries, bowel and bladder issues, and mental health issues.53,54 As well environmental barriers to social and community participation may also adversely impact social participation post-injury. Our findings indeed suggest that the risk of social isolation was increased in those with SCI during the pandemic. However, some people minimized this isolation and loneliness through online interactions and hobbies. Further research is required to determine the complex interaction between the COVID-19 quarantine and social isolation in individuals with SCI.
Several participants could not receive their necessary medical care due to the cancellation of many in-person appointments, medical procedures, and laboratory tests. Individuals with SCI have unique medical concerns that are often overlooked in emergencies, highlighting the need for additional literature on perceived access to medical care. 55
Most participants in our study found that telemedicine services were adequate and could promptly address medical issues with their physicians. Telemedicine for individuals with SCI has also been found to have many advantages, including limiting transportation costs, saving travel time, and limiting the spread of infection in vulnerable populations. 56 Although there are barriers to providing telemedicine services to individuals with SCI that must be addressed, telemedicine can be considered an alternative to in-person healthcare to support the care of individuals with SCI in the community during COVID-19. Telemedicine will likely be used at an increased rate post-COVID-19, even as in-person visits resume.44,57,58
While the media (television, radio, and social media) has disseminated guidance on physical distancing, hand washing and the importance of wearing face masks for non-disabled individuals, similar messaging specifically for individuals living with a disability is severely lacking. Media campaigns and messages for individuals with disabilities are critical as they may face challenges donning and doffing face masks, adequately washing their hands and maintaining physical distance from others. As more than 1 billion individuals live with disabilities worldwide, there is an important need to ensure that individuals living with disabilities are not forgotten.
Limitations
Despite the strengths of this study, there are some limitations. Most participants lived in medium-sized cities outside the Greater Toronto and Hamilton Area. There may have been geographic variations in the type of restrictions that participants faced compared to those living in larger cities that were not captured in our study. Further, the sample size was relatively small and is likely not representative of the broader group of individuals with traumatic SCI. Small sample sizes are a common challenge within the field of SCI internationally due to the relatively small prevalence of traumatic SCI and well-known issues in recruitment and compliance.59 -61 The current sample likely represented a healthier group of individuals with traumatic SCI as most participants were recruited from an accessible exercise community program. Therefore, it may not reflect the experiences of individuals with an SCI who lived more sedentary lives or with a higher level of injury. Additionally, as this study was conducted within Ontario, we cannot generalize the experiences to other individuals with SCI who reside within other provinces in Canada or other countries.
Conclusions
This study is an essential first step in exploring the impact of the COVID-19 pandemic on individuals with SCI. Overall, the findings of this study contribute to a greater understanding of the impact of the pandemic and its associated restrictions on individuals with SCI. Building on this research, future studies are required to explore the effects of the COVID-19 pandemic on individuals with SCI nationally. Collectively, this research enhanced our understanding of the impact of the pandemic and provided insights on how to better support and respond to the specific and unique needs of individuals with SCI and their families during a public health emergency and quarantine conditions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.