
Abstract
As a result of working conditions, a variety of determinants or risk factors lead to the development of occupational health and safety impairments or outcomes such as injuries and musculoskeletal disorders among sanitary personnel, which must be identified in order to anticipate concerns. PubMed, Medline, Embase, and Lilacs databases were used from 2010 to April 2022. Searched strategies used logical words “AND/OR”: Occupational *OR Work AND Injuries OR Musculoskeletal Disorder AND Associated Factors [Socio-demographic *OR Behavioral factors *OR Institution Factors *OR Work pattern] AND Sanitary workers [Waste collectors and emptier *OR Street Sweepers *OR Sewage workers *OR Health facilities Cleaners] AND Cross-Sectional Studies. The databases and other collected data and reports yielded a total of 86 studies and finally 16 studies were included. From total of sanitary workers (5833), 4990 (85.5%) were solid waste collectors, and 618 (10.6%) and 225 (3.9%) were and healthcare cleaners and street sweepers, respectively. Regarding associated factors, Age (OR: 22.57, 7.29-69.88); education (OR: 2.22, 1.22-4.00); and experience (OR: 1.92, 1.11-3.31) were predictors for occurrence of injuries. Smoking cigarettes (OR:2.6, 1.55-4.34); sleeping disturbance (OR: 2.57, 1.48-4.47); eating/smoking/drinking at work (OR: 3.85, 1.34-11.06); and lack of personal protective equipment (OR: 2.62; 1.48-4.63) are the other predictors. On other side, Education (OR: 6.73, 1.92-23.51), age (OR: 7.56, 2.18-26.18), and job experience (OR: 10.79, 3.49-33.38) are socio-demographic variables that impact the development of MSDs. Cigarette smoking (OR: 0.14, 0.03-0.64) and job satisfaction (OR: 11.43, 2.04-64.08) are behavioral factors. While, working longer than 8 h (OR: 3.5, 1.543-8.204) and time pressure (OR: 3.25, 1.08-9.77), working for more than 2 h (OR: 8, 2.25; 28.85) and having a bad back (OR: 15.7, 6.47-38.18) were risk factors for MSDs where all P-value < .05. According to current reviewed evidence, socio-demographic indicators, occupational safety with work pattern features, and behavioral factors all significantly contributed to musculoskeletal disorders; occupational injuries among sanitation workers, which require emphasis from government policy and other initiatives.
Now –a- day, the burden of occupational health and safety outcomes commonly observed in all employee and workers particularly among sanitary workers due to variety of determinants. It also as the result of their working conditions, unsafe, unhygienic, more exposed with different type of wastes in all work setup like in the municipality, in the factories, commercial, health care facility sectors and plants. Moreover, a lot of studies indicated that sanitary workers are exposing with numerous occupational hazards and accidents. Also, they are discriminated, violated and ignored groups from the rest of the societies. However, only few studies have been conducted on the quantifying associated factors of occupational related outcomes among these groups, which was our current work to conducted systematic review across the world.
This Systematic review report give the evidence on determinants of occupational health and safety outcomes among sanitary workers across the world, which is not properly reported yet. Therefore, this review slightly gives overall prevalence of occupational related injuries their work setups across the world.
The study provides that government bodies particularly Ministry of health; and Ministry of Social affairs and other associations should be amended and incorporated the occupational health and safety policy, regulations and guideline for work place factors among these groups in any work setup. Then, it needs to enforce and monitor these amendments for further implementation in any work giving sector.
Introduction
Sanitation workers encompasses a vast line of services, the number of sanitation workers globally is difficult to estimate because they often have multiple jobs or are categorized with other sectors like solid waste and healthcare facility management. 1 However, they are facing many challenges like issues related to their health and safety problems such as musculoskeletal disorders, injuries, respiratory problems, gastro intestinal problems and infectious diseases, dermatitis, rhinitis, hepatitis B and C, parasitic diseases, eating disorders and sleep, depression, neurosis, allergic and toxic reactions, HIV, acute or chronic infections.2,3 As the result, millions of sanitation workers across the world particularly in low income countries and middle-income countries are forced to work in conditions that endanger their health and lives, and violate their dignity and human rights.1,4
The review only limited to self-reported from occupational related injuries and musculoskeletal disorders from the result of occupational health and safety (OHS) outcomes. occupational related injuries are self-reported injuries that included physical harm caused by accident or disease associated with the occupational exposure. Includes self-reported, clinically confirmed or others recorded morbidity or mortality, including but not limited to punctures, abrasion, laceration wounds, cuts, or blunt force trauma. 5 While, Musculoskeletal disorders is self-reported and 9 body regions of sanitary workers such as Neck, shoulder, upper back, elbow, lower back, wrist/hand, hips/thighs/, knee and ankle/feet trauma. 5
A lot of studies found that safety measures, lack of institutional support, lack of education, high or low of experience sanitary workers, behavioral factors, lack of supervisor, unregulated or unenforced environmental and labor protections, lack of pre-job training and lack of are the most common associated factors for occurrence of these outcomes. 6 Moreover, there was poor social recognition for these group: As evidence indicated professional cleaning is often considered as unskilled extra work that everyone knows how to do. The fact that cleaning receives poor social recognition is a factor affecting negatively the cleaners’ motivation and identification with the work. 7 Even some sanitary workers themselves are of the opinion that cleaning is a job that does not require special qualifications and that anyone can do it. 8 Low appreciation of the job tends to harm workers’ satisfaction and lead to stress, with subsequent negative effects on mental and physical health. 9
In this review, the associated factors are limited to occupational injuries and musculoskeletal disorders. The occurrence of occupational related injuries could be due to difference of gender10,11; Marital status and family size.11,12 The other factors are work experiences10,12,13; Training.3,13 -16 The other factors are due to formal education and majority of sanitary workers are illiterate13,17 and low income. 13 Moreover, environment satisfaction, 18 job satisfaction, sleeping disorder 13 and job stress 13 are also associated factors for occurrence of occupational related injuries. In addition, alcohol consumption, Khat chewing and cigarette smoking3,19 are also other associated factors. In this review institution factors could trigger an employee’s action that could lead directly or indirectly to an occurrence of an accident and injury due to less attention of institutions, work overload and lack of follow up.3,15,16,20
Moreover, there were a lot of associated factors for development of musculoskeletal disorders among sanitary workers. As studies indicating work experiences were significantly more likely to suffer from MSDs.21 -23 From these evidences we learnt, as work experience increases, the development of MSDs also increases among sanitary workers. Moreover, the respondents over the age of 40 years old were 5.41 times more likely to developed MSDs of the knee as compared to less than 30 years old. 23 Therefore, increment of age leads to development of MSDs among sanitary workers. Furthermore, Job satisfactions: It also found to be significantly correlated as the sanitary workers who were not satisfied with their job were more likely to have suffered from the MSDs. 21 Moreover, those had time pressure, feeling exhausted, and working hours more likely to develop MSDs as compared to those didn’t have.12,24
The study revealed that the those working in high slum concentration areas and those came far from working place were more likely to get MSDs as compared with those working in the low slum concentration areas. 21 While, distance and length of the broom, there was a positive association with weight of broom, and total weight of broom and dustpan. 25 Those working in awkward posture and sustaining position more than 2 h were more likely to develop MSDs as compared to the counterpart. 24 Furthermore, the study indicated poor mental health status were significantly more likely to report MSDs for upper back and shoulders, respectively as compared to those had good mental health. 22 Therefore, the aim of this review was to identify associated factors for occurrence of occupational health and safety outcomes and intensify the problems to the world for better solution. Finally, this review will attempt to publication for further scholars and policy makers in order to sustain the sanitary workers.
Method and Materials
Review Protocols
For the flow diagram, Preferred Reporting Items for Systematic Reviews (PRISMA) updated criteria was used. 26 PICOS (Population, Intervention, Comparison, Outcome, and Study type) was used for the developed systematic review questions, which was adapted from Amir-Behghadami and Janati. 27
Study Eligibility Criteria
Inclusion criteria
i. Population (P): -It stands for sanitary workers, namely, solid waste collectors, health care facility cleaners, sewage workers, waste treatment workers and sweeping streets
ii. Intervention(I): -Associated Factors of Occupational exposure
iii. Comparison (C): -Not applicable
iv. Outcome(O): -Occupational or job or any work-related injuries and musculoskeletal disorders
v. Study type(S): -Cross Sectional study.
vi. Language: All studies published in English Language
vii. Articles/Studies: Articles with their full texts and abstracts, reports, dissertations, conference papers, and other non-peer-reviewed sources with clear objectives and methodology were included
viii. Publication Year: 2010 to 2022
ix. Countries: Both low-income- and high-income countries
Exclusion criteria
i. Population: Office cleaners, hotel, and restaurant cleaners were excluded in this review due to their work type and characteristic about their job.
ii. Outcomes: Studies on occupational associated respiratory track and gastro intestinal problems, track and other non-occupational related accident didn’t include
iii. Study Design: Non-cross-sectional studies like Randomized controlled trials (RCTs) that are individually or cluster RCTs. The following non-randomized controlled studies (NRS): quasi-RCTs, non-RCTs, controlled before and after studies, case-control studies, and cohort studies.
iv. Language: Studies published in non-English languages.
v. Articles/Studies: studies that haven’t clear objectives and methodology, studies excluded
vi. Publication: Studies published prior to 2010 were not included.
Searching Engine and Strategies
Searching engine such as PubMed, Medline, Embase, and Global Health electronic databases, as well as Cochrane Library and Web of Science were used. The keywords and MeSH (Medical terms with Boolean logic operators (AND, OR) were used individually or in conjunction as the following: Occupational *OR Job *OR Work AND Occupational Injuries OR Musculoskeletal Disorder AND Cross-Sectional Studies AND Associated Factors [Socio-demographic Character *OR Behavioral factors *OR Institution Factors *OR Work pattern] AND Sanitary workers [Waste collectors and emptier *OR Street Sweepers *OR Sewage workers *OR Health facilities] AND Countries [Developed or High-income countries *OR Developing or Low-income countries].
Data Extraction
A specified extraction form created in a Microsoft Excel spreadsheet was used to extract data. It includes the reference number, primary authors, years, country, job categories, assessment tool, and quality evaluation.
Data Screening
Titles and abstracts returned by the search were screened by using Microsoft excel and full copies of titles and abstracts were obtained. Then finally, the results from the databases were managed and duplicates were removed in the reference management software, Zotero.
Data Synthesis
Eligible studies for associated factors of occupational injuries and musculoskeletal disorders were synthesized according to their kind and corresponding associated variables. Then number of population and number of studies were explained by numeric, percentage with tabulation and charts.
Quality Assessment
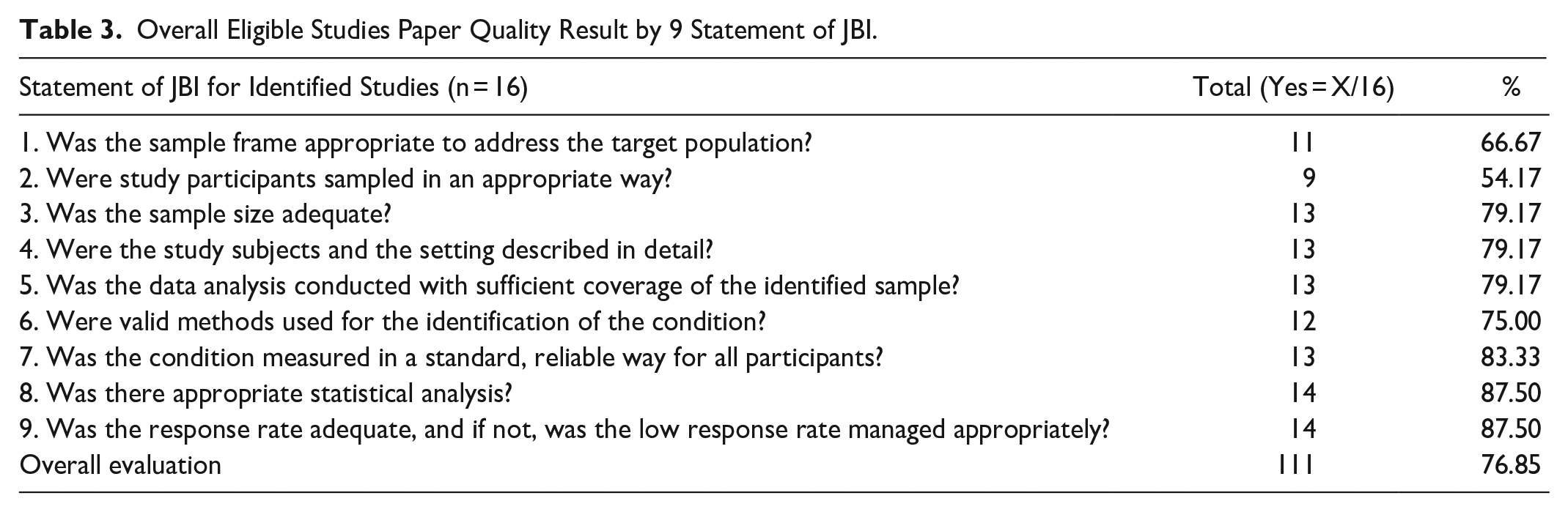
All quality of published studies was appraised using JBI Critical appraisal checklist Table 3, which was developed for cross sectional studies adapted from Munn et al. 28 It has 9 criteria that and all these criteria measured as (1) Yes, (2) No, (3) Unclear, and (4) Not applicable. If accounted 5 Yes, it is high publication risk or low quality of paper, if 5-7, it is medium and if 8-9, it is low publication bias.
Result
Selection Studies
The databases and other collected data and reports yielded a total of 86 studies. Three of these studies were included in the previous version of the review, 65 were new research via databases and registers, and 17 were new studies via other approaches and 4 studies from the previous review. As a consequence, 16 studies were included (Figure 1).

Flow diagram for systematic reviews adopted from PRISMA 2021.
Studied Population
From total of reviewed sanitary workers (5833), majority of them 4990 (85.5%) were municipal solid waste collectors. The remaining 618 (10.6%) and 225 (3.9%) were and healthcare cleaners and street sweepers, respectively.
Techniques of Statistical
More than half percent (53%) of the authors used logistic regression to regret associated factors with occupational related injuries and musculoskeletal disorders among sanitary workers. The remaining 39% of them used chi-square with another model and 8% of them used chi alone (Figure 3).
Overall Quality of Paper
The total quality of the articles was supposed to be 9 × 16 = 114 according to JBI standards. However, in our evaluation, the total paper quality was 111/144 (73.80%), which met the JBI requirements (Table 3). The quality of article discovered as medium publication and low publication bias accounted for 56.25% and 43.75%, respectively (Tables 1 and 2).
Associated Factors of Occupational Related Injuries Among Sanitary Workers Across Worldwide.
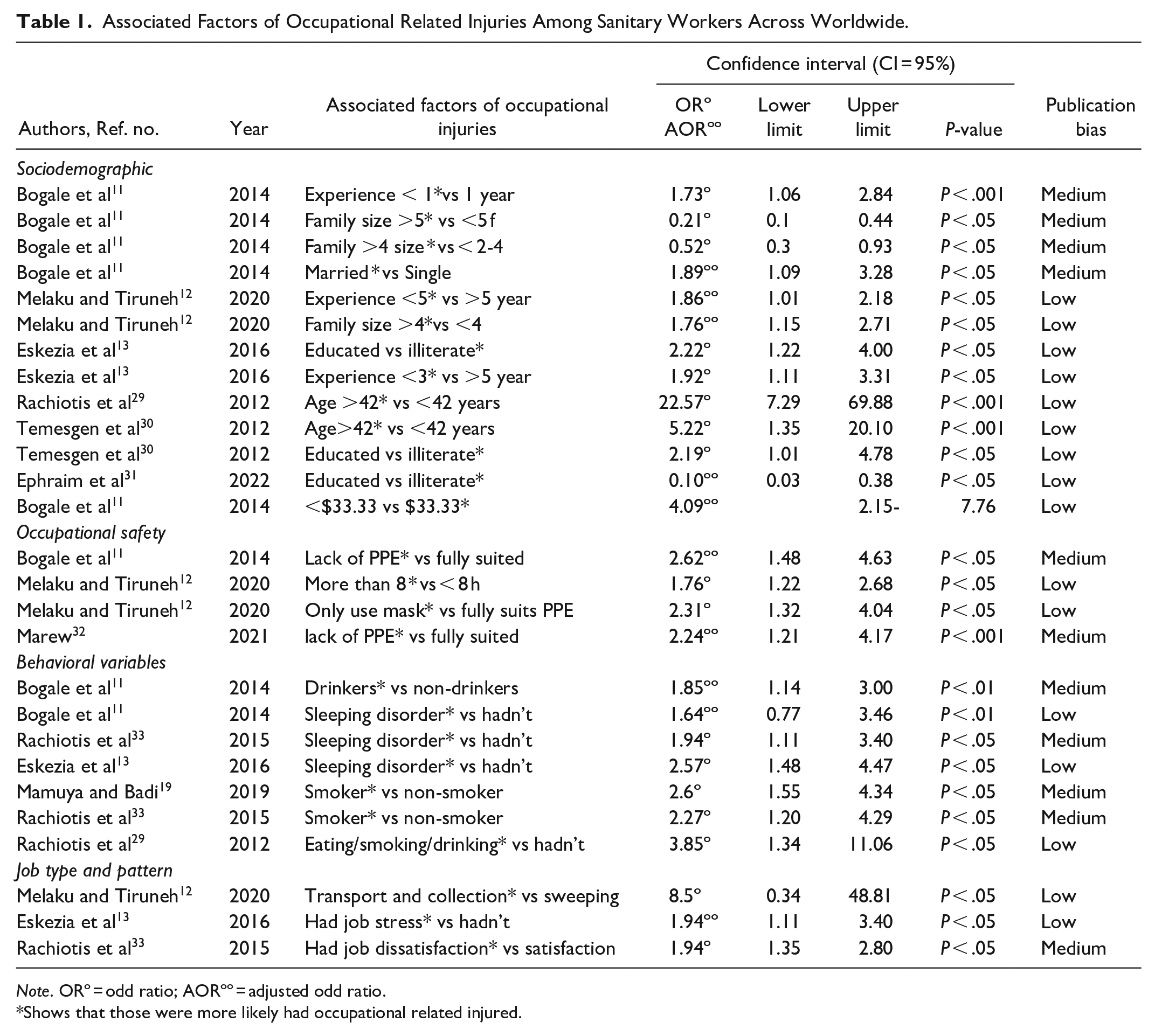
Note. ORº = odd ratio; AORºº = adjusted odd ratio.
Shows that those were more likely had occupational related injured.
Associated Factors of Musculoskeletal Disorders Among Sanitary Workers Across Worldwide.

Note. ORº = odd ratio; AORºº = adjusted odd ratio.
Indicates that they are more likely to acquire MSDs than their counterparts.
Associated Factors of Occupational Injuries
Sociodemographic such as age (OR: 22.57, 7.29-69.88; P < .05), education (OR: 2.22, 1.22-4.00; P < .05), and work experience (OR: 1.92, 1.11-3.31; P < .05) were the significant predictors for the occurrence of occupational injuries. While, cigarette smoking (OR: 2.6, 1.55-4.34; P < .05); sleeping disorder (OR: 2.57, 1.48-4.47; P < .05); eating, smoking, drinking at work (OR: 3.85, 1.34-11; P < .05) were behavioral factors to incur occupational injuries (Table 1).
Associated Factors of Musculoskeletal Disorders
Socio-demographic variables such as education (OR: 6.73, 1.92-23.51; P < .05); age (OR: 7.56, 2.18-26.18; P < .05); work experience (OR: 10.79, 3.49-33.38; P < .05) were the most significant predictors for the development of MSDs. While. Meanwhile, cigarette smoking cigarette (OR: 0.14, 0.03-0.64; P < .05) were behavioral factors for MSDs development. From Occupational safety variables such as time pressure (OR: 3.25, 1.08-9.77; P < .05); working more than 8 h (OR: 3.5, 1.54-8.20; P < .05) were associated factors for development of MSDs impairments (Table 2).
Discussion
A total of 86 studies found from the databases and other sources and of these, some of them removed due to duplicates, unmatched design, outdated, mixed with other occupations out and unfit output; with unknown population, unclear methods and output. As the result, 16 studies were included for associated factors of occupational related injuries and musculoskeletal disorders (Figure 1). From these, 9 studies were used to identify the associated factor for occurrence of occupational injuries11 -13,19,29 -33 and 7 studies were to identify the associated factors for development of MSDs.21 -24,34 -37 Moreover, from 7 studies11 -13,19,29 -33 were gathered through research done on related variables of occupational injuries. Geographically, 5 studies found from Ethiopia,11 -13,30,32 2 studies found from Greece.29,33 1 study from Ghana, 31 and 1 study from Tanzania. 19 Meanwhile, 7 studies21 -24,34,36,37 were identified for associated factors of MSDs. Of these, 4 studies found from India,21 -23,34 Ethiopia, 24 Thailand, 36 and Nigeria. 37
As eligible population, the ranges of age and work experience for eligible participants were between 19 to 45-year-old and 6 months to 15 years, respectively. Moreover, from 5833, majority of them were solid waste collectors (85%), which were obtained from Refs.11 -13,21-24,29-32,34 -37 The rest approximately 11% and 4% were obtained health care cleaners24,36,37 and street sweepers,21,35 respectively (Figure 2). Moreover, 3967 (68%) of these sanitary employees were gathered through research done on related variables of occupational injuries. Meanwhile, the remaining 1866 (32%) were derived from research on MSD-related variables (Figure 2). In term of study design, The more than 3-quarters of the studies utilized cross sectional studies with an observational checklist11 -13,19,21-24,29 -37; 3 studies used cross sectionals with a control group12,13,29 and 2 studies used cross sectionals with a focus group discussion.24,34 In terms of statistical models, more than half percent of the authors used logistic regression, binary and multiple regression analysis, as well as bivariate and multivariate regression analysis to regret associated factors with occurrence of occupational injuries and MSDs development. About 13% of the authors used Chi-square with additional models such as chi-square with Fisher’s exact test, logistic regression, multiple comparison, and binary logistic regression and only 8% Chi-square alone used for the same purpose (Figure 3).

Number of eligible populations for systematic Review across the world.

Statistical used for assessment of associated factors of OHS outcomes.
In terms of the quality of eligible articles, each of the 16-studies included in this systematic review was evaluated using the JBI criteria, which consist of 9 assertions. Accordingly, low publication bias accounts for 56.25% (9/16) of the total, followed by medium publication bias 43.75% (7/16) of the total (Table 1). The overall quality of eligible studies met more than 3-quarters of the JBI criteria based on descriptive evidence quality (Table 3). However, one-fourth didn’t meet the criteria and this implies that it is the presence of bias due to chance and low methodological quality of smaller studies, where selection bias is very predominant problem in this review. The method utilized to sample study participants in a suitable way, the sample frame used to address the target population, and the issue with using reliable techniques to identify the condition are some of these. The majority of research did not outline the inclusion/exclusion criteria and method of selection for the workers who perform workplace cleanliness.
Overall Eligible Studies Paper Quality Result by 9 Statement of JBI.
Regarding to associated factor of occupational health and safety outcome, occupational injuries and MSD will be discussed separately as below.
Factor for Occupational Injuries
Associated factor of occupational injuries, they can be classified into socio-demographic characteristics, occupational safety variables, and behavioral variables, all of which have been presented in Table 1. All of the factor categories are addressed in detail below. Sociodemographic factors: One of the risk factors for occupational injuries was the age of the sanitary personnel. Rachiotis et al discovered that people over the age of 42 were 22.57 times more likely (OR: 22.57, 7.29-69.88) to be exposed to the occupational associated infections than those under the age of 42. 33 Rachiotis et al with other study also indicated that waste collectors being greater than 42 years old 5.22 time more like (OR: 5.22, 1.35-20.1) were independently associated with the anti- hepatitis B virus infection positivity exposed to waste (OR: 4.05, 1.23-13.33) as compared to less than 42 years. 29 The other one is gender, one study found that male workers were 2.2 times more likely to be injured (OR: 2.2, 1.39-3.56) than female workers. 11
This can be explained by the fact that the majority of males conduct heavy work such as hauling, lifting, and loading vehicles, whilst the majority of females perform jobs such as rubbish transfer from the roadside to a local transfer station. The third factor is the marital status of the sanitation workers. According to the findings of this study, married workers were 1.89 times more likely to be injured (OR: 1.89, 1.09-3.28) than single. 11 Furthermore, this study found that those with 2 or fewer children had a 79% lower risk of occupational injury (AOR: 0.21, 0.10-0.44) than those with 5 or more children. 11 Similarly, the odds of injury were cut in half for individuals with 3 to 4 children (AOR: 0.52, 0.30-0.93). 11 According to the other study, those had family size of more than 4 were 1.76 times more likely to experience occupational problems (AOR:1.76, 1.15-2.71) than those with a less 4 family size. 12 The fourth factor is work experience, in which sanitary workers had more than 1 year of experience were 1.73 times more likely (OR: 1.73, 1.06-2.84) than their counterparts to have occupational injury. 11 The other study also reported that those have more duration of employment was associated with the risk of occupational infection (OR: 3.57, 1.15-11.08) as compare with counterpart. 33 The other study also found that the likelihood of occupational injury was found to be significantly higher (OR:1.92, 1.11-3.31) among respondents with 3 or less service years. 13 In contrast, sanitary workers with more than 5 years of experience were 1.86 times more likely to suffer occupational complaints than those with less than 5 years of experience (AOR: 1.86, 1.01-2.18). 12 The fourth one is a monthly salary. According to one study, having less than $33.33 monthly pay was 4.09 times more likely to get harmed (AOR: 4.09, 2.15-7.76) than having more than $33.33 monthly salary. Furthermore, illiteracy was 2.22 times (AOR: 2.22, 1.22-4.04) more common among wounded waste collectors than among literate waste collectors. 13 The sixth factor is education, which was independently associated occupational infection (OR: 2.19, 1.01-4.78) as study reported among sanitary workers from Greece. 33 Occupational safety variables: According to certain research, a lack of PPE was strongly connected with occupational injury among solid waste collectors. Ephraim et al reported that those lack of PPE during waste collecting and transportation were 2.24 times more likely than those involved in other work activities to incur an occupational injury (AOR: 2.24, 1.21-4.17) as compared to those had PPE. 31 Moreover, another study found that those didn’t wear a mask were 2.31 times more likely to experience occupational problems (AOR: 2.31, 1.32-4.04) than those who wore a full body suit. Moreover, those worked more than 8 h per day were 1.76 times more likely to develop occupational symptoms than those who worked 8 or less hours per day (AOR: 1.76, 1.22-2.68). 12 According to the study, who did not use PPE at all times while on duty had 2.62 times more injured (AOR: 2.62, 1.48-4.63) than those who did PPE at all times while on duty. 11 Behavioral Variables: The study’s findings demonstrated that alcohol use was statistically connected with the occurrence of occupational injury. The study found that those who ate, smoked and drank during waste collection were 3.85 times more likely to be had occupational related infections (OR: 3.85, 1.34-11.06) than those who did not. 33 The other study on other side, found that alcohol use and cigarette smoking were found to be statistically associated with occupational injury in this study. For example, one study found that alcohol users were 1.85 times more likely to be injured (AOR: 1.85, 1.14-3.00) than non-alcohol users. 11 In same manner, cigarette smokers were 2.60 times more likely than nonsmokers to be injured (OR: 2.60,1.55-4.34). 19 Furthermore, those who reported job-related sleeping disturbance had 2.57 times (OR: 2.57, 1.48-4.47) higher risk of occupational injury than their counterparts. 13 The final is job related stress, which is 1.94 times more likely to occur (AOR: 1.94, 1.11-3.40) than not having job stress, indicating that it was significantly positively correlated with occupational injury. 13
Factor for Musculoskeletal Disorders
The second OHS outcome was MSDs, where socio-demographic characteristics variables, occupational safety variables, and behavioral variables, work design and pattern, material used, work location, distance, and body mass index were significantly associated with it (Table 2). Socio-demographic Variables: As study indicated male sanitary workers were 3.06 times more likely to develop MSDs than (AOR: 3.06, 1.19-7.87) as compared to female sanitary workers. The second socio-demographic factor was job experience, with sanitary workers with 10 years or more experience being 10.79 times more likely to suffer from MSDs in the elbows (OR: 10.79) than those with less than 10 years of experience. 21 Moreover, sanitary workers who had more than or equal to 6 months of work experience were 3-times more likely to develop MSDs compared to those who had less than 6 months (AOR: 2.5, 1.12-5.52). MSDs are the cumulative effect of repetitive physical load and work experience was found to be positively associated with MSDs among cleaners. 24 Similarly, an increase in work duration was correlated with an increase in complaints of MSDs in different parts of the body. For instance, respondents working for more than 10 years were more likely to report MSDs of the shoulder (OR:2.01) compared to those who had been working for 4 years. Moreover, the respondents over the age of 40 were 5.41 more likely to experience MSDs of the knee (OR: 5.41) compared to those in the 18to 30-year-old age group. 23 As contrast, one study highlighted that the complaints of MSDs were significantly 3.04 times higher among aged 35 years old and above (OR: 3.04) as compared to 19 to 34 years old. 22 This study also stated that waste loader those who were working for 10 or more years were more likely to suffer from MSDs for shoulders (OR: 4.57) compared to those working for less than 10 years. 22 As expected, those having 10 or more years of engagement in waste loading were significantly 5.78 times more likely to report disabilities for wrists/hands as compared to those working for less than 10 years.
Behavioral variables: As a study reported that sanitary workers those having 2 or more types of addiction were 3.03 times more likely to develop MSDs (OR: 3.03) as compared to those who were not consuming any substances. 22 Distance and length of the broom, time pressure and exhaustion: Distance and length of the broom, there was a positive association with working experience, weight of broom, and total weight of broom and dustpan (P < .05). 35 The study found sanitary workers who had time pressure while performing their tasks were 3.2-times more likely to develop MSDs (AOR: 3.25, 1.08-9.77) compared to those who had no time pressure. 24 Moreover, this study also revealed that those who felt exhausted after their work were 2.7 times more likely to develop MSDs than (AOR: 2.7, 1.16-6.20) as compared to those who had not felt exhausted. 24
Occupational Safety variables: The other study indicated that those working hours greater than or equal to 8 h/day 3.55 times more likely to develop MSDs (AOR: 3.55, 1.54-8.20) than those less than 8 h/day. 24 Moreover, cleaners those who work more than 2 h in a sustaining position were 8.05 times (AOR: 8.055, 2.25-28.85) as compared to less than 2 h in a sustaining position. 24 Moreover, the other study indicated that those working hours greater than or equal to 8 h/day 4.64 times more likely to develop MSDs (AOR: 4.64, 2.12-6.98) than those working hours less than 8 h/day. 37 Posture and work Design and pattern: As study found cleaners working in an awkward position were 15-times more likely to develop MSDs and were strongly associated with MSDs (AOR: 15.7, 6.47-38.17) as compared to the counterpart. 24 The other study also found that moping posture also 2.81 more likely to develop MSDs and were strongly associated with MSDs (OR: 2.81, 1.43-5.50) as compared to the counterpart. 36 The location of work too was found to be a significant predictor of developing MSDs. Sanitary workers working in high slum concentration areas were 10.64 times more likely to get MSDs in the hips/thighs (OR: 10.64). 21 Health condition: Health condition of the workers also statistically significant for development of musculoskeletal impairments. For example, the analysis of the effect of mental health on MSDs revealed that workers with poor mental health status were significantly 3.26 times more likely to report MSDs (OR: 3.26) as compared to workers having good mental health status. 22 Moreover, the study found Thailand showed that history of injuries 4.37 more likely develop MSD (OR: 4.37, 1.27-15.11) as compared to with counterparts. 36 Type of job: The study indicate that job satisfaction and MSDs were also found to be significantly correlated as the sweepers who were not satisfied with their job were more likely to have suffered from the MSDs (OR: 11.43). 21
Limitations
Almost all of the included studies in this systematic review used a cross-sectional study design, which may result in selection bias and information bias at the sampling stage, and confounders may be one of the weak points of this design that leads to erroneous interpretation. It used a thorough search technique, however phrases used to describe sanitation employees may differ among geographical regions, countries, languages, and cultures, and some research may have gone unnoticed. Moreover, linguistic restrictions for included articles produced in English but expressly excluding papers written in non-English language that might be induced linguistic bias.
Conclusion
Despite the limitations, the consistency of the evidence suggests that whatever sanitation workers are working in different situation, they are facing with occupational related problems as the result of socio-demographic characteristics, occupational safety variables, and behavioral variables, work pattern. As a result, the findings suggested that these linked determinants of occupational health and safety outcomes necessitate governmental institutional guidelines, legislation, and other reduction efforts among sanitary personnel.
Footnotes
Acknowledgements
Our acknowledgment will be going our Host University. Next, we would like thank Water Aid jointly with WHO and ILO those are recommending Occupational health and safety and sanitary workers research as priority across the world. Moreover, we acknowledged all scholars and authors those their papers found on free open access data of engines.
Authors’ Contributions
ST* and GK developed systematic review extracted data from engines. WD and GD systematized data and assessed quality of the paper. ST* and GD compiled data and framed all components. All authors equally contributed for the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Not applicable
Consent for Publication
The current publication is not published yet.
Availability of Data and Materials
We consent the data deposit in a public repository that meets appropriate standards of archiving, citation, and supplement information files under alongside of our manuscript; we can provide an explanation and details of any restrictions on access if data are not freely available, and acceptable justifications for restricting access may include legal and ethical concerns.