
Abstract
Early detection of cervical cancer through screening practice in developing countries is still low. The study is aimed to determine cervical cancer screening practice and associated factors among women of age 25 to 59 years old. Community-based study design was employed and systematic sampling was used to get 458 samples. The data were entered into Epi info version 7.2.1.0 and exported to SPSS version 20 for cleaning and analysis. Binary and Multivariable Logistic regression was used and adjusted odds ratio with 95% CI at P-value <.05 was reported as significant value. Cervical screening practice among the study participants was 15.5%. Women’s age 40 to 49 (AOR = 2.95, 95% CI = 0.94, 9.28), educational status (AOR = 4.19, 95% CI = 1.31, 13.37), employed women (AOR = 2.59, 95% CI = 1.01, 6.68), parity above 4 (AOR = 3.09, CI = 1.03, 9.31), sexual partners 2 to 3 (AOR = 5.32, CI = 2.33, 12.14), good knowledge about cervical cancer (AOR = 3.88; 95% CI = 1.83, 8.23) and positive attitude toward cervical cancer (AOR = 5.92, CI = 2.53, 13.87) were independently associated with cervical cancer screening practices. The study revealed that the utilization of cervical cancer screening was very low. Educational status, Women’s age, number of sexual partners, knowledge, and attitude were significantly associated with cervical cancer screening practice. Therefore, intervention programs intended at improving cervical cancer screening practice among women should focus on the significant factors.
Cervical cancer screening among women is poor.
It helps as input for stake holders working there
It gives direction for health care workers as they have to go to the community and address this gap.
Introduction
Cervical cancer is one of the many cancer types that adversely affect reproductive age group. It is referred to as “hidden or silent” cancer because most patients have no symptoms and their diagnosis occurs incidentally. 1
In the world, cervical cancer accounts for 9% of all female cancer cases, 2 with an estimated 500 000 new cases in 2018—more than 3-quarters of which occur in less developed nations.1,3 The estimate of global cervical cancer prevalence is 13.1%, and is most prevalent in Africa (27.6%), South-Eastern Asia 17.2%, and Central and Eastern Europe (16.0%).4,5
Cervical cancer was indeed the second most commonly diagnosed cancer in African women in 2018 (119, 284 new cases), with the highest number of cases in Sub-Saharan Africa, wherein Swaziland had the highest rate followed by Malawi in which their Age-standardized incidence rates were 75.3 and 72.9 per 100 000 women respectively. 6
Current estimates indicate that Ethiopia has nearly 26 million female populations greater than 15 years who are at risk for developing cervical cancer. 7 Cervical cancer is the second leading cause of death among all cancer patients in Ethiopia 8 and incidence was estimated to be 35.9 new cases per 100 000 women annually while the age-standardized incidence rate from cervical cancer in Ethiopia was 18.9/100 000 in 2018.5,8 These figures are probably lower than the actual number of cases, due to the low level of awareness, cost, limited access to screening services and other factors (like distance, poor attitude, and perceptions). 9
Early detection through screening and treatment of Precancerous Cervical Cancer Lesion (PCCL) remains the best possible protection against cervical cancer which can prevent 75% of cases in developing countries, if women start cervical cancer screening at the age of 21 at least once every 3 to 5 years interval. 10
Unfortunately, in Ethiopia, only 1% of age-eligible women receive effective screening for cervical cancer and 90% of women have never had a pelvic examination at all. 9 Low screening coverage in our country causes most patients to present to the hospital with advanced disease. 11 Cervical screening practice is the effective recommended method for the prevention and early detection of cervical cancer. However, cervical cancer screening coverage among childbearing age women is still far from the significant goal set by Federal Ministry of Health (FMOH) across the country.
Barriers to the uptake of screening in LMICs include a low level of awareness, cost, limited access to screening services, poor infrastructure, lack of trained and skilled professionals, poor knowledge, and illiteracy.9,12-16
The national cancer control program in Ethiopia has a strategy to lower cancer burden through primary prevention, lifestyle modification, screening, and early detection to target 80% screening coverage. This strategy is included in the Ethiopian Health Sector Transformational Plan (HSTP). Despite the effort of the government and other stake holders, the cervical cancer screening practice still low. Though different studies conducted concerning cervical cancer screening, several other factors hinder women from attaining those services. For example, a woman may have a cervical cancer screening facility available in her locality; however this does not guarantee the uptake of the facility for better health because of cultural and norm related issues. Therefore, this study aims to assess cervical cancer screening practices and associated factors among women in South Ethiopia.
Materials and Methods
Study Design
Community-based cross-sectional study design was employed.
Population
Randomly selected women ages of 25 to 59 years were included in the study.
Sample Size Determination
The sample size for the first objective (prevalence of cervical cancer) was calculated based on single population proportion formula as follow.

Where:



Then, considering 10% Non-Response Rate (NRR)


The sample size for the second objective (for factors associated to cervical cancer) was calculated using Epi info statistical calculator for unmatched case-control with the ratio of 1:1 for exposed to unexposed by considering some variables that have a significant association in a study conducted by Mettu Karle Hospital 17 and presented as follow in the table below (Table 1).
Sample Size Determination for Cervical Cancer Screening Practice.

Note. *sexually transmitted infections.
Since the larger sample size from associated variables is presence of Sexually Transmitted Infections (STI), thus the total sample size for the second objective considering non-response rate was,

Thus, the sample size for the first objective was smaller than the second objective; therefore, the largest sample size for the second objective (
Inclusion and Exclusion Criteria
All women in age group of 25 to 59 years old who were available at the time of data collection were included. Severely acute sick looking women were excluded from the study.
Sampling Procedure
Samples were selected from each kebele independently after proportional allocation of the sample was done using formulas. Systematic random sampling technique was used to employ the study participants according to the computed kth value. The spinning pen technique was applied at the center of each kebele to decide the direction and to pick the first household. The lottery system was considered to select 1 woman whenever 2 or more women exist in the selected household. If the candidate were not available during the data collection, waiting for her was considered as an option not to miss her information.
Proportional allocation of sample size to each Keble,

Where: n
Nj = is population size of the kth unit
n = n1+ n2+n3+n4 +. . . is the total sample size (
N = N1+N2+N3+N4+. . . is total population size (
Proportional allocation of sample among Keble’s in Negelle Borena Town (Figure 1).
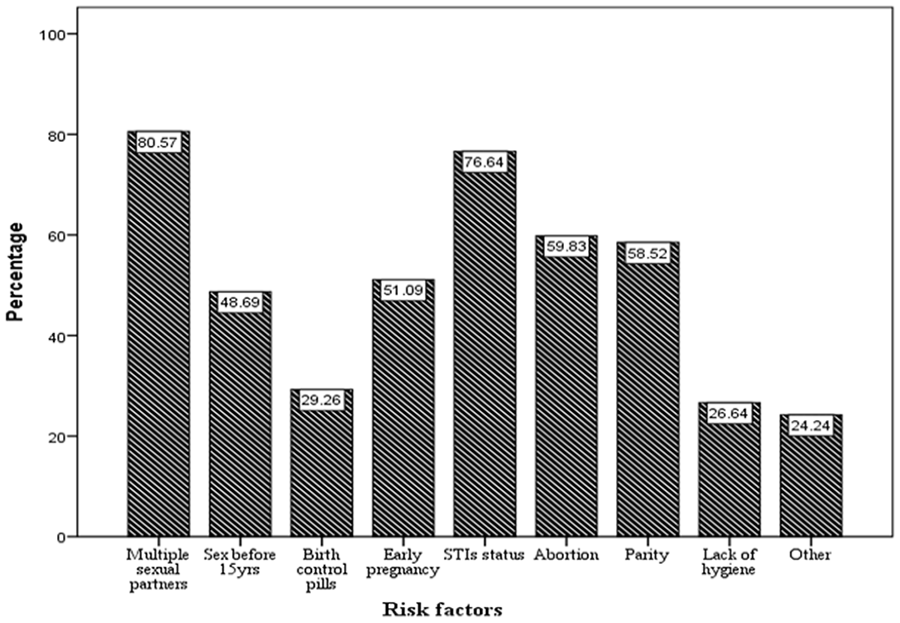
Risk factors identified for cervical cancer among women age 25 to 59 years old at Negelle Borena Town, Oromia, Ethiopia.
Dependent Variables
Cervical cancer screening practice
Independent Variables
Socio-demographic factors: Age, Income, Marital Status, and Educational status.
Personal factor: Multiple sexual partners, Early initiation of sex, Multiparty, Contraceptive use, Fear of screening, and Smoking.
Knowledge toward cervical
Attitude toward cervical
Operational Definition
● In general 26 different questions regarding cervical cancer and screening, risk factors, and prevention methods were forwarded, scored, and then pulled together. ● The cumulative mean score is knowledge of participants about cervical cancer and cervical cancer was assessed using the mean score. Based on this, those who had scored ● Less than the mean value were reflected to have ● Greater than or equal to the mean value were considered as having
● In general, the overall attitude of the respondents toward cervical cancer and screening was assessed using a ● ●
● Ever screened within the past 5 years were regarded as ● Never screened were regarded as having
Data Collection Procedures (Instruments, Personnel, and Measurements)
Data were obtained from a primary source directly from the study unity in the study population. Data were generated by using structured interview forms, which were adopted from similar studies 17 on the identified scales of the study. Data collectors were nominated from health science college instructors and health center staff having a minimum of the first degree and preferably a female professional who were having a similar experience with other studies.
Data Quality Assurance
A pre-test was conducted on 5% (24 of samples) in Bule Hora town before actual data collection. Based the pretest some amendments were done to maintain the reliability of the data. Cronbach alpha was calculated and it was .76. Data collectors were also trained and allowed to practice during the pretest and they were supervised especially at the earlier stage to extract possible factors affecting the actual data quality. The data collection process was thoroughly supervised, and the completeness of all questionnaires was checked by the investigators and the supervisors on daily basis.
Data Analysis
Afterward the data collection, questionnaire was checked for completeness and consistency. The data were entered in the prepared template into Epi info version 7.2.1.0. Then data were transferred to SPSS version 20 for clearing and analysis. Descriptive analysis was employed to describe the percentages and distributions of the respondents for the independent variables. Binary Logistic regression was used and all independent variables which fulfilled the minimum requirement (P < .25 on the bivariate analysis) were entered into multivariate analysis. Hosmer and Lemeshow Goodness of Fit test was used to assess the fitness of the model during multivariate analysis, at P > .05. Multivariable logistic regression analysis was performed by means of the backward stepwise approach and then variables with P > .05 were removed from the adjusted analysis. Adjusted odds ratio with a 95% confidence interval and P-value of less than .05 were used to identify factors associated with the utilization of cervical cancer screening.
Result
Socio-Demographic Characteristics
A total of 458 clients participated in the study giving a response rate of 98.07% and 258 (56.3%) respondents were between the age of 35 and 39 years, where a median age of 35 (IQR = 9). The study revealed that 203 (44.3%) participants were Muslim, 271(59.2%) were Oromo, 317 (69.2%) were married, and 147 (31.7%) belonged to high school education (Table 2).
Sociodemographic Characteristics Among Women Age 25 to 59 Years Old in South Ethiopia.

Reproductive Health and Lifestyle Characteristics Participants
Among the study’s participants, 396 (86.5%) had only 1 sexual partner, while 413 (90.2%) had begun having sex after turning 18 years old. Regarding the use of contraceptives, 283 (61.8%) had a history of using modern contraceptives and the majority of participants 190 (41.5%) were using injectable contraceptives followed by 115 (25.1%) of oral contraceptive users (Table 3).
Reproductive Characteristics Among Women Age 25 to 59 Years Old in South Ethiopia.

Knowledge of Respondents Regarding Cervical Cancer and Cervical Cancer Screening
The mean score was 16.33 with a minimum value of 4.00 and a maximum value of 26.00. Based on this those who scored above 16.33 mean value were considered as having good knowledge. Generally, in this study 255 (55.0%) participants with 95% CI (40.4, 49.6) were had good knowledge on cervical cancer screening practice and out of the 61 (84.1%) were respondents who had undergone screening services.
In this study, having multiple sexual partner was the greatest risk factors for cervical cancer (Figure 1).
With regards to source of information 394 (86%) respondents were at least heard information about cervical cancer with 346 (75.5%) participants were heard from radio/TV, the number of respondents who mentioned at least 1 symptom of cervical cancer were 285 (62.2%) as shown in Table 4.
Selected Knowledge Characteristics Among Women Age 25 to 59 Years Old at South Ethiopia.

Attitude of the Respondents Toward Cervical Cancer and Cervical Cancer Screening
The overall attitude of the respondents toward cervical cancer and screening was assessed using Likert scale with 10 different questions having 5 multiple responses for each question which is also scored and computed pulled together, and then the mean was calculated. Respondents with a score above the mean value were considered as having a positive attitude. The mean score was 7.03 with a minimum value of 0.00 and a maximum value of 10.00. Based on this those who scored above the 7.03 mean value were considered as having a positive attitude.
Among the total participants, only 155 (33.8%) neither agree nor disagree that carcinoma of the cervix is to be a problem in our country, 247 (53.9%) and 241 (52.6%) participants agreed that cervical cancer a preventable disease and can be cured respectively. Whereas 228 (49.8%) agreed that cervical cancer screening can prevent cervical cancer and Only 200 (43.7%) of the respondents agreed that screening is effective in detecting cervical cancer.
Overall, in this study 214 (46.7%) with CI (42.4, 51.7) participants have had a positive attitude toward cervical cancer screening practice, and out of the 66 (91.7%) were respondents who had a history of cervical cancer screening practice.
Cervical Cancer Screening Practice and Its Barriers
As per this study 386 (84.3%) participants with 95% CI = 81.0, 87.3 were not intended to accept and practice cervical cancer screening practice. Whereas 72 (15.7%) participants with 95% CI = 12.7, 19.0 were accepted and practiced cervical cancer screening and among those who screened 61(84.7%) were screened within the past 5 years. The most common reason by those who screened was self-initiated 50 (10.9%) whereas 306 (66.8%) participants mention feeling healthy as a reason for not be screened and 284 (62.0%) were had a plan to be screened for cervical cancer as shown in Table 5.
Cervical Cancer Screening Practice Among Women Age 25 to 59 years Old at South Ethiopia.

Factors Associated With Cervical Cancer Screening Practice
The effects of different independent variables were tested for utilization of cervical cancer screening practice using binary logistic regression analysis. Among the variable age, marital status, parity, educational status, oral contraceptive use, fear of the pain of screening, multiple sexual partners, employment status, knowledge and attitude toward screening, age at first sexual intercourse, lack of health education on cervical cancer, and limited information on cervical cancer were found to be associated on bivariate analysis.
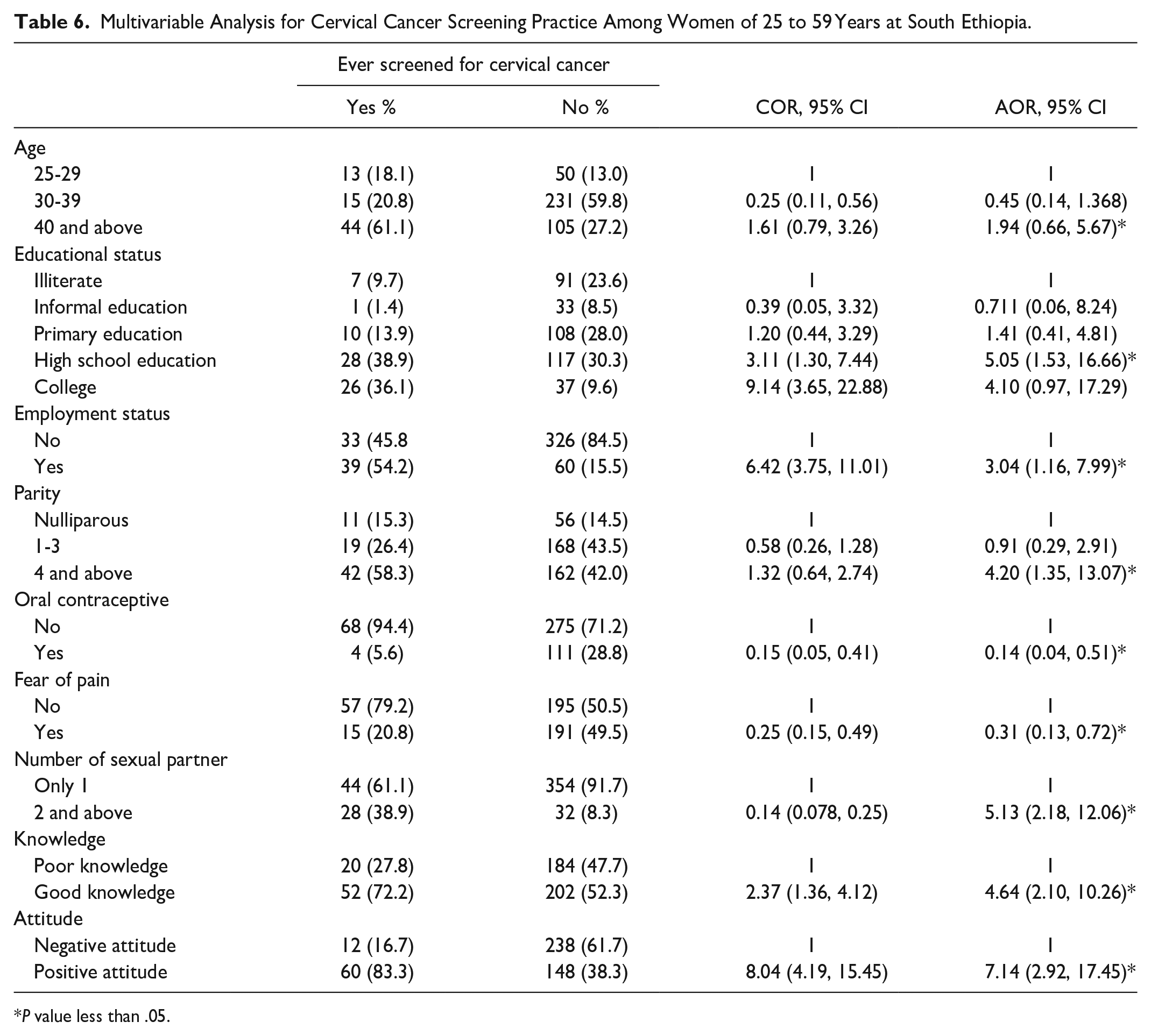
Finally, all independent variables which fulfilled the minimum requirement for bivariate analysis (P < .25) were entered into multivariable logistic regression. Using the backward stepwise approach outlined in the methods section, variables with P-values >.05 were removed from the adjusted analysis. Among the variables age, knowledge, oral contraceptive use, educational status, parity, the pain of the procedure, fear of the pain of screening, number of sexual partners, attitude, and employment were independently and significantly associated with cervical cancer screening practice. The odds of practicing cervical screening is 1.94 times (AOR = 1.94, 95% CI = 0.66, 5.67) higher among women age 40 to 49 years compared to those women of age 25 to 29 years. The odds of practicing cervical cancer screening is 4.64 times (AOR = 4.64; 95% CI = 2.10, 10.26) higher among participants with good knowledge compared to those women with poor knowledge. The odd of practicing cervical cancer screening was 7.14 times (AOR = 7.14, CI = 2.92, 17.45) higher for those with positive attitudes than those with negative attitudes. The odds of practicing cervical cancer screening is 5.05 times (AOR = 5.05, 95% CI = 1.53, 16.66) higher among participants with high school education compared to their counterparts. The odds of practicing cervical cancer screening is 4.20 times (AOR = 4.20, CI = 1.35, 13.07) higher among participants with 4 and above birth compared to nulliparous women. The odds of practicing cervical cancer screening is 0.14 times (AOR = 0.14, CI = 0.04, 0.51) higher among participants who use oral contraceptives compared to the non-users. The odds of practicing cervical cancer screening is 3.04 times (AOR = 3.04, 95% CI = 1.16, 7.99) higher among participants who are employed compared to the non-employed. The odd of practicing cervical cancer screening among respondents with 2 to 3 sexual partners were 5.13 (2.18, 12.06) times (AOR = 5.13, CI = 2.18, 12.06) higher than those with a single sexual partner. The odds of practicing cervical cancer screening is 0.31 times (AOR = 0.31, 95% CI = 0.13, 0.72) higher among participants who had fear of pain from procedure compared to those who do not fear the procedure as shown in Table 6.
Multivariable Analysis for Cervical Cancer Screening Practice Among Women of 25 to 59 Years at South Ethiopia.
P value less than .05.
Discussion
Only 72 (15.7%) participants in this study involved in cervical cancer screening, which is a relatively low rate compared to the Federal Ministry of Health’s National cervical cancer preventive strategy goals (80%).13,20 The inconsistency of the result may be due to the cervical cancer screening program initiated in recent times in the study area. Despite the probable justification given the current outcome is much better than the result from a population-based WHO steps study in Ethiopia, 2017 where the screening rate prevalence was 2.9%. 21 The possible explanation might be attributed to the difference in the sample size, study design, and study population. This result is in line with studies done in Nepal (18.3%), Dare Salaam, Tanzania (21%), and Jimma town (15.5%).12,20,22-24 The participants in the study were urban women with access to media and other sources of information, which could account for the similarity. If women have information concerning cervical cancer severity, they may utilize screening services. However, this finding was lower than the study conducted in Thailand (65.9%), Jamaica (66%), and Kenya (39%). The possible explanation for the observed discrepancy might be due to accessibility of the service, having many methods of pre-cervical cancer screening and availability of more trained health providers, and differences in the health status of the study population in the previous study area. It may also be due to differences in socio-demographic characteristics such as the level of education of the study participants in the countries, the difference in sample size, the difference in the study area, and the method of the study used.
According to the current study, the main reason for not taking cervical cancer screening services was fear of screening related to pain. Almost 44.97% of respondents who had fear of pain were 65% less likely to undergo cervical cancer screening compared to those without fear of pain. This is comparable with a similar study conducted in low and middle-income countries in 2015 where fear as reason for refusing to be screened was mentioned by 51% of participants. 25 However, the current finding is much higher than the study done in Cameroon and Burkina Faso reveals 4.35% and 3.4% of participants were thought that the procedure could be painful.18,26 The probable explanation for the discrepancy might be ascribed to the difference in the educational background, socioeconomic status, level of awareness and attitude of the study population, and accessibility of the service. Furthermore, a study done among commercial sex workers in Northwest Ethiopia in 2019 shows that the primary reasons in 19.65% of the respondent for never having cervical cancer screening were fear of the test result. 27 The difference might be attributed to the difference in the study population.
This study showed that, women’s age was one of the significant factors for the utilization of cervical cancer screening. Women’s ages between 40 and 49 years were 1.94 times more likely to utilize cervical cancer screening as compared to women in their age of 25 to 29 years. This finding was supported by the study done in Peru in 2018 states that the age group of women between 40 and 49 years old having a stronger association when compared to the age group 20 to 29 years. 28 Similarly, this finding is in line with a study done among Health Workers in Low Resource Setting in Africa in 2019 reveals that being 40 years had 1.18 times increased chances of being screened. 29 Moreover, the current study finding is similar to the study done at Mettu, Ethiopia, and Debremarkos town in 2019 where age between 40 and 49 years was had a strong association with cervical screening behavior compared to those aged between 21 and 29 years.17,30 This could be explained by the fact that as women gets older; their tendency to seek out health care may also increase. The other possible explanation is that when women get older, the risk increases and they visit medical institutions more frequently.
Educational status was also the main significant factor for the utilization of cervical cancer screening. Those participants with High School education were 5.05 times more likely to have cervical cancer screening practice compared to their counterparts. This finding is in line with a study from Hong Kong, China 2016 where women with a higher educational level (post-secondary) were more likely to have had the test compared to their counterparts (primary or below). 31 Moreover finding from the current study is also comparable with finding from study done in Burkina Faso 2016, Finote Selam town 2018, Shabadino District 2019, and age-eligible women in Ethiopia 2020 where a higher level of education were significant predictors of cervical cancer screening.25,32-34 The probable explanation might be women with higher education had higher levels of knowledge about cervical cancer and were much more willing to go for cervical cancer screening practice than those who had less education.
As observed from the study, participants who were employed were 3.04 times more likely to be screened than unemployed. This finding is in line with a study from Japan in 2018 where respondents who were working full time were 4 times more likely to have screening than those who were unemployed. 35 Likewise, the current finding has consistency with a study from Burkina Faso in which cervical cancer screening was 2 times more prevalent among employed women compared to their counterparts. 36 Moreover, similar findings were observed in the study done in Bishoftu town, and southwest Ethiopia where the odds of having cervical cancer screening were about 6 and 3 times higher among government employees than those who were unemployed.22,36 This could possibly be explained by the fact that employed women have a source of cash, allowing them to prioritize their health problems.
Findings from this study also show that participants who gave 4 and above birth were 4.20 times more likely to practice cervical cancer screening than those nulliparous women. This finding is in line with a study from Turkey and Peru in 2018 where the frequency of undergoing Pap smear testing at least once in a lifetime was 1 times higher among multiparous women than nulliparous women.28,37 Likewise, the current finding is comparable with the study finding from Dares Salaam, Tanzania, 12 and Tigray region 2019 and Dabat District 2020 38 where multiparous women were 3 times more likely to utilize the service than the nulliparous women. 39 The probable explanation for the similarity might be since previous pregnancies of a woman may expose her to receive health education many times compared to those with no previous pregnancies.
The number of sexual partners was also one of the significant predictors for the utilization of cervical cancer screening. The odd of practicing cervical cancer screening in the current study among respondents with 2 to 3 sexual partners were 5.13 times higher than those with single sexual partner. This study is in line with studies done by Japanese, Dar es Salaam, Tanzania, Mekele North Ethiopia, and Addis Ababa, Ethiopia, where respondents with greater than 5 sexual partners during their lifetime were 2 times more likely to have undergone the screening than those with only 1 sex partner.9,12,35,40 This is comparable to the finding from Mettu Ethiopia having a history of multiple sexual partners found to have 3 times association for cervical cancer screening compared to those with 1 sexual partner. 17 The possible explanation may be increased lifetime sexual partners might also increase the chance of being diseased with STI and STD with its signs and symptoms which lead to visit health facilities.
As per this study, the odd of practicing cervical cancer screening among participants who were using oral contraceptives were 0.14 greater than the non-user. This finding is in line with the study done in France where the overdue rate for Pap smear tests was 2 times higher among those using contraceptives than those with an IUCD. 41 The current study finding is also comparable with findings from Mettu, southwest, Ethiopia, where the participants who were using contraceptives had odds of 0.206 times cervical cancer screening than those who did not use contraceptives.
Women’s knowledge about cervical cancer screening was another significant factor in the utilization of cervical cancer screening services. Knowledge generally does not necessarily interpret to practice in numerous cases as has been perceived on certain occasions. For instance, despite the better awareness observed about cervical cancer prevention in the study conducted in Legos, Nigeria, preventive practices were low in which of all knowledgeable about cervical cancer only 18.5% had undergone a Pap smear test. 42 This is comparable to the present study results where among participant cervical cancers who had good knowledge about cervical cancer and screening only 16.9% were undergone cervical cancer screening. This is in line with finding from a study in Arba Minch Town, Mekelle, and Jimma town were having good knowledge of cervical cancer screening were independently associated with cervical cancer screening.9,22,43 This might be explained by increases the level of women’s knowledge about the benefits of screening directly lead the women to utilize cervical cancer screening.
In general, in the current study, 46.7% of participants were those who score below the mean value and consider as having a negative attitude toward cervical cancer and screening. Despite the low positive attitude in the current study, the odd of practicing cervical cancer screening were 6 times higher among those with positive attitudes than those with a negative attitude. This finding is supported by a study from Nigeria where 47% of the respondents mention dislike of pelvic examinations main reason for not screening. 44 This is in line with the study from Hawassa (55.3%), Finote-Selam-town (58.1%) where respondents who scored mean and above the mean had a positive attitude toward cervical cancer screening.39,45,46 The probable explanation might be women who have a favorable attitude toward cervical cancer screening will have self-initiative to know about cervical cancer risk factors and the benefits of its screening.
Despite this study has revealed significant finding regarding cervical cancer screening, it is not free from limitation. One of its limitation is being cross-sectional design which is a snapshot at 1 time and cannot show cause effect relationship. Recall bias might be another limitation of this study. Thus, for future we recommend longitudinal and qualitative (to identify their perception) study to get better information to design best strategies to enhance this services.
Conclusion
Cervical cancer screening proportion in the study area is very low as compared to the proportion of other areas. Factors like Women age, educational status, and employment status, having 2 to 3 numbers of sexual partners, knowledge, attitude, and parity showed significant association. Therefore, intervention programs intended at improving cervical cancer screening practice among women should focus on the significant factors.
Supplemental Material
sj-docx-1-inq-10.1177_00469580231159743 – Supplemental material for Cervical Cancer Screening Practice Among Women: A Community Based Cross-Sectional Study Design
Supplemental material, sj-docx-1-inq-10.1177_00469580231159743 for Cervical Cancer Screening Practice Among Women: A Community Based Cross-Sectional Study Design by Frew Tadesse, Abebe Megerso, Ebrahim Mohammed, Desalegn Nigatu and Ebissa Bayana in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Author Contributions
All authors agreed to be held accountable for all aspects of the work, made significant contributions to conception and design, data collection, analysis, and interpretation, participated in writing the article or critically revised it for important intellectual content, gave their final approval on the version to be published, and gave final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Study Area
Study was conducted at Negelle Borena which is located in the East Guji zone 600 km away from the capital city of Addis Ababa. This zone is one of the zones in the Oromia region is bordered on the south by the Borna Zone, on the west by the West Guji zone, on the north by Sidama region, on the northeast by Bale zone, and on the east by Liben zone of Somali region.
Ethical Approval and Consent
Ethical clearances were gained from the institutional ethical review board of Adama Hospital Medical College (AHIRB/121/2021) before engaging in the study. The permission and support letters were obtained from Negelle Borena health office. Confidentiality and respect for persons during the interview, analysis, and dissemination were guaranteed for all participants using information sheets. Data collectors were strongly informed about obligations like justice to protect the well-being of the study units. Subsequently, informed consent was assured from all participants for their willingness to be part of the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.