
Abstract
As the COVID-19 pandemic impacted mental health, this longitudinal study examined the effect of age-friendly communities (AFC) action plan on older adults’ depressive symptoms. Using the CLSA, the CLSA COVID-19 Questionnaire study, survey of Canadian municipalities, and the census, the depressive symptoms trajectories were modeled with multilevel multinomial regressions. Most respondents (66.1%) had non-depressed trajectories, 28.1% experienced a moderate increase in depressive symptoms, and 5.8% had a depressed trajectory. AFC action plans did not have a protective effect on these trajectories. Being a female, greater loneliness, lower income, ≥2 chronic conditions, inferior social participation, weaker sense of belonging, COVID-19 infection, and pandemic stressors predicted a depressed trajectory. Neighborhood’s deprivation had a weak protective effect on the declining trajectory. Although AFC action plans provided no benefits during the pandemic, volunteers facilitating resource access and social interactions could limit any increase in depressive symptoms.
Governments worldwide implemented measures to limit the spread of COVID-19, most notably quarantines, restricted access to healthcare, and limited social interactions, which had adverse effects on the mental health and well-being of older adults.
Although not supporting the effect of age-friendly communities action plan on depressive symptoms, the results highlighted the importance of preventing loneliness and verbal or physical conflicts, as well as providing safe social opportunities during the pandemic and neighborhood amenities meeting older adults’ needs (safe transportation, green spaces and public places).
Having an AFC action plan did not have a protective effect against older adults’ depressive symptoms; however, the results suggested that in times of pandemic, priority should be given to identifying older adults self-reporting as lonely, and informing and helping them to use support resources.
Introduction
During the Coronavirus Disease 2019 (COVID-19) pandemic, governments worldwide, including the Canadian federal and provincial governments, implemented a variety of public health measures to prevent the spread of the virus, most of which were especially restrictive for aging populations. 1 Public health measures included physical distancing, wearing a mask, minimizing interactions with others, temporary closure of many gathering places, and staying home when symptomatic. 2 The measures applied to all adults, but had substantial implications for older adults: (1) when quarantined, they faced higher risks of violence, abuse, and neglect; (2) the concentration of health resources on COVID-19 reduced their access to healthcare for their existing conditions; (3) the measures restricted their in-person social interactions, and home and community services and support, especially for those living alone. 1 Although these measures aimed to prevent the spread of infection, the resulting social isolation had adverse impacts on physical and mental health. Particularly for mental health, physical distancing and social isolation led to increased mental health issues including depressive symptoms, such as stress, anxiety, irritability, and insomnia, 3 already widely observed in older populations before the COVID-19 pandemic.4,5 Studying depressive symptom trajectories can provide important insights about the changes in mental health of populations in situations of vulnerability. More than 4 aging or older Canadians in 10 reported increasing depressive symptoms after the initial lockdown according to the Canadian Longitudinal Study on Aging, 19 and about one in 10 had amplified deterioration, mainly explained by pandemic-related stressors (eg, difficulties accessing resources, family conflicts). Other known individual factors that contributed to increased symptoms of depression in older adults include being a woman, 6 having a lower household income 7 and having multiple chronic conditions. 8
Depressive symptoms were also found to be associated with environmental factors. The Neighborhood stress process model indicates that stress is central in the associations between depressive symptoms and environmental characteristics. 9 The daily level of stress is influenced by the social characteristics of the neighborhood (eg, disorder, danger), and the lack of resources and services that facilitate the daily activities. Residents with a negative perception of the neighborhoods reported their social network as less supportive, which weakens its protection against depressive symptoms. 10 The Global Age-Friendly Cities policy framework of the World Health Organization 11 has been guiding the development of age-friendly cities and communities (AFC) initiatives around the world for almost 2 decades, promoting factors known to have a protective effect on depressive symptoms. 12
Widely implemented, the aims of AFC initiatives are to optimize policies, services, settings and structures, and to improve active aging by ensuring older adults enjoy good health, stay socially involved, and feel safe. 13 A recent scoping review of 27 AFC interventions targeting health and social outcomes observed improvements such as fewer depressive symptoms, less social isolation or more frequent social participation. 13 In Canada, greater age-friendliness in rural communities has been shown to be associated with enhanced life satisfaction and better health in older Manitobans. 14 A pan-Canadian survey showed that municipalities that had successfully implemented an AFC action plan were more age-friendly, particularly in the domains of transportation, physical environment, opportunities for participation, communication and information, and community support and health services. 15 Specifically related to social relations, emotional (contact with family, friends and neighbors) and instrumental (access to or delivery of medications and groceries) support can be improved, particularly for individuals without close family support, by AFC action plans targeting transportation and connectivity, which increase proximity and availability of services. 14
Although AFC can increase support, communication, and perceptions of trust in communities, few studies have evaluated the impacts of AFC initiatives on older adults’ depressive symptoms during a pandemic or large-scale crisis. For example, older Americans engaged in social organizations prior to the pandemic reported fewer depressive symptoms during the COVID-19 pandemic. 15 By mitigating some of the pandemic stressors, especially in relation to communication and access to food and medicine, active existing networks could also have a beneficial effect on mental health. According to local leaders from 490 American AFCs surveyed during the COVID-19 pandemic, more than one in 2 communities believed that having implemented an AFC action plan (eg, partnerships, improved communications, reaching out initiatives, and volunteer networks) had prepared them better for the pandemic.16,17 Worries about access to food, medicine, information and healthcare were nonetheless expressed, as was the ability to keep older adults engaged. In a study conducted by the Pan American Health Organization, 18 most AFCs surveyed had implemented strategies for safe access to medications (15 out of 16), and supported community-led services for daily activities (12 of 16), such as delivery of groceries and medications. Contact with friends and neighbors, and participation in social organizations, prior to the pandemic, protected Americans (n = 3033, mean age 67.5 ± SD = 7.3 years) from increasing depressive symptoms. 15 To our knowledge, no study has examined the effect of living in or outside an AFC before and during the COVID-19 pandemic on the trajectories of depressive symptoms of older residents. Trajectories of depressive symptoms can provide valuable information about the potential protective effect of AFCs on older Canadians during the pandemic, which can help guide actions and policies. This study thus aimed to explore the potential protective effect of having an AFC action plan on older Canadians’ depressive symptom trajectories during the pandemic, and to examine individual (ie, age, sex, household income and chronic conditions) and community (social and material deprivation) predictors of these trajectories. The individual predictors examined were age, sex, household income, chronic conditions, loneliness, social participation, sense of belonging, probable or confirmed COVID-19, and COVID-19 stressors.
Materials and Methods
Design and Participants
To achieve these objectives, secondary data analyses were carried out using: (1) the Canadian Longitudinal Study on Aging (CLSA) first follow-up (2015-2018), and the data collected periodically between April and December 2020 in the CLSA COVID-19 Questionnaire study, (2) an updated survey of Canadian municipalities, and (3) the 2016 Canadian census. The CLSA is a national cohort study that used a stratified random sampling strategy to recruit 51 338 adults aged 45-85 at baseline (2012-2015) with a follow-up every 3 years for at least 20 years. 19 The sampling strategy was based on age, sex and province. Individuals residing in Canada’s 3 territories, on First Nations reserves, or in long-term care facilities, members of the armed forces, individuals unable to communicate in English or French, and individuals with severe cognitive deficits were not included in the study. Completed in mid-2018, the first follow-up involved 43 255 participants (excluding 1560 respondents with partially or completely missing data) and was used to describe respondents’ baseline depressive symptoms and individual characteristics. During the pandemic, all participants who were still actively participating in the CLSA study were invited to participate in the CLSA COVID-19 Questionnaire study between April and December 2020 via baseline, weekly/biweekly, monthly and exit phone- and web-based interviews. Of the 43 255 respondents having complete data from the first follow-up, 26 855 (15 363 respondents died, were lost to follow-up or had missing data) respondents completed a questionnaire at entry (referred to as the COVID-19 baseline; April 2020), 4 weekly (web) or 2 biweekly (phone) questionnaires, 3 monthly questionnaires and an exit questionnaire (September-December 2020; Supplemental File 1). 20 For the COVID-19 exit questionnaire, 22 701 respondents were considered (4154 respondents dropped out or had missing data). At the time of the COVID-19 baseline, a state of emergency was declared in all provinces, and most had prohibited gatherings, postponed non-urgent procedures in healthcare, suspended visitors’ access to long-term care homes and hospitals, and recommended against non-essential travel. 21 In most provinces at the time of the exit interviews, non-essential services (eg, restaurants, gyms, recreational facilities) were closed, indoor gatherings were restricted to small groups, and visitors’ access to healthcare institutions was limited, but not prohibited. In the current study, participants included were 65 or older at the first follow-up study (age group targeted by AFC initiatives). 22 Of the 22 701 respondents, 11 726 were 65 or older at the first follow-up. Respondents were excluded because of missing data at any time points (n = 2017) or if they lived in municipalities with < 20 respondents (n = 3050), which left 6659 respondents. Compared to participants, excluded respondents (n = 5067) had a similar level of depressive symptoms at the first follow-up, but less at COVID-19 baseline (P = .001; data not shown) and exit (P = .001), were older (P < .001), and reported lower incomes (P < .001), less social participation (P < .001), and greater loneliness (P < .001). A smaller percentage of excluded respondents also reported a stronger sense of belonging (P = .001), a probable or confirmed COVID-19 infection (P = .02), and difficulties accessing resources (P = .04).
In addition to the CLSA and CLSA COVID-19 Study, data from a survey completed in June 2017 involving 921 Canadian municipalities were used to classify their level of AFC initiative implementation by applying the Pan-Canadian milestones, including 0) no step initiated; 1) established an advisory committee; 2) secured a local municipal council resolution toward becoming age-friendly; 3) established an action plan; 4) publicly posted the action plan; and 5) committed to measuring activities, reviewing action plan outcomes, and reporting on them publicly. 23 To represent the pandemic context better and include as many municipalities as possible, for municipalities that had not yet reached the fifth milestone or that had not completed the survey, survey data were updated in December 2021 using information from local government websites. Only municipalities that had reached the fifth milestone by April 2020 or earlier were updated, to correspond to the CLSA COVID-19 Study timeframe. Lastly, communities’ characteristics were drawn from the 2016 Canadian census, 24 specifically the material and social deprivation indices, as compiled by the National Institute of Public Health of Québec. 25 Statistics Canada’s Census subdivision geographic codes were used to match respondents with their municipality. Written consent was provided by all CLSA respondents. The Research Ethics Committee of the Health and Social Services Centre, University Institute of Geriatrics of Sherbrooke, approved the secondary analyses for the current project (MP-31-2017-656).
Individual Measures
Self-report instruments and questionnaires were used at the CLSA first follow-up and for the CLSA COVID-19 Study baseline and exit interviews to describe the respondents, depressive symptoms, experience of the pandemic and COVID-19 status. To explore their power to predict depressive symptom trajectories, measures were collected as close as possible to the CLSA first follow-up.
Sociodemographic and health data
Usual sociodemographic data were collected (age, sex, household income, dwelling type, tobacco and alcohol consumption; Table 1). Loneliness was measured using the 3-item UCLA loneliness scale (hardly ever, some of the time or often felt left out, isolated from others and lacked companionship; responses were summed, with total scores ranging between 3-9; scores > 3 were classified as lonely. The UCLA loneliness scale showed good internal consistency (α = .72) and construct reliability with the 10-item Centre for Epidemiological Studies Short Depression Scale (CES-D-10; r = .49; P < .01). 26 Social participation reflected frequency of participating in 8 activities done with others (family or friends outside the household, church or religious, sports or physical, educational and cultural, service club or fraternal organization, neighborhood, community or professional association, volunteer or charity work, and other recreational activities). Responses were converted into frequency of participation for each activity (“at least once a day” = 20; “at least once a week” = 6; “at least once a month” = 2; “at least once a year” = 1; and “never” = 0) 27 and summed. A difference of one point on each activity score is considered clinically significant. 28 Internal consistency of the scale, established through application of the principles of item-response theory, was high (α = .85). Finally, participants were asked to describe their sense of belonging to their local community using 4 response categories (very strong, somewhat strong, somewhat weak, very weak). 29 This question presents good construct validity with self-reported mental health. In this study, participants’ answers were classified as either “very or somewhat strong” or “very or somewhat weak.”
Description of Participants and Municipalities (n = 6659).

Note. se = standard error; AFC<5: no step initiated or not yet committed to measuring activities, reviewing action plan outcomes, and reporting on them publicly; Fifth milestone: committed to measuring activities, reviewing action plan outcomes, and reporting on them publicly; aFirst follow-up; bCOVID-19 baseline;ct-test comparing municipalities that have versus have not achieved the fifth milestone; dchi-squared test comparing AFC<5versus AFC=5; efrom 10 categories of diseases (musculoskeletal, respiratory, cardiovascular, endocrine-metabolic, neurological, gastrointestinal, genitourinary, ophthalmologic, renal and cancer); fthree-item loneliness scale.
Depressive symptoms
The dependent variable was measured at 3 time points (CLSA first follow-up, COVID-19 baseline and exit) using the CES-D-10, which assesses the respondent’s depressive symptoms in the previous week. The items address being bothered by things, having trouble concentrating, feeling depressed, feeling as if everything is an effort, feeling hopeful, feeling fearful, being restless, being happy, feeling lonely, and being unable to get going. Each item includes 4 ordered responses: (1) rarely or never (<1 day); (2) some of the time (1-2 days); (3) occasionally (3-4 days); and (4) most or all of the time (5-7 days). Items are summed into a total score ranging from 0 to 30. CES-D-10 has shown good internal consistency (α = .72) 30 in community-dwelling older adults, and good test-retest reliability (r = .71; P < .005). 31 The concurrent validity of the scale has also been studied and showed positive correlations with self-rated health (r = 0.37; P < .005), daily pain (r = .30; P < .005), and stress (r = .43; P < .005). However, the item “feeling lonely” had to be removed from the CES-D-10 scale because of its correlation with the UCLA loneliness scale, which contains the item “felt left out.” Thus, the CES-D-10 scale used for the present study ranged from 0 to 27.
Activities outside the home during the pandemic
Respondents were asked if they had to leave their home in the previous month and, if so, to identify at least one reason from a list of 10 possible reasons (yes or no). From this list, reasons selected were deemed most relevant in the context of AFC: buying food, going to the pharmacy, meeting friends or relatives. These answers were collected at the CLSA COVID-19 Study baseline time point.
Pandemic-related stressors
A series of questions concerned the participants’ experience with 5 types of events or situations likely to increase pandemic-related stress: (1) health stressors (you were ill, people close to you were ill, a person close to you died); (2) difficulties accessing resources (loss of income, unable to access necessary supplies or food; unable to access my usual healthcare; unable to access my usual prescriptions or treatments); (3) increased verbal or physical conflict; (4) separation from family; and (5) caregiving responsibilities. Stressors were measured at the COVID-19 baseline.
COVID-19 status
Respondents were classified as no, suspected, probable or confirmed COVID-19. 32 Suspected COVID-19 was selected if respondents reported ≥2 symptoms from a list including fever, cough, runny nose, sore/scratchy throat, headache, chills or shivering, muscle and/or joint aches/pains, loss of smell or difficulty breathing, and had a close contact with a probable COVID-19 case. Probable COVID-19 cases had an inconclusive laboratory test, did not have a test but reported fever over 38°C and were in the same room as a person who had COVID-19 or who had COVID-19 symptoms, or were told by a healthcare provider they had COVID-19 but did not have a confirmatory test or reported testing positive for SARS-CoV-2 by nucleic acid amplification test. Finally, confirmed COVID-19 participants tested positive for SARS-CoV-2 on a nucleic acid amplification test. Participants were classified as either 1) no or suspected COVID-19, and 2) probable or confirmed. Answers to these questions were collected at the COVID-19 baseline.
Community Measures
Age-friendliness
The municipalities reported their level of implementation of the AFC process. 33 Even if the fifth milestone is the last level of implementation, initiatives may not have been undertaken and no details about them or their magnitude were available. Nonetheless, as an action plan could potentially have better prepared municipalities for the pandemic, AFC was classified as having, or not having, reached the fifth milestone.
Deprivation
Indices of material and social deprivation are syntheses, respectively, of 1) education, income and employment indicators, and 2) the proportion of persons living alone, separated, divorced or widowed individuals, and single-parent families. 34 Because the 2016 indices were grouped in quintiles and were available only for the dissemination areas, 35 not for the larger census subdivisions (ie, municipalities), the weighted average of quintiles associated with the indices for all dissemination areas comprising a municipality was calculated, similarly to other works. 36
Analyses
Participants and municipalities were described using means and standard errors, or frequencies and percentages, and compared according to their level of implementation of the AFC process, with bilateral t-tests and chi-square tests. As missing data restricted the sensitivity analysis to evaluate the sample attrition between time points, respondents were compared according if they participated in the COVID-19 study or not. Consistent with research by Raina et al., 19 latent class growth modelling 37 was first used to identify distinct trajectories of respondents’ depressive symptoms in aging adults before (first follow-up, 2015-2018) and during the COVID-19 pandemic (at 2 times, April and December 2020). Latent class growth 38 was a data-driven modeling technique that identifies individuals with similar patterns of depressive symptoms over time and classifies them into as homogeneous as possible trajectories. Using a censored normal model, each trajectory was defined by a latent variable that produces a predicted score on a dependent variable for a particular trajectory. Group membership probability was calculated for all combinations of respondents and trajectories, and individual membership was assigned according to the highest probability. The trajectories were modeled using linear and quadratic patterns. The Bayesian Information Criterion (BIC) was computed for each model and used to identify the best model between the different trajectory shapes. Bilateral paired sample t-tests compared CES-D-10 scores between time points, for each trajectory. Additionally, a robustness analysis was used to identify respondents that could be ambiguously classified into a trajectory, by subtracting the probabilities of being assigned one trajectory or the others.
Multilevel multinomial logistic regression models were then developed to examine the potential protective effect of having an AFC action plan on the depressive symptom trajectories. First, a minimal model was tested to verify the effects of municipalities with and without an AFC action plan on depressive symptom trajectories. Second, individual-level variables (level-1; age, sex, household income and chronic conditions) were added to test for fixed and random effects (Model 1). Third, an intermediate model considered the addition of all individual (sociodemographic and clinical measures, activities outside the home, pandemic-related stressors and COVID-19 status) and community characteristics (age-friendliness, material and social deprivation). Finally, using a backward elimination strategy, the control variables and significant predictors (P < .05) were preserved in the final model. The impact of ambiguous trajectory membership on the predictors was addressed with a sensitivity analysis, by comparing the models with (n = 6659) and without (n = 6404) the ambiguously classified participants. A sample size of 77 participants allowed detection of a standardized difference smaller than 0.33 between 2 paired means, based on a significance level of 5% and a power of 80%, which is sufficient for the current analyses.
Results
Most respondents were womenaged 65 to 87, who had a household income above CAN$50 000 and lived in a house or an apartment (Table 1). At all 3 time points (first follow-up, COVID-19 baseline and exit), average CES-D-10 scores were below the clinical diagnoses for depression and increased by about one point between first follow-up and exit, regardless of whether a municipality had achieved the fifth milestone. Most participants had at least one chronic condition, did not smoke and occasionally drank alcohol. More than one-third felt lonely, and a majority reported a strong sense of belonging to their local community prior to the COVID-19 pandemic (Table 1). Fewer than one in 5 respondents had a probable or confirmed case of COVID-19, approximately 3 out of 4 reported stress from being separated from family members, and almost half reported difficulties accessing resources (eg, necessary supplies or food, healthcare, prescriptions or treatments). Most participants left their home to buy food or go to the pharmacy, while less than one in 5 met friends or relatives outside their home (Table 1). About half of the communities had already developed and committed to review their AFC action plan (n = 24), and had average material and social deprivation. When comparing respondents living in municipalities with and without an AFC action plan, few differences were observed. Older respondents in municipalities without an AFC action plan had a higher frequency of social participation and a higher percentage of participants with a stronger sense of belonging to the local community (Table 1). During the pandemic, a greater proportion of these respondents also went out to buy food, and fewer had a probable or confirmed COVID-19 infection. Compared to respondents that completed the COVID-19 study, those who did not were more likely to be men (P < .001; data not shown) and older (P < .001), had inferior household income (P < .001), participated socially less frequently (P < .001), felt less lonely (P < .001) and reported more depressive symptoms at the first follow-up time point (P < .001).
Overall, depressive symptoms increased over time. Respondents were grouped in 3 trajectories. While respondents in the stable and not depressed trajectory had low mean scores at all time points (3.14, 3.43, and 3.47, for first follow-up, COVID-19 baseline and exit, respectively), respondents in the declining mental health related to depressive symptoms (6.86, 9.48, and 9.63) and depressed (13.44, 17.28, and 17.39) trajectories had steeper increases between the first follow-up and the COVID-19 baseline interview but were almost stable between the baseline and exit surveys (Figure 1). For all trajectories, CES-D-10 scores were significantly different between the time points (P < .001), except for COVID-19 baseline and exit in the stable and not depressed trajectory. Although similar, the declining trajectory was about 7 points lower than the depressed trajectory at all times. The robustness analysis identified 940 respondents (14.1%) with a similar probability (difference < .15) of being assigned 2 trajectories.

Trajectories of depressive symptoms (n = 6659).
An AFC action plan was not associated with depressive symptom trajectories when no level-1 predictors were added (model not shown), nor when introducing individual-level variables for age, sex, household income and number of chronic conditions (Model 1, Table 2). Women and respondents with lower household incomes and at least 2 chronic conditions were more likely to be in a declining or depressed trajectory of depressive symptoms than in a stable and not depressed trajectory. Participants under 75 had higher odds than older participants of being in a declining than a stable and not depressed trajectory. Smoking tobacco, consuming alcohol, and activities outside the home, except for caregiving responsibilities, were not associated with any of the trajectories (intermediate model not shown). Considering all individual and community predictors, being female, feeling lonely, having at least 2 chronic conditions, a weaker sense of belonging to the local community, and a probable or confirmed case of COVID-19, and experiencing pandemic-related stressors (especially increased verbal or physical conflicts) were more likely to be in a declining or depressed than in a stable and not depressed trajectory (Final Model, Table 2). Feeling lonely and experiencing increased verbal or physical conflict more than doubled the risk of being in the depressed rather than the declining trajectory. Respondents living in a municipality with greater material deprivation had lower odds of being in a declining than in a stable and not depressed trajectory (Table 2). Specifically for the declining trajectory, being younger and material deprivation had a weak protective effect, while having a very low income and less frequent social participation increased the odds of being in a depressed trajectory (Table 2). Finally, the statistically significant random effect indicates that there is still significant variance between municipalities to be explained regarding the depressed trajectory (see Random effect, Table 2). The sensitivity analysis replicated the models without ambiguous trajectory membership (n = 6404) showing low to no differences in terms of odds ratios and significance.
Final Results From Multilevel Multinomial Logistic Regression Model, by Depressive Symptom Trajectories (ref = Stable and Not Depressed; nr = 6659; nm = 50).
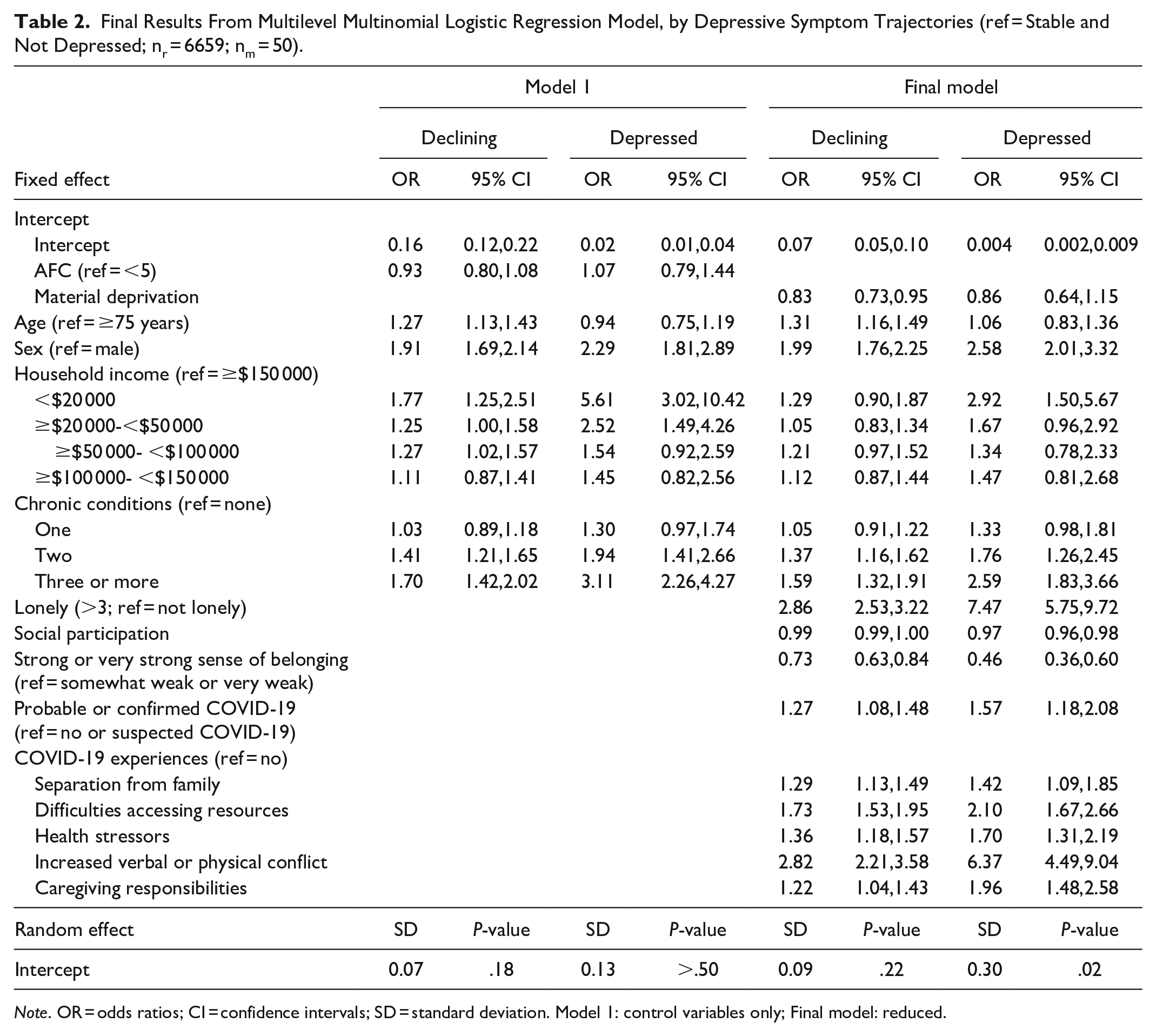
Note. OR = odds ratios; CI = confidence intervals; SD = standard deviation. Model 1: control variables only; Final model: reduced.
Discussion
This study aimed to explore the protective effect of having an AFC action plan on the trajectories of older Canadians’ depressive symptoms during the pandemic, and to examine individual and community predictors of these trajectories. The results did not indicate that having an AFC action plan at the highest level of the AFC initiative process 32 had a protective effect on the trajectories of older Canadians’ depressive symptoms during the pandemic. Nonetheless, the results highlighted the importance of preventing loneliness and verbal or physical conflicts. Going out to buy food was the only activity outside the home during the pandemic that was reported less often by respondents in AFC with an action plan, which could be associated with their weaker sense of belonging, that might be explained by a poorer social network. 39 The unfamiliar challenges created by the current COVID-19 pandemic could have limited the capacity of all communities, including those with an action plan, to support older adults properly. This support could have been reduced, for example, by difficulty recruiting volunteers, which was one of the difficulties reported by community organizations that support older adults. 37
The majority of older adults in the present study were in the stable and not depressed trajectory, despite the COVID-19 pandemic, which is common in studies of depressive symptom trajectories.40,41 For example, in the early pandemic, 3 similar trajectories were observed in British adults. 42 As observed in the current study, the declining and depressed trajectories indicated little improvement in depressive symptoms in the first few weeks of lockdown, followed by a decline when a state of emergency was applied. 19
This study identified individual and community predictors for the trajectories of depressive symptoms. Similar to the United States and Europe, 6 older Canadian women reported higher levels of depressive symptoms than their younger counterparts and men. A lower household income and multiple chronic conditions increased the likelihood of being in a depressed trajectory, both of which predictors had been previously observed in older Canadians 7 and Americans. 8 Loneliness, a weak sense of belonging to the community and restricted social participation predicted being in a declining or depressed trajectory; these social factors had already been recognized as negatively affecting mental health.15,43 Material deprivation was a community factor that had a weak protective effect on the trajectory of older Canadians’ depressive symptoms. This result is surprising, especially since it has been argued that older adults in deprived urban neighborhoods are more likely to experience a “double lockdown” 44 : in other words, in addition to physical distancing for the pandemic, deprived neighborhoods are associated with greater social exclusion. Respondents living in a municipality without an AFC action plan might also have shared favorable characteristics that protected them from depressive symptoms, such as a higher frequency of social participation, a stronger sense of belonging, and not having COVID-19 infections, as highlighted in the present study. Additionally, older adults in wealthier communities with substantial social support may have experienced a greater drop in this assistance during the pandemic, as found with older Americans (n = 12 434) reporting more help than those living in deprived communities. 45 However, according to Fone et al, 46 the adverse effect of income inequality on mental health is more likely to operate at the regional level, where investments in social infrastructure and support are more substantial than at the community level.
Implications
This study’s results did not confirm or refute the effectiveness of AFC action plans but highlighted the importance of not completely isolating residents from their communities, to limit the harm done to mental health. While communities should focus on structuring support networks to provide access to food, medication and care, emergency preparedness must go beyond that.
A prepared community should be ready to provide safe opportunities to reduce loneliness and conflicts, and enhance social support, 47 an essential element during a pandemic, when older adults rely on casual contacts to maintain their social connectedness. 15 Indeed, instrumental support from neighbors was found to be heavily dependent on spatial proximity and important for older adults’ functional independence. 14 Priority should be given to identifying lonely older adults, informing them about support resources and helping them to use them. Many programs providing older adults with safe social opportunities were developed or adapted specifically for the pandemic 48 ; however, they were not necessarily initiated in an AFC action plan but possibly by community organizations or governments. Adapted as an immediate response, these programs should address recovery from the consequences of the lockdown and pandemic adversities, including insufficient mental health support. 49 It is also important to provide neighborhood amenities that respond to older adults’ needs (autonomy, health, well-being, social connection, safety), such as safe transportation, green spaces and public places with services and activities. 14 Future research should verify if social support networks previously established in a community reduce the need to implement an AFC action plan by providing social amenities that foster social belonging.
Strengths and Limitations
Among its strengths, the longitudinal nature of this study allowed depressive symptoms before and during the pandemic to be considered as well as potential exposure to or infection with the virus. The multilevel analyses made it possible to consider the interdependence of respondents nested in the same community. Among the limitations, the CLSA COVID-19 Study included 3 time points and was conducted in the early months of the pandemic (April and December 2020), which may have been too early to allow AFC support services to be fully optimized. The fifth milestone, as described by the Public Health Agency of Canada, 33 requires a commitment to measure activities and outcomes, and does not necessarily imply that the planned initiatives had already been undertaken by the municipalities, which can vary substantially. 36 Lastly, material deprivation was initially measured at the neighborhood level (dissemination area) and was rescaled at the municipality level (census subdivision) by a weighted average, which can flatten the variability of deprivation. 36
Conclusions
This study explored the potential protective effect of having an AFC action plan on the trajectories of older Canadians’ depressive symptoms during the pandemic, and examined individual and community predictors of these trajectories. Having an AFC action plan did not have any protective effect on these trajectories. However, a declining or depressed trajectory was predicted by individual factors, including being female, feeling lonely, having a lower income, having at least 2 chronic conditions, less frequent social participation, a weaker sense of belonging, and a probable or confirmed COVID-19 infection, as well as experiencing pandemic stressors. Future studies should consider coping strategies that facilitate access to resources and allow for safe opportunities for social interactions in outdoor spaces, which are beneficial against depressive symptoms. To improve the development of future interventions, more studies are needed to explore the protective effect of more specific aspects of AFC action plans on the health of older adults and the diverse initiatives that allowed for safe gathering and access to resources.
Supplemental Material
sj-docx-1-inq-10.1177_00469580231225918 – Supplemental material for Effect of Age-Friendly Communities Action Plan on Trajectories of Older Canadians’ Depressive Symptoms Between 2018 and 2020: Multilevel Results From the Canadian Longitudinal Study on Aging
Supplemental material, sj-docx-1-inq-10.1177_00469580231225918 for Effect of Age-Friendly Communities Action Plan on Trajectories of Older Canadians’ Depressive Symptoms Between 2018 and 2020: Multilevel Results From the Canadian Longitudinal Study on Aging by Mélanie Levasseur, Daniel Naud, Verena Menec, Marie-France Dubois, Christina Wolfson, Lauren E. Griffith, Lise Trottier, Jacqueline McMillan, Mélissa Généreux, Mathieu Roy, Yves Couturier and Parminder Raina in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors thank the Quebec Population Health Research Network (QPHRN) for its contribution to the financing of this publication. Material and Social Deprivation Indices (MSDI), indexed to DMTI Spatial Inc. postal codes, were provided by CANUE (Canadian Urban Environmental Health Research Consortium). Material and Social Deprivation Indices (MSDI) used by CANUE were provided by the Institut national de santé publique du Québec (INSPQ). Indices were compiled for 1991, 1996, 2001, and 2011 Census data by the Bureau d’information et d’études en santé des populations [https://www.inspq.qc.ca/en/expertise/information-management-andanalysis/deprivation-index]. Please refer to the Material and Social Deprivation Indices dataset documentation available under the Data section of the CANUE website (![]() ) for additional information.
) for additional information.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Foundation Grant (#148466) from the Canadian Institutes for Health Research. Mélanie Levasseur is a Fonds de recherche du Québec –Santé (FRQS) Senior Researcher (#298996), a Canadian Institutes of Health Research (CIHR) New Investigator (#360880) and she is now a Tier 1 Canada Research Chair (#CRC-2022-00331). Parminder Raina holds the Raymond and Margaret Labarge Chair in Optimal Aging and Knowledge Application for Optimal Aging, is the Director of the McMaster Institute for Research on Aging and the Labarge Centre for Mobility in Aging, and holds a Tier 1 Canada Research Chair in Geroscience. Lauren Griffith is supported by the McLaughlin Foundation Professorship in Population and Public Health. Nicole Basta holds a Tier 2 Canada Research Chair in Infectious Disease Prevention.
Funding to support the CLSA COVID-19 Questionnaire study is provided by the Juravinski Research Institute, Faculty of Health Sciences, McMaster University, Provost Fund from McMaster University, McMaster Institute for Research on Aging, Public Health Agency of Canada, and Government of Nova Scotia. Funding for the Canadian Longitudinal Study on Aging (CLSA) is provided by the Government of Canada through the Canadian Institutes of Health Research (CIHR) under grant reference LSA 94473 and the Canada Foundation for Innovation, as well as the provinces of Newfoundland, Nova Scotia, Quebec, Ontario, Manitoba, Alberta, and British Columbia. This research was conducted using the CLSA Baseline Tracking Dataset version 3.7, Baseline Comprehensive Dataset version 5.2, Follow-up 1 Tracking Dataset version 2.2, Follow-up 1 Comprehensive Dataset version 3.0, and COVID-19 Questionnaire data under Application ID No. 21CON001. The CLSA is led by Drs Parminder Raina, Christina Wolfson and Susan Kirkland.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.