
Abstract
Few studies have investigated whether improve electronic health (eHealth) literacy can alleviate food neophobia in university students. We explored the associations among online health information (OHI)-seeking behaviors, eHealth literacy and food neophobia. A questionnaire-based, cross-sectional study of 5151 university students in China was conducted from October to December 2022. The study used Chinese versions of the eHealth literacy scale (C-eHEALS), and the food neophobia scale (FNS-C), as well as the OHI-seeking behaviors scale. Data were collected through Wenjuanxing software. Analysis of variance, t-tests, the Pearson correlation coefficient and chi-square tests were performed for data analysis. The average (SD) scores of C-eHEALS and FNS-C were 26.81 (5.83) and 38.86 (6.93), respectively. University students in China had a low C-eHEALS and a high FNS-C level, and there were significant differences between the high and low groups of C-eHEALS (P < .001) and FNS-C (P < .001). There was also a significant correlation between eHealth literacy and food neophobia (P < .001), and a lower eHealth literacy level indicated a higher probability of food neophobia occurrence. University students with high FNS-C and low C-eHEALS show more OHI-seeking behaviors. When schools, communities, and parents want to alleviate students’ food neophobia, OHI-seeking training to improve eHealth literacy may be a good intervention.
Keywords
University students with food neophobia face many health problems and seek health-related information online.
A lower electronic health (eHealth) literacy is correlated with a higher probability of food neophobia occurrence, and with increase online health information (OHI)-seeking behaviors,
which indicates that improving eHealth literacy to improve OHI-seeking ability may be a beneficial intervention to reduce food neophobia.
When schools, communities, and parents want to alleviate university students’ food neophobia, improving their eHealth literacy based on OHI-seeking training may be a good intervention.
Introduction
University students increasingly use the Internet to obtain health information. 1 eHealth literacy is defined as multidimensional skills to search, obtain, understand, and evaluate health-related information from electronic resources, and use this information to solve health problems. 2 University students have particular health concerns, such as getting adequate sleep, maintaining a healthy diet, and appearance anxieties, and they are often exposed to the health issues of others on social media. The popularization of eHealth knowledge has a significant impact on the quality of health information sought and retained. The impact of eHealth literacy on an individual’s behaviors varies by country, cultural background, and Internet use,3,4 including OHI-seeking behaviors and dietary behaviors, such as food neophobia.
In 1992, Pliner and Hobden defined food neophobia as an unwillingness or avoidance of eating new foods, 5 and compiled a food neophobia scale in the English language. Food neophobia is a personality trait that affects an individual’s daily food choices. 6 University students are a special social group for whom a balanced diet, reasonable nutritional intake, and healthy eating habits are particularly important for their physical and mental health. However, previous studies have found that Chinese university students have low levels of eHealth literacy, 7 while their levels of food neophobia are high, 8 leading to unhealthy eating habits. Students with food neophobia eat smaller amounts of vegetables, salads, poultry, and fish, 9 so their intakes of protein, monounsaturated fats, and magnesium are insufficient. 10 In 2017, Schnettler 5 conducted a survey on 372 college students in southern Chile, and found that 67.7% of them had food neophobia. Food neophobia is also related to living environments, computer skills, time spent visiting other countries, numbers of visits to ethnic minorities per week, lifestyle behaviors, 11 and the degree of exposure to university students with different cultures. 12
At present, the relationship between food neophobia and electronic health literacy is unclear. Few studies have investigated whether improved eHealth literacy alleviates food neophobia in university students. Therefore, an urgent need exists to conduct this study to explore a variety of interventions that universities, communities, and parents could use to reduce food neophobia in university students.
Methods
Study Design
This non-experimental correlation study used quantitative research methods. Questionnaires completed by Chinese university students were used to explore the correlations between OHI-seeking behaviors and the Chinese versions of the eHealth literacy scale (C-eHEALS) and the food neophobia scale (FNS-C).
Participants
University students (5672) were recruited to fill in questionnaires from WeChat groups of Xinyang University anonymously and voluntarily. They were all native mandarin speakers and voluntary participation. Participants were ineligible if the questionnaires incomplete (eg, completely, unanswered questions, or incomplete personal information). Finally, 5151 participants aged 18 to 22 years were selected (response rate: 90.81%). The participants were in freshman to senior years at university and studying humanities and sciences.
Questionnaires
The C-eHEALS questionnaire (Appendix 1) 13 is a 5-point Likert scale questionnaire comprising 8 items. The scale has excellent reliability: Kaiser-Meyer-Olkin (KMO) =0.914, and Cronbach’s Alpha = 0.933 (Appendix 2). Higher scores indicate higher eHealth literacy.
The Chinese version of the FNS questionnaire FNS-C (Appendix 3) 6 was translated by Zhao (2020) of South China Medical University. 14 FNS-C comprise 10 items with a 7-point Likert scale and good reliability (KMO = 0.723, and Cronbach’s alpha = .663; Appendix 4). Higher scores indicate more severe food neophobia.
The questionnaire on OHI-seeking behaviors 15 asked participants to self-report OHI-seeking behaviors (yes or no) on the Internet in the past 6 months (Appendix 5). The investigation was conducted from October to December 2022. Furthermore, the questionnaire also involves demographic information, such as gender, age, origin, parental education level, major, grade, Internet devices, and quantity.
Data Collection and Analysis
In the study, data were collected with an anonymous questionnaire in Wenjuanxing software. Specifically, the questionnaire link was sent to WeChat groups for university students to fill in the questionnaire anonymously and voluntarily. Additionally, C-eHEALS was divided into 2 levels, low( < 26) and high(≥26), with an average score of 26 points for eHealth literacy (N = 5151). Similarly, FNS-C was divided into 2 levels, low (10-38) and high (38-70) based an average score of 38. Data were tested for normal distribution. Analysis of variance, t-tests, chi-square tests and the Pearson correlation coefficient were performed by SPSS 20 for data analysis.
Ethics Approval and Consent to Participate
This study was performed in compliance with the Declaration of Helsinki. All procedures relevant to study participants were approved by Xinyang University ethics committee. Participation was voluntary. Participants were informed of the study objective and context and provided their written informed consent regarding privacy and information management policies.
Results
Participant Characteristics
The participants were mostly women, from rural areas, and their parents had a low educational level (Table 1). Interesting, the device and network conditions for eHealth information seeking behaviors were available to all participants, so they only lack of corresponding interventions and training. For eHealth literacy and food neophobia, there were significant differences between gender, origin, parental education level, major, and Internet device numbers, excluding grade (P = .940) for eHealth literacy.
Participant Characteristics (N = 5151).
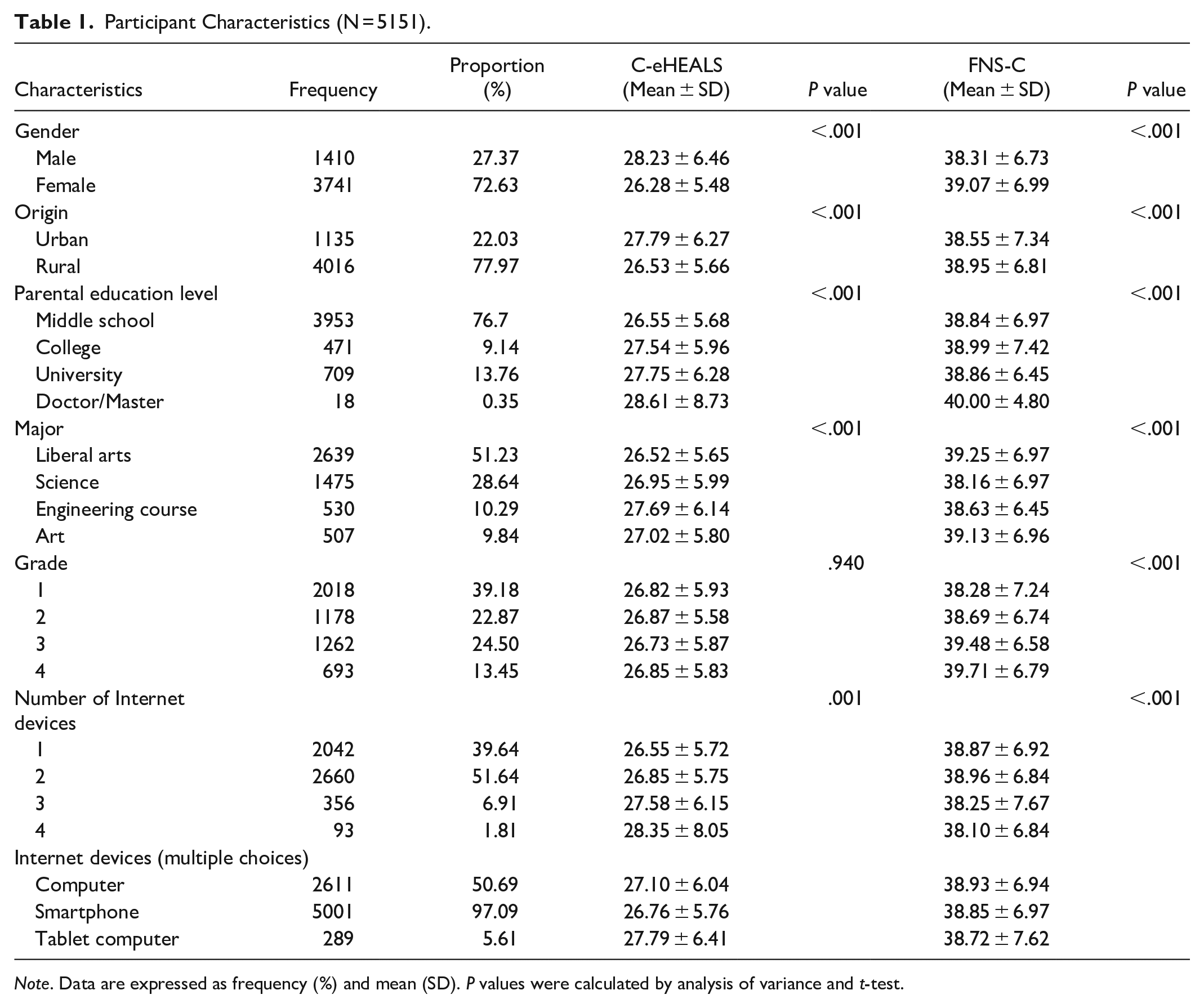
Note. Data are expressed as frequency (%) and mean (SD). P values were calculated by analysis of variance and t-test.
C-eHEALS level
As shown in Table 2, the mean and standard deviation of C-eHEALS scores were 26.81 and 5.83, respectively. The group with low C-eHEALS scores included 57.08% of participants, and the group with high C-eHEALS scores included 42.92%. There was a significant difference between the 2 groups (P < .001). In particular, the mean score of the high C-eHEALS group was 32.11, which was much higher than the overall average score of 26.81.
C-eHEALS Score (N = 5151).

Note. P values were calculated by t-tests.
Food Neophobia Level
As shown in Table 3, the mean and standard deviation of the FNS-C scores were 38.86 and 6.93, respectively. The average score of one item of FNS-C varied from 3.15 (FNS-C5) to 5.24 (FNS-C3). The higher the FNS-C score, the more serious the food neophobia. Therefore, food with unknown ingredients was most likely to be neophobic for university students. In other words, “If I don’t know what a food is, I won’t try it.” The FNS-C low group included 34.15% of participants, whereas the FNS-C high group included the majority of participants (65.85%). There was a significant difference between FNS-C high and low groups (P < .001). Thus, food neophobia affects university students in China at a higher proportion than that previous reported in 2021. 5
FNS-C Score (N = 5151).

Note. An t-test was used.
The Correlations Among OHI-Seeking Behaviors, FNS-C, and C-eHEALS
To analyze the correlations among OHI-seeking behaviors, FNS-C and C-eHEALS, Pearson correlation analysis was conducted. As shown in Table 4, there were significant positive correlations between FNS-C and C-eHEALS with OHI-seeking behaviors excluding 4 items. The same significant positive correlations were found between FNS-C and C-eHEALS.
Pearson Correlation Analysis (N = 5151).

Note. ** indicates a significant correlation at the .01 level (bilateral); * indicates a significant correlation at the .05 level (bilateral).
OHI-seeking behaviors are an important part of eHealth literacy. For each group (Table 5), the OHI-seeking behaviors of participants all had the same variation pattern. Top 3 behaviors were purchasing health care products online (P = .002), reading or sharing health information via social media (P < .001), writing, or sharing health information via social media (P < .05). Apart from finding health or medical information (P = .145) and the last 3 behaviors (P = .556, .319, .940), there were significant differences between the 4 groups (P < .05), and participants’ preferred behavior corresponded to a low level of eHealth literacy. LH and LL group participants were less than HH and HL groups, perhaps because of the higher food neophobia in the HH and HL groups. Comparing the HH group with the HL group, the HL group had a high proportion of participants. This finding suggests that university students with high food neophobia have low eHealth literacy and need to seek more health information online.
OHI-seeking Behaviors of Participants (N = 5151).
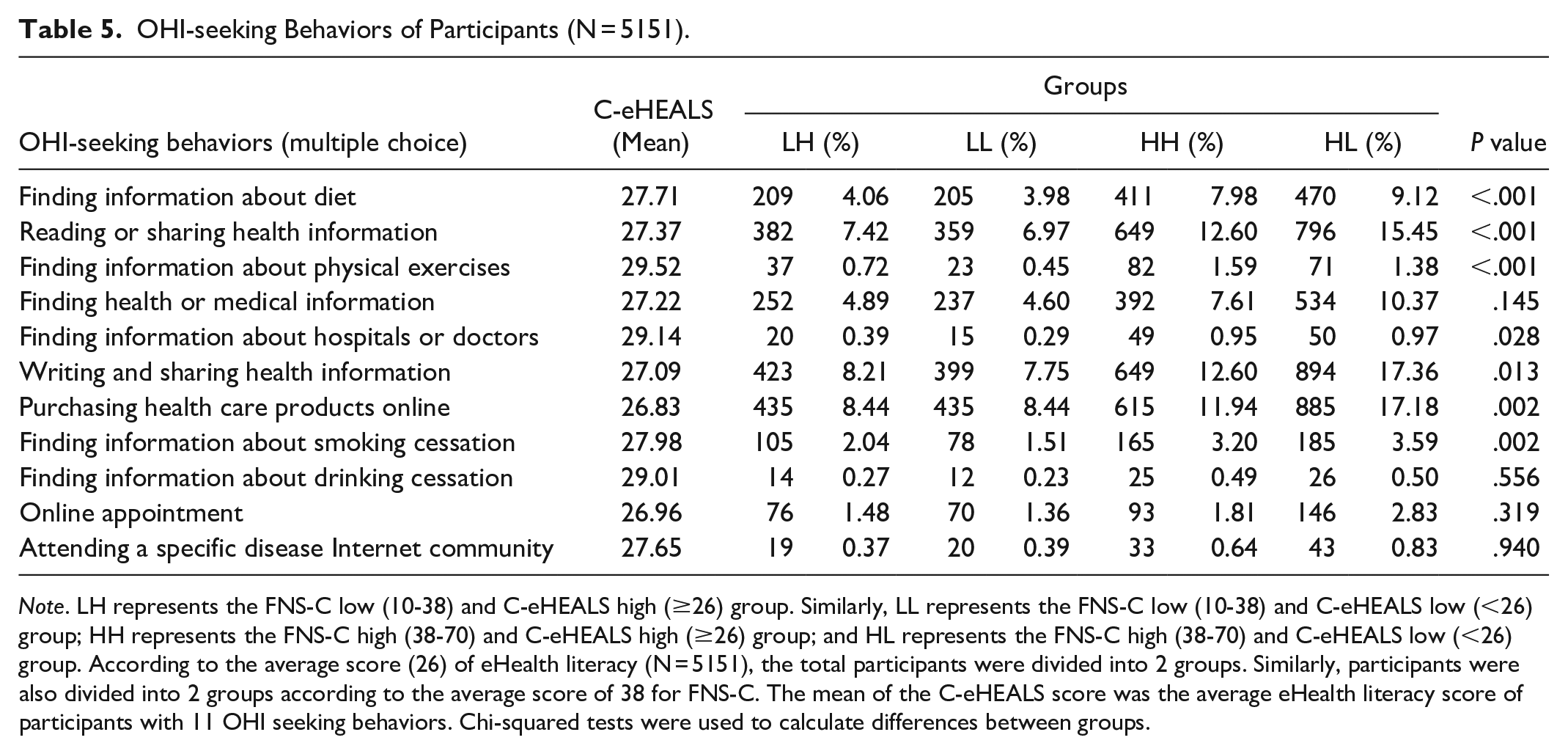
Note. LH represents the FNS-C low (10-38) and C-eHEALS high (≥26) group. Similarly, LL represents the FNS-C low (10-38) and C-eHEALS low (<26) group; HH represents the FNS-C high (38-70) and C-eHEALS high (≥26) group; and HL represents the FNS-C high (38-70) and C-eHEALS low (<26) group. According to the average score (26) of eHealth literacy (N = 5151), the total participants were divided into 2 groups. Similarly, participants were also divided into 2 groups according to the average score of 38 for FNS-C. The mean of the C-eHEALS score was the average eHealth literacy score of participants with 11 OHI seeking behaviors. Chi-squared tests were used to calculate differences between groups.
Discussion
The average score of C-eHEALS in this study was 26.81, which is lower than the average score in young adults from Pakistan (29), 16 American college students (31.9), 17 and adults from Iran (28.2) 18 and Kuwait (28.6). 19 In some Asian, American, and European countries, the eHEALS scores of the general population are also relatively high, ranging from 28.1 to 30.5.20 -22 Only the scores of Japanese adults (23.4) 23 and college students (23.6) 21 were lower than the scores in this study. These findings indicate that the level of eHealth literacy among Chinese university students urgently needs to be improved. For universities, parents, and the community, the current focus is on how to improve eHealth literacy. Designing and implementing intervention measure is needed. For example, improving computer skills, social support, and education are all factors that need to be considered.
The average score of food neophobia in this study was 38.86 (n = 5151), which is a higher score than that of university students from Xinyang Normal University (36.27), 5 and South China Medical University (33.59) 14 in China, and others in Lebanon (36.4), 24 and Southern India (37.3-38.9). 12 Furthermore, the FNS-C average score in this study was much higher than that reported countries in the United States (29.80), 26 United Kingdom(26.67-30.30), 25 Spain (31.74), 26 in Finnish youth (32.3), 27 and in South Korea (33.50). 28 It is shown that less developed areas seem to have higher food neophobia scores. In this study, 77.97% of participants came from rural areas, and 76.74% of their parents only had a middle school educational level. Previous studies have also shown that educational level and eating habits impact on young people’s food choices, dietary behaviors, and food-related well-being. 29
Food neophobia is influenced by personal variables, such as gender, age, marriage, race, education level, computer skills, urbanization level, and the economic status of the place where the individual lives. 26 This exploratory study found that Chinese university students are likely to focus on purchasing health care products online and reading, writing, or sharing health information via social media. These 3 OHI-seeking behaviors were highest among participants in the HL group, possibly because their FNS-C scores were high and C-eHEALS were low.
The university students with high FNS-C may be more able to understand the health risks related to food neophobia because of their high educational level, 30 so they ensure that they obtain sufficient eHealth information. University students with low C-eHEALS might not be able to obtain more health-related information online because of barriers including access and skills. 31 In summary, there is an interactive association of OHI-seeking behaviors between eHealth literacy and food neophobia. University students with low eHealth literacy only have access to limited OHI, which may hinder the reduction of food neophobia. Similarly, university students with high food neophobia have poor acceptance of eHealth information conducive to health, which may hinder improvement in eHealth literacy. OHI-seeking behaviors are a useful perspective for interventions for reducing food neophobia.
In this study, all students had Internet devices, and more than half of the students had 2 devices, especially smartphone. The 5G network is unblocked and can be used anytime and anywhere. The device and network conditions for eHealth information seeking have been provided. Appropriate intervention measures to reduce food neophobia should be undertaken according to different students’ eHealth literacy and OHI-seeking behaviors. In particular, universities should fully leverage their educational functions, conduct sufficient courses and training, and pay attention to eHealth literacy and food neophobia from multiple perspectives, such as the environment, culture, nutrition, and psychology.
Limitations
This study had several limitations. First, this study had a cross-sectional design, which means that causality cannot be determined. Second, the findings only theoretically infer the effectiveness of eHealth literacy in alleviating food neophobia. Further empirical support is needed, such as continuous dietary observation and interviews. Third, data were obtained from a self-administered questionnaire, which may create some biases in the results. Although our study included more than 5000 university students from different university years and majors, there may be some biases in the results because of the anonymity, freedom, and voluntary nature of participating in the study. However, this heterogeneity still provides insights to this study. Future health professionals need further eHealth literacy training based on OHI-seeking ability to explore various interventions for university students’ food neophobia.
Conclusions
This exploratory study focused on associations among OHI-seeking behaviors, eHealth literacy, and food neophobia in university students in China. The results showed that the C-eHEALS scores of university students are low, while the FNS-C scores are high. The low eHealth literacy level indicates the higher probability of food neophobia occurrence. University students with high food neophobia need to seek relevant health information online. Therefore, when schools, communities, and parents consider exploring ways to alleviate university students’ food neophobia, improving their eHealth literacy by designing and implementing OHI-seeking methods and content may be a good intervention. Especially for universities, offering enough courses to enhance computer skills, OHI-seeking skills, and strengthening teachers’ guidance on eHealth literacy and food neophobia are also effective interventions for university students.
Supplemental Material
sj-docx-1-inq-10.1177_00469580231217982 – Supplemental material for Associations Among Online Health Information Seeking Behaviors, Electronic Health Literacy and Food Neophobia: A Cross-Sectional Study
Supplemental material, sj-docx-1-inq-10.1177_00469580231217982 for Associations Among Online Health Information Seeking Behaviors, Electronic Health Literacy and Food Neophobia: A Cross-Sectional Study by Hua Tian and Jie Chen in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The author would like to thank Nanhu Scholars Program for Young Scholars of XYNU.
Abbreviation
OHI-seeking, online health information seeking; eHealth literacy, electronic health literacy; C-eHEALS, Chinese eHealth literacy scale; FNS-C, Chinese food neophobia scale; KMO, Kaiser-Meyer-Olkin.
Author Contribution
Jie Chen drafted and revised the manuscript. Hua Tian performed the statistical analysis. Both authors read and approved the final manuscript.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Nanhu Scholars Program for Young Scholars of XYNU (Xinyang Normal University, China), Education and Teaching Reform and Key Research Projects in Xinyang Normal University (XYNU [2022] No. 69) and UGS teaching reform research project of plan to strengthen basic education teacher force of Xinyang Normal University (2022-GTTZD-01).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.