
Abstract
Anemia progresses due to low red blood cells counts or hemoglobin. The World Health Organization (WHO) has suggested the condition to be a serious global public health problem that affects pregnant women worldwide. Anemic pregnant women may suffer post-partum hemorrhage, pre-term delivery, seizures, and severe cases of anemia that potentially lead to cardiac failure or death. However, it is pertinent for pregnant women and health service providers to have the adequate knowledge about the factors associated with anemia in pregnancy. Thus, this study assessed the factors associated with anemia in pregnancy women attending primary healthcare (PHC) centers in Ibeju-Lekki Local government area, Lagos state. This study employed descriptive cross-sectional design using multi-stage sampling method to recruit 295 pregnant women into the study. Data were collected using a semi-structured, self-administered questionnaire. The recruited participants (56.6%) were majorly in their third trimester, of which their mean age was 28.7 ± 5.9 years. About 80.7% of the participants were married, having a mean knowledge score of 6.6 ± 3.2. More than half of respondents (56.3%) were anemic and had a poor knowledge (50.5%) of anemia in pregnancy. The mean hemoglobin concentration within the population was 11.06 ± 0.73 g/dl with a range of 8.3 to 12.0. There was no significant association between the respondents’ knowledge of anemia in pregnancy and anemic status (X2 = 0.549; P = .45). However, this study observed a significant association between dietary diversity score and anemic status (X2 = 8.66; P = .01) and the trimester status of respondents’ first antenatal visit (X2 = 9.603; P = .008). The study concluded that anemia in pregnancy was associated with maternal factors such as their first antenatal visit and the dietary diversity score. Due to this, proper education of pregnant women on anemia by health workers during antenatal clinics or visits should be prioritize to improve their anemia status.
Anemia is a condition that progresses as a result of low red blood cells counts or hemoglobin levels. The World Health Organization (WHO) has suggested the condition as a serious global public health problem that affects pregnant women worldwide.
As a result of the increasing prevalence of anemic conditions in Nigeria, there has been a need for the adequate implementation of improved strategies to mitigate the negative effects of anemia on maternal and child health. This study therefore addresses on the local knowledge of anemia, antenatal care (ANC) practices and dietary habits in relation to cases of anemia among pregnant women who attend primary healthcare (PHC) centers in the region of investigation.
The findings suggest that health workers and other preventive care officials should take a responsibility to effectively educate pregnant women on anemia during their antenatal clinics or visit to improve their anemic status and prevent pregnancy complications due to anemia.
Introduction
Pregnancy is usually associated with several undesirable health challenges including hypertension, anemia, urinary tract infection, gestational diabetes, obesity and weight gain, hyperemesis gravidarum, among others. Yearly, about half a million women suffer ill health, disability or death from pregnancy related complications and childbirth. 1 Anemia has been found to be directly or indirectly associated with neonatal, child and maternal morbidity and mortality especially in low- and middle-income countries. 2 Mild to moderate anemia status in pregnancy can lead to reduced maternal and fetal well-being. Anemic pregnant women may suffer post-partum hemorrhage, pre-term delivery, seizures, and severe cases of anemia that lead to cardiac failure or death. 3 This condition regularly informs a nation’s socio-economic status as it leads to long-term consequences of impaired cognitive development, reduction in economic productivity and quality of life, thereby contributing to the poor economic status of a country. 1
Anemia is a condition of reduced number of red blood cells in circulation or depleted hemoglobin levels in blood below the normal range. As a result of this deficit, the capacity of red blood cells to transport oxygen- to body tissues and organs is diminished. 4 This illness affects any human population, although, children and pregnant women are most vulnerable. WHO 1 characterizes anemia as hemoglobin level below 12.0 and 11.0 g/dl among non-pregnant and pregnant mothers, respectively. For pregnant mothers, hemoglobin levels between 10.0 and 10.9 g/dl are considered mild anemia. Those with moderate anemia have hemoglobin levels ranging from 7.0 to 9.9 g/dl, while those with severe anemia have hemoglobin values below 7.0 g/dl. 5
Anemia becomes a mild global health issue when the prevalence is between 5.0% and 19.9%, Once this increases between 20% and 39.9%, it is considered as a moderate global health problem. However, a prevalence of 40% or higher is considered a severe public health problem. 1 Globally, anemia affects over half a billion women aged 15 to 49 years (29.9% of the global population) and it presents as a common health complication particularly in developing countries as compared to other developed nations. 6 Over 32 million pregnant women in the world (about 38%) are anemic and in Africa alone, there are 9.2 million pregnant women (46.3%) affected by anemic conditions. 7 The Nigerian Demographic Health Survey (NDHS) 8 reported that 61.1% of pregnant mothers are anemic, an indication that anemia is a severe global health concern. Given the population, the classification was grouped into mild anemia (25.8%), moderate anemia (33.0%), and severe anemia (2.3%). 8
The risk for pregnancy related illnesses increased with malnutrition, a lack of micronutrients required for the well-being of the mother and child. 9 Moreover, having the necessary knowledge of anemia in pregnancy is also a basic factor that can influence the disease condition as it is a prerequisite for the prevention of anemia. 10 Notably, within rural settlements, anemic conditions are influenced by a limited access to healthy dietary resources to prevent malnutrition, low level of education affecting access to health education, and poor health practices including antenatal care (ANC), which is necessary to promote the wellbeing of the mother and unborn child. 11
Given the high prevalence of anemic condition in Nigeria, there is a need for the adequate implementation of improved strategies to mitigate the negative effects of anemia on maternal and child health. As a result, this study was conducted to identify the underlying knowledge of anemia, ANC practices and dietary habits to understand their associations with anemia among pregnant women who attend primary healthcare (PHC) centers in Ibeju-Lekki LGA in Lagos state.
Methods
Study Design and Setting
A cross-sectional research design was adopted to assess different variables in population during this study. The location of study, Ibeju-Lekki is a conglomeration of 2 communities, Lekki and Ibeju-Agbe within the Eti-Osa-East Local Council Development Area (LCDA). Eti-Osa East is bordered by the local government office to the West, Epe community to the East, and the Atlantic Ocean to the South. Ibeju-Lekki is estimated to have a land mass of 75 km2 in length and about 20 km2 width at its widest point, encompassing a circumference 646 km 2 . The study population was focused on pregnant women who attended the PHC centers in Ibeju-Lekki LGA, Lagos State within February-April, 2002, regardless of age or period of pregnancy. There are 9 PHC facilities in this LGA, of which 5 were selected by stratified random sampling.
Participants included pregnant women who attended antenatal clinic, having a secondary hemoglobin report and consented to the study, whereas those without a hemoglobin report were excluded from participation.
Ethical Clearance
An ethical approval for the study was secured from the Ethical Review Committee of Babcock University’s Department of Public and Allied Health in Ilishan-Remo, Ogun state, (BUHREC number 429/22). Also, consents were voluntarily taken from chosen PHC facilities and the study participants. Data gathered were strictly handled as confidential. To preserve authenticity, all respondents were recognized solely by serial numbers. Respondents had the rights to withdraw from the study at any time without consequences.
Sampling Size Determination and Technique
Minimum sample size was determined by the Cochran formula for estimating sample size for smaller population. 12

Z = at a 95% confidence interval, the Normal deviation is considered normal (1.96).
P = 49.5%, 13 which is the prevalence of anemia identified among pregnant mothers in Lagos Nigeria.
q = 1 − P
d = 0.05, with a significance value of .05 (constant)

n0 = 384.
The sample size was adjusted using the formula,

n0 = sample size, 384.
N = population size = 880
A 10% non-response rate was added to the sample size to obtain 295.
The multi-stage sampling technique was adopted to recruit 295 participants for the study. Using a systematic sampling technique, 5 PHC facilities were selected for the study similar to Appiah et al. 10 The selected centers were Awoyaya PHC, Bogije PHC, Ibeju PHC, Orimedu PHC, and Solu-Alade PHC. Simple random sampling technique was used to select participants from each of the PHC centers for the study.
Data Collection
To collect information from respondents, a semi-structured pre-tested interviewer administered questionnaire developed from literature by the researcher was employed in this study. Face validity, construct and content validity were performed by expert researchers to ensure that the instrument was standardized. The instrument was pre-tested in Denro PHC to ensure its reliability.
The questionnaire was developed in English language, translated to Yoruba, which is the local community dialect. Afterward, the Yoruba questionnaire was back translated to English language to screen for inadequacies or changes in meaning of words.
Statistical Analysis
Data collected were analyzed with IBM Statistical Package for Service Solutions (SPSS) version 25 using descriptive and inferential statistical tests. Chi-square was used to test for the association between study variables at P < .05 significance level.
Results
Socio-Demographic Characteristics of the Respondents
A total of 295 participants with a mean age of 28.7 ± 5.9 years were involved in the study. Less than half (48.1%) of the pregnant women were within ages 27 to 36 years. Majority (83.1%) of the respondents were Christians and 52.5% of the Yoruba ethnic group. About 39.0% were self-employed, with 52.2% having at least a secondary level of educational. Up to 80.7% of the respondents were married and 33.9% had no children at the time of conducting the study (Table 1).
Socio-demographic Characteristics of the Respondents.

Respondents Knowledge of Anemia in Pregnancy
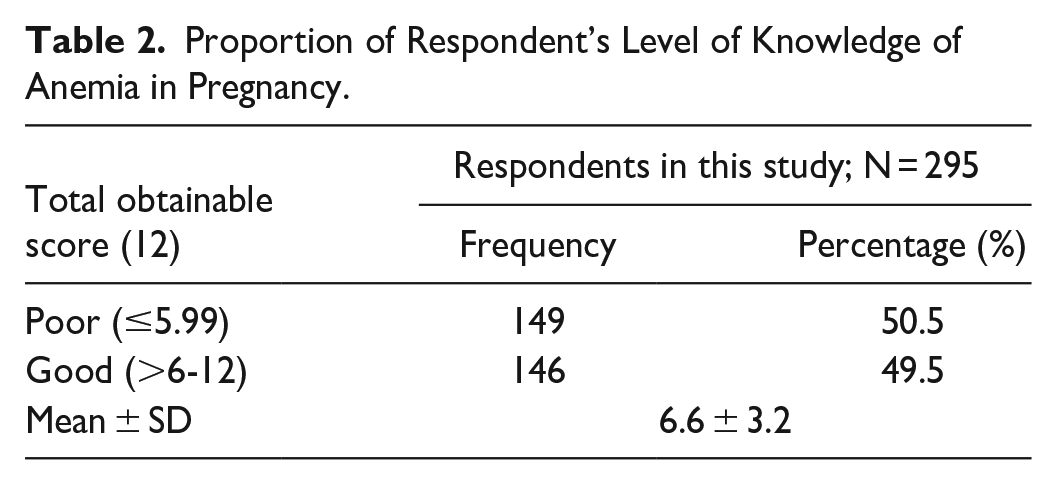
The respondents’ knowledge of anemia measured on a 12-point rating scale showed a mean score of 6.6 ± 3.2. The knowledge of anemia was also grouped into 2 categories based on a 50th percentile. Those who scored less than equal to 6 (≤5.99) were regarded as having a poor knowledge, while those who scored greater than 6 (>6-12) were regarded to as having high knowledge of the disease. Overall, approximately half of the respondents (50.5%) showed they had a poor knowledge of anemia in pregnancy (Table 2).
Proportion of Respondent’s Level of Knowledge of Anemia in Pregnancy.
Respondents’ ANC in Pregnancy
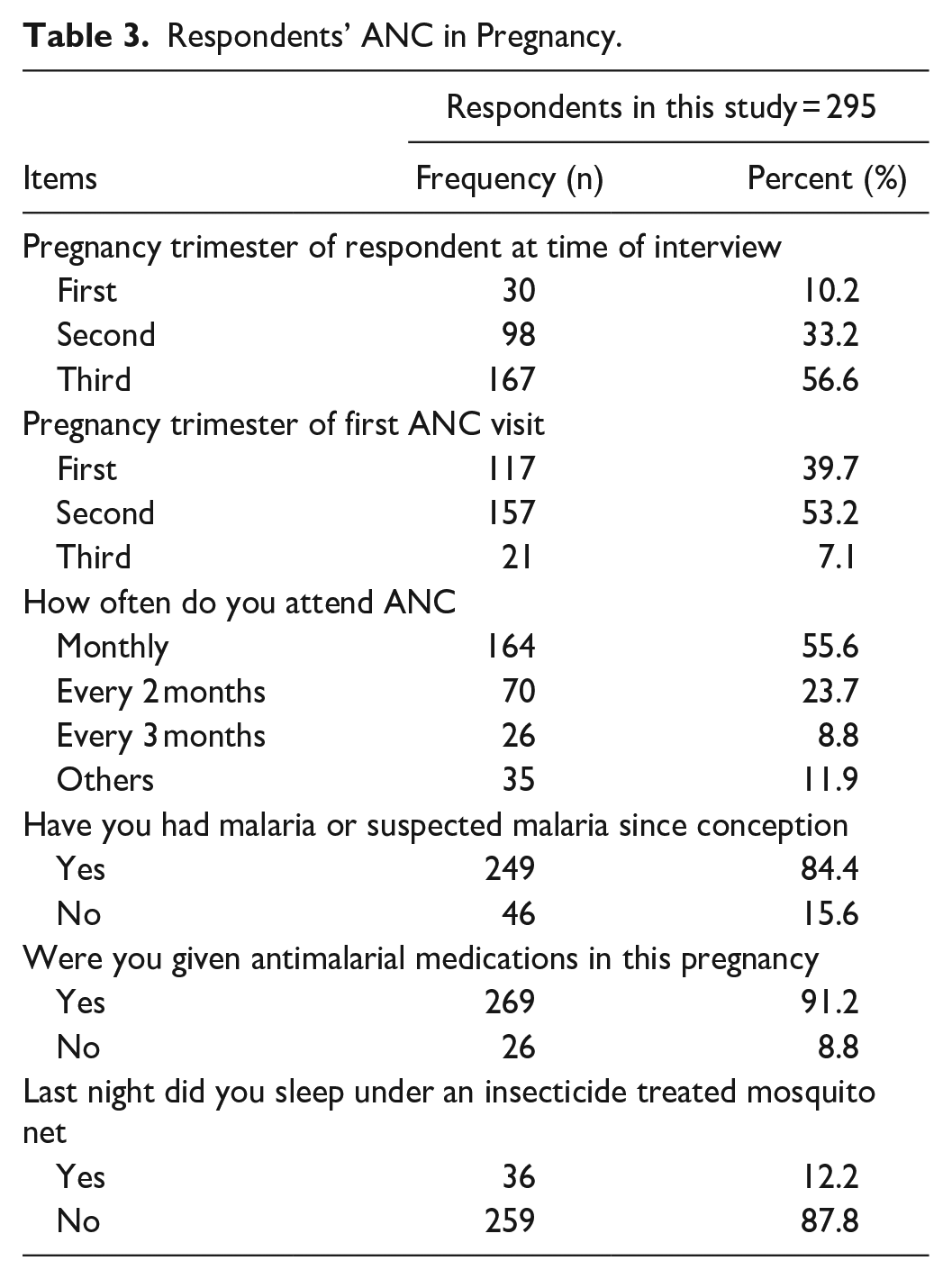
More than half (56.6%) of the respondents were in their third trimester of pregnancy and 53.2% reported that they had registered for their first antenatal visit during the second trimester of their pregnancy. For the antenatal clinic visits, 55.6% of the respondents reported that they attended monthly. Majority (84.4%) of the respondents reported that they had malaria since conception, of which 91.2% were receiving antimalarial medication. When further investigated, only 12.2% of the respondents reported the use of an insecticide treated mosquito net the night preceding the collection of the personal study information (Table 3).
Respondents’ ANC in Pregnancy.
Respondent’s Dietary Habits
With respect to the dietary habits of study participants, 65.4% reported that they practiced pica, of which 31.1% of them ate clay, mostly (93.8%) during the first trimester of their pregnancy. Few (16.9%) of the respondents reported that they drank alcoholic beverages, while 85.8% drank tea and/or coffee. Of those who consumed tea and/or coffee, 39.5% reported the consumption of tea and/or coffee at least, once daily. Majority (80%) took multivitamin supplements, of which 75.8% also reported taking folic acid. In addition, respondents reported the consumption of the following food group—grains (100%), pulses (74.9%), meat, poultry and fish (61.7%), dark green leafy vegetables (31.5%), fruits (15.9%), eggs (14.6%), nuts and seed (5.4%), and dairy (6.8%) (Table 4).
Respondent’s Dietary Practices.

Furthermore, the Minimum Dietary Diversity for Women (MDD-W) was calculated from 24-h dietary recall data. All foods consumed day before the study were categorized into 10 food groups. Those who consumed a food item from any of the groups responded “Yes,” otherwise, the response was “No.” Dietary diversity score of 10 points was computed by adding all values of the groups. Following this, the total score values were categorized as a low (≤3), medium (>3-6), or high (≥7) dietary diversity score. When estimated, 43.7% of the respondents had a medium dietary diversity score (Figure 1).
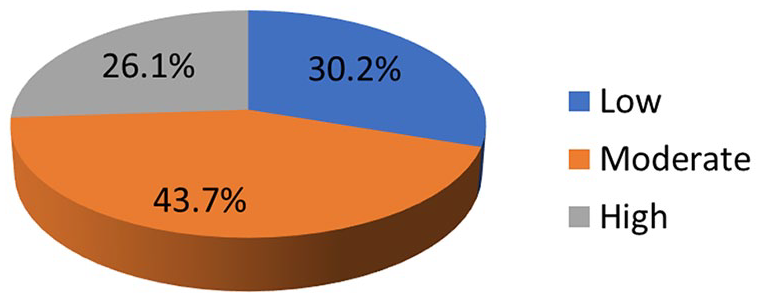
Respondents dietary diversity score.
Respondents’ Anemic Status
This study identified the mean hemoglobin concentration level of participants as 11.06 ± 0.73 g/dl with a range of 8.3 to 12.0 g/dl, suggesting that many of the respondents 8.4 ± 0.45 g/dl (56.3%) were anemic. More than half (53.9%) of the respondents had conducted a hemoglobin estimation during their second trimester (Table 5).
Respondents Anemia Status.

Factors Associated With the Variables and Anemic Status in Pregnant Women
To test the association between variables, a chi-square analysis was conducted on the respondents’ anemia and status. There was no significant association between knowledge of anemia and their anemic status (X2 = 0.549; P = .45) among the respondents. A similar analysis was conducted on a respondent’s antenatal practices and their anemic status. This study further identified a significant association between the trimester of first antenatal visit and participants’ anemic status (X2 = 9.603; P = .008), and between participants’ dietary diversity score and anemic status (X2 = 8.66; P = .01) (Table 6).
Associated Factors of Variables and Anemia Status in Pregnancy Women.

Discussion
In this study, the mean age of the respondents was identified as 28.7 ± 5.9 years, of which less than half were within the ages of 27 to 36 years, similar to reports by Adokiya et al 14 and Woldegebriel et al 15 in Ghana and Ethiopia, respectively. This similarity suggests the relative reproductive age, unrestricted by country borders. However, in another study by Weldekidan et al 16 in Southern Ethiopia, the reproductive age group was lower, that is between 20 and 29 years.
Here, respondents were mostly Christians, similar to reports by Weldekidan et al, 16 which may be as a result of conducting the study in a Christian-dominated area. The study revealed that the respondents were Yorubas, as in reports by Oyelese et al, 17 in South-west Nigeria, also likely resulting from a Yoruba-dominated location of study. Respondents in this study identified as self-employed, at variance to the study of Weldekidan et al 16 in Southern Ethiopia and Woldegebriel et al 15 where respondents were mainly housewives. This difference in findings may be that more women were encouraged to work outside their home in the current study area. Consistent with this, most of the respondents only had a secondary educational level in contrast with the reports by Weldekidan et al 16 where most of their respondents had primary educational level and those of Woldegebriel et al, 15 where most respondents were illiterates. In the current study, respondents were majorly married women and less than half had no children.
This investigation observed the poor knowledge of anemia among participants, similar to the reports by Wemakor, 5 Balasubranian et al, 18 and Keneni et al. 19 However, the result is at variance with the findings of Yesufu et al 20 in Lagos, Nigeria where they reported that more than half of the respondents had an average knowledge score.
The study also revealed that most of the respondents had their first ANC booking during the second trimester pregnancy, similar to reports by Welekidan et al. 21 This current observation is however at variance with the reports by Wemakor 5 in Ghana where many of the study women started ANC visit in the first trimester. The study revealed that most of the respondents were given anti-malaria drugs, in contrast with the reports by Wemakor 5 in Ghana where only a few of their respondents received anti-malaria drugs. The difference in result could be because antimalarial medication is a routine pregnancy care in Nigeria as opposed to Ghana, where it may not be a routine practice. Also, the current study revealed that few of the respondents used insecticide-treated nets. This corroborates the finding of Wemakor 5 in Ghana but the use of insecticide-treated nets was unpopular and explains why most of their respondents presented with malaria during pregnancy. Malaria in pregnancy is associated with poor maternal and child health outcomes such as intrauterine growth retardation, preterm birth, low birth weight, and maternal anemia.
Most of the respondents practiced pica involving the ingestion of chalk, kolanut, uncooked maize and clay. The current study also revealed a high intake of tea and/or coffee among respondents, majority of which reported a low intake of alcoholic beverages. This is similar to the reports by Wemakor 5 in Ghana. This study revealed that majority of the respondents used multivitamin drugs containing folic acid, also similar to reports by Wemakor 5 in Ghana. The study revealed that the respondents had low to moderate dietary diversity score and is similar to the results of Tulu et al 22 in Ethiopia. The Minimum dietary diversity score (MDDS) is used as the proxy measure of nutritional quality in pregnant women. Since pregnancy physiologically demands high nutrition, it is advisable to diversify the diet than the usual one. Low average monthly income and food taboos during pregnancy in rural communities might have caused the low and medium dietary diversity scores, which in turn resulted in anemic conditions among respondents in the study area.
The prevalence (56.3%) of anemia observed in this study was higher than those reported reported by Sholeye et al 12 in Sagamu and a repeat study Sholeye and . Animasahun. 23 Another study by Dim et al 24 also showed that anemia was identified in 42.6% of pregnant women and another in South-eastern region reported that 28% of the pregnant women were anemic. There is certainly an extra demand for iron by pregnant women for fetal growth and development during pregnancy and a difficulty in fulfilling this demand. The high prevalence of anemia in this study could be due to the socio-economic status of the women, which may have a reflective effect on their nutritional status and health behavior. These differences in the prevalence of anemia might be due to variations in socioeconomic status, attention given for focused ANC, supplementation of iron sulfate throughout the pregnancy, dietary patterns, sample size, geographical and lifestyle variations.
This study also showed an association between respondents’ maternal age and anemic status and is consistent with previous reports by Kumar et al 25 and Lin et al 26 in India. This might be because as maternal age increases, the mother may face repetitive and relentless pregnancies, endure the collective result of the exhausting labor-related complications, and be subjected to other illnesses which may predispose her to anemia.
This study suggested that respondents’ knowledge of anemia had no association with their anemic status, which is at variance with results by Wemakor 5 and Keneni et al 19 where they reported an association between knowledge of anemia and anemic status. The difference in finding may be because of the difference in study location and educational level. This study however revealed that ANC visits was associated with anemic status, correlating with the result of Tulu et al 22 where they reported an association between ANC and anemic status.
The study found an association between the respondent dietary diversity score and their anemic status, consistent with reports from Deriba and Jemal 27 that revealed an association between the dietary diversity score and anemia among pregnant women in West Shewa zone, Ethiopia.
Although the consumption tea and/or coffee immediately after food intake may interfere with iron absorption, leading to insufficient dietary iron intake in pregnant mother, as tea is known to reduce iron absorption, this study revealed no association between tea and/or coffee intake and anemic status. However, some participants reported tea and/or coffee intake, which could be related to alteration in iron absorption. The findings from Zekarias et al 28 and Mulepati and Chaudhary 29 indicated an association between drinking tea and/or coffee and reduction in blood iron level.
Conclusion
Anemia in pregnancy was associated with maternal factors such as their first antenatal visit and the dietary diversity score. In order to improve the outcome of this condition, health interventions should be specifically targeted at the individual level, including health-related factors to improve access to ANC and nutritional status in pregnancy.
Supplemental Material
sj-docx-1-inq-10.1177_00469580231159961 – Supplemental material for Factors Affecting Anemia in Pregnancy Women in Ibeju-Lekki, Lagos State, Nigeria
Supplemental material, sj-docx-1-inq-10.1177_00469580231159961 for Factors Affecting Anemia in Pregnancy Women in Ibeju-Lekki, Lagos State, Nigeria by Olusesan Oyewole Oyerinde, Essien Annieye Nkanga, Ifeoluwa Emmanuel Oyerinde, Onamade Akintoye, Ifeoluwa Asekun-Olarinmoye and Quadri Kunle Alabi in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Author Contributions
OOO, NAE, AOI intellectualized the knowledge, performed the experiment, prepared the data, done data analysis and wrote the draft of the manuscript. OEI, OA, AQK intellectualized the knowledge, corrected and reviewed the results, and contributing to writing and editing of the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Standards Disclosure
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Ethic Review Board of Institute of Public Health, Babcok University. Written informed consent was obtained from all subjects.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.