
Abstract
Young women (18-45 years of age) with breast cancer often view the end of active treatment as a significant milestone. While completing treatment is largely celebrated, little is known about the immediate time after completing active treatment. The purpose of this qualitative, descriptive study was to explore the needs of young women survivors transitioning out of active breast cancer treatment and into survivorship. We used a qualitative design with convenience sampling of young women who completed active breast cancer treatment within the last 5 years to participate in semi-structured online focus groups from November 2020 to May 2021. Thematic analysis was used to reveal the needs as women transitioned out of active treatment and into survivorship. Thirty-three young women breast cancer survivors (75.8% White, 12.1% Black, 12.1% other) participated in 7 online focus groups each lasting approximately 90 min. Three dominant themes with accompanying subthemes emerged from the data: (1) “feeling like a different kind of woman” (physical [cognitive, weight, sexual] changes, emotional changes [defining normal, loss of purpose]); (2) lingering emotional trauma (active treatment, survivorship); and (3) recommendations (services needed, content needed). Participants in this study did not feel prepared for the physical and emotional changes associated with the transition from active treatment and into survivorship as identified in our 2 main themes of “feeling like a different kind of woman” and lingering emotional trauma. Participants recommended more thorough communication about expectations in survivorship focusing on physical aspects like cognitive, weight, and sexual changes as well emotional challenges like loss of identity in survivorship. More communication specific to young women could assist in the transition to survivorship.
We know that transition to survivorship is fraught with many challenges for women with breast cancer.
This research further describes young women’s unmet needs as they transition from active treatment and into immediate survivorship and offers recommendations for future patient education topics to assist with the transition.
Oncology team member communication with young women should focus on physical changes (cognitive, weight, sexual) and emotional changes into survivorship.
The median age of diagnosis of breast cancer in women is 62 years of age. Yet, for young women between the ages of 15 and 39, breast cancer is the most common cancer diagnosis 1 and these young women have profoundly different cancer experiences compared to their older counterparts. First, young women are more likely to have more aggressive subtypes, exhibit larger tumor sizes, and show higher incidence of node involvement. 2 This can result in more complex treatment regimens consisting of lengthy radiation treatments and variations of chemotherapy cycles. 3 Second, young women are often in the stage of life where they are embarking on new adventures such as starting or planning for families,4,5 developing careers, 6 and possibly coping with limited finances. 7 Thus, receiving a breast cancer diagnosis and entering into active treatment can be particularly burdensome and unsettling for young women.
Active treatment of chemotherapy and radiation can be particularly troublesome. Chemotherapy cycles of 2-to-3 week intervals lasting several months can be physically taxing and take young women away from their job- and family-related activities. Additionally, young women have to mitigate chemotherapy and radiation side effects of nausea and vomiting, mouth sores, skin changes, diarrhea, and bone pain while in active treatment.8-10 After several months of chemotherapy cycles and/or radiation regimens, many young women complete their active treatment marked by “ringing the bell” to symbolically enter into survivorship. While this ringing of the bell is largely celebrated marking the end of the cancer “journey,” the initial transition into survivorship can be incredibly anxiety-provoking and distressing.11,12
As young women transition into survivorship, they meet with oncologists and oncology team members with reduced frequency compared to active treatment appointments. 13 They may also sporadically attend support groups while in survivorship as compared with regular attendance while undergoing active treatment. Young women may have spontaneous medical questions arise and no longer have a standing appointment with their oncology team and thus are unsure of where to get their questions answered. As a result, young women may feel isolated, lonely, and overwhelmed.14,15 Additionally, they may be simultaneously trying to navigate routine medical follow-up care while transitioning their care back to their primary care providers. 16 These changes can result in an overwhelming array of unmet needs ranging from informational needs about hormonal therapies, psychosocial needs for cancer-specific social support, physical needs of stress management, and emotional needs to reduce fear of cancer recurrence.17-20 While some unmet needs can be resolved with additional resources and services (ie, providing access to support groups, educating about hormonal therapy side effects, supplying mental health services), young women may still face challenges in the transition into permanent survivorship approximately several years after completing active treatment.17,21
Much research has centered on improving psychosocial problems stemming from unmet needs and maintaining quality of life within the stage of permanent survivorship. 22 Evidence supports the effectiveness of educational interventions at improving knowledge and increasing symptom self-management for young breast cancer survivors.23,24 Additionally, structured cognitive and behavioral interventions are effective methods at reducing depression, anxiety, and improving quality of life for women in treatment and survivorship.25-27 However, little is known about the distinct time of transitioning out of active treatment particularly for young women who are experiencing life-changing events such as deciding on family planning and dealing with life-altering changes post cancer treatment. Thus, the purpose of this qualitative, descriptive study was to explore the needs of young women breast cancer survivors transitioning out of active treatment and into survivorship.
Methods
Study Approach and Design
The authors used a qualitative descriptive design to explore the needs of young women transitioning out of active breast cancer treatment into survivorship. This study was approved by the University of Arkansas for Medical Sciences Institutional Review Board (Protocol #239621). All participants provided informed consent prior to participating in the study through an online portal.
Participant Recruitment
Study team members used 4 main strategies to recruit potential participants which occurred during the onset of the COVID-19 pandemic. First, direct e-mails detailing the study were sent to participants currently enrolled in a statewide research registry (AR Research) who indicated an interest in women’s health and cancer.28,29 Second, printed fliers were displayed in waiting rooms and elevators of various oncology clinics at a major academic medical center with a QR code linking to the study’s consent and demographic questionnaire. Third, a digital flier with a link to the study’s website detailing time commitment and incentives was distributed through boosted posts on Facebook and through listservs for specific adolescent and young adult populations such as the Young Survival Coalition, Moffitt Cancer Center’s Adolescent and Young Adult (AYA) program, and the Tampa Bay Community Cancer Network (TBCCN). Fourth, providers endorsed the study and referenced the flier during in-person visits at the survivorship clinic. All of our strategies allowed women to self-enroll in our study. Potential participants were not identified prior to our distribution of recruitment materials. We also encouraged potential participants and community members (ie, local cancer organizations) to informally share of our study information. Further details of these recruitment strategies are described elsewhere. 30
Data Collection
Potential participants completed the consent and demographic questionnaire through a REDCap portal. 31 The investigator-developed questionnaire included 23 questions covering topics from demographics (race, marital status, employment, income) and cancer characteristics (type, stage, treatment). Answer choices ranged from multiple choice to select all that apply. Once the questionnaire was complete, a research assistant scheduled a password-protected online focus group hosted on the Zoom video platform. 32 An experienced qualitative nurse researcher conducted the focus groups using a semi-structured interview guide. Questions were open-ended and designed to encourage discussion. A sample question was, “Can you give me a brief overview of your treatment and where you are today?” The nurse researcher focused on maintaining a safe, therapeutic environment by using patient-centered interviewing skills 33 and checked for understanding by reflecting to the participants what she interpreted. 34
Each focus group was held with a welcome from the study team (nurse researcher and/or research assistant) and introduction from the participants. The focus group began with a general opening question about the women’s experiences with their breast cancer diagnoses and life thereafter. Probing questions were used to expand and clarify discussion. Data for this analysis were restricted to women’s experiences transitioning from active treatment to survivorship. Although the focus groups were hosted on the Zoom video platform, only the audio was recorded for transcription. Most of the groups lasted approximately 90 min. After the conclusion of the focus group, participants were mailed a $50 Wal-mart gift card as a thank you for their time.
Trustworthiness
Lincoln and Guba described trustworthiness as a measure of reliability and validity for qualitative studies. We ensured trustworthiness of our findings by: (1) having one qualitative researcher (and principal investigator) lead all of the focus groups; (2) verifying all transcripts for accuracy against the audio recordings for every 10 pages; (3) soliciting feedback, and making changes if necessary, from multiple investigators from different disciplines (nursing, medicine, epidemiology) in designing the research plan; (4) engaging a seasoned qualitative expert on the study team to read transcripts and confirm findings; and (5) maintaining an audit trail of definitions of codes (available by request) in a codebook. All of these steps helped establish credibility, transferability, dependability, and conformability. 35
Data Analysis
Audio recordings were transcribed verbatim and were cross-checked for accuracy. The transcripts and audio were compared for accuracy every 10 pages. The verified transcripts were redacted and loaded into the qualitative analysis software, MAXQDA. 36 Data were managed, grouped, linked, and annotated using this software.
Data were analyzed using Braun and Clarke’s 6 step framework of thematic analysis to identify and organize patterns of meanings, or themes, across data to understand collective experiences. 37 The 6 steps were: (1) become acquainted with the data; (2) generate initial codes (small chunks of meanings); (3) search for themes (significant patterns of meanings); (4) review potential themes; (5) define and name themes; and (6) produce the report.
After the study team members became acquainted with the data (Step 1), small segments of text were labeled with potential meanings, or codes (Step 2). The study team members met and agreed upon codes after the initial 2 steps. The codes from the first 2 focus groups were organized into a code book which contained exact definitions to guide subsequent coding. Study team members then searched the text for any significant patterns of meaning, or themes (Step 3). The principal investigator then used constant comparison to compare data across focus groups for similarities and differences in order to develop potential themes 38 (Step 4). Data were then aggregated and clustered into increasingly abstract interrelated units of meaning in which the final themes were named (Step 5). The principal investigator met with study team members throughout all steps of the data analysis to ensure validity of the results. Any discrepancies between the study team members were resolved by a seasoned nurse researcher with expertise in qualitative methodology.
We conducted descriptive statistics for demographic characteristics, breast cancer stages, and types of treatment using SAS version 9.4.
Results
Sample
Thirty-three women comprised the convenience sample for this descriptive study. Seven focus groups were conducted and approximately 5 women participated in each group. Women were English-speaking and were at most the age of 45. Most of the women were White (n = 25, 75.8%), and the sample included women of various backgrounds (Black/African American (n = 4, 12.1%) and other (n = 4, 12.1%). The data did not reflect any discrepancies among demographics between focus group participants. See Table 1 for additional characteristics.
Demographic Characteristics of Focus Group Participants.

About half of the participants were diagnosed with Stage 2 (n = 17, 51.5%) breast cancer and most women completed chemotherapy (n = 31, 93.9%), radiation (n = 23, 69.7%), and targeted and immune therapies (n = 15, 45.5%). See Table 2 for additional clinical characteristics.
Summary of Cancer and Type of Treatments.
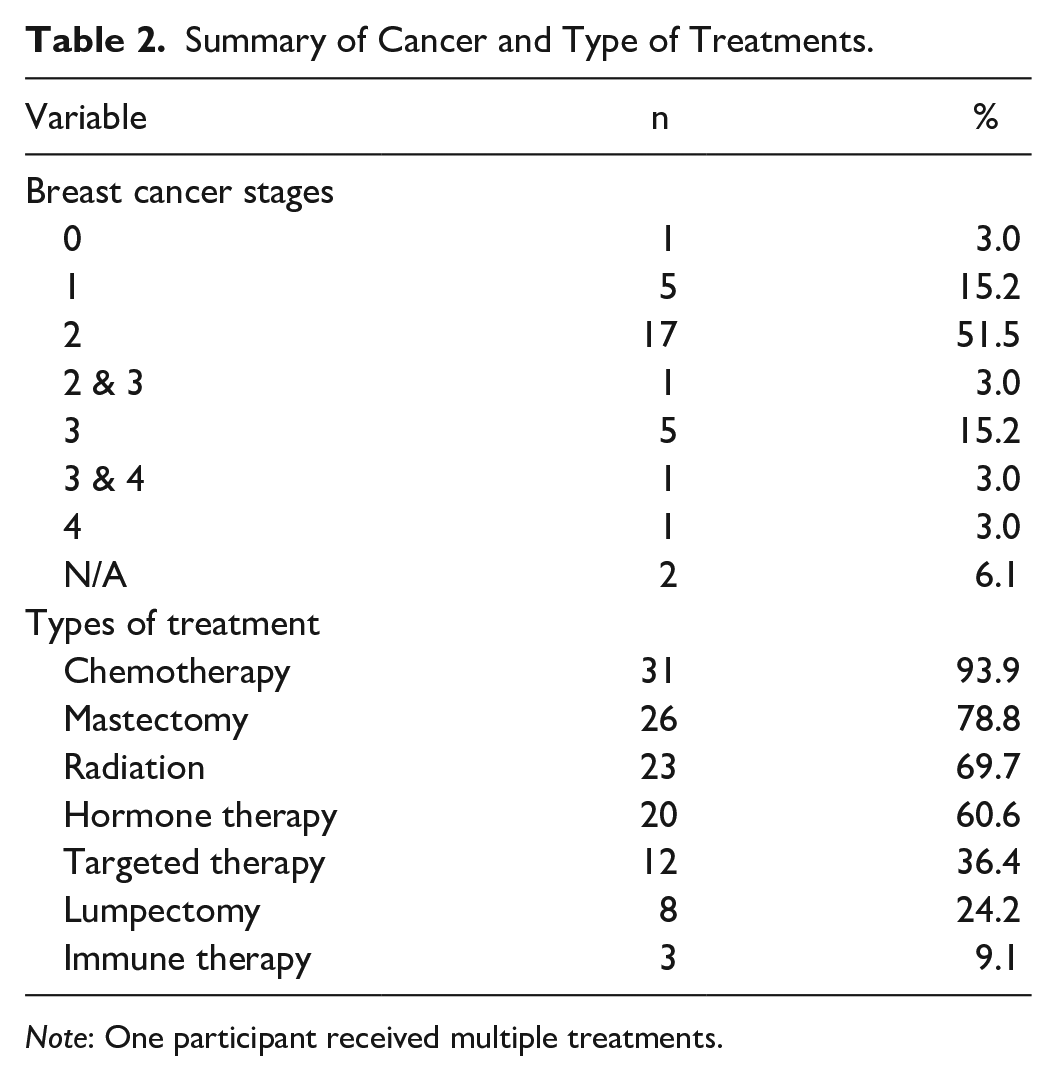
Note: One participant received multiple treatments.
Focus Group Themes
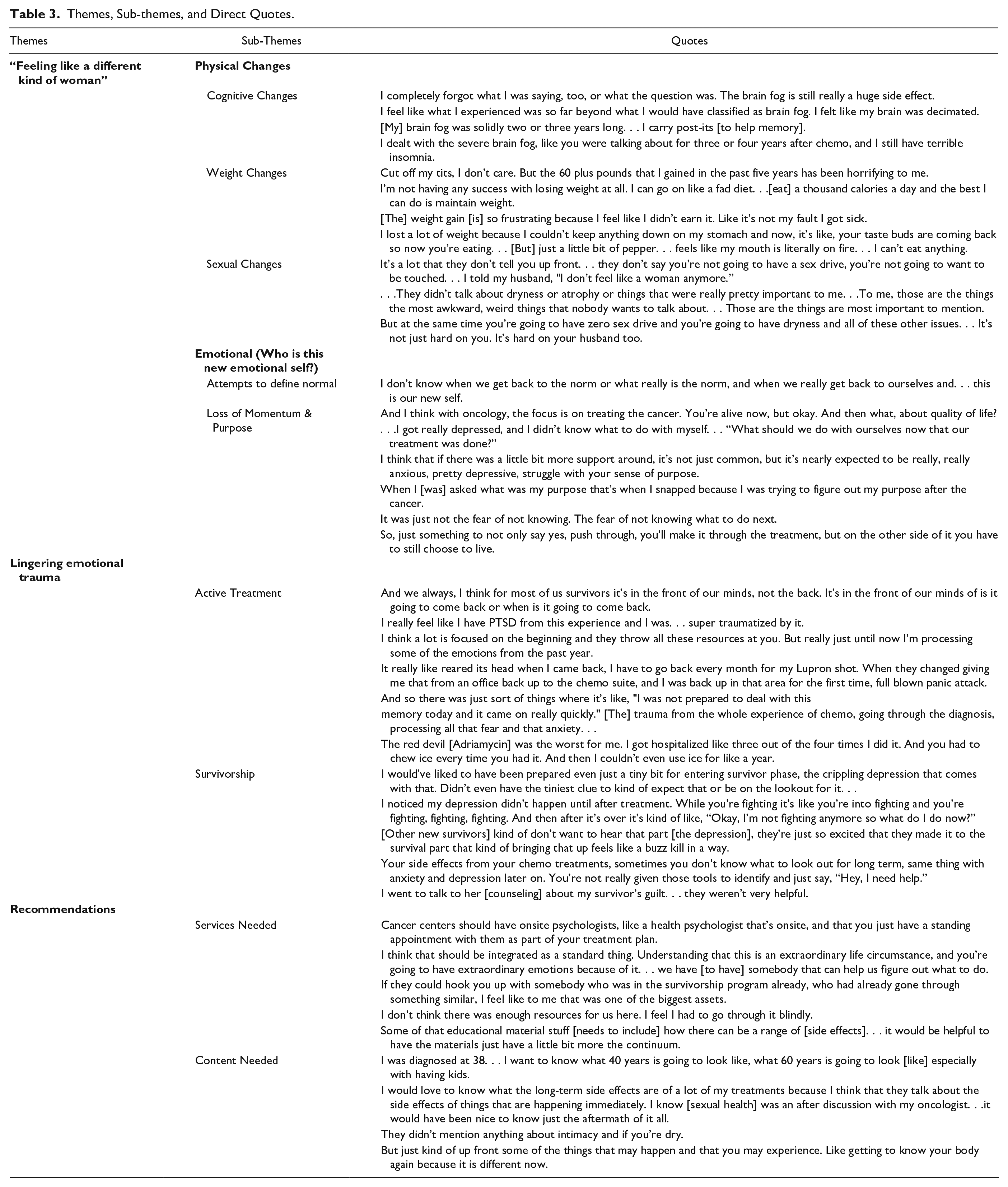
Three major themes emerged from this descriptive data with accompanying subthemes under each category. The first theme to emerge from the data was “feeling like a different kind of woman” a direct quote which best captured the subthemes of physical and emotional changes in their new selves. The second theme was named lingering emotional trauma which was related to 2 distinct time points of subthemes of active treatment and survivorship entry. The final and third theme was labeled recommendations which were centered around the subthemes of services and communication content needed for women transitioning into survivorship. See Table 3 for an overview of the themes, sub-themes, and direct quotes from participants.
Themes, Sub-themes, and Direct Quotes.
Feeling like a different kind of woman
Cognitive changes
Insomnia and brain fog were frequent topics as women described their major changes after completing active treatment. One woman said, “Insomnia is still a really big problem for me and forgetting what I’m talking about in the middle of sentences. . . forgetting words is a problem.” Another woman described the continuous effects of treatment and said, “It [severe brain fog, insomnia, joint pain] goes and it goes, and it’s never really over.” A few women talked about their strategies to cope with brain fog and one particularly mentioned using notes as reminders saying, “Now I use my post-its. . . I’m like, okay, I got to write this all down.” However, another woman remarked that she still underestimates her ability to recall information. She said, “. . . my husband will say, ‘I told you that.’ And then I’ll be like. . . ‘did I just tone you out, or did I really just not remember?’”
Weight changes
Apart from the cognitive changes related to treatment effects, weight was frequently mentioned among women across the focus groups. One woman talked about how her body slowly went back to normal after treatment, but weight was still a concern. She said, “After treatment, my period came back and everything like that, but the weight gain after chemo. . . I’m having a really hard time getting it off.” Another woman tearfully spoke about her struggles with weight gain and said, “But, it’s not like I got like happy fat in a great relationship. . . it’s not like a relationship weight or that I’m just getting older. . . [it’s] not normal for a 20-year-old to gain that much weight.” Most of the women remarked how they did not anticipate the weight gain and were not adequately informed of the potential side effect. “[The weight gain was] not something that I was prepared for and. . . it never even got touched on,” one woman commented.
Sexual health changes
Another area that women felt ill-prepared for was the sexual health changes resulting from treatment. The hormonal changes from treatment were incredibly distressing for most of the women, and one woman commented about the lack of communication regarding her menstrual period. She said, “They didn’t tell me that it was going to start menopause. My period stopped. They didn’t tell me to expect that.” She later said, “That seems like something that you would want to communicate to a patient.” Another woman described a similar lack of preparation, but then commented on her follow up communication with her providers. She said, “. . . one thing I wasn’t prepared for was hot flashes. I did mention it to my oncologist a couple times and she suggested [medications]. . .[But] I just dealt with it.” Another woman talked about her frustration from the treatment side effects and the consequences on her body image and sexuality. She said, “Well, and if you’re already going through all of these things that make you feel like a different kind of woman, or like not as much of a woman. . . and then you can’t even have sex comfortably.”
Attempting to define
Women transitioning from active treatment and into survivorship recalled their attempts to define their new emotional self in relation to their past versions before breast cancer treatment. One woman discussed the process in which she questioned her new self by saying, “My thought is, what really is the new self? I mean, what is your new self? Is it. . . the gaining of weight? Is it the chemo brain?” Another woman talked about comparing her new self to other women her same age without the experience of breast cancer. She said, “This is like our generativity time, where we’re supposed to be really active in our careers, or really active as parents or with our churches or our volunteer work or whatever it is that we’re doing.” She later explained how she regretted the limitations of her new self and said, “This is the time in our life where we’re intensely doing those things. I remember tearfully saying, ‘I just feel like an old woman.’”
Loss of momentum & purpose
One of the most common topics across the focus groups was the loss of momentum and purpose as women transitioned out of active treatment and into survivorship. This specific time was abruptly marked by the discontinuation of treatment and was met with mixed emotions. One woman recalled, “Before treatment I felt like I had a plan, so there’s always progress. I had something active that I was doing to put the cancer in remission.” She then described the devastating consequences after treatment ended. She said, “And then when I was done with my treatment it was like this big letdown.” Another woman echoed these sentiments and said how her diagnosis of triple negative breast cancer made her experience different. She said, “. . . There’s nothing left once we’re done with radiation. You don’t get a pill. You get sent home, and that’s it. And I actually got really depressed when I was finished with my treatment.” Another woman talked about her efforts to understand her purpose after completing treatment. “I still [have survivor’s remorse]. When I look at my auntie’s pictures. . . why did they leave and I’m still here?” She continued to express her reasoning in an attempt to make peace with her survival by saying, “. . . just knowing that you’re still here for a purpose. And that apparently your purpose hasn’t been fulfilled yet because you’re still here.”
Lingering (unresolved) emotional trauma
Women consistently talked about the lingering, unresolved emotional trauma they experienced within 2 distinct time periods: active treatment and into survivorship. Many of the women reflected on triggers which marked their unresolved emotions toward particular events or settings. None of the women, even those furthest from active treatment, discussed the resolution of the traumatic experiences.
Active treatment
The period of active treatment appeared to have the most triggering memories for the women across all the focus groups. One woman was surprised about her own reactions and said, “No matter how strong you were before cancer in your mental health, now you just have different things that are going to cause triggers for you and things that you don’t really realize they will.” Small events such as a smell was upsetting for some women and reminded them of treatment. One woman said, “I was at a grocery store and I smelled. . . the same cleaner that they used in the oncologist office and that triggered a panic attack.” Many of the triggering events were unanticipated and the women said they had no way to prepare for their emotional reactions. Another woman talked about how small ice cubes reminded her of sitting in the chairs undergoing chemotherapy. “I can only have real big ice cubes now. I mean, it’s a little bit better, but I can’t do Sonic [ice]. If I can see them, all bets are off but if there’s a lid on it, I’m fine.” None of the women talked about a complete dissolution of triggers but instead mentioned how they still expected to have some emotional responses to unexpected sights, smells, or environments.
Survivorship entry
Women talked about their feelings toward entering survivorship, and most of the women said they felt unprepared for the emotional toll of the transition. One woman was aware of the emotional challenges but still was not prepared for the depth of the feelings. She said, “There’s going to be emotional trauma, and I was dealing with those little bits of it as I went along, but the depression part of it blindsided me completely.” She later reflected that her oncology team did not prepare her for the depression entering survivorship. “And, I don’t think there was anything mentioned by anybody.” Another woman knew about the upcoming emotional changes and said she was waiting to talk to her oncology team once treatment ended. She said, “[A doctor] told me the 3 goals were to treat the cancer, treat the cancer, treat the cancer, and then they’ll deal with other stuff later. But, later was never addressed.” After treatment concluded she expected to touch on her other challenges (such as depression and anxiety) with her providers, but she said she was disappointed when her symptoms were not discussed. “It was just like, okay, we’re going to treat the cancer and then, okay, goodbye.” Other women talked about their overall transition into survivorship and did not focus on specific aspects such as depression and anxiety. One woman described how she knew she could not fully prepare for the transition into survivorship and said, “no one [clinical] at least set up the stage that would be part of the journey, and learning how to be a survivor and learning how to handle those bumpy parts of the road.” She later said how she could have benefited from more clinical guidance.
Recommendations
Throughout the focus groups women consistently gave suggestions to improve the transition from active treatment into survivorship. Two main subthemes of services and content emerged as distinct categories of recommendations. Most of the women talked about services they needed but were unavailable, and only a few women talked about services that were helpful to their own experiences.
Services needed
The women in the focus groups commented on their need for additional mental health services throughout active treatment and into survivorship. One woman wanted specific counseling for patients with cancer and said, “There is a certain amount of education [needed for counseling someone] that is going through cancer treatment, or that is going through that survive. . .a special kind of treatment is needed.” She later commented that traditional mental health services were not specific enough for her needs. One woman echoed this same frustration with regards to mental health providers and said, “I did have a therapist that I went to for a while, and then we switched to a different therapist and this young lady was like, ‘Oh, you’re so inspirational.’ No, I don’t need that right now. Not from a therapist.”
Another woman wanted more assessments from clinical staff after completing active treatment. She said, “[We need to] have more check-ins after active treatment because I do feel like it’s kind of like you’re just kind of left to fend for yourself at some point, and that’s scary.” During one particular focus group a woman described her involvement with a peer survivors group which was incredibly beneficial for her mental health. One woman adopted that concept and proposed a program directed by a nurse navigator. She said, “I think that that would have been a huge thing. . . if the nurse navigator said, ‘Hey, I’m going to hook you up with, if it’s okay with you, of course, there’s somebody who would love to talk to you. She’s a year ahead of you and answers some real-life questions for you.’”
Content needed
Sexual health communication from providers relating to body image, vaginal dryness, and sex drive was the most recommended areas of needed content. One woman talked specifically about vaginal dryness being an issue and the resulting impact on a relationship. She stated, “I think [vaginal dryness] is a real concern for women. . . [it’s] a big piece of the puzzle that, I don’t even know if my husband really knows much of that I’m going to be on menopause and that life could be different.” She realized the potential impact of this and stated, “It really could wreak havoc on a relationship.” Another woman explicitly said how she wanted more sexual health communication. “I feel like that’s something that I wish there was more of. I just feel like it’s not talked about really that much.” She later laughed and said with some frustration, “I mean who really wants to say, “Hey, whenever you have breast cancer you’re not going to have a sex drive and your vagina’s going to be dry.”
Discussion
This study explored the needs of young women breast cancer survivors transitioning from active treatment and into survivorship. Our findings highlighted areas where women in this study felt particularly underprepared navigating the physical effects of brain fog, weight gain, and sexual changes. These concerns are consistent with the literature,39-42 and multiple efforts have been made to improve not only the communication about the areas but also to mitigate the effects of these changes. The participants in our study explicitly described brain fog (ie, chemo brain or cognitive impairment) as one of the most challenging physical changes following active treatment. Much of the literature included descriptive studies where breast cancer survivors described both the emotional toll of cognitive impairment and the accompanying strategies (eg, using daily calendars, making prompts) used to overcome the effects.43,44 Mindfulness-based interventions have demonstrated some significant results in reducing cognitive impairment overall for breast cancer survivors,45,46 but some of the outcomes did not distinguish between different components of cognitive function. 47
Our participants described their frustrations with weight gain, which was, and continues to be, a heavily researched area. The most effective physical activity interventions to combat weight gain in breast cancer survivors included a combination of physical activity, diet, and cognitive behavioral therapy.48,49 While these interventions demonstrated significant success for breast cancer survivors,50,51 not all women had access to such interventions and may have felt isolated in their attempts to manage their weight. Furthermore, communication and prioritization about the anticipated changes in weight was subject to the discretion of the oncology team and subject to each woman’s individual treatment plan. Thus, reducing weight or managing weight gain may not have been a priority of care over improving overall health outcomes.
Another area in which our participants described feeling ill-prepared for was sexual health. We define sexual health broadly as related to sexual satisfaction, vaginal dryness, and body image. Sexual health remains one of the most frequent unmet needs for young breast cancer survivors.39-41 The physical changes (eg, vaginal dryness, dyspareunia) coupled with the psychosocial effects of decreased libido and changes in body image can have devastating effects on a woman’s satisfaction. 48 Further, endocrine therapy commonly prescribed in survivorship can sustain these effects hindering a woman’s quality of life and sexual satisfaction. Unfortunately, many women and oncology care team members do not initiate conversation surrounding sexual health despite women’s desires to communicate about this topic.52,53 Our results reflect this lack of communication.
Some interventions are designed to improve the communication process between patients and oncology team members, whereas others directly target women’s sexual health in survivorship. Reese et al and colleagues created an intervention targeting oncologists and advanced practice providers’ communication skills with breast cancer survivors surrounding sexual health concerns. Results indicated that providers’ understanding of their patients’ sexual health needs improved as well as providers’ comfort in communicating about sensitive topics. 54 Sella et al and colleagues took a different approach by targeting their web-based intervention specifically to young breast cancer survivors. The intervention was designed to improve self-management of symptoms among breast cancer survivors and covered topics from stress and mindfulness to weight management. More than 90% of participants sought information about sexual health, and one-third of the participants reported that the intervention improved their communication with providers although the content area of communication was not disclosed. 24 Regardless of the approach used to improve sexual health among breast cancer survivors, communication between young women and oncology team members is critical.
Aside from the physical changes described by the young breast cancer survivors, reducing the emotional toll from experiences in active treatment and into survivorship remains a critical area of need. Our participants reflected on the continued grief tied to losing their identities (ie, concepts of self before cancer) and often had difficulty defining their “new selves” (ie, a young woman who experienced cancer). The loss of purpose associated with ending cancer treatment is frequently seen for patients with other cancers.55,56 As such, peer support groups are effective methods to assist breast cancer survivors with these internal challenges, 57 but young women may have difficult accessing these resources while juggling family and careers. Oncology care team members will need to recommend support groups with virtual options to attend.
Lastly, our participants described the onset of depression and anxiety when they transitioned into survivorship. The shock and onset of depression and anxiety at the conclusion of treatment commonly described in the literature,58,59 and evidence shows significant association between younger women and depression and anxiety.60,61 Interventions ranging from a range of mindfulness meditation and survivorship education to cognitive behavioral therapy have demonstrated effectiveness at reducing symptoms of depression and anxiety for young breast cancer survivors.56,62,63 However, some studies excluded women who were already practicing mindfulness. 62 Given the increase in mindfulness among young women, further research may need to include women who already have a standard practice of mindfulness and other self-care practices (meditation, yoga, breath work).
Clinical Implications
The transition from active treatment and into survivorship is marked by a period of uncertainty. The external (physical) and internal (emotional) changes noted in the transition are burdensome for young breast cancer survivors. The oncology team with whom the survivors have an established relationship is crucial in facilitating this transition for young women; however, the communication process can sometimes fall short. Oncology team members may need to teach more about what to expect in survivorship and provide numerous written and digital resources for patients before concluding active treatment. Despite the efforts of the oncology team, young survivors’ ability to learn and prepare for the next phase in the cancer care continuum can be hindered. As in the cancer journey metaphor, 64 young women may be too focused on reaching the end goal of “ringing the bell” of active treatment and are not mentally and emotionally prepared to learn about the upcoming stages. As a result, communication about the upcoming changes need to be threaded throughout from active treatment into survivorship visits and well into the longer permanent survivorship stage (more than 5 years post treatment).
Limitations
Several limitations within this study should be noted. First, our sample includes mostly White women who were married, highly educated, and comfortable using technology. Our findings may not be reflective of other women’s experiences particularly those of different racial, social, and educational backgrounds. Second, our sample includes 33 young women breast cancer survivors and due to the nature of a qualitative descriptive study, our findings are not generalizable to the larger population. However, we reached data saturation, and our conclusions are supported in the literature. Third, we did not collect specific ages of our participants. Instead, we relied on the inclusion criteria of the age range of 18 to 45 for women to self-select to participate in the study. Fourth, the young women in our study reflected on their experiences within the last 5 years. They may not have fully processed the trauma of their cancer experience, and their feedback may be biased as a result. Fifth, the focus groups were conducted within the first year of the COVID-19 pandemic. The timing of the data collection and pandemic may have affected women’s abilities to access resources like in-person support groups or peer-led physical activity sessions. The drastic change in accessibility to services may have negatively impacted their experiences in the transition into survivorship.
Future research should be centered on asking young women to reflect on topics which they have downplayed to providers initially in the early survivorship phase. Additional perspective of time may provide valuable insight to the needs of young women transitioning from active treatment and into survivorship.
Footnotes
Acknowledgements
Dr. Parker would also like to acknowledge the guidance provided during preparation of this manuscript made possible by the Center for Childhood Obesity Prevention funded by the National Institute of General Medical Sciences of the National Institutes of Health under Award Number P20GM109096 (Arkansas Children’s Research Institute, PI: Weber). She would also like to thank Heidi Charton, BA for her assistance with this project, Dr. James V. Parker, Jr, EdD, JD, for his editing assistance, and most of all, the participants in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Parker is currently supported by the University of Arkansas for Medical Sciences Translational Research Institute (TRI) grants KL2TR003108 and UL1TR003107 through the National Center for Advancing Translational Sciences of the National Institutes of Health (NIH) and Arkansas Breast Cancer Research Program.