
Abstract
Dietary diversity is a crucial element of an inclusive care for people living with HIV (PLWHIV), particularly in resource-limited countries where undernutrition, poor intention, and poor attitude toward diversified diets are the common challenges. The aim of this study was to assess the
• Poor dietary diversity can hasten the progression of HIV infection and increase the risk of developing opportunistic infections (OIs). • Optimal nutrition can help boost immune function, maximize the effectiveness of ART, reduce the risk of OIs, and improve the overall clinical care and life expectancy. • Undernutrition is more common among PLWHIV at advanced clinical stages, untreated people, and those who earn a poor livelihood.
• Assuring adequate access to food in HAART treatment programs has been a central demand of PLWHIV in low-income countries • The Food by Prescription program involves nutritional assessment, counseling, and support to address nutritional problems in malnourished patients with HIV. • The Food by Prescription program is challenged by individual, institutional, community, and health systemrelated factors
• Intention can be used to extend theories and to design interventions, which can increase the ability of these programs to change behavior rather than treat only malnutrition of the PLWHIV • The qualitative findings indicated that delivery of HIV care requires a drive for livelihood development and economic improvement, creating a sense of responsibility for sustainable HIV care by creating behavioral change at the individual level. Conclusion: Dietary inadequacy was strongly correlated with being in the sociodemographic groups that are at heightened risk of adverse clinical outcomes. It is worthwhile to investigate behavioral intention as a potential determinant of the clinical outcomes rather than choose symptomatic treatment of malnutrition. • It is worthwhile to investigate behavioral intention as a potential determinant of the clinical outcomes for sustainable HIV care. • The paradigm model is supportive and can be suggested for application to any behavioral change program considered to prevent undernutrition and improve quality of life through education focused on subjective norm, attitude, and social norms, other than the Food by Prescription program which is focused on symptomatic treatment.What Do We Already Know About This Topic?
How Does Your Research Contribute to the Field?
What Are Your Research’s Implications Toward Theory, Practice, or Policy?
Introduction
A many-sided and negative emphasis is given to the role of behavioral intention in people infected with human immunodeficiency virus (HIV).1,2 Poor dietary diversity can, in turn, hasten the progression of HIV infection and increase the patient’s risk of developing opportunistic infections (OIs).
There is a similarity between the cellular effects of malnutrition and HIV—the immune system becomes compromised by decreasing CD4 T cells, suppressing delayed hypersensitivity, and abnormal B-cell responses. Providing sufficient food to meet people’s basic nutrition needs for health, growth, and development has been a long-standing challenge for African countries. 3 Thus, they require greater protein and micronutrient intake in order to improve the weakened immune system.4,5 Optimal nutrition can help boost the immune function, maximize the effectiveness of antiretroviral therapy (ART), reduce the risk of OIs, and improve the overall clinical care and life expectancy of PLWHIV. 6
HIV-positive individuals require 20–30% more extra energy than HIV-negative individuals of the same age, sex, and physical activity level. 7 Dietary diversity scores (DDs) have been positively correlated with increased mean micronutrient density adequacy of complementary foods and micronutrient adequacy of the diet in adults. 8 Even then, there is complex interaction between dietary diversity/intake, immune function, HIV/AIDS, and malnutrition. 9
In Ethiopia, 9% PLWHIV are severely malnourished and 25% are moderately malnourished.10,11 Assuring adequate access to food in highly active antiretroviral therapy (HAART) treatment programs has been a central demand of PLWHIV in low-income countries, and as a result, nutrition by prescription and therapeutic feeding has been established.12-16
Nutritional problems are among the first negative effects of HIV infection. These problems are due to inadequate diet intake and altered metabolic conditions, provoking impaired balance of energy and nutrients in patients even when they are treated with ART. 3 The effect of poor nutrition in the case of PLWHIV is more serious as they have to grapple with opportunistic infections. Dietary management of PLWHIV is key to sustaining the ability to participate in the workforce and contribute to socioeconomic development. 17 Food insecurity and poor nutritional status may speed up progression of acquired immunodeficiency syndrome (AIDS)related illnesses. 18
The dietary diversity score at the individual level is a proxy indicator of adequate intake of energy and micronutrients. 19 Eating a diversity of foods (varieties of food groups) is an internationally accepted recommendation for a healthy diet, and is associated with positive health outcomes such as reduced incidence of mortality. 20 Dietary diversity is therefore a key concept that should be promoted in managing the nutritional situation of PLWHIV. 15 The relationship between nutrition and HIV infection is very complex and can fluctuate due to factors such as nutritional status, including wasting or weight loss and micronutrient deficiencies; HIV disease stage; other physiological factors; and diets. 21
A number of development partners have participated in the planning and implementation of major initiatives and programs for HIV treatment, prevention, care, and support in Ethiopia and Africa at large. For example, the “3 by 5” initiative was designed to treat 3 million people in 2005. “Getting to Zero” was a theme of the 2015 World AIDS Day commemoration targeted to achieve “Zero Mother to child transmition, Zero discrimination and Zero AIDS-related deaths. “Treat all,” Food by Prescription, appointment spacing model (ASM) care, and HIV continuum care are other strategies that eloquently promote the universal HIV care coverage to ensure that all HIV-positive individuals receive ART irrespective of their CD4 count, World Health Organization (WHO) clinical stage, or viral load.
From the above list, a program directly concerned with nutritional care is the Food by Prescription program that involves nutritional assessment, counseling, and support to decrease nutritional problems in malnourished patients with HIV. However, food insecurity often occurs. The program is challenged by individual, institutional, community, and health systemrelated factors. Scholars criticize this program by saying “symptomatic treatment is very expensive/the cheap intervention is very expensive.”
As far as the authors’ knowledge is concerned, there is no evidence regarding the behavioral
Methods and Materials
Study Area and Period
A hospital-based study was conducted in 5 public hospitals in the Jimma zone (Jimma Medical Center, Shenen Gibe, Agaro, Seka, and Limmu hospitals) from March to May 2018. During the study period, a total of 11 186 adults and 2683 pediatric individuals were on chronic HIV care (from 5 public hospital databases).
Study Population
403 adult (≥ 18 years) PLWHIV were randomly selected and included in the study. However, patients who were too sick (WHO stage/grade IV) and HIV-positive adults with additional chronic non-communicable disease such as diabetes mellitus, hypertension, and current pregnancy were excluded from the study.
Sample Size and Sampling Procedure
The single population proportion formula was used to estimate the study sample size with the assumptions of prevalence of 50%, confidence level of 95%, 5% margin of error, and 5% allowance for non-response rate. The study participants were allocated proportionally based on the number of HAART patients in each hospital, and then, 403 samples were drawn from the total listed patients’ records.
Data Collection Tools and Procedure
Based on their relevance, most of the question items in the tools were adapted from theory of planned behavior (TPB).1,2 The format for the questionnaire consists of seventy five items separated into nine domains. The first domain was to assess PLWHIV knowledge; past experience and economic status on dietary diversity (14 items); the second domain was to ascertain the future and past behavioral inclination of PLWHIV (2 items); the third domain was about behavioral beliefs (6 items); the fourth domain was about outcome evaluation (6 items); the fifth, sixth, seventh, and eighth deal with normative beliefs (9 items), motivation to comply (9 items), control beliefs (4 items), and power of control (4 items), respectively; and the ninth domain was to collect background information (20 items). Finally, data were collected through face-to-face interviews by 5 BSc nurses and supervised by 2 masters of public health. Additionally, an in-depth interview was conducted to explore factors related to inclination toward dietary diversity behavior and to explore the quantitative findings.
The overall aim of the in-depth interview was to investigate exploratory factors affecting behavioral inclination toward dietary diversity of PLWHIV, and to strengthen the capacity for quality and sustainable clinical care of PLWHIV with the new approach to care, ASM. This approach helps reduce direct and indirect costs of clients, reduce stigma and discrimination, and improve satisfaction by 2 visits per year (every 6 month) to answer the following 3 questions. (a) First, to what extent are patients who began HIV treatment after the rollout of ART continuing to engage in ART care? (b) Second, what are the characteristics of patients, and what is the existing support of PLWHIV other than ART? And (c) third, why do people fail to improve their nutritional status; ART care; and the overall livelihood of PLWHIV, like availability of food at home, practice of dietary diversity, and knowledge of dietary diversity, and what is the challenge to using dietary diversity?
In this regard, a mixed methods approach within a specific economic and socio-cultural context was used as an exploration of the predictors for undernutrition among 14 study participants (key informants) from HAART service providers, community advocators, HAART coordinators, and adult PLWHIV, who were purposively selected considering the roles and experiences they had to provide rich and relevant information. Finally, the research team leader further probed the content of the field notes and conducted debriefing sessions.
Data Processing and Analysis
Data were coded and entered to EpiData version 3.14 and then exported to SPSS version 20.0 for analysis. Independent variables with P ≤ .25 at the bivariate analysis level were entered into multiple linear regressions to control potential confounders. Finally, variables, which have P ≤ .05 within respective confidence intervals at multiple linear regression analysis, were considered to be independent predictors of dietary diversity behavior of PLWHIV. The relationship and steps of data analysis are indicated in the conceptual framework given in Figure 1. The conceptual framework of the study, adapted from the theory of planned behavior, Ajzen
1
1991.
Results
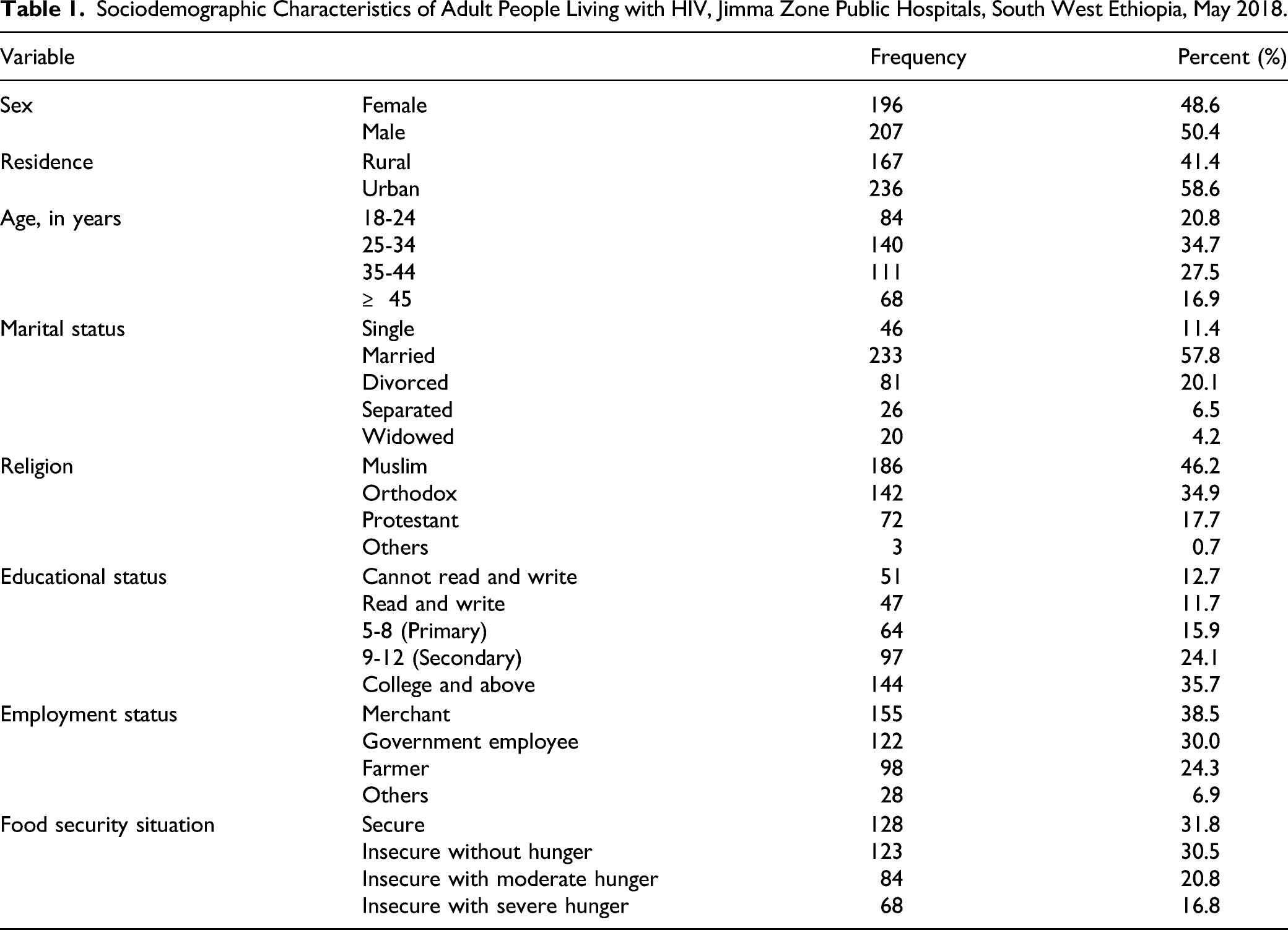
A total of 403 adult PLWHIV, of which 196 (48.6%) were females, participated in this study. The mean age of the study participants was 29.5 (±8.4) years. Concerning marital status, 233 (57.8%), 81 (20.1%), and 46 (11.4%) were married, divorced, and single, respectively. More than half, 236 (58.6%), of the study participants were urban residents.
Sociodemographic Characteristics of Adult People Living with HIV, Jimma Zone Public Hospitals, South West Ethiopia, May 2018.

Graphic abstracts.
Intention of Adult PLWHIV Toward Dietary Diversity Behavior
Perceived Risk of Undernutrition, Perceived Risk of Severe Clinical Outcome, and Intention of Dietary Diversity Behavior of PLWHIV in Jimma Zone, Ethiopia, May 2018.

Overall Descriptive Findings of Behavioral Intention of PLWHIV Toward Dietary Diversity
Overall Descriptive Findings of TPB Constructs of Adult PLWHIV on HAART in Jimma Zone Public Hospitals, May 2018.
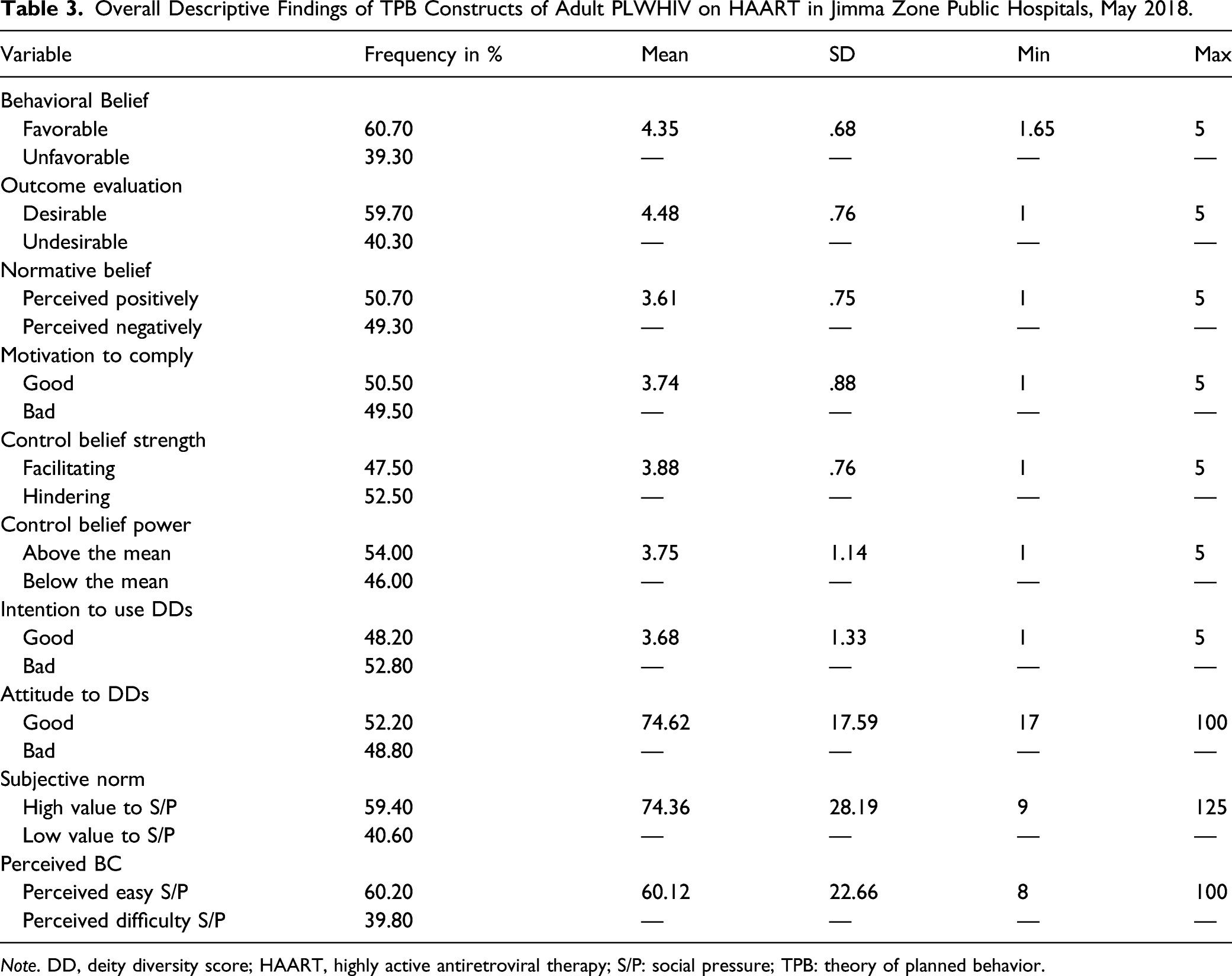
Note. DD, deity diversity score; HAART, highly active antiretroviral therapy; S/P: social pressure; TPB: theory of planned behavior.
Correlation of Dietary Diversity Behavioral Intention to TPB Constructs
Among the constructs, the subjective norm showed the highest correlation (r = .42, P < .001), followed by perceived behavioral control (r = .39, P < .001) and attitude (r = .38, P < .001).
Correlation of the Indirect and Direct Measures of Theory of Planned Behavior Among Adult PLWHIV, Jimma Zone Public Hospitals, 2018.

Note. Correlation is significant at ++ P < .001, +P < .05; DATT: direct attitude; DPBC: direct perceived behavioral control; DSN: direct subjective norm; IATT: indirect attitude; IPBC: indirect perceived behavioral control; ISN: indirect subjective norm; PBC: perceived behavioral control.
Predictors of Intention Toward Use of Dietary Diversity
Statistically significant predictors of intention to use dietary diversity were found to be attitude (β = .196, P < .01), subjective norm (β = .390, P < .01), PBC (β = .048, P = .001), and motivation to comply (β = .03, P < .01). This indicates that for a unit positive change in the individual’s perception about any counseling support from health professionals to use diversified food in their usual feeding as normative action will increase the intention to use dietary diversity by .39, provided that the other conditions and medical cares are in place.
Distal, Intermediate, and Proximal Constructs of TPB Among Adult PLWHIV With Intention to Use Dietary Diversity in Jimma Zone Public Hospitals, May, 2018.

PBC: perceived behavioral comply.
In-Depth Interview Findings
Most common challenge to dietary diversity was explored, and the findings were presented in 5 themes. These are household food security, health system, income opportunity, individual behavior, and support-related hindering factors.
Lack of Food at Home
Lack of food at home is one of the problems of adult PLWHIV on ART follow-up. It was found to be critical according to the quantitative findings. Most of the in-depth interviewees emotionally mentioned the problem of availability and access to food at home. A female participant explained the condition by saying: “Let alone living with the disease and the limited capacity we have now, it is difficult to survive in Ethiopia even for a bachelor graduate who has regular monthly salary. Life for PLWHIV is getting very difficult.”
Another healthcare provider for PLWHIV participant said that “all PLWHIV have a demand to eat four to six times a day. The drug needs that much. But in most of the cases, they couldn’t even afford to eat two to three times a day. Sometimes, I feel shame when I hear such sound of PLWHIV.”
Problem of the Health System
The study participants also suggested that the health system design routine behavioral change initiatives as strategies to encourage dietary diversity at home for all PLWHIV, rather than designing a treatment protocol for undernutrition. In addition to the issue of individual behavioral change, creating income opportunities for PLWHIV on HAART as a strategy to sustainably reduce malnutrition and improve quality of life was mentioned.
A male participant said that “taking HAART can effectively prevent suffering and death. However, to sustain this promising outcome longer and to start thinking more about our health, we need to have healthy diet differently from people free of HIV. In addition, when they have behavioral change and have their own job, they can support their own life and even they can bring impact on the primary prevention program of HIV in the country.”
Income-Generation Opportunity
Majority of the discussants repeatedly reported that they went days without food to eat but they did not miss doses of their HAART, for they said it was their life. A male discussant said that “The issue of HAART is serious. You can argue about food after taking your pills but you can’t say anything about any issue by discontinuing your pills because this is a life issue. Sometimes you need to take the pills without food if conditions didn’t allow you to access food.”
One female participant quoted that “The difference in the effectiveness of the treatment is a matter of access to the food you want at the time and amount you need. I even believe the disease could be eliminated from the face of the world if PLWHIV on HRART could access the required food needed for the drug from government or non-governmental stakeholders.”
Individual Behavior
The participants also reflected that HAART improved their general health status; decreased frequency of infections; improved appetite; and enhanced sense of wellbeing, self-esteem, hope to live indefinitely, and weight gain; and increased CD4 count, but they did not know the importance of dietary diversity at home. A servant in the health institution said that 30% weight gain, 43% increase in CD4 count, 29% improvement in BMI, and 27% reduced OI were detected in the last 2 years/before data collection time from the individuals who show positive behavior on dietary diversity, meaning they tried their best to eat diversified food at home and it was documented.
A female participant is quoted that “When PLWHIV started the treatment their CD4 count was only 1 per micro liter. Now, it is more than 600 per micro liter. Their weight was also 40 kg and now their weigh is 60 kg. But this improvement is not merely due to HAART rather it is the combined effect of HAART and diversified food eating at home. It is also due to the psychological stability, pleasure and care they are getting from health professionals who are taking care of us in the hospital.” Almost all discussants perceived that lack of food with HAART will impact the level of benefits PLWHIV would gain from the treatment if the level of behavioral change toward dietary diversity is not assured.
Absence of Food Aid/Support
The discussants from the in-depth interviews agreed that lack of food/absence of food at home is an issue that is overlooked by the program and a challenge to the successful implementation of the Food by Prescription program for PLWHIV in the stage of undernutrition.
On the other hand, the discussants mentioned that PLWHIV continue to depend on the food aid and Food by Prescription program without behavioral change; consequently, they may withdraw from their treatment due to lack of food and become hopeless/negligent. This, in turn, may lead to a new strain of the virus which is resistant to the drug; if this appears in the country or in the community, it would mean failure of the whole program.
Discussions
The components of TPB help explain determinants for a certain behavior to be endorsed or avoided by clients in their usual feeding habit. In addition, the theory explains that intention to practice a preferred behavior is a function of favorable attitudes toward that behavior without any pressure to perform, and patients believe that the health practice is crucial to their life and perceived behavioral control.
The study revealed that more than 50% of respondents in each construct have had desirable beliefs (control of their beliefs in terms of the intention for using dietary diversity in their home) while all the comprehensive HAART cares are in place. The fact that the TPB explained more than a quarter of the intention of using dietary diversity is in line with the study conducted in Dilla, Ethiopia, and South Africa,22,23 where 35% variation in the intention for use of healthy diet was explained.
Similarly, a study conducted in Burkina and Tanzania24,25 explained 30% and 31% variation in the inclination toward dietary diversity use; the social cognitive aspects explained 27%, 26%, and 29% variation in Mozambique, Addis Ababa, and Kenya,26-28 where the theory explained about two-thirds of the variance in inclination toward diversified feeding at home. On the other hand, this is lower than the findings of studies done in Uganda and Malawi where 58.8% and 59% of the study participants had low dietary diversity, respectively.29,30 This shows that HIV-positive adults in the present study area had inadequate dietary intake compared to those in the previous studies, with dietary diversity, that is, standards/the number of foods consumed across time and within food groups over a reference period, widely recognized as a key indicator of nutrient adequacy.31,36
Each of the model’s constructs was positively correlated with the inclination toward using dietary diversity, and this is consistent with the results of other studies done in Addis Ababa and other African countries to predict intention to use HAART comprehensive services.37-39 From the constructs of the TPB model, the subjective norm was the first strong positively correlated variable, followed by attitude. This suggests that each variable explained the variation in intention of dietary diversity use.
Absence of food aid and duration of antiretroviral treatment was significantly associated with dietary diversity. It was noticed that HIV-positive adults who were on ART for less than 2 years and 2–3 years were more likely to have low dietary diversity, which exacerbates the weight loss and nutritional problems experienced by PLWHIV. It is known that the drug without adequate food and antiretroviral side effects, such as nausea, taste changes, and loss of appetite, may reduce food consumption, while inadequate food and side effects such as diarrhea and vomiting may increase nutrient losses. 40 From this point of view, the findings of this study can help identify the variables of focus in intervention programs intended to bring about the desired healthy feeding and reduction of malnutrition. This has significant impact and warrants counseling on the practice of dietary diversity as part of comprehensive HAART intervention programs. Both PBC and subjective norm explained 25.9% of the variance in the inclination toward dietary diversity, which is less than the findings of a study done in Kenya 41 on healthy diet behavior of PLWHIV. Studies revealed that subjective norm and perceived behavioral control (PBC) are pertinent predictors of intention to increase dietary diversity practice at home. As a result, a variety of nutrients are obtained and thus nutrient adequacy is attained.42-44
Nutrition interventions that support, educate, and create income-generation opportunity for low-income PLWHIV are very critical because healthy eating should be embraced. Changes at policy level should be well thought-out to increase affordability and accessibility of healthy food in low-income settings. 45 This difference could be because of the personal and cultural differences and the low contribution of behavioral intention observed in the present study.
Ajzen also argues the magnitude of the PBC–intention relationship is dependent upon the type of behavior and nature of the situation. The highest predictor of inclination toward dietary diversity was subjective norm followed by attitude. This finding corresponds with studies conducted in 21,22, Metema, and Hawassa.19,46,47 This might be due to similarity in terms of source of social pressures and underlying normative beliefs. In addition, salient belief measures the nature of TPB, which is local and culture sensitive; it might have contributed to the instances of the findings.
Conclusions
From this study, it was understood that PLWHIV’s inclination toward dietary diversity was low which explained 32.2% of variation in intention to use dietary diversity among adult PLWHIV. The predictors of behavioral inclination toward dietary diversity were direct and indirect attitude, direct and indirect subjective norm, and direct and indirect perceived behavioral control. Additionally, the study documented that the intermediate variables and proximal variables of TPB explained the nearly equal variance, suggesting both variables are equally important and should be taken into account in the behavioral change interventions. Therefore, intention can be used to extend theories and to design interventions, which can increase the ability of those programs to change behavior rather than only treat malnutrition of the PLWHIV. The paradigm model (Theory of planed behavior) is supportive and can be suggested for application to any nutritional program considered to prevent undernutrition, reduce HAART care resistance, and improve quality of life through nutritional education focused on subjective norm, attitude, and social norms and perceived behavioral control, other than the Food by Prescription program which is focused on symptomatic treatment. This study recommends a further longitudinal or interventional study which covers more area and factors of behavioral change compared with HIV-positive patients who have favorable inclination toward dietary diversity.
Strength
Quantitative data was supported by qualitative data. The instrument was developed according to standard guidelines and relevant literatures, and an elicitation study was conducted to identify the salient beliefs of intention to apply the theory to the local context.
Limitation
This study did not account for the actual behavior that was predicted based on the TPB constructs, which may show how much behavioral intention could be transformed into the actual behavior. The TPB is purely psychosocial and lack of similar local literatures may affect the scope of the study. In addition, there might be a possibility for bias to emerge in systematic sampling, since the samples were selected randomly and the researcher used his own discretion.
Implication
It is worthwhile to investigate behavioral intention as a potential determinant of the clinical outcomes for sustainable HIV care. The paradigm model is supportive and can be suggested for application to any behavioral change program considered to prevent under-nutrition and improve quality of life through education focused on subjective norm, attitude, and social norms, other than the Food by Prescription program which is focused on symptomatic treatment.
Footnotes
Acknowledgments
Study participants are greatly acknowledged for the information they provided. Research assistants are also appreciated for collecting, supervising, and encoding the data. Jimma University is highly acknowledged for covering the cost of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Jimma University, Institute Health. The views presented in the article are solely of the author and do not necessarily express the views of the funding organization.
Ethical Approval and Informed Consent
This study was approved by the institutional review board of the Institute of Health Jimma University, Ethiopia (Ref. No. IHRPGC/1095/2017). All participants provided written informed consent prior to enrollment into the study, and data were explained in an aggregated way to maintain confidentiality throughout the data analysis and manuscript preparation.
Consent for Publication
Not applicable.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
AIDS: acquired immunodeficiency syndrome, ART: antiretroviral therapy, BB: behavioral belief EBB: evaluation of behavioral belief CI: confidence intervals, DD: diet diversity score, HAART: highly active antiretroviral therapy, HIV: human immunodeficiency virus, PLWHIV: people living with HIV, PBC: perceived behavioral control, SN: subjective norm, TPB: theory of planned behavior.