
Abstract
To better prepare for a potential future pandemic, it is important to investigate factors that influenced responses to the recent COVID-19 pandemic. The aim of the present study was to investigate factors that influenced the decision to get the COVID-19 vaccine. The COVID-19 pandemic has affected almost everyone throughout the world. Vaccines are a significant factor in managing a pandemic. As vaccines are developed, governments develop vaccine roll-out plans. Unfortunately, vaccine hesitancies can slow the implementation of any vaccine program. A question arises as to the factors that are associated with the decision to get vaccinated. The present study explored associations between vaccine hesitancy, and the Health Belief Model (HBM) in student samples from the Czech Republic, Israel, and the United States. From August, 2021 through December, 2021, an online survey was distributed in Czech, Hebrew, and English. A total of 447 participants completed the survey. A binomial logistic regression was conducted to ascertain the influence of perceived susceptibility, severity, benefits, and barriers on the likelihood that participants are vaccinated. Results revealed that the factors of perceived severity and perceived benefits explained 52.6% (Nagelkerke R2) of the variance in vaccination. An analysis of Variance (ANOVA) found significant differences between countries for the 4 HBM factors. Based on these findings, it is recommended that policymakers put forth added emphasis on the severity of a virus and the benefits associated with the vaccine. Further, since there appears to be variability between countries in perceptions of the virus, and associated vaccine, governments should consider factors within their own environment when developing a strategy to combat a pandemic. More specifically, government could explore their own strengths, weaknesses, opportunities, and threats as they develop a pandemic strategy. Additional practical and theoretical implications are discussed.
The COVID-19 pandemic has affected almost everyone throughout the world. Vaccine hesitancy has been a challenge for healthcare systems and policymakers who work to mitigate the challenges of a pandemic. The global aspect of the COVID-19 pandemic has provided an environment to better understand the factors that influence the decision to get vaccinated.
The aim of the present study was to investigate factors that influenced the decision to get the COVID-19 vaccine. An analysis of a sample of college students from the Czech Republic, Israel, and the United States revealed similarities in perceptions of the severity of the virus, as well as the perceived benefits in relation to the decision to get vaccinated. In addition, results provide evidence as to the differences in the levels of perceptions relative to getting vaccinated.
Dealing with the COVID-19 pandemic has been a significant global challenge. The present study provides evidence that policy makers should further promote the benefits of a vaccine and emphasize potential severity of the virus. In addition to highlighting the death rate of a virus, it may be prudent to highlight the severe and potentially long-term symptoms of a virus. Finally, the present study provides evidence of country-specific varying perceptions of susceptibly, severity, benefits, and barriers associated with a virus and vaccine. Rather than a global model for dealing with a virus, governments should consider their own strengths, weaknesses, opportunities, and threats in creating an effective model to mitigate the virus.
Introduction
Coronavirus disease (COVID-19) is an infectious disease caused by the SARS-CoV-2 virus. 1 The disease can cause mild to severe respiratory symptoms which can lead to death. In December, 2019, the first cases of patients with shortness of breath and fever of unknown origin were reported in Wuhan, Hubei Providence, China. Reporting of the first cases led to the identification of the novel coronavirus on January 5, 2020. 2 As of December 2022, there have been 650 879 143 confirmed cases, 6 651 415 confirmed deaths, and 13 008 560 983 vaccine doses administered. 3 The aim of the present study was to investigate factors that influenced the decision to get the COVID-19 vaccine.
Early in the pandemic, global lockdowns were instituted. The lockdowns ranged from highly restricted immediate lockdowns, to graduated phased lockdowns. 4 There is debate about the value of these lockdowns. For example, in a study of COVID-19 containment policies in 31 countries, it was found that high levels of strictness in public policy did not significantly reduce confirmed cases and fatality rates when compared to low levels of strictness in public policy. 5 Another study found similar levels of confirmed cases, hospitalizations, and admission to Intensive Care Units (ICUs) during the pandemic period (2020) and after the vaccine became available (2021). 6
In addition to lockdowns, the World Health Organization (WHO) recommended several prevention practices including staying 6 feet apart from others, wearing a mask if unable to maintain physical distance or in poorly ventilated settings, washing hands regularly, and staying home if unwell. 7 As a result of these implemented measures, almost everyone’s life was impacted. Geng et al 8 found that the pandemic adversely affected the income of more than two-thirds (67%) of households. As a result, households altered food consumption, and energy usage to safeguard income. Sadly, the impact on household incomes has been particularly difficult for lower-income segments of society. 9
Consumers also resorted to more online purchasing of necessities,10,11 as well as increased social media access. 12 Social media has played a significant role in dealing with challenges of the COVID-19 pandemic. 13 While easily accessible social media content provides useful information pertaining to the pandemic, researchers also find it can cause a strain on mental health.12,14,15 Although, in a survey of 348 individuals, researchers found a positive link between COVID-19 knowledge and attitudes toward social media usage. 16 Evidence suggests that the perceived value of social media content, and its impact on an individual’s wellbeing, varies based on social media platform (eg, YouTube, Twitter, Instagram, etc.) and the associated amplification of either questionable or reliable information. 17
Educational institutions globally also had to quickly shift to online learning and services. Access to class materials and library content needed to be robust enough to handle the increased student needs for electronic (eg, e-library) access. One study found that due to the education shift to online learning, Internet usage increased by 35%. 9 Beyond the need to ensure readiness of physical infrastructures such as the e-library, researchers have found evidence as to the importance of understanding the students’ attitudes and beliefs regarding the intention to use such (eg, e-library). 18 Unfortunately, researchers also find that underdeveloped countries cannot produce the desired educational results since many students have limited access to the internet. 19
The abrupt shift to online learning also had an impact on student wellbeing. In a study of 500 students from different universities in Pakistan, researchers found severe levels of anxiety in 22.7% of the sample and severe levels of depression in 15.9% of the sample. 20 Significant increases in depression levels were also found in a sample of 7228 college students in Poland. 21
On December 31, 2020, the WHO issued its first emergency use validation for a COVID-19 vaccine. 22 Governments and policymakers had to quickly implement vaccination campaigns. As part of a vaccination campaign, policymakers must better understand contributing factors to an effective campaign. For example, there is evidence as to the importance of quality governing, and intensive vaccination campaigns early in the pandemic as important aspects of an effective vaccination campaign.23,24 In addition, Coccia 25 posited that 70% of a population being vaccinated can be achieved without coercion. While a vaccination campaign is a necessary part of mitigating the COVID-19 crisis, Coccia 26 posits that is not in and of itself a sufficient public policy. Among various factors, the act of being vaccinated may result in an increase of risky behavior.
In addition to factors associated with an effective vaccination campaign, policymakers must understand factors associated with vaccine hesitancy. While the phenomena of vaccine hesitancy is not new, 27 it has been brought to the forefront due to the COVID-19 pandemic. 28 According to the World Health Organization (WHO), vaccine hesitancy is in the top 10 of global health threats. 29 The factors contributing to vaccine hesitancy may vary from interpersonal, social, to psychological influences. 30 Specific factors related to vaccine hesitancy include fear of unknown side effects (due to the rapid development of the vaccine), peer adherence/acceptance, beliefs in conspiracy theories, and lack of trust in the government. 31 In a recent qualitative study using focus groups and interviews, researchers identified mistrust, fear, and lack of information as the most significant in driving COVID-19 vaccine hesitancy. 32
Public surveys regarding COVID-19 vaccine acceptance have been conducted worldwide resulting in evidence that the policy adopted by the government regarding vaccine rollout, influences COVID-19 vaccine acceptance and public perception of the vaccine. 33 Research also suggests higher willingness to get the COVID-19 vaccine among low- and middle-income countries (eg, countries in Africa and South America) when compared to upper- middle-income countries such as the United States and Russia. 34 In a study of 31 peer-reviewed articles, high acceptance rates were found in countries such as Ecuador (97.0%), Malaysia (94.3%), Indonesia (93.3%), and China (91.3%). Low acceptance rates were found in countries such as Kuwait (23.6%), Jordan (28.4%), Italy (53.7%), Russia (%4.9%), Poland (56.3%), the United States (56.9%), and France (58.9%). 35 Machingaidze and Wiysonge 33 posit that low-income countries are more accepting of vaccines due to lived experiences of witnessing thousands of deaths annually due to vaccine-preventable infectious diseases. High income countries have effectively eliminated these diseases and therefore have not experienced the devastating effects, resulting in a complacency relative to vaccinations. These differences in acceptance rates may be due in-part to country-specific response patterns to the governments’ COVID-19 vaccine distribution policy. 36 For example, cross-national comparisons revealed that in Belgium, Italy, and Ireland, pharmacists are authorized to administer the vaccine, while in countries such as Croatia and the Czech Republic they are not. 37
In another study, males with a history of flu vaccinations, perceiving higher risk and severity of COVID-19 infections, were more likely to get vaccinated. 38 A survey of 1942 working-age adults in France was conducted to explore COVID-19 vaccine hesitancy. 39 Among the findings was vaccine refusal being associated with lower perceived severity. Viswanath et al 40 explored the individual and social determinants of COVID-19 vaccine uptake. In the sample of 1012 individuals, 68.3% agreed to get the vaccine for themselves. Personal susceptibility to the threat and perceptions of severity of the threat were associated with likelihood of vaccinating self.
During the months of September through November, 2019, a qualitative study was conducted on 19 point-of-care vaccinators the Cape Metropolitan District of South Africa. 41 From the interviews, 4 themes were identified as major drivers of vaccine hesitancy. Firstly, religion was the most common reason for vaccine hesitancy. Internet content was also expressed as a driver of vaccine hesitancy, specifically, the negative information about vaccines. The concern of the pain associated with getting vaccinated was also an issue. Finally, the idea that children should develop their own natural immunity was also a driver of vaccine hesitancy.
In a recent study of university students pursuing higher education in non-medical/health related fields, COVID-19 vaccination refusal rates were explored. A total of 27 studies were included in this global review with an overall rate of COVID-19 vaccination refusal of 22%. 42 They also found that students pursuing non-health/ medical related college academic studies are more likely to refuse COVID-19 vaccines compared to college students in health and medical fields (22% vs 18.9%). A study of 237 college students found a willingness to get vaccinated against COVID-19, provided the vaccines are proven safe and efficacious. 43
A systematic review with meta-analysis was conducted to explore vaccine hesitancy rate among healthcare students. 44 From the 31 articles included in the analysis, results revealed a prevalence of vaccine acceptance of 68.8%, and a vaccine hesitancy rate of 25.8%. A suggested reason for the hesitancy rate was that the healthcare students may be exposed to large amounts of healthcare information which could make them aware of the vaccines potential serious side effects thus influencing their decision to get vaccinated.
There is a need to understand the predictors of vaccine hesitancy. One such avenue would be through the use of the Health Belief Model (HBM), which is used by researchers to better understand motivations to health-related behavior.45-48 While the constructs of the HBM range from 4 to 6 which include, perceived susceptibility, perceived severity, perceived benefits, perceived barriers, motivation and external cues to action, 49 the first 4 constructs are most often found in research. Perceived susceptibility addresses perceptions of the risk of acquiring a disease. Perceived severity addresses beliefs regarding the seriousness of contracting the disease. Perceived barriers refer to perceptions regarding the difficulty of performing a recommended action in preventing a disease. 50 The health belief model has been used as a foundation for experimental research, as well as uncovering associations with various factors. For example, in an experimental study, researchers have provided evidence that an educational program based on the health belief model, promoted hypertension prevention behavior in a sample of medical staff members. 51
Researchers have also used the HBM to explore associations with vaccine hesitancy. Cheney and John 52 found that vaccine-reluctant individuals significantly differed in their health beliefs compared with vaccine-accepting individuals. Relative to the COVID-19 vaccine, Al-Metwali et al 53 found perceived susceptibility and severity of COVID-19 to be significantly higher in a sample of health care workers, than the general population. The researchers also found perceived benefit and barriers predicted willingness to receive the COVID-19 vaccine.
A survey was conducted on 504 people prior to the vaccine operation in Israel. Using the Health Belief Model, it was found that barriers and benefits were associated with vaccine acceptance. More specifically, there was a positive association between perceived benefits and vaccine acceptance, and a negative association between perceived barriers and vaccine acceptance. 54
Vaccine hesitancy has been well documented in the literature leading to research that examined ways to overcome the hesitancy. Shmueli 55 explored the influence of various incentives on intention to get vaccinated. In a sample of 461 Israeli adults, results revealed that perceived susceptibility, perceived benefits, and cues to action were linked to intention to receive the vaccination. Further, perceived severity and perceived barriers were not associated with the intention to get vaccinated.
Experiences and outcomes from the COVID-19 pandemic are of significant value as society moves beyond the COVID-19 pandemic into an unknown future. A future that is post-pandemic, but where COVID-19 continues to exist. We as a collective of international researchers have endeavored to offer a unique view of collected data from our respective countries. Therefore, the purpose of the present study was to explore the influence of HBM factors on vaccine hesitancy in an international sample of college students. The study considered 2 research questions. First (RQ1): In an international sample of college students, how do factors of the HBM influence the decision to get vaccinated? Second (RQ2): In an international sample of college students, how does country of residence influence factors of the Health Belief Model?
Methodology
When presenting a study’s methodology, researchers may choose to apply a study specific format for example,56-58 while others may apply a more formal (eg, PRISMA, JARS) format (eg, Beigel et al, 59 Zeidabadi et al, 60 Kim and Jeong, 61 and DeDonno et al. 62 Based on the present studies design, the methodology is reported based on the Journal Article Reporting Standards (JARS), offered by the American Psychological Association. 63
Inclusion and Exclusion Criteria
Inclusion criteria for the present study included individuals 18 years of age or older with the ability to read in the country’s language. Being an online, anonymous survey, there were no stated exclusion criteria.
Participant Characteristics
The study included college students from 3 countries, Czech Republic, Israel, and the United States (US). The selection of these 3 countries was based on collaborative relationships between 3 institutions in each country. In addition, relations between these 3 countries have been favorable since prior, during and after the pandemic. A total of 509 individuals consented and started the online survey. A total of 447 participants completed all the items within the survey. The 62 individuals who did not complete the survey, did not complete more than 15% of the survey items, so no data imputation was conducted. Recruitment occurred through posting of survey link on social media sites that catered to college students. Of the 447 participants, 311 participants self-reported as female, 126 as male, 8 participants selected prefer not to answer, and 2 participants did not select any response (ie, skipped the item). The average age of the participants was 29.55 (SD = 11.85). Table 1 provides a summary of sex and age by country.
Sex and Age by Country.

Category result included Mean (Standard Deviation). Total result does not include 2 participants who skipped the question pertaining to sex.
Sampling Procedure
The study was approved by each universities Institutional Review Board (IRB). Due to the anonymous structure of the study, the IRBs exempted the study. A voluntary response sampling method was used in the study.
Sample Size
A power analysis using G*Power 64 was conducted to provide an estimate for the sample size. The analysis includes an estimated effect size of 0.20, power of 0.80, alpha (α) of .05, and 3 groups. Results revealed a total sample size of 416 would be required to identify a significant difference, if a difference exists.
Measures of Variables
Several variables were included in the study. Firstly, demographic variables included sex and age. The variable sex had 3 options; female, male, and prefer not to answer. The variable age was a 2-digit fill-in item.
A variable was included to assess vaccination status. This dichotomous variable included options of yes (vaccinated), or no (not vaccinated). To assess health beliefs, items were grouped based on the HBM factors of susceptibility, severity, benefits, and barriers. The susceptibility factor included 3 items:
1) the likelihood the participant would get COVID-19
2) likelihood children would get COVID-19
3) likelihood the elderly would get COVID-19.
Response options included very unlikely, unlikely, likely, and very likely. Results of the 3 items were summed to generate a susceptibility score with higher scores representing higher perceived susceptibility. The severity factor included 4 items:
1) seriousness if the participant got COVID-19
2) seriousness of long-term health issues after getting COVID-19
3) seriousness of COVID-19 for children
4) seriousness of COVID-19 for the elderly.
Response options included mild, moderate, severe, and very severe. Results of the 4 items were summed to generate a severity score with higher scores representing higher perceived severity. The benefits factor included 3 items:
1) likelihood vaccine will reduce chance of infection
2) likelihood vaccine would decrease severity and complications of COVID-19
3) likelihood vaccine would prevent the spread of COVID-19.
Response options were very unlikely, unlikely, likely, and very likely. Similar to other studies using the HBM, results of the 3 items were summed to generate a benefits score with higher scores representing higher perceived benefit of the vaccine. The barriers factor included 2 items:
1) difficult to find a location that offers the vaccine
2) difficult to find time to get the vaccine.
Response options included strongly disagree, disagree, agree, and strongly agree. Results of the 2 items were summed to generate a barriers score with higher scores representing higher perceived barrier.
Data Collection
Participants completed an anonymous self-reporting questionnaire designed to obtain information on demographics, health belief perceptions, and COVID-19 vaccination status. Initially, questionnaires were written in English and then translated into Hebrew and Czech, and then back translated into English. Any disparities in the questionnaires were amended to be equal across samples.
A survey methodology was used in the present study. Created in Qualtrics, online anonymous survey links were created for each country. During the months of August, 2021 through December, 2021, the links were posted on country specific social media site (eg, Facebook) group pages for college students. The online survey could be completed on desktop computers, laptops, tablets, or smartphones. Individuals who were interested in participating, would select the link and review a description and if desired, electronically consent to participate. To participate, the individual would click “I consent” and be directed to the survey form. As an alternative, individuals could either close the link, or click “I do not consent” which would close the survey form. Participants could skip questions as desired and could exit the form at any time without repercussions. At the end of the survey, participants were thanked for their participation. The total time to complete the survey was less than 10 min. Being an anonymous online survey, there was no interaction between the participants and researchers.
Psychometrics
Reliability coefficients were computed for the Health Belief Model variables. Table 2 provides reliability coefficients for each variable of the Health Belief Model.
Cronbach’s Alpha Results for Variables of the Health Belief Model.

Models and Data Analysis Procedure
The statistical package SPSS version 28 was used for statistical analyses. The statistical methods applied in the present study included descriptive statistics, correlation, analysis of variance (ANOVA), and binomial logistic regression.
To investigate the first research question (RQ1), in an international sample of college students, how do factors of the HBM influence the decision to get vaccinated, a binomial logistic regression was conducted. For the regression analysis, the dichotomous response of being vaccinated (yes/no) served as the criterion, while the HBM factors served as the predictor variables. Rather than explore the difference between countries, separate logistic regressions were conducted to explore the influence of the HBM factors on being vaccinated within each country.
To investigate the second research question, (RQ2) in an international sample of college students, how does country of residence influence factors of the Health Belief Model, a correlation analysis was conducted to explore associations between the HBM factors of susceptibility, severity, benefit, and barriers. An ANOVA was conducted to explore differences in HBM factors between countries. Specifically, country (Czech Republic, Israel, US) served as the independent variable, while susceptibility severity, benefit, and barriers were the dependent variables. All data were available for statistical analyses (ie, no missing data). A P < .05 was considered significant in all statistical analyses.
Results
COVID-19 Vaccination Status
A total of 359 (80.3%) of the sample self-reported receiving at least one dose of a COVID-19 vaccination. From the Czech Republic sample, 114 (73.5%) reported receiving the vaccination, 147 (92.5%) from the Israel sample, and 98 (73.7%) of the US sample reported having received the vaccination.
RQ1: In an international sample of college students, how do factors of the HBM influence the decision to get vaccinated? A binomial logistic regression was performed on the total sample to assess the influence of perceived susceptibility, severity, benefits, and barriers on the likelihood that participants are vaccinated. Separate regression models were conducted individually for each country as the scope of the study was not to conduct a critique between the countries.
Total Sample
Prior to conducting the regression analysis, normality of distribution was assessed by visual inspection of Normal Q-Q Plots. The data appeared to be normally distributed as it follows the diagonal line closely and did not appear to a have a non-linear pattern. In addition, 7 assumptions were explored prior to conducting the analysis. The first 4 assumptions relate to study design and measurements, while the other 3 relate to how the data fits the binomial regression model. The first assumption verified was that the dependent variable of vaccination status (vaccinated, not vaccinated) is dichotomous. The second assumption verified was that all the independent variables were continuous. The third assumption verified was independence of observations of the dependent and independent variables. The fourth assumption verified was the there was a minimum of 15 cases per independent variable. The fifth assumption being linearity of the continuous variables with respect to the logit of the dependent variable was assessed via the Box-Tidwell procedure. The assumption of linearity was validated as the 4 continuous independent variables were found to be linearly related to the logit of the dependent variable (P > .05). The sixth assumption that data must not show multicollinearity was validated through variance inflation factor (VIF) for each of the independent variables ranging from 1.027 to 1.048. Finally, the seventh assumption that there should be no significant outliers was validated as no observation was greater or less than 2.5 standard deviations from the associated mean score.
The logistic regression model was statistically significant, χ 2 (4) = 179.512, P < .001. Table 3 provides results for pseudo R-squared values.
Pseudo R 2 values.

The model explained 52.6% (Nagelkerke R 2 ) of the variance in vaccination and correctly classified 87.2% of cases. Sensitivity was 95.3%, specificity was 54.5%. Positive predictive value was 89.5% and negative predictive value was 73.9%. The area under the ROC curve (Figure 1) was 0.909, 95% CI [0.875, 0.943], which is considered as outstanding level of discrimination according to Hosmer et al. 65
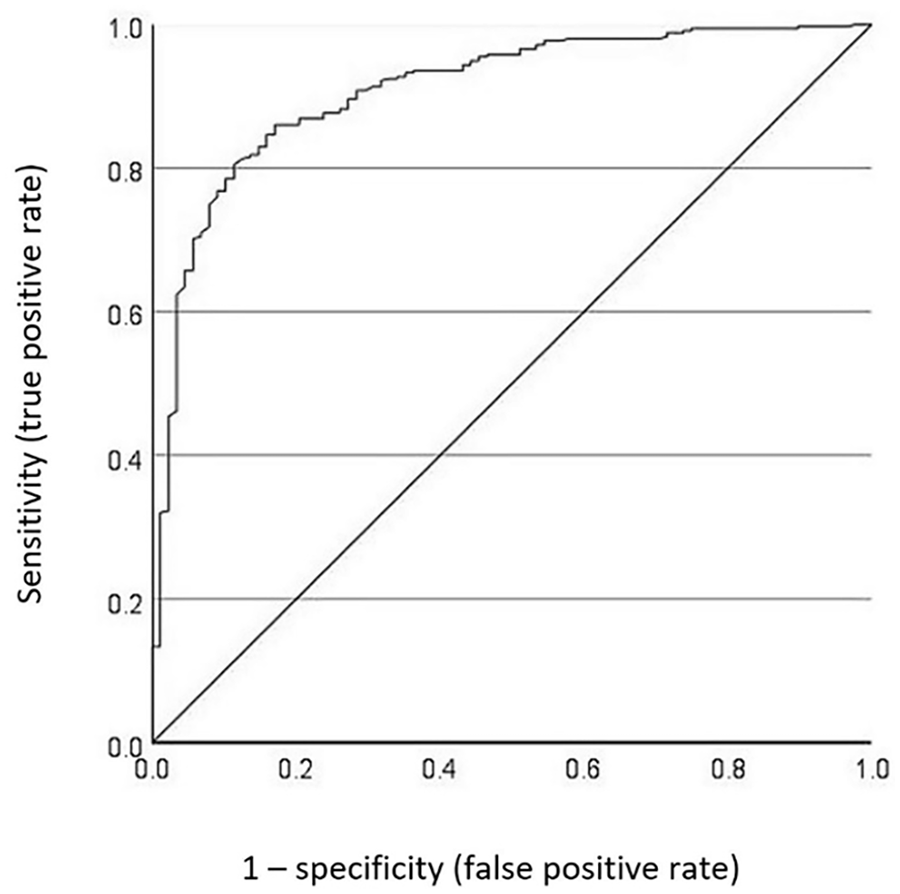
ROC curve predicting vaccine status based on HBM factors.
Of the 4 predictor variables only 2 were statistically significant: severity and benefit for the total sample (see Table 4). Increasing scores on severity and benefit were associated with increased likelihood of being vaccinated.
Logistic Regression Predicting Likelihood of Vaccination Based on Susceptibility, Severity, Benefits, and Barriers.

Czech sample
Logistic Regression Predicting Likelihood of Vaccination based on Susceptibility, Severity, Benefits, and Barriers. The logistic regression model was statistically significant, χ 2 (4) = 56.604, P < .001. The model explained 44.7% (Nagelkerke R 2 ) of the variance in vaccination and correctly classified 83.2% of cases. Of the 4 predictor variables, only 2 were statistically significant: Severity and Benefit (Table 5).
Czech Sample—Logistic Regression Predicting Likelihood of Vaccination Based on Susceptibility, Severity, Benefits, and Barriers.

Israel sample
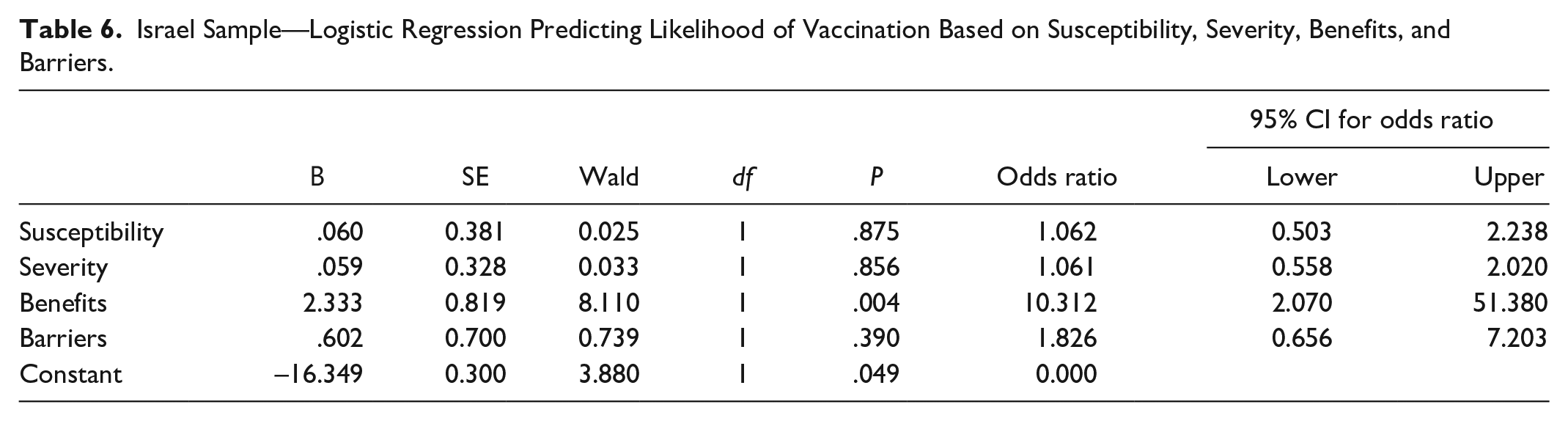
Logistic Regression Predicting Likelihood of Vaccination based on Susceptibility, Severity, Benefits, and Barriers. The logistic regression model was statistically significant, χ 2 (4) = 64.776, P < .001. The model explained 80.7% (Nagelkerke R 2 ) of the variance in vaccination and correctly classified 96.9% of cases. Of the 4 predictor variables, only Benefit was statistically significant (Table 6).
Israel Sample—Logistic Regression Predicting Likelihood of Vaccination Based on Susceptibility, Severity, Benefits, and Barriers.
US sample
Logistic Regression Predicting Likelihood of Vaccination based on Susceptibility, Severity, Benefits, and Barriers. The logistic regression model was statistically significant, χ 2 (4) = 73.561, P < .001. The model explained 62.1% (Nagelkerke R 2 ) of the variance in vaccination and correctly classified 73.7% of cases. Of the 4 predictor variables, only 2 were statistically significant: Severity and Benefit (Table 7).
US Sample—Logistic Regression Predicting Likelihood of Vaccination Based on Susceptibility, Severity, Benefits, and Barriers.

(RQ2) In an international sample of college students, how does country of residence influence factors of the Health Belief Model? To explore differences in HBM factors by country of residence, a One-way Analysis of Variance (ANOVA) was conducted. The independent variable was country (Czech Republic, Israel, US), while the dependent variables were the factors of the HBM; susceptibility, severity, benefits, and barriers. Descriptive statistics of HBM factors by country results of the one-way ANOVA are provided in Table 8. Results of the one-way ANOVA revealed statistically significant differences by country for all 4 HBM factors, with effect sizes ranging from small to large. As can be seen, there was a large effect for severity (η 2 = 0.223), and small effect sizes for the remaining 3 HBM factors (η 2 = 0.042-0.124).
Descriptive Statistics of HBM Factors by Country and One Way ANOVA Results.

Note. Sample sizes, Czech Republic (n) = 155, Israel (n) = 159, US (n) = 133, Total (n) = 447.
As illustrated in Figure 2, post-hoc analysis using Lease Square Difference (LSD) revealed several statistically significant differences within HBM factors and between countries. For susceptibility, there were significant differences between Israel and the US, and the Czech Republic and the US (P < .001). Pertaining to severity, there were significant differences between all 3 countries (P < .05). For benefit, there was significant difference between Israel and the US (P < .001). For barriers, there were significant differences between Israel and the US, and the Czech Republic and the US (P < .005).

Health belief model (HBM) factors by country.
Discussion
This study was the first to perform a cross-cultural comparison of COVID-19 related to vaccination among college students residing in either the Czech Republic, Israel, or the United States. Further, it provides evidence to the influence of the Health Belief Model on the decision to get vaccinated for COVID-19. There were both similarities, as well as differences in HBM perceptions between the countries.
With respect to the first research question (RQ1), In an international sample of college students, how do factors of the HBM influence the decision to get vaccinated, a binomial logistic regression was performed on the entire sample (Total Sample) and individually for each country. Table 9 highlights the predictors of vaccine hesitancy from the HBM for the total sample and the 3 countries. As can be seen, all models included the factor of perceived benefits as a predictor of vaccine hesitancy, while 3 of the models also included perceived severity of COVID-19 as predictors of vaccine hesitancy.
Health Belief Model Predictors of Vaccine Hesitancy by Country.

It appears based on the present study’s findings; perceived benefit is a significant motivator to get vaccinated. This is in-line with research showing that perceived benefits of vaccination are a good predictor of an intention to receive the vaccine, 66 and acceptance of COVID-19 vaccine. 53 Results are also similar to research conducted on a sample of adults in Israel. Results revealed that perceived benefits, but not severity was associated with vaccine hesitancy. 54 Although, the researchers also found susceptibility and barriers to be associated with vaccine hesitancy.
To truly have an effect on behavior, appropriate factors need to be considered. Here in, it seems appropriate to emphasize the benefits of a vaccine, as well as its severity, beyond death. Governments and policymakers should consider added emphasis on promoting the benefits of a vaccine. This however may be difficult as anti-vaccine (anti-vax) social media accounts have gained more than 7.8 million followers, an increase of 19% since 2019 Center for Countering Digital. 67 Many anti-vaxxers site a study claiming a causal relationship between the measles, mumps, and rubella (MMR) vaccine and autism spectrum disorders (ASD). 68 However, numerous studies have provided evidence that casts doubt on the claimed causal relationship between the MMR vaccine and ASD occurrence.69-71 However, despite these studies, some parents remain hesitant to accept the MMR vaccine, resulting in a resurgence of measles. 72 Further, the message put forth by policymakers relative to getting the vaccine may have an impact on hesitancy. One study tested 4 standard vaccine education strategies designed to increase parental intent to vaccinate their child or children. Results revealed none of the strategies increased parent intent. In fact, one strategy designed to correct parents’ misperceptions of a link between MMR and ASD, actually had a reverse effect, decreasing vaccine intent among the most vaccine hesitant parents. 73
Policymakers may also want to consider further promoting the severity, beyond death, of the virus. Many reporting websites such as the CDC and WHO, seem to focus on number of deaths (which is certainly severe), but only offer more detailed severity factors on secondary web pages, which are more difficult to find.1,74 In addition to death, reporting entities may want to put forth greater emphasis on the severe symptoms such as difficulty breathing or shortness of breath, fatigue, difficulty thinking, headache, chest pain, joint or muscle pain, diarrhea, sleep problems, and change in smell or taste.1,75
With respect to the second research question, (RQ2) in an international sample of college students, how does country of residence influence factors of the Health Belief Model, results revealed a significant difference between countries. For perceived susceptibility and barriers, the US differed from both the Czech Republic and Israel, while there was no difference between the Czech Republic and Israel. More specifically, the US sample had lower perceived susceptibility, but higher perceived barriers than both the Czech Republic and Israel samples. Both the Czech Republic sample and the US sample found perceived severity and perceived benefit to predict vaccination status. In other words, perceived severity of the disease if contracted, was a significant motivator in the US and Czechia but not Israel. The Israel sample found only the factor of benefit to predict vaccination status.
The different predictors of vaccine hesitancy in the countries further promotes the need for culture specific campaigns/policies adopted by the local government of countries. Country specific factors that can cause variability include, countries population, overall health expenditures, overall government health expenditure per capita, policies to related air pollution, timely application of containment policies, as well as an effective and timely vaccination plan.76,77
Another variable that appears to influence vaccine hesitancy is confidence in government. Trent et al 78 found participants in Sydney and Melbourne who had high confidence in their government had greater willingness to receive the vaccine, while participants in New York and Phoenix, Arizona with high confidence in their government were less likely to receive the vaccine.
The variation in perceptions may also be due to a difference in reality. Essentially, it is possible that the incidence rates and death rates in each country, may have been a cause of the perceptions of that countries sample. It would reason that in countries where incidence rates and death rates were high, perceived views of susceptibility and severity would also be high. Future research could explore various COVID-19 perceptions and the potential alignment with reality (ie, country incidence rates and death rates).
Secondly, the differences in perceptions and reality may be due to participants general knowledge of COVID-19. It is possible that the sample, being college students, were not engaged in COVID-19 information such as real susceptibility and severity. Thirdly, it is possible that that sample had engaged in COVID-19 information, but the information gathered was inaccurate (ie, disinformation). There is good evidence as to the dissemination of inaccurate COVID-19 information. 79 A more accurate understanding of the risks during a pandemic, may yield better acceptance of prevention practices.
Strengths and Limitations
The strength in the present study is the sample being from 3 countries. This can provide unique perspectives to vaccine hesitancies. A limitation is that of the sample being primarily college students. While the Israel sample was older, they were still recruited from university websites.
Theoretical and Practical Implications
From a theoretical perspective, the present study offers additional insight into vaccine hesitancies. Future research could apply an experimental methodology to explore interventions that could influence perceived severity and benefits so as to reduce vaccine hesitancies. Practically, policymakers could put forth added emphasis as to the severity of the virus as well as benefits of the vaccine. While death is certainly severe, other severity factors that are potentially more aligned with the younger and healthy population could be further promoted. In addition, policymakers should focus on a pandemic strategy that is specific to their own environment. The variability in the 3 countries suggests a generic project template for a pandemic strategy may not be appropriate.
Conclusion
Dealing with the COVID-19 pandemic has been a significant global challenge. The present study provides evidence that policy makers should further promote the benefits of a vaccine, as well as potential severity of the virus. In addition to highlighting the death rate of a virus, it may be prudent to highlight the severe and potentially long-term symptoms of a virus. Finally, the present study provides evidence of varying perceptions by country of susceptibly, severity, benefits, and barriers associated with a virus and vaccine. Rather than a global model for dealing with a virus, governments should consider their own strengths, weaknesses, opportunities and threats in creating an effective model to mitigate the virus.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: From Ariel Research and Development Authority
Ethics Approval and Consent to Participate
All methods used in this study were carried out following all relevant guidelines and regulations (Declaration of Helsinki). The purpose of the study was fully disclosed to all participants. All participants provided informed consent. Participant data was anonymized (participants’ names replaced with number randomized numbers) and data gathered was kept private and secure. The study was approved by Institutional Review Board in each in each country separately.