
Abstract
Telemedicine utilization of people with an Intellectual or Other Developmental Disability (IDD) during the COVID-19 Pandemic is not well known. This study compares telemedicine utilization of those with and without IDD prior to the pandemic to after it began. Using the Utah All Payers Claims Database from 2019 to 2021, the study identified telemedicine utilization of adults aged 18 to 62 years old in 2019. Propensity score matching was used to minimize observed confounders of subjects with and without IDD in 2019. Negative binomial regression was used to identify factors that were associated with telemedicine utilization. The final number of subjects in the analysis was 18 204 (IDD: n = 6068, non-IDD: n = 12 136 based on 1:2 propensity score matching). The average (SD) age of the subjects was 31 (11.3) years old in 2019. Forty percent of the subjects were female, about 70% of subjects were covered by Medicaid in 2019. Average (SD) number of telemedicine use in 2020 (IDD: 1.96 (5.97), non-IDD: 1.18 (4.90); P < .01) and 2021 (IDD: 2.24 (6.78) vs 1.37 (5.13); P < .01) were higher for the IDD group than the non-IDD group. The regression results showed that the subjects with IDD had 56% more telemedicine encounters than those in the non-IDD group (Incidence Rate Ratio (IRR) = 1.56, P < .01). The growth of telemedicine during the COVID-19 pandemic has the potential to reduce persistent healthcare disparities in individuals with IDD. However, quality of telemedicine should be considered when it is provided to improve health of subjects with IDD.
Despite the widespread adoption of telemedicine in the general population during the pandemic, there is currently no available information on its utilization by individuals with IDD.
Our research contributes by comparing the utilization of telemedicine and the types of visits via telemedicine between subjects with IDD and without IDD during the pandemic.
The substantial increase in telemedicine use following the onset of the COVID-19 pandemic may have the potential to significantly reduce persistent healthcare disparities in individuals with IDD.
Introduction
Roughly 1 in 6 individuals in the U.S. population has an intellectual or other developmental disability (IDD). 1 IDD is defined by deficits in both intellectual function (eg, reasoning, problem solving) and adaptive function (eg, communication, social participation, and practical living skills) with onset during childhood or adolescence. Persons with IDD constitute about 10.8% of Americans with a disability, and their numbers are growing due in part to increasing life expectancy. 2 However, adults with IDD in the U.S. die approximately 9 years earlier than those without IDD. 3
Adults with IDD experience higher rates of multiple chronic physical and mental health comorbidities.4 -8 Utilization of preventive health care, including long-acting reversible contraception, colorectal, and cervical cancer screenings, are significantly lower in adults with IDD. Lack of utilization is multifactorial. Inadequate provider training, knowledge, awareness, communication problems, and reliable access to primary care are the most noted factors plaguing IDD patients.9 -13
The COVID-19 pandemic has forever changed how patients, clinicians, and all involved parties’ interface with health care. 14 An area of growing modifiability for patients with IDD is the emergence of telemedicine’s availability, especially in the context of meeting patient needs during the COVID-19 pandemic. Telemedicine is the distribution of health-related services and information via electronic information and telecommunication technologies. It allows long-distance patient and clinician contact, care, advice, reminders, education, and intervention. 14 People with IDD often encounter hurdles that may discourage them from using modern technologies. This population often displays linguistic and cognitive limitations that may make it difficult for them to use text-rich applications. Social communication difficulties can make interacting with others through video or telephone more problematic. There are also physical obstacles that may make it difficult for patients to use, such as using a computer keyboard, and sensory barriers that make it difficult to view information on small screens. Nevertheless, it has been shown that people with a mild-to-moderate intellectual disability can effectively learn given simple options with electronic devices. 15
The use of modern technologies creates new opportunities to improve the quality and accessibility of medical care for those with IDD. Previous studies have shown a significant improvement in balance in low-active adults with Down Syndrome following a telemedicine exercise program. 16 Patients with IDD continued to utilize all healthcare service types at pre-pandemic rates and remained steady except for virtual physician visits, which showed increased rates. 17
The COVID-19 pandemic has rapidly transformed service delivery opportunities for those with IDD, providing an unprecedented opportunity to evaluate how those with IDD interact with telemedicine for their healthcare needs, both within the context of a global pandemic and beyond. 18 However, to our knowledge, no previous studies have assessed the use of telemedicine in individuals with IDD, whether in the context of the COVID-19 pandemic or otherwise. Thus, our aim is to evaluate telemedicine utilization of people with and without IDD in Utah pre- and post-beginning of the pandemic, utilizing a statewide dataset spanning from 2019 to 2021.
Methods
Data
This study used the 2019 to 2021 Utah All Payers Claims Database (APCD) to compare telemedicine uses of subjects with IDD to telemedicine use of subjects without IDD. The APCD includes data from about 70% of individuals in Utah who are insured through private insurance, Medicaid and Medicare Advantage. Enrollment and claims files were used to identify the subjects and the controlled variables. More detailed information about the Utah APCD can be found from previous studies.19 -21 To enable using data of human subjects, this study was approved by Institutional Review Board (IRB) at the University of Utah (IRB 00151091).
Subjects
Adults (≥18-62 years old in 2019) who had an IDD diagnosis were included in the study. IDD diagnosis was identified based on International Classification of Diseases, tenth revision diagnosis codes (ICD-10 dx) from Centers for Medicare and Medicaid Services (CMS) Chronic Conditions Data Warehouse. 22 This included Down Syndrome, Cerebral Palsy, Autism spectrum disorder or Pervasive Developmental Disorder, and Intellectual Disability. 2 Matched adults with no IDD were identified in 2019. The 2021 data was the last year of data available in the APCD when the study was conducted. Therefore, the study included the 2019 to 2021 data for the analysis. Those who were dual eligible for Medicare and Medicaid were excluded in the study.
Outcome
The number of telemedicine encounters each year (2019-2021) by both groups, as well as which healthcare services were used via telemedicine, were the primary study outcomes. The telemedicine uses were identified with place of service (POS: 2, 12) and current procedure terminology (CPT) codes (99441, 99442, 99443, 99444, 99421, 99422, 99423, 98970, 98970-2, 98971, 98972, G0071, G2025, G2061, G2061-3, G2062, G2063, G2250-2). 23
Covariates
An indicator for a diagnosis of IDD (Yes/No) was the key independent variable in our analysis. Age (18-30, 31-40, 41-50, 51-64), sex (male/female), race/ethnicity (non-Hispanic White, non-Hispanic others, Hispanic and missing), type of insurance (private insurance, Medicaid), Elixhauser comorbidity index score, and comorbid conditions (diabetes, hypertension, obesity, asthma, anxiety, depression, cognitive disorder, epilepsy, bipolar, schizophrenia, ADHD) in the year 2019 were included in the analysis. These comorbid conditions could be highly correlated to telemedicine uses during the pandemic. The non-Hispanic others category included non-Hispanic African American, American Indian, Asian, and Pacific Islander. In addition, the Elixhauser comorbidity index score was calculated with diagnosis codes in 2019. Comorbidity conditions were identified based on ICD-10 dx from Clinical Classifications Software Refined (CCSR) from the Agency for Healthcare Research and Quality (AHRQ) and the CMS Chronic Conditions Warehouse.22,24
Statistical Approaches
Summary statistics such as mean, standard deviation (SD), and percent were used to summarize the study population. Propensity score matching (PSM) was used to identify matched subjects with no IDD who had similar characteristics of subjects with IDD in 2019. We estimated the propensity to have an IDD diagnosis using a logistic regression with age (as continuous), sex, race/ethnicity, type of insurance, and Elixhauser comorbidity index scores as independent variables. Matched controls utilized 1:2 matching. Standardized differences in the control variables were used to compare any differences after matching. Less than 0.1 was defined to indicate no difference in a variable between the 2 groups. T-test for continuous variables and Chi-square test for categorical variables in the summary table were used to compare the characteristics of the 2 groups. For the outcome model, we used a population-averaged negative binomial regression (NBR) to reflect the nature of the outcome variables as count data over time (ie, 3 years from 2019 to 2021), including the independent variables listed above in a doubly robust approach. Incidence rate ratios (IRR) from NBR were calculated for the controlled variables. E-value approach was used to calculate a point estimate that could invalidate the IRR of the IDD variable due to unobserved potential confounders. After applying PSM, the standardized differences for the controlled variables were all below 0.1, indicating that there were no significant differences in these variables between the 2 groups. P-value less than .05 was defined as statistically significant.
Results
In our analysis, we considered both phone and video utilization as forms of telemedicine, as there was no way to split out these datasets with the current claims data. Among those who had continuous enrollments from 2019 through 2021, 564 045 adults in 2019 were included. Among these adults, excluded subjects due to dual eligibility numbered 11 399. Out of 552 646 total including individuals, 6566 subjects had an IDD diagnosis code in 2019. Among the subjects with IDD, 498 subjects had no matched controls and 6068 subjects had 2 matched controls. The final sample size was 18 204 (IDD: n = 6068; non-IDD: n = 12 136).
Average (SD) age of the subjects between the 2 groups was similar (IDD: 31 (11.3) years old vs no IDD: 31 (11.3) years old; P = .34), and 40% of subjects in both groups were female (P = 1.00). Average (SD) comorbidity score was 1.5 (1.7) in both groups, and about 70% of the subjects were covered by Medicaid in both groups (P = 1.00). While 5.9% of those with no IDD had ADHD, 9.9% of subjects with IDD had ADHD (P < .01). Cognitive disorder had 5.7% and 50.1% of subjects with and without IDD, respectively (P < .01) (Table 1).
Summary Statistics of Subjects With and Without Intellectual or Other Developmental Disability (IDD) in 2019.
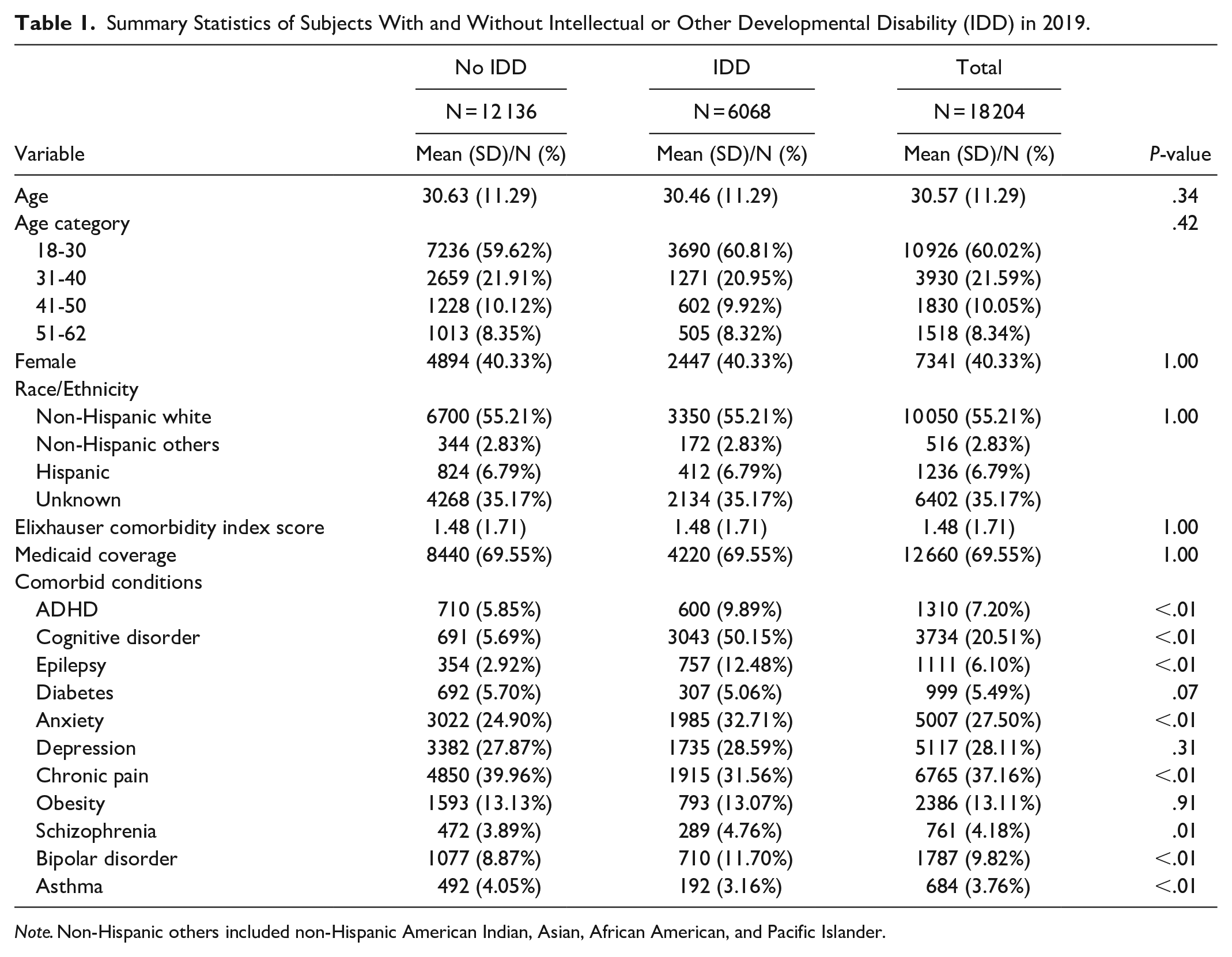
Note. Non-Hispanic others included non-Hispanic American Indian, Asian, African American, and Pacific Islander.
Average number of telemedicine visits was low for both groups in 2019 (0.03vs 0.02, P = .06). The IDD group had higher telemedicine use in both 2020 and 2021 than the no IDD group. The average (SD) number of telemedicine visits in 2020 was 1.96 (5.97) for the IDD group and 1.18 (4.90) for the non-IDD group (P < .01). In 2021, the averages were 2.24 (6.78) for the IDD group and 1.37 (5.13) for the non-IDD group (P < .01) (Table 2).
Average Number of Telemedicine Use Over Time.

Note. The numbers in the parentheses represent standard deviations.
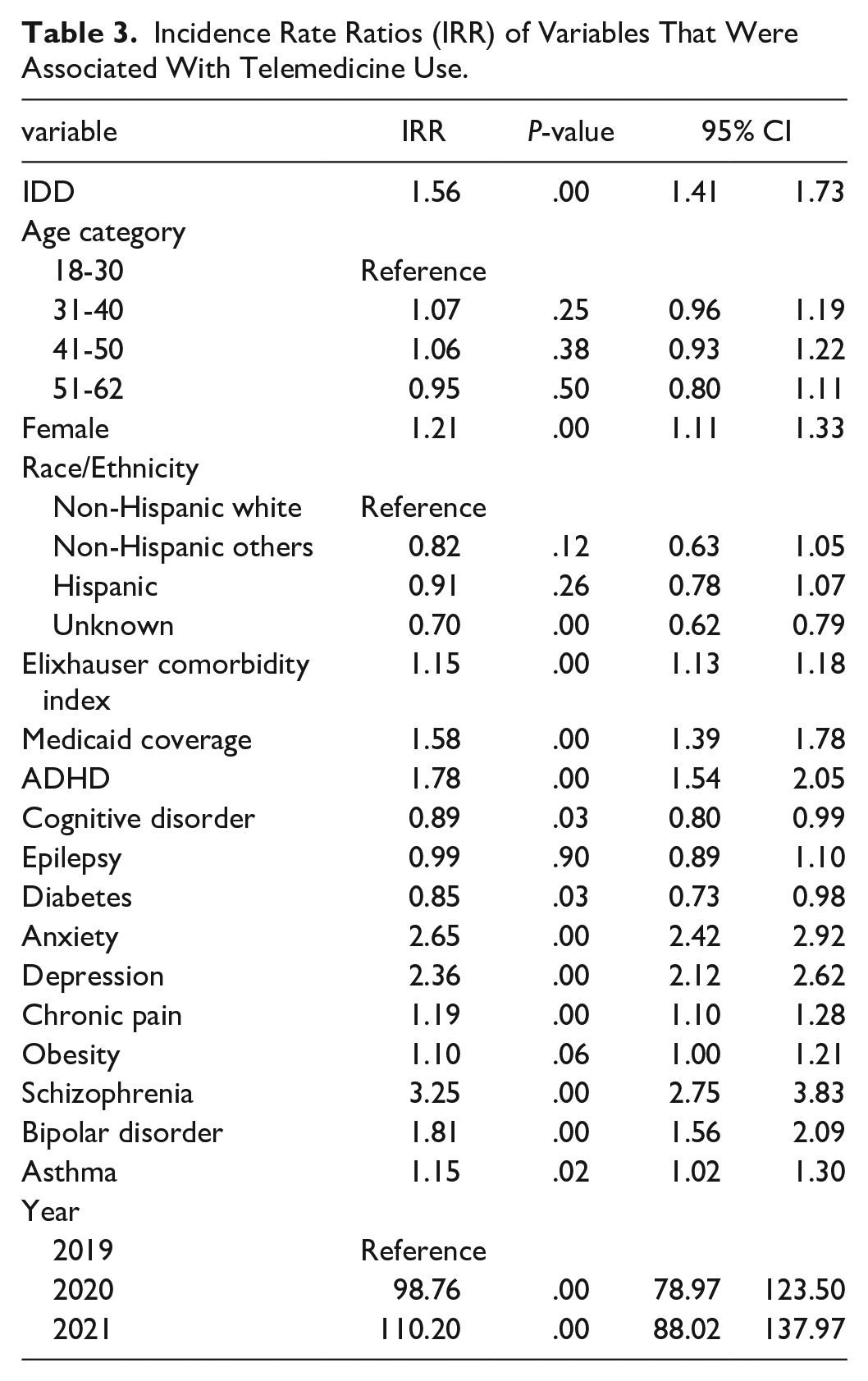
The subjects with IDD had 56% more telemedicine encounters (IRR = 1.56, P < .01), and females were more likely to use telemedicine than males (IRR = 1.21, P < .01). Those who were covered by Medicaid were 58% more likely to use telemedicine (IRR = 1.58, P < .01). Subjects with comorbid conditions such as ADHD (IRR = 1.78, P < .01), anxiety (IRR = 2.65, P < .01), depression (IRR = 2.36, P < .01), schizophrenia (IRR = 3.25, P < .01), bipolar (IRR = 1.81, P < .01), and asthma (IRR = 1.15, P = .02) had more telemedicine use (Table 3).
Incidence Rate Ratios (IRR) of Variables That Were Associated With Telemedicine Use.
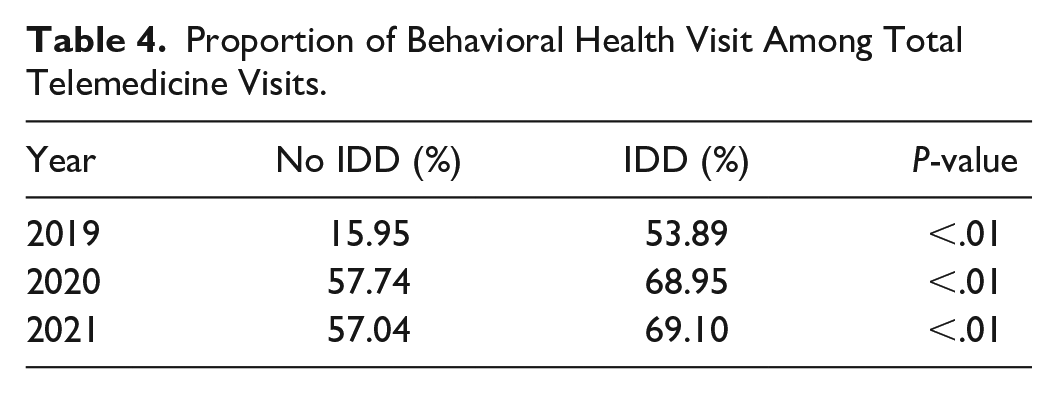
Nearly 70% of telemedicine visits of the subjects with IDD after the start of the pandemic were for behavioral health visits, versus almost 60% for individuals without IDD (2020: 69%vs 58%, P < .01; 2021: 69%vs 57%, P < .01) (Table 4).
Proportion of Behavioral Health Visit Among Total Telemedicine Visits.
The IRR from the E-value was 2.50, which was greater than all other controlled variables, except anxiety and schizophrenia. Thus, the impact of any unmeasured confounding that could be bigger than 2.50 to invalidate the IRR of IDD (vs no IDD) is likely minimal.
Discussion
The study findings reveal a significant increase in the utilization of telemedicine among patients with IDD after the start of the pandemic compared to patients without IDD (on average 1.96 visits among IDD vs 1.18 visits for non-IDD in 2020, P < .01). While utilization was low in both groups pre-pandemic, subjects with IDD had 56% more telemedicine use compared to those without IDD (IRR = 1.56, P < .01). Our findings suggest that the pandemic may have transformed healthcare service delivery among subjects with IDD and accelerated the adoption of telemedicine in this group. Furthermore, 70% of telemedicine visits were for behavioral health among subjects with IDD, compared to 60% among those without IDD. This highlights opportunities for improving behavioral healthcare services and making them more accessible to subjects with IDD. To our knowledge, this is the first study that looks at telemedicine utilization among patients with and without IDD, comparing utilization pre- and post- the start of the pandemic. This study provides robust evidence to the evolving landscape of healthcare delivery for individuals with IDD, both during and beyond the pandemic.
In recent years, the rapid evolution of telemedicine, accelerated by the COVID-19 pandemic, has garnered considerable attention. Despite this growth, individuals with IDD have remained a relatively understudied demographic within the telemedicine landscape. Research indicates that individuals with IDD encountered significant disruptions in healthcare access during the COVID-19 pandemic, with a study by Jeste et al revealing that 36% of respondents with IDD lost access to a healthcare provider. 25 Notably, those within this group who needed healthcare primarily turned to telehealth for assistance. This underscores the critical need to evaluate the impact and utilization of telemedicine among patients with IDD. Our study contributes to filling this knowledge gap by demonstrating a marked increase in overall telemedicine utilization post- the start of the pandemic. Specifically, patients with IDD exhibited a higher rate of telemedicine utilization compared to their non-IDD counterparts, as evidenced by an average of 2.24 visits (SD: 6.78) in 2021 for the IDD group, compared to 1.37 visits (SD: 5.13) for the non-IDD group (P < .01). This underscores the pivotal role telemedicine can play in promoting accessible and equitable healthcare for this vulnerable population, while mitigating challenges faced by this group.
People with intellectual disabilities often face a higher prevalence of mental illnesses, 7 limited access to specialized services, and barriers to receiving preventive care. Telemedicine emerges as a promising solution to bridge this healthcare gap, enabling individuals with IDD to access necessary care, preventive services, and specialized interventions more effectively. Our study indicates that 70% of telemedicine visits for people with IDD were behavioral health-related, supporting the efficacy of telemedicine in managing health conditions in this group. Digital mental health interventions, including cognitive-behavioral therapy, can be successfully implemented in this cohort. 26 Clinicians increasingly integrate digital interventions into routine mental health treatment for people with IDD. Telepsychiatry, delivered among 300 youths with IDD, was successful in preventing emergency room visits. 27 Telemedicine has the potential to address some common challenges faced by people with IDD. For example, communication challenges are common among people with IDD, hindering their healthcare experiences. 28 Telemedicine facilitates remote patient monitoring in home environments, providing a comforting and less intimidating approach. 29 Modern technologies empower individuals with IDD to access health information in more understandable formats, fostering better comprehension of the connection between health knowledge, healthy lifestyles, and physical activity. Instructional videos that demonstrate an activity from start to finish have been shown to be effective among people with IDD. 30 Moreover, people with IDD frequently have multiple co-existing health conditions, 7 and multiple comorbidities like diabetes, obesity, and kidney disease, which complicates their care within a healthcare system primarily focused on acute medical conditions. Telemedicine can be valuable in increasing access to multiple specialists, thus improving care co-ordination to manage mental and physical healthcare needs. For example, physical activity interventions were successfully delivered over teleconference in a group with IDD. 31
While telemedicine offers many potential benefits, there are potential barriers to the utilization of modern technology for individuals with IDD. For example, people with disability are 20% less likely to own computers, smartphones, or tablets than those without, making access to telehealth difficult. 32 However, our research findings demonstrate a higher adoption of telemedicine within this population compared to those without IDD, indicating that with appropriate support, individuals with IDD can effectively adapt to modern technology. Nonetheless, the use of digital technology among individuals with IDD also poses certain risks, which may be heightened compared to the general population. A potential concern pertains to the handling of sensitive data by certain applications, which may exploit users’ personal information for commercial purposes. Individuals with intellectual disabilities may encounter difficulties in comprehending the privacy policies of such applications, rendering them more vulnerable to abuse. Lastly, communication difficulties experienced by individuals with IDD could result in diagnostic errors in the context of telemedicine. Telemedicine from non-routine care providers has been linked to increased need for in-person follow-up, 33 raising patient safety concerns. Yet, risks may be reduced when telehealth is offered by clinicians within the patient’s existing medical home, ensuring access to medical records, facilitating testing, follow-up, and specialist referrals. Integrating telemedicine as a complementary service to in-person care holds the potential to enhance healthcare delivery for people with IDD.
Although this study used a population level dataset, several limitations could affect the findings. First, this study considered adults who were covered by Medicaid and private insurance. Thus, our findings may not be generalizable to adolescents or elderly subjects who were covered by Medicare. Second, many of the subjects were missing (35%) in race/ethnicity. This missing information may influence our findings. Third, any medications such as anti-depressants and anti-diabetic drugs were not used to identify comorbid conditions. This could underestimate the impact of the comorbid conditions in the regression. Fourth, although the study used a state-wide claims database, this study could be impacted by measurement bias and unmeasured confounders. Fifth, this study was not able to assess whether IDD subjects either independently accessed telemedicine or if they accessed by initiative and assistance from family, caregivers, or others. This could limit the impact of outcomes if patients are dependent on other individuals to interface with healthcare. Lastly, whether the telemedicine visit was based on video only or audio only was not identified using the claims data. Because about 98% of telemedicine uses were captured by POS, this study was not able to distinguish any differences in video only or audio only between the 2 groups.
Conclusions
The significant increase in telemedicine use after the start of the COVID-19 pandemic can meaningfully reduce persistent healthcare disparities in individuals with IDD. Robust policies and regulations should be established, and measures taken to address the responsible handling of personal data, secure communication platforms, and other explicit protections for individuals with IDD. Collaboration between healthcare providers, policymakers, advocacy organizations, and technology developers is crucial in establishing ethical standards and regulations that safeguard the rights and privacy of individuals with IDD in the telemedicine realm.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241226540 – Supplemental material for Differences in Telemedicine Use Between People With and Without an Intellectual or Other Developmental Disability During the COVID-19 Pandemic
Supplemental material, sj-docx-1-inq-10.1177_00469580241226540 for Differences in Telemedicine Use Between People With and Without an Intellectual or Other Developmental Disability During the COVID-19 Pandemic by Jaewhan Kim, Indrakshi Roy, Joseph Sanchez, Peter Weir, Richard Nelson and Kyle Jones in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
There are no additional acknowledgments.
Data Availability
The data is not publicly available because of privacy and ethical restrictions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for all datasets in the study was provided by the University of Utah Matheson Center for Health Care Studies.
Ethics and Informed Consent Statement
The study protocol (IRB-00151091) was reviewed by the University of Utah Institutional Review Board, which determined that the study does not constitute human subjects research as defined under federal regulations and does not require IRB approval.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.