
Abstract
Purpose: This study investigated the impact of the COVID-19 pandemic on homecare service use among individuals with physical disabilities, stratified by age, sex, and mental health conditions. Methods: Monthly utilization of personal support and nursing services was assessed using linked health administrative databases from ICES in Ontario, Canada, over two periods: pre-pandemic (March 2015 to February 2020) and during the pandemic (March 2020 to June 2022). Predictive Autoregressive Integrated Moving Average (ARIMA) models were used to estimate changes in service use. Results: During the pandemic, personal support service use declined significantly across multiple subgroups with some groups experiencing greater impacts. Significant decreases were observed in 78.5% of months for males, 14.3% for females, 78.5% for individuals aged 65 years and younger, 17.9% for those older than 65 years, and 78.5% for individuals with mental health conditions. In contrast, nursing service use increased significantly, with significant increases observed in 85.7% of months for males, 60.7% for females, 60.7% for those aged 65 years and younger, 17.9% for those older than 65 years, 85.7% for individuals with mental health conditions, and 28.6% for those without mental health conditions. Conclusion: The findings highlight substantial variation in the pandemic’s impact across subpopulations, with certain groups disproportionately affected. Targeted strategies are needed to mitigate these disparities and ensure equitable access to homecare services. Further research is warranted to explore the long-term implications and the underlying factors contributing to these differences.
Introduction
The COVID-19 pandemic had an unprecedented impact on healthcare utilization in Canada, especially on homecare services.1-4 Disruptions in homecare services were previously quantified in two studies conducted in Canada, one in the general adult population and another among adults with dementia.1,2 In the general adult population compared to the pre-pandemic period (March 2019-February 2020), a 18.9% decrease in personal support services, and 8.5% decrease in nursing services was found in April 2020. 2 However, in adults with dementia, although personal care services decreased by 16% in April 2020, nursing service rates did not decrease, but instead increased significantly by 14% in September 2020 compared to 2019 levels. 1 These studies found the pandemic impacted homecare services and the extent and direction of impact varied by population.1,2
Individuals with physical impairments often rely on homecare services as it allows them to continue living in their own homes, provides families with respite or employment support for caregivers, while facilitating client independence and improving their quality of life.5,6 Over 25% of Canadians experience a disability, 7 hence understanding the impact the pandemic had on these individuals in a Canadian context is important. To begin to understand the impact on homecare services due to the pandemic, it is important to investigate homecare service utilization across different subpopulations within the physical disability population. Older adults, over the age of 65, with physical disabilities, may experience increased vulnerability to the COVID-19 virus 8 and/or differences in availability of unpaid caregiving support,9,10 hence their homecare services may be impacted differently. Similarly, literature has outlined differences in caregiving support and homecare service utilization and needs between gender and sex, therefore, the pandemic may have impacted homecare services in males and females differently.11,12 Furthermore, those with both a physical disability and mental health concerns during the pandemic may require additional homecare supports or specialized services.1,13 It is imperative to quantify the differences across patient subpopulations to determine if certain groups were more vulnerable to the impacts of the pandemic and at greater risk of experiencing reduced care. Once these are identified, strategies or recommendations can be created to improve care for individuals who may have been disproportionately impacted. Quantifying current homecare services use and shifts may also provide insight to the different needs for various subpopulations. To our knowledge, no previous studies have investigated homecare in different subpopulations with physical disabilities during the pandemic in Canada using administrative health data. The purpose of this paper was to investigate the impact the pandemic had on homecare service use in individuals with physical disabilities stratified by age, sex, and mental health conditions. We hypothesize that the COVID-19 pandemic has led to varying impacts on home care service utilization across different subpopulations causing disparities in access and care.
Methods
This was a stratified repeated cross-sectional study using linked health administrative databases in Ontario, Canada. We used data from March 2015 to June 2022 inclusive, with the pre-pandemic period designated as March 2015 to February 2020 and the pandemic observation window designated as March 2020 to June 2022. A representative cohort of persons with physical disability population was created with data from individuals with traumatic or non-traumatic spinal cord injury/disease. Spinal cord injury/disease appropriately represent the physical disability population due to their profound impact on mobility, daily functioning, and the need for specialized medical care, which reflects the diverse challenges faced by individuals within the broader spectrum of physical disabilities. We evaluated homecare personal support services and nursing visits. Data were stratified by sex, age and mental health conditions.
Data Source
Data for this study was obtained from ICES (formerly named the Institute for Clinical Evaluative Sciences), an independent, non-profit research institute funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). As a prescribed entity under Ontario’s privacy legislation, ICES is authorized to collect and use healthcare data for the purposes of health system analysis, evaluation, and decision support. Secure access to these data is governed by policies and procedures that are approved by the Information and Privacy Commissioner of Ontario. The initial data processing, de-identification, extraction, cleaning, and linkage were performed by ICES using standardized protocols and statistical programming within their secure environment. The authors then extracted the data from the ICES secure environment using SAS were further data processing, cleaning and linkage, a well as statistical analyses was conducted.
The cohort was created using the Discharge Abstract Database (DAD) to identify cases of traumatic spinal cord injury, and the National Rehabilitation System (NRS) database to identify cases of non-traumatic spinal cord injury. The Home Care Database (HCD) was used to identify publicly funded homecare services. Patient characteristics, specifically socio-demographics (age, sex, and postal code) were extracted from the Registered Persons Database (RPDB). History of mental health was identified in DAD and Ontario Health Insurance Plan (OHIP) records based on flags in multimorbidity macro for mood disorders and other mental health conditions. 14 The presence of either or both conditions indicated that an individual had a history of mental health conditions.
Cohort
A previous ICES study investigating healthcare utilization and identified a cohort of 5754 with traumatic or non-traumatic spinal cord injury, who had their first admission and discharge from acute hospitalization in the DAD or inpatient rehabilitation in NRS between April 1, 2004, and February 28, 2014. Additional details about the cohort can be found in Senthinathan et al. 15 The original cohort was then linked to the HCD.
Outcomes
The main outcome measure of interest was person-level data for monthly homecare utilization, which included monthly total number of personal care services, and nursing visits. Based on how visit information was captured, personal care services were recorded in hours per 100 persons; whereas nursing visits were recorded as number of monthly visits per 100 persons.
Data Analysis
Initial descriptive statistics were conducted to describe the cohort’s socio-demographics and clinical characteristics. Pre-pandemic differences between different subpopulations’ (males vs females; those 65 and under vs those over 65; those with mental health conditions vs those without mental health conditions) homecare utilization was calculated. Relative differences between the subpopulations pre-pandemic and pandemic homecare utilization were also calculated by taking the difference between pandemic and pre-pandemic utilization rates, dividing by the pre-pandemic rate, and expressing the result as a percentage change.
For each type of homecare service (1. personal care services; and 2. nursing visits), an Autoregressive Integrated Moving Average (ARIMA) model was fitted to the pre-pandemic values (March 2015 to February 2020) to forecast the expected values and their 95% confidence intervals (CIs) during the pandemic (March 2020 to June 2022). ARIMA modelling is a common statistical technique used for time series forecasting. 16 All observed values that fell outside of the range of the 95% CIs for the forecasted values were considered statistically significant. 16 For all ARIMA models, non-stationarity and seasonality were accounted for when required by differencing the series (i.e., calculating the difference between the current time period and the previous time period). Stationarity (defined as a constant mean and variance over time) was confirmed using the augmented Dickey–Fuller test. 17 We identified the model orders (autoregressive or moving average terms) using the autocorrelation function (ACF), partial ACF and inverse ACF plots, as well as white noise probability plots and Ljung–Box χ2 tests for white noise. A percentage of number of months with services outside of the expected range was calculated for the post-pandemic period. As a sensitivity analysis the ARIMA models were run for each subpopulation for overall homecare service utilization by adding personal care services hours to the number of nursing visits to create an amalgamated homecare service unit. This was done to test if there was an overall change to homecare utilization in any of the subpopulations. All analyses were completed using SAS® software, version 9.4 (SAS Institute Inc., Cary, NC, USA, 2013).
Ethical Approval
ICES is a prescribed entity under Ontario’s Personal Health Information Protection Act (PHIPA). Section 45 of PHIPA authorizes ICES to collect personal health information, without consent, for the purpose of analysis or compiling statistical information with respect to the management of, evaluation or monitoring of, the allocation of resources to or planning for all or part of the health system. Projects that use data collected by ICES under section 45 of PHIPA, and use no other data, are exempt from further REB review. The use of the data in this project is authorized under section 45 and approved by ICES’ Privacy and Legal Office.
Results
A total of 3381 from the original cohort of 5754 individuals who received homecare services and comprised the cohort for this study. Clinical and demographic details are outlined in Table 1.
Demographic Characteristics.
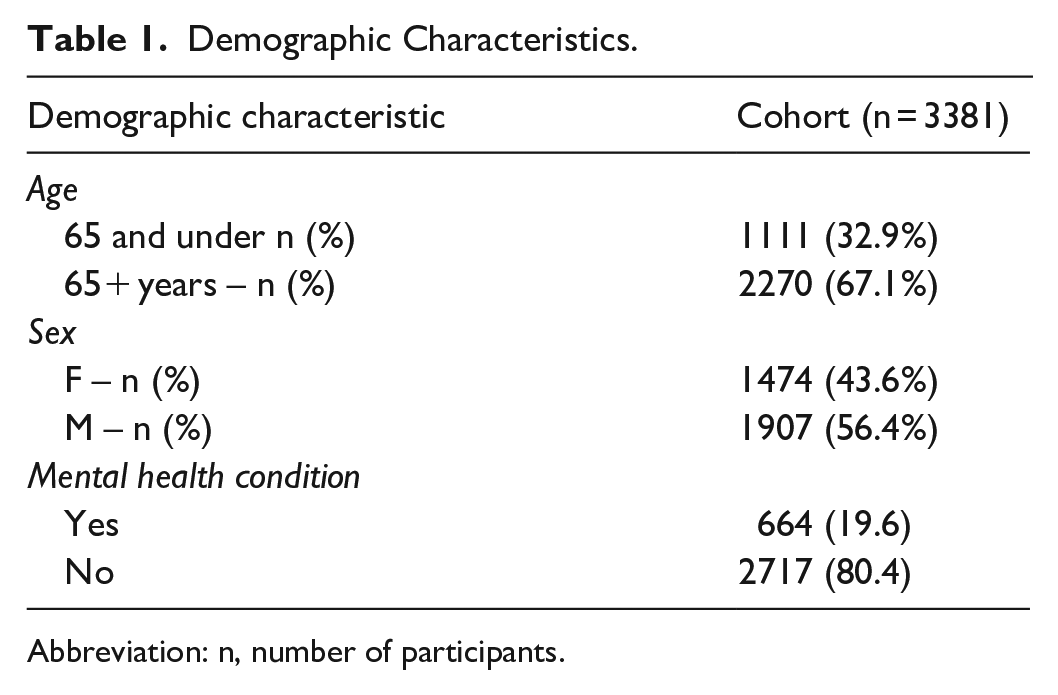
Abbreviation: n, number of participants.
Pre-Pandemic Baseline
During the pre-pandemic period, females, those over the age of 65, and those without a diagnosed mental health condition had significantly higher (P < .0001) utilization of personal support services compared to males, those 65 and under, and those with mental health conditions respectively (Table 2). Males, those 65 and under and those with mental health conditions had significantly higher (P < .0001) utilization of nursing homecare services during the pre-pandemic period compared females, those over the age of 65, and those without mental health conditions respectively (Table 2) .
Average Monthly and Statistical Differences in Personal Support and Nursing Homecare Services Utilization Per 100 Persons During the Pre-Pandemic and Pandemic Period for Cohort.
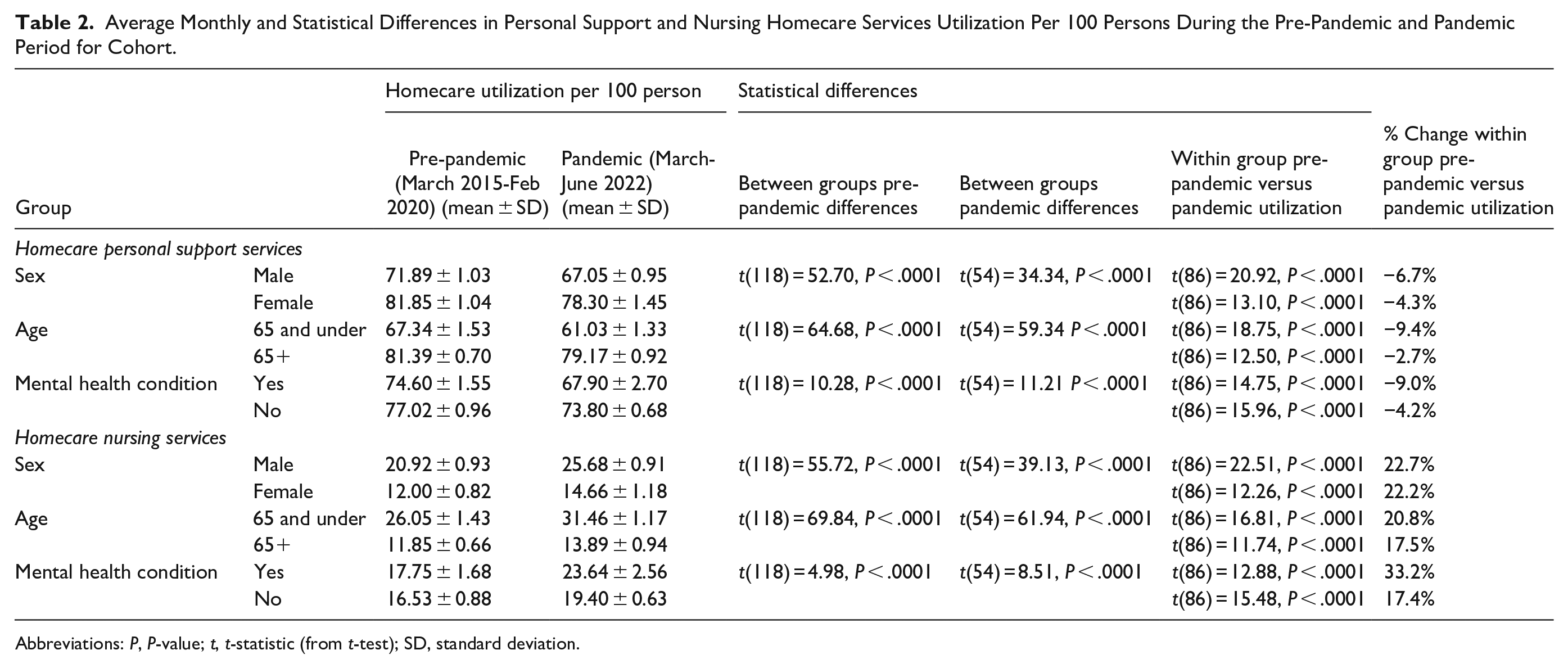
Abbreviations: P, P-value; t, t-statistic (from t-test); SD, standard deviation.
Pre-Pandemic Period Compared to Pandemic Period
Sex (Male vs Females)
Males experienced a significant 6.7% decrease (P < .0001), and females experienced a significant 4.3% decrease (P < .0001) in personal support services from the pre-pandemic to the pandemic period (Table 2, Figure 1a). For males, personal support service use was lower than expected in 22 out of 28 months (78.5%) during the pandemic period from April 2020 to February 2022 with the exception of May 2021 (Table 3, Figure 2a). Females experienced a lower than expected personal support service use in 4 out of 28 months (14.3%), specifically from December 2020 to March 2021 (Table 3, Figure 2b).
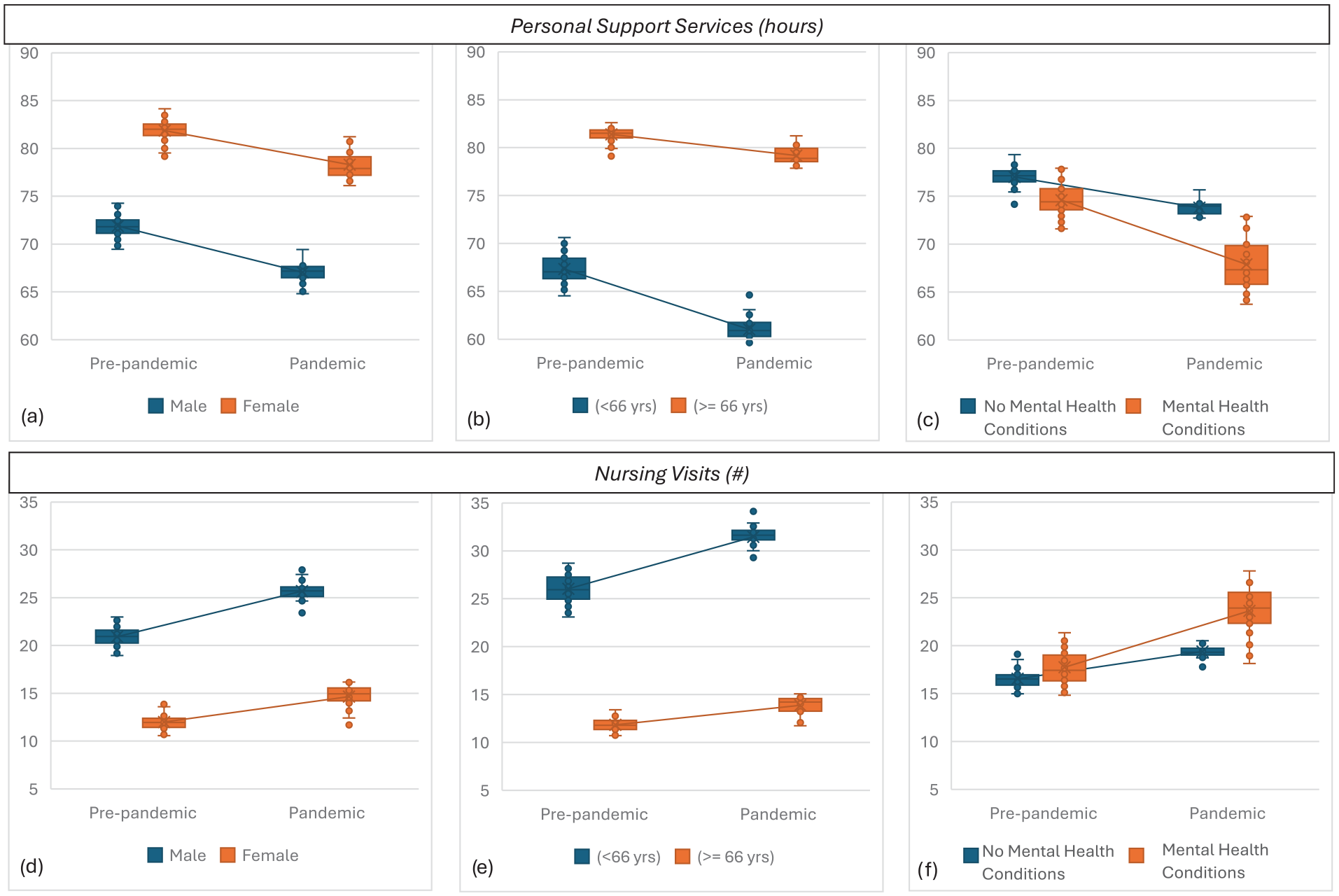
Average monthly rate of homecare services pre-pandemic versus pandemic for personal support services hours by (a) sex, (b) age and (c) by mental health condition status; and number of nursing serevice visits by (d) sex, e0 age and (f) mental health condition status.
Personal Support Services Stratified by Sex.
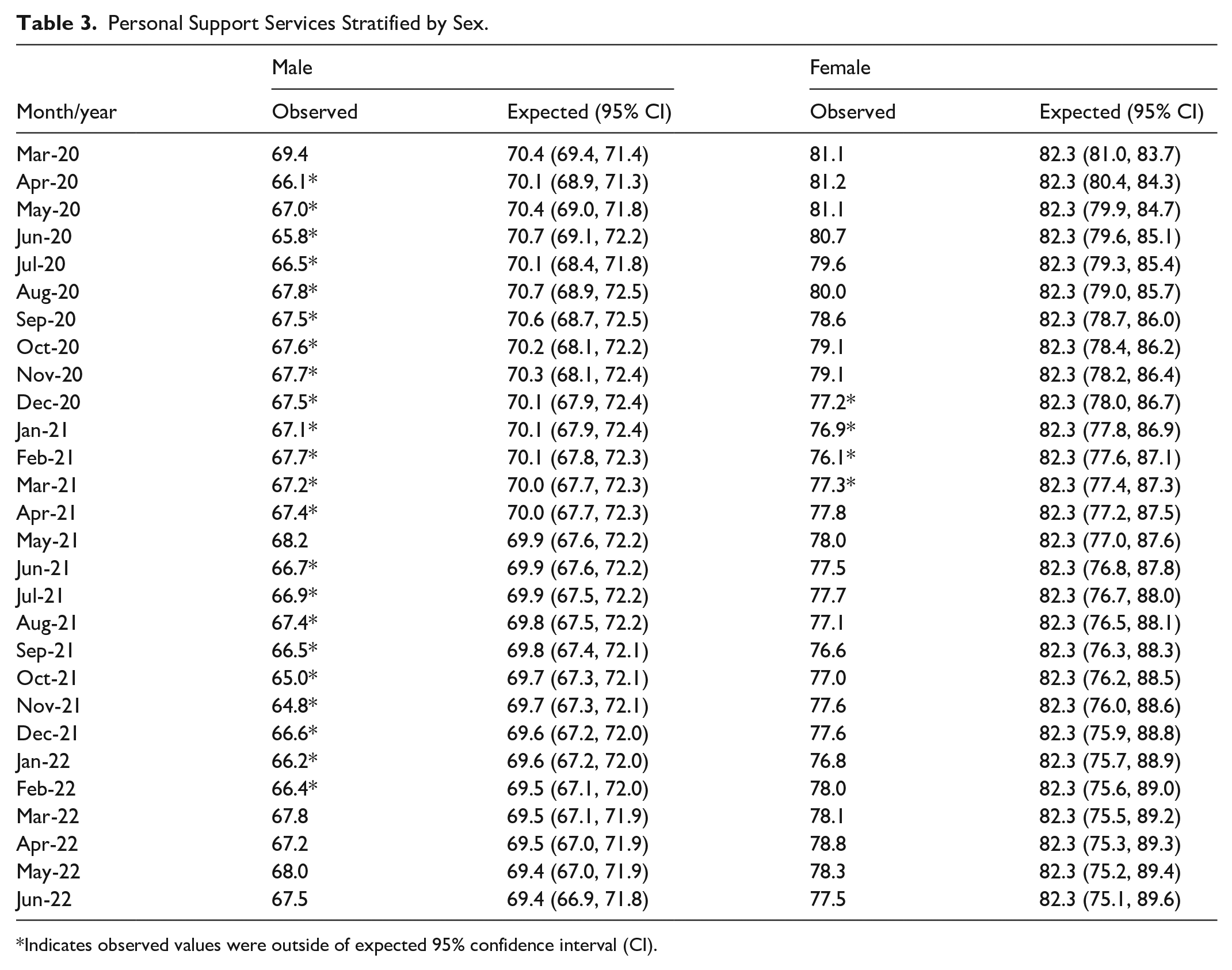
Indicates observed values were outside of expected 95% confidence interval (CI).
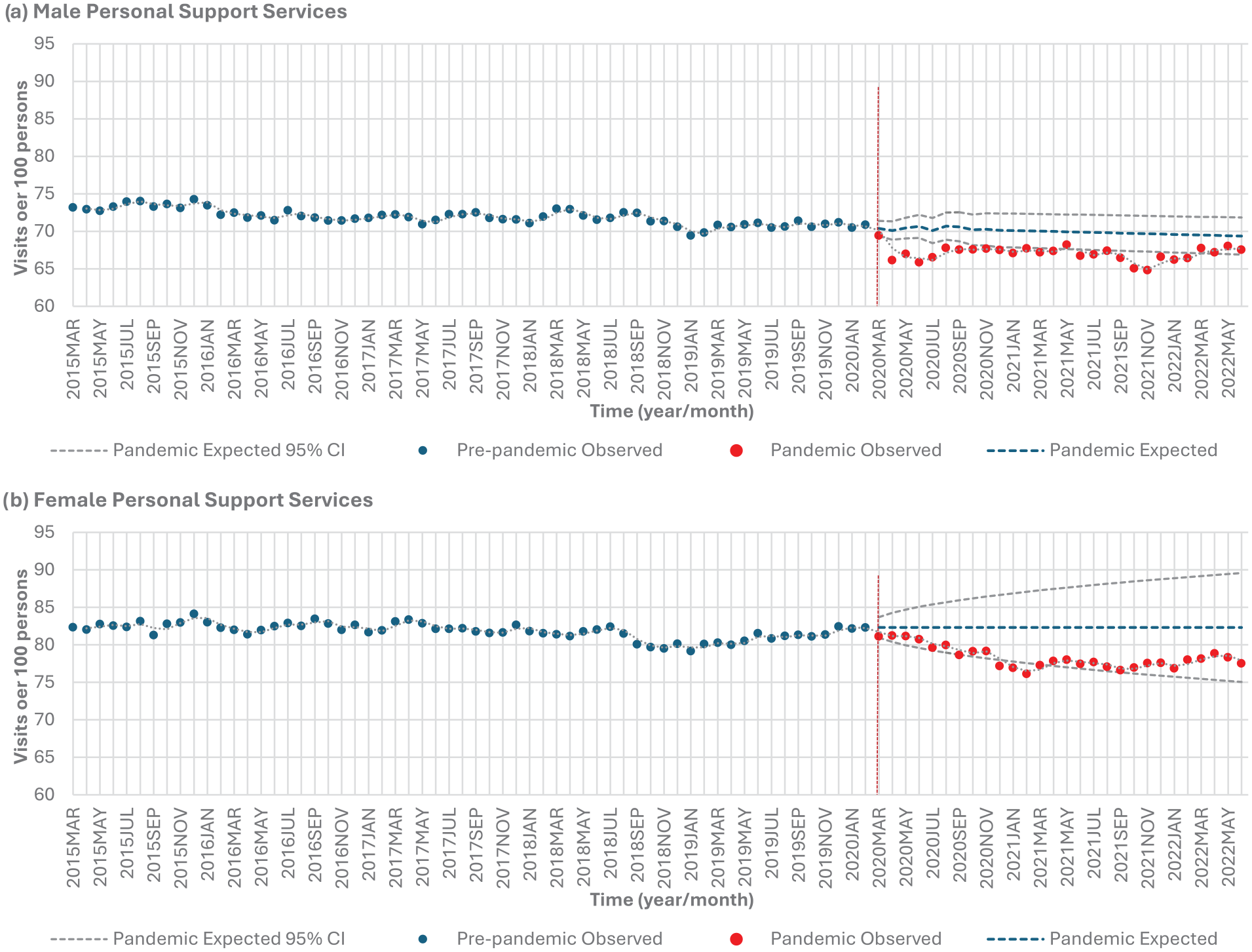
Homecare personal support services stratified by sex: (a) males and (b) females.
Both males and females experienced approximately a significant 22% increase (P < .0001) in nursing services from the pre-pandemic to pandemic period (Table 2, Figure 1d). For males, nursing service use was higher than expected in 24 out of 28 months (85.7%) during the pandemic period from March 2020 to February 2022 (Table 4, Figure 3a). For females, higher than expected use of nursing services occurred in 17 out of 28 months (60.7%), spanning from June 2020 to October 2021 (Table 4, Figure 3b).
Nursing Services Stratified by Sex.
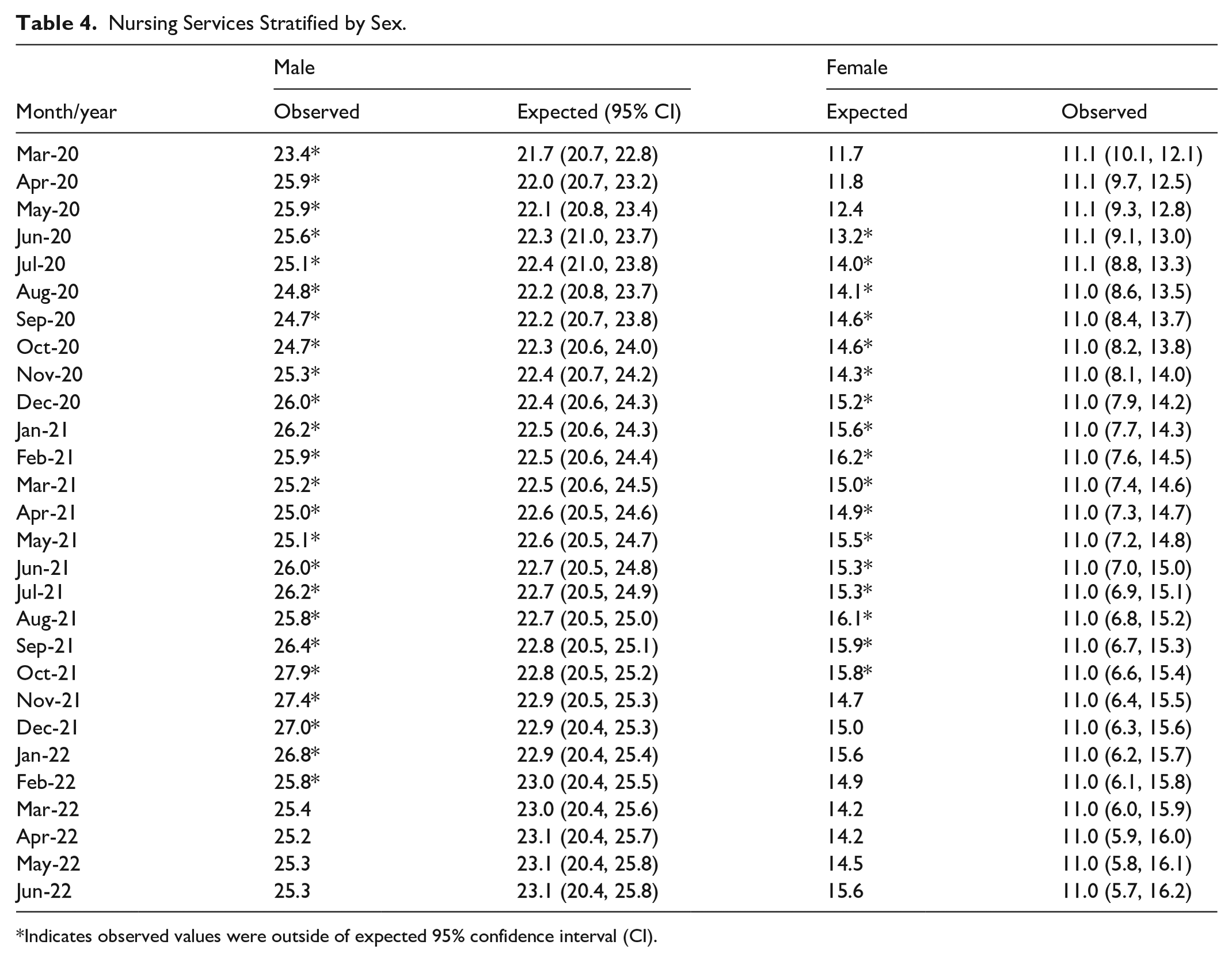
Indicates observed values were outside of expected 95% confidence interval (CI).
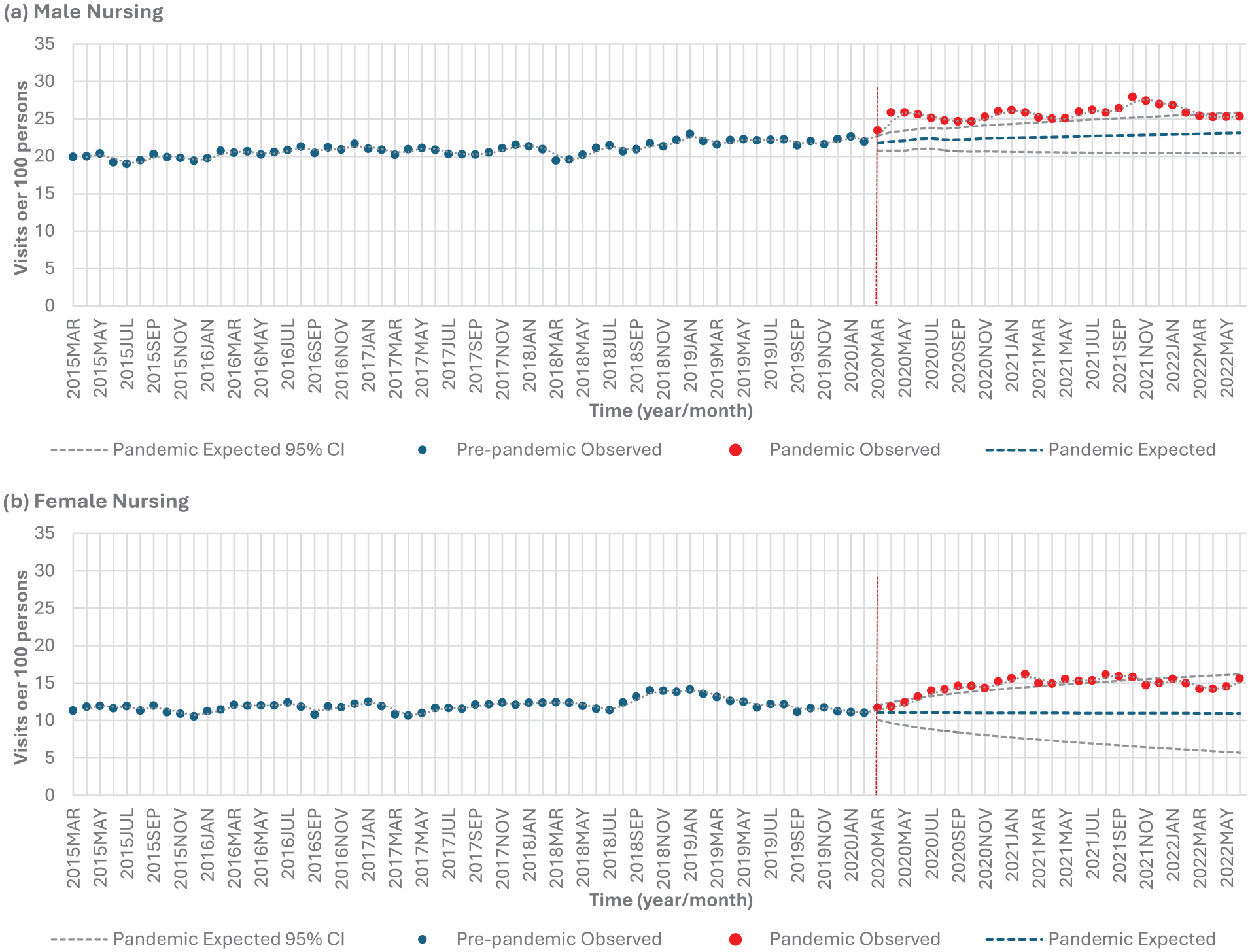
Nursing services stratified by sex: (a) males and (b) females.
Age (65 and under vs 65+)
Those 65 and under experienced a significant 9.4% decrease (P < .0001), and those above 65 experienced a significant 2.7% decrease (P < .0001) in personal support services from the pre-pandemic to pandemic period (Table 2, Figure 1b). Individuals aged 65 and under experienced lower than expected personal support service use in 22 out of 28 months (78.6%) during the pandemic period from April 2020 to January 2022 (Table 5, Figure 4a). Individuals over 65 experienced lower than expected use in 5 out of 28 months (17.9%) (July 2020, September 2020, and December 2020 to February 2021) (Table 5, Figure 4b).
Personal Support Services Stratified by Age.
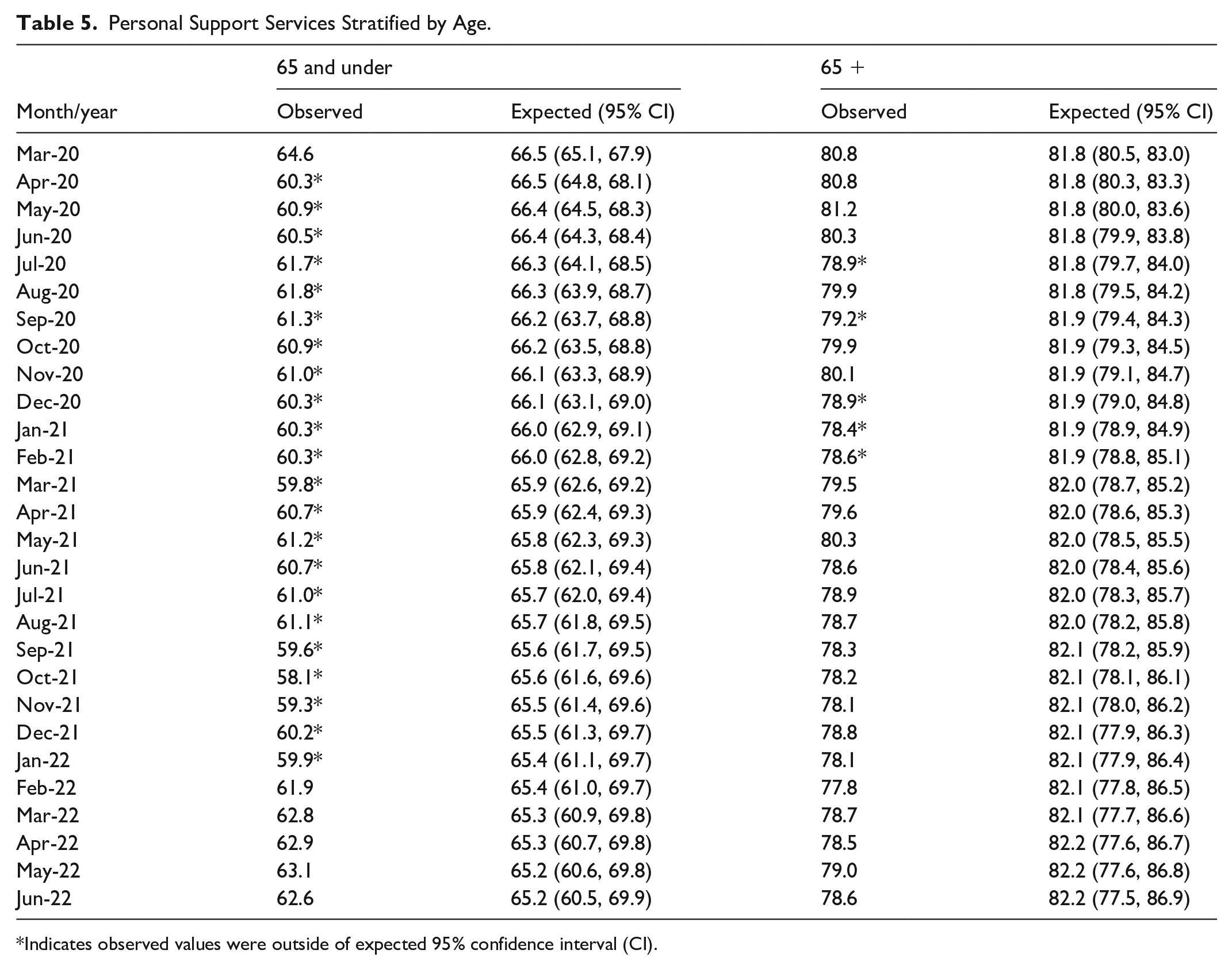
Indicates observed values were outside of expected 95% confidence interval (CI).
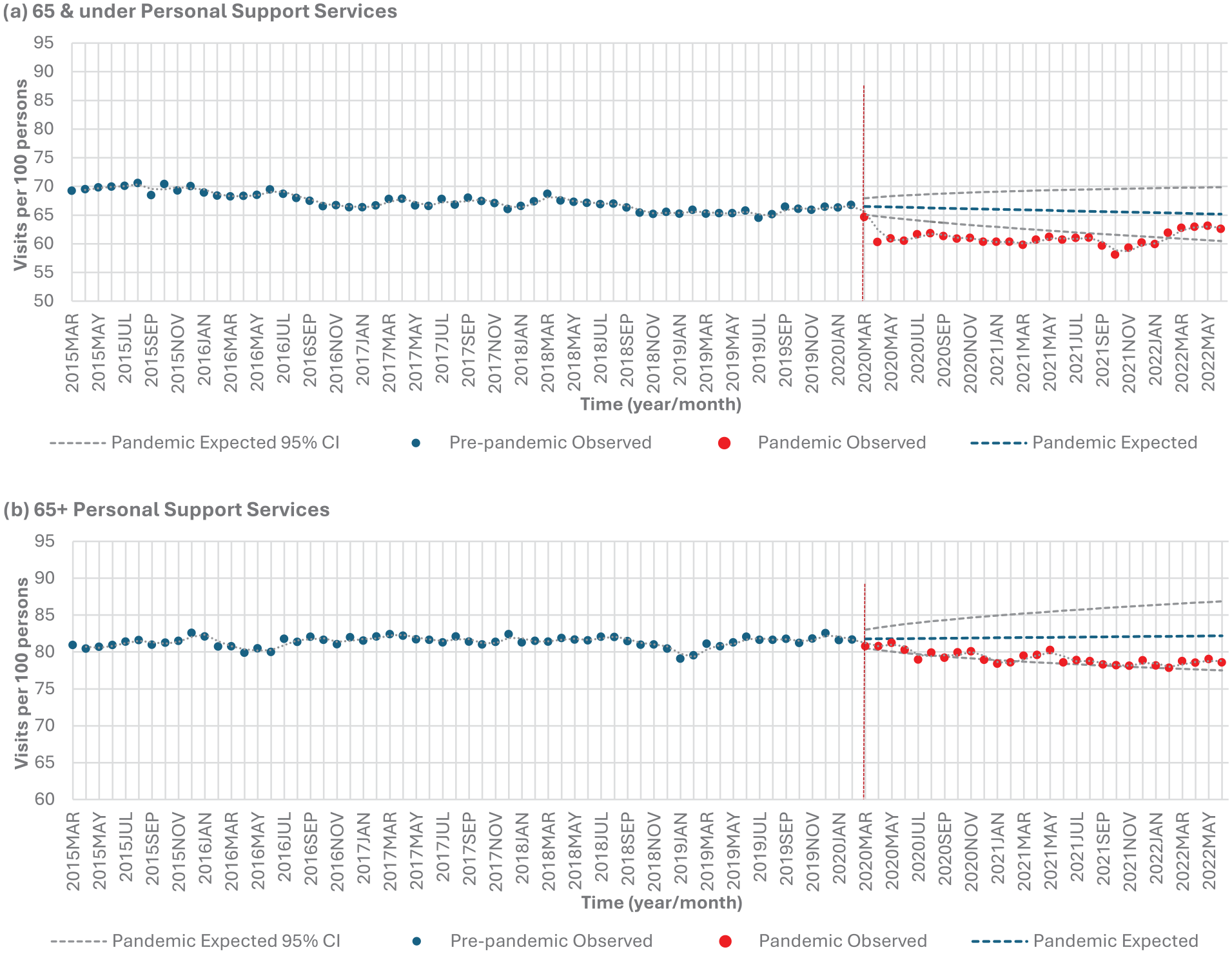
Homecare personal support services stratified by age: (a) 65 and under versus (b) 65+.
Those 65 and under experienced a significant 20.8% increase (P < .0001), and those above 65 experienced a significant 17.5% increase (P < .0001) in nursing services from the pre-pandemic to pandemic period (Table 2, Figure 1e). Individuals aged 65 and under experienced higher than expected nursing service use in 17 out of 28 months (60.7%) during the pandemic period (April 2020 to March 2021, June 2021 and September to December 2021) (Table 6, Figure 5a). Individuals over 65 experienced higher than expected use in 13 out of 28 months (46.4%) (April 2020, July to September 2020, December 2020 to February 2021, June to October 2021, and January 2022) (Table 6, Figure 5b).
Nursing Services Stratified by Age.
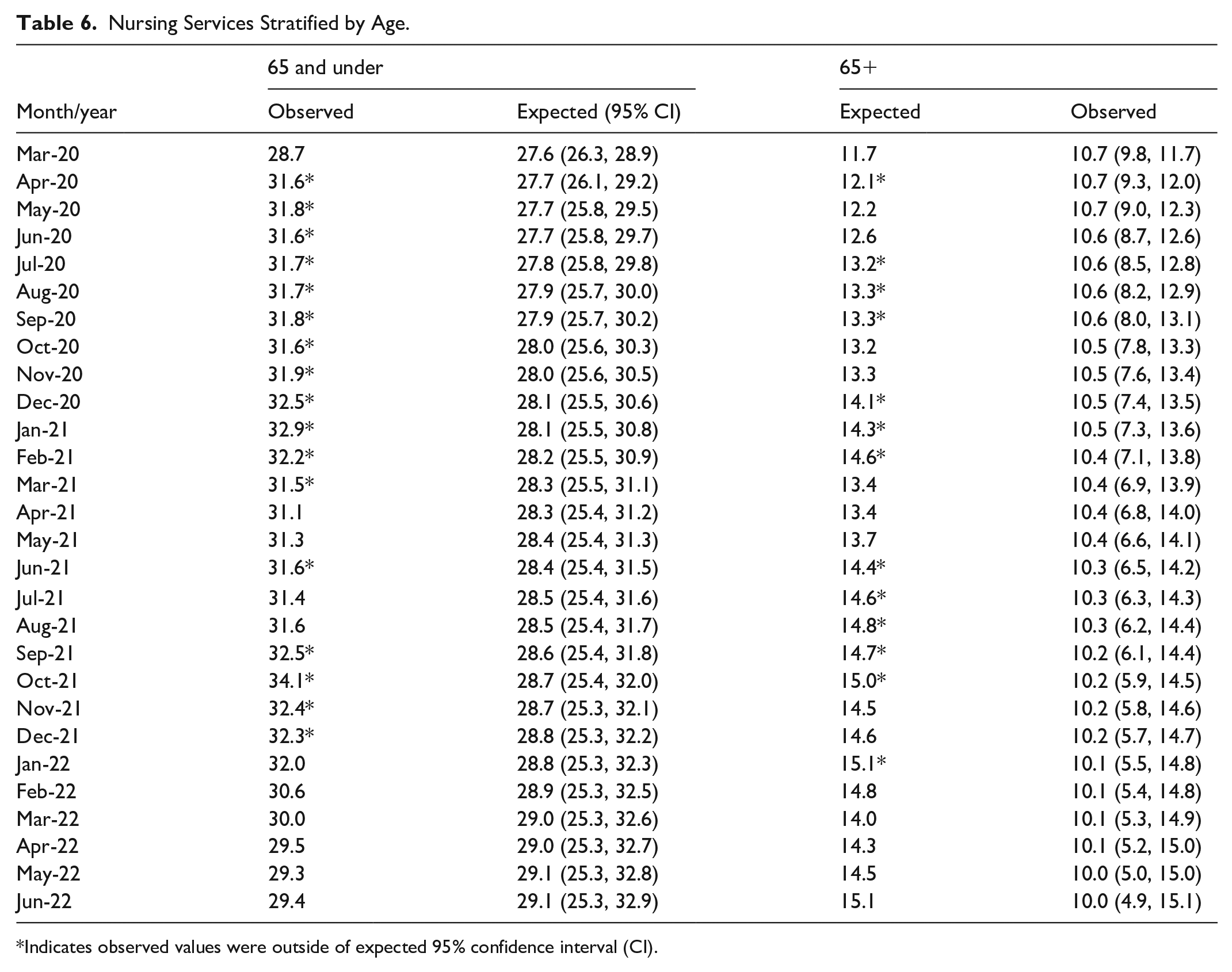
Indicates observed values were outside of expected 95% confidence interval (CI).
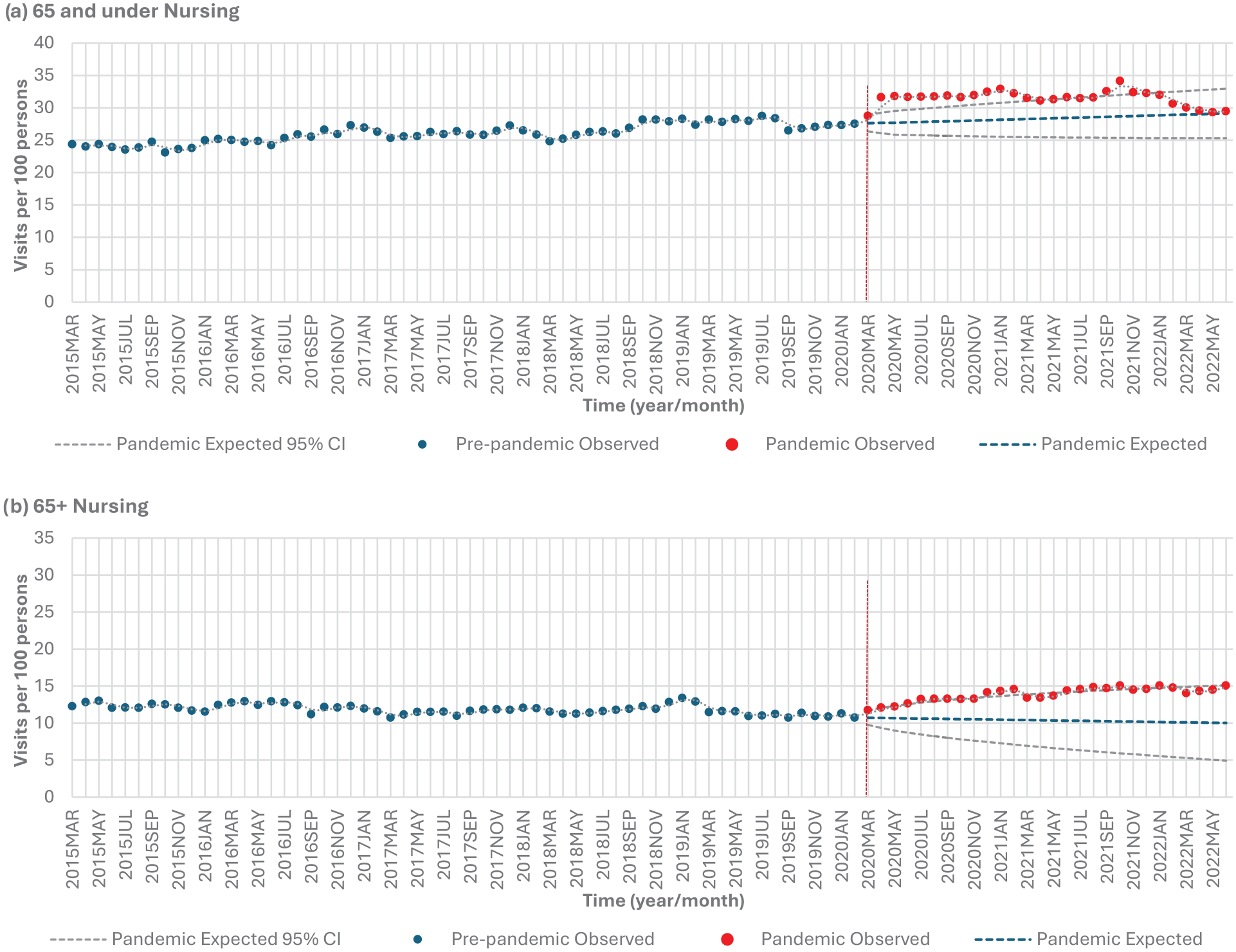
Homecare nursing services stratified by age: (a) 65 and under versus (b) 65+.
Mental Health (Those With Mental Health Condition and Those Without Mental Health Condition)
Those with mental health conditions experienced a significant 9.0% decrease (P < .0001), and those without mental health conditions experienced a significant 4.2% decrease (P < .0001) in personal support services from the pre-pandemic to pandemic period (Table 2, Figure 1c). Those with mental health conditions experienced lower than expected personal support service use in 22 out of 28 months (78.6%) during the pandemic period (April 2020 to February 2021, June 2021, September to November 2021, January to February 2022, and June 2022) (Table 7, Figure 6a). (Table 7, Figure 6a). Those without mental health conditions had no months that experienced a lower than expected range in personal support services (Table 7, Figure 6b).
Personal Support Services Stratified by Mental Health Condition.
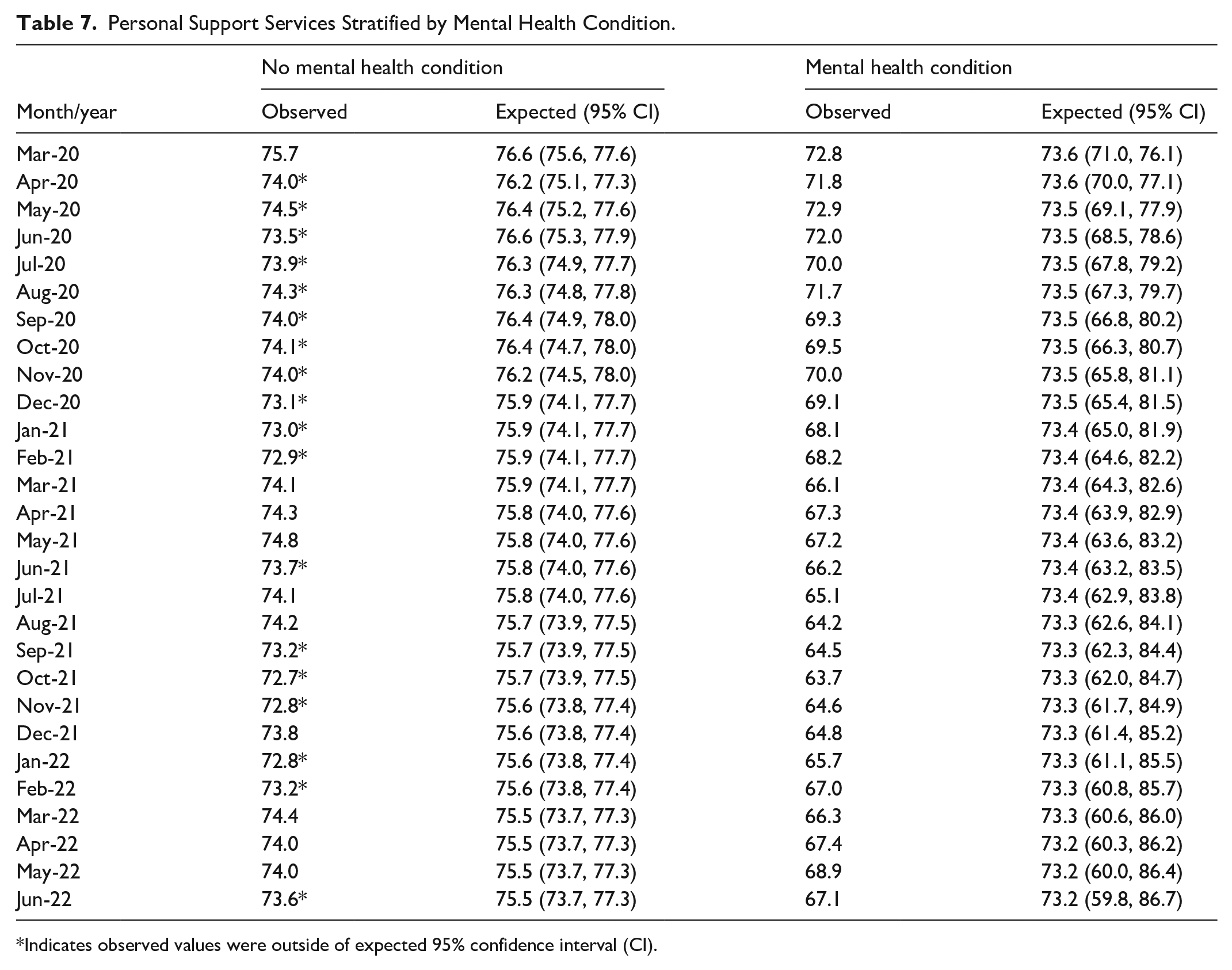
Indicates observed values were outside of expected 95% confidence interval (CI).
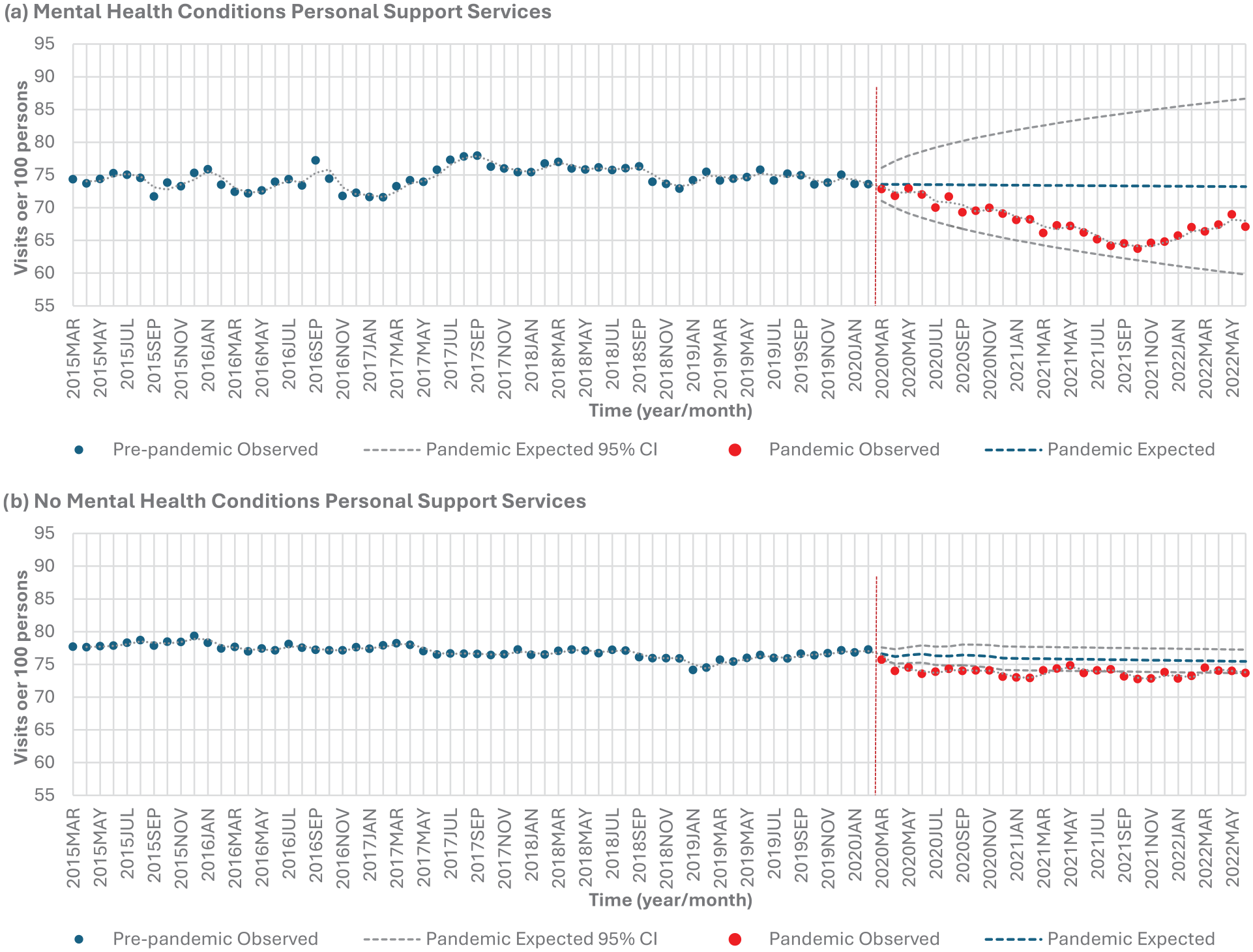
Homecare personal support services stratified by mental health: (a) mental health conditions versus (b) no mental health conditions.
Those with mental health conditions experienced a significant 33.2% increase (P < .0001), and those without mental health conditions experienced a significant 17.4% increase (P < .0001) in nursing services from the pre-pandemic to pandemic period (Table 2, Figure 1f). Those with mental health conditions experienced higher than expected nursing service use in 24 out of 28 months (85.7%) during the pandemic period from July 2020 to June 2022 (Table 8, Figure 7a). Those without mental health conditions experienced higher than expected use in 8 out of 28 months (28.6%) (March to July 2020, and December 2020 to February 2021) (Table 8, Figure 7b).
Nursing Services Stratified by Mental Health Conditions.
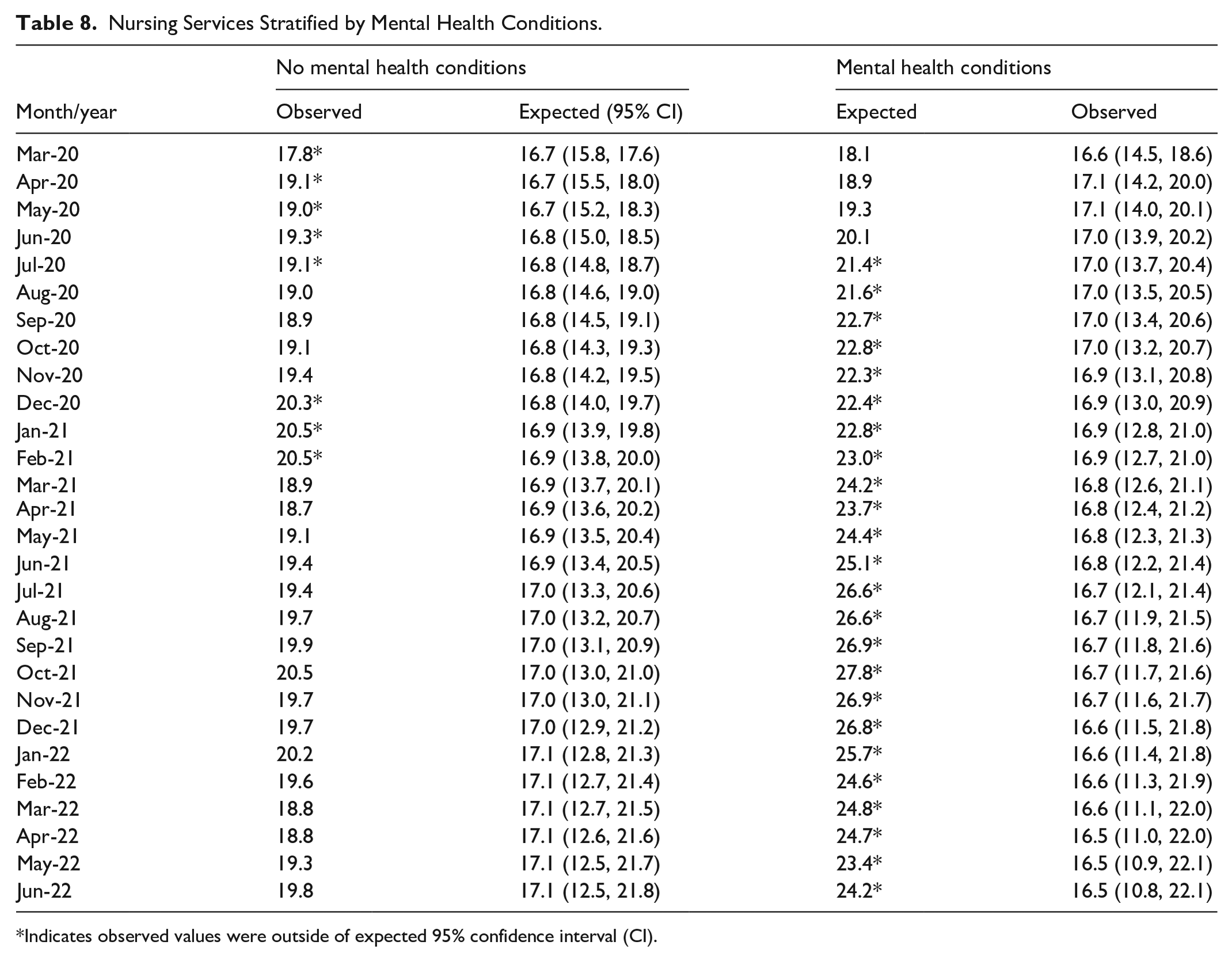
Indicates observed values were outside of expected 95% confidence interval (CI).
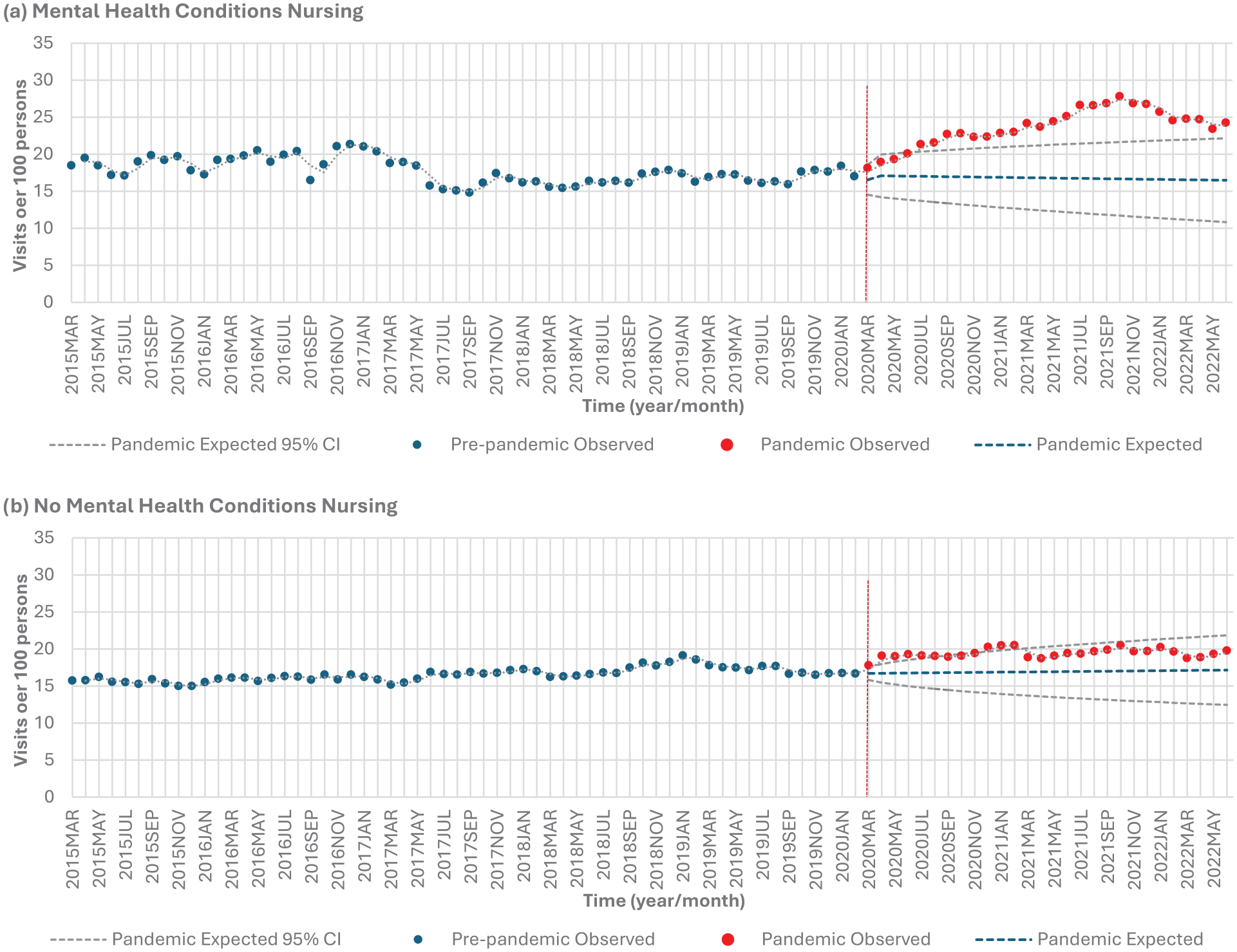
Homecare nursing services stratified by mental health: (a) mental health conditions versus (b) no mental health conditions.
Sensitivity Analysis
No significant findings were found for overall homecare utilization (personal care services plus nursing visits) for any of the subpopulations.
Discussion
Our study investigated the impact of the COVID-19 pandemic in a population with physical disabilities stratified by sex, age, and mental health conditions. In general, we found a decrease in personal support services and increase in nursing services for most subpopulations. Males, those under the age of 65, and those with mental health conditions experiences greater shifts in their homecare services during the pandemic, compared to females, those above the age of 65, and those without mental health conditions. Similar to the findings in adults with dementia, which found males and females exhibited similar changes in homecare services during the pandemic, 1 we also found a significant decrease in personal support services across both sexes, particularly among males, while nursing services increased for both males and females. Individuals aged 65 and under experienced a more pronounced decrease in personal support services but higher increases in nursing services compared to individuals above 65. Finally, those with mental health conditions exhibited a significant increase in nursing services, highlighting potential vulnerabilities within this subpopulation.
Similar to our findings, previous studies also found decreases in personal support services in the general adult population and adults with dementia.1,2 The observed decrease in personal support services may be due to issues with service availability or client preferences.3,18 Although there were decreases in the availability of workers to provide personal support services, 18 a previous study indicated client initiated holds and cancellations accounted for 99.3% of service reduction during the pandemic. 3 Clients may have chosen to hold or cancel visits to reduce exposure to the COVID-19 virus; however, this could result in these individuals having unmet healthcare needs, or relying on unpaid or privately funded caregivers to fulfill this need. 18 As such, certain subpopulations with access to unpaid or private caregiving support during the pandemic may have been more inclined to reduce homecare personal support services during the pandemic.
Interestingly we found no change to overall homecare utilization in our study when the sensitivity analysis was conducted. Our study found subpopulations with decreases in homecare personal support services during the pandemic also experienced an increase in nursing services during this period. The increase in nursing visits during the pandemic would allow for the access of medical care, including monitoring of vital signs, medication management, and wound care. As such this may reduce the need for patients to visit their healthcare provider, emergency department, or hospital to receive care. A prior study investigating healthcare utilization and delivery during the COVID-19 pandemic in individuals with spinal cord injuries did experience a decrease in utilization of primary care, hospital and emergency department services during the pandemic. 15 It is possible the increase in nursing visits for homecare services was intentional to decrease exposure to infectious diseases like COVID-19 by limiting contact with healthcare facilities. Alternatively, the increase in nursing services this may indicate certain subpopulations began to experience increased health needs during the pandemic requiring specialized care provided by nursing services, rather than personal support services. In particular, our study highlighted the increase in nursing services for individuals with mental health conditions, potentially indicating an increased health need in this group during the pandemic. This finding aligns with previous research, which highlighted that adults with dementia experienced an increase in nursing services during the pandemic, 1 even though this was not found for homecare services in the general adult population. 2 Further research is needed to understand this increase in nursing homecare services in those with mental health conditions, especially if homecare services have shifted again post-pandemic. Qualitative research is needed to provide a more comprehensive understanding of context and individual experiences, preferences, and factors contributing to accessing and receiving homecare services.
While further research is needed, homecare agencies can use the findings from this study to enhance preparedness for future epidemics, pandemics, or other public health emergencies. Since we found no changes in overall homecare utilization in our study, but changes at the service level for both nursing and personal support services, agencies should proactively strengthen nursing services, develop contingency plans for personal support staffing, as well as consider implement real-time monitoring to detect service gaps early. Special attention must be given to disproportionately impacted populations, such as individuals with mental health conditions, and services should be tailored to meet the diverse needs across sex and age groups. To co-create practical solutions and implement strategies effectively, agencies should engage clients, caregivers, and staff through qualitative and mixed methods research process.
Limitations
This study relied on the retrospective secondary use of health administrative data and is limited by the extent and type of data available. We did not have any additional information on functional status of individuals in our cohort. We also do not have clinical details regarding the visits or any information on the reason homecare services were changed, canceled, delayed, or increased. Our data rely on publicly funded homecare services, and we do not have data on private homecare services. The study uses data only from Ontario, and the focus on a specific geographic region may limit the generalizability of findings to broader populations.
Conclusion
This study uniquely investigated the intersection between sex, age, mental health conditions, and physical disability in homecare services utilization during the COVID-19 pandemic. We found nuanced impacts in homecare services across different subpopulations, emphasizing the importance of considering multiple factors when identifying the impact COVID-19 had on healthcare utilization and access. Our findings align with other studies that reported disruptions in homecare services during the pandemic. However, we highlighted that individuals with mental health conditions may have been disproportionally impacted. As such future work should create recommendations or strategies to improve care for this population. The findings from this study can be used for future research to ensure equitable access to homecare services for individuals with physical disabilities in Canada. During the pandemic, to prioritize infection control and to ensure adequate medical care increases in nursing services may have implemented. However, homecare service delivery should be re-assessed post-pandemic to determine if the distribution of services between personal support services and nursing visits meets the current needs of individuals receiving homecare, as well as the healthcare system.
Footnotes
Acknowledgements
This study was also supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). Dr. Guilcher is currently supported by the University of Toronto Centre for the Study of Pain Scientist Salary Award. Dr. Tu is supported by a Chair in Family and Community Medicine Research in Primary Care at UHN and a Research Scholar award from the Department of Family and Community Medicine at the University of Toronto. Dr. Craven is supported by UHN Foundation in her role as the University of Toronto/University Health Network COPE Family Chair in SCI Health Services Innovation. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Data for this study was obtained from ICES (formerly named the Institute for Clinical Evaluative Sciences), an independent, non-profit research institute funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). As a prescribed entity under Ontario’s privacy legislation, ICES is authorized to collect and use health care data for the purposes of health system analysis, evaluation, and decision support. Secure access to these data are governed by policies and procedures approved by the Information and Privacy Commissioner of Ontario. This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from Canada Post Corporation and Statistics Canada. Parts of this material are based on data and/or information compiled and provided by the Ontario Ministry of Health, and the Canadian Institute for Health Information. The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. Parts of this material are based on data and information provided by Ontario Health (OH). The opinions, results, view, and conclusions reported in this paper are those of the authors and do not necessarily reflect those of OH. No endorsement by OH is intended or should be inferred
Ethical Considerations
ICES is a prescribed entity under Ontario’s Personal Health Information Protection Act (PHIPA). Section 45 of PHIPA authorizes ICES to collect personal health information, without consent, for the purpose of analysis or compiling statistical information with respect to the management of, evaluation or monitoring of, the allocation of resources to or planning for all or part of the health system. Projects that use data collected by ICES under section 45 of PHIPA, and use no other data, are exempt from REB review. The use of the data in this project is authorized under section 45 and approved by ICES’ Privacy and Legal Office.
Consent to Participate
Section 45 of PHIPA authorizes ICES to collect personal health information, without consent, for the purpose of analysis or compiling statistical information with respect to the management of, evaluation or monitoring of, the allocation of resources to or planning for all or part of the health system.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from the Canadian Institutes of Health Research (CIHR) (#478336).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (e.g., healthcare organizations and government) prohibit ICES from making the dataset publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at ![]() (email:
(email: