
Abstract
Sepsis is a widespread problem that can create clinical and economic difficulties. This study aimed to determine the knowledge, attitudes, practices, and barriers related to the sepsis and sepsis management among emergency nurses and physicians. Data was collected using a self-questionnaire completed by the participating nurses and physicians (n = 243), with a 61% response rate. The study found that both emergency nurses and physicians had poor-to-moderate levels of sepsis knowledge, with emergency physicians having better attitudes regarding sepsis and sepsis management than emergency nurses. However, moderate knowledge levels of sepsis practice and management were shown among both nurses and physicians. It is evident that for emergency nurses and physicians, the biggest barrier to providing quality care to patients with sepsis is the lack of monitoring equipment. Both nurses and physicians need consistent sepsis management information provided by continual education programs. Development of an approved protocol can improve nurses’ knowledge, attitudes, and practices.
What do we already know about this topic?
Despite advancements in diagnostic and treatment methods, the incidence of sepsis continues to climb substantially.
How does your research contribute to the field?
Dissemination of current recommendations about sepsis and sepsis management among emergency nurses and physicians to avoid mistakes, risky attitudes, and practices.
What are your research’s implications towards theory, practice, or policy?
Implementation of training and continual education programs for emergency nurses and physicians by using the latest guidelines regarding the proper management of sepsis.
Introduction
Sepsis is an extreme reaction of the body to an infection, and is a life-threatening condition. Sepsis affects an estimated 31.5 million people worldwide each year, resulting in 5.3 million deaths. 1 The global burden of sepsis is difficult to assess. According to a recent scientific publication, there were 48.9 million cases of sepsis and 11 million sepsis-related deaths worldwide in 2017, accounting for nearly 20% of all global deaths. 2 The burden of sepsis is likely the greatest in low- and middle-income nations and raises the financial costs of care. 2 The condition is notoriously expensive to treat and has been associated with an increased risk of readmission. 3
Sepsis can progress to septic shock, characterized by vasodilatation-related altered fluid volume, increased capillary permeability, and circulating volume maldistribution, in which certain organs (eg, the lungs, skin and kidneys) do not receive the blood they need. 4 Sepsis management consists of interventions using a critical care algorithm and specialized diagnostic equipment aimed at rapid identification of sepsis in the emergency room. This is followed by rapid treatment of symptoms, while simultaneously identifying the etiology of the infection. 5 Rapid diagnosis and early sepsis management may decrease mortality and enhance outcomes in patients with sepsis or septic shock.6,7
Barriers to sepsis management include lack of interest in improving existing procedures, lack of awareness of the guidelines, lack of understanding of the guidelines or medical condition, contradictory instructions in the workplace, and insufficient use of the sepsis screening form at the time of triage.8,9 In order to optimize and maximize outcomes for patients with sepsis, it is important to determine the levels of knowledge, expertise, attitude and practice in healthcare professionals, and overcome barriers in implementing a treatment bundle with early detection of sepsis. 10 Lack of knowledge and training, staff nursing, and difficulties in identifying sepsis patients in the Emergency department (ED) are the main obstacles in sepsis management. 11 A good level of understanding, attitude, and practice regarding sepsis protocols is therefore necessary for the management of this condition to be improved. 12 The prompt and efficient treatment of sepsis accompanied by good practices and availability of equipment will aid in preventing the development of septic shock, which can lead to organ dysfunction and is associated with a high mortality rate.5,13,14
Good knowledge, a positive attitude, and best practices in sepsis care by emergency nurses and physicians may help to improve patient clinical outcomes and reduce morbidity and mortality rates in Palestinian hospitals. There have been no previous studies related to this topic conducted in Palestine. Therefore, the current research project will determine the knowledge, attitudes, practices, and barriers of emergency nurses, and physicians regarding sepsis and sepsis management. Furthermore, it will examine the correlation between knowledge, attitude and practices regarding sepsis, sepsis management, and social demographic characteristics among emergency nurses and physicians.
Materials and Methods
A cross-sectional descriptive study design was used. A convenience sample of 243 emergency nurses and physicians was taken, consisting of 172 (70.8%) emergency nurses and 71 (29.2%) physicians. The convenience sampling used the following inclusion criteria: nurses and physicians aged 21 years and older who have been working in the emergency department for at least 6 months.
Population
In this study, the target population was all nurses working in the ED at Palestinian hospitals. The total population in these hospitals is 258 emergency nurses and 128 emergency physicians. Data was collected during the months of February to May, 2021.
Sample Size
The sample size depended on the response rates of the nurses and physicians working in the emergency department. According to the Raosoft online sample calculator, 15 the minimum sample size was 164.
Instrumentation
Data was collected from nurses and physicians working in the ED through a survey,5,16 designed to determine the knowledge, attitudes, practices and barriers regarding sepsis and sepsis management. The survey was compiled through literature review, and consultation with supervisors, experts in the field of general medicine and specialists in internal medicine. Modifications were made accordingly. The time frame to complete the questionnaire was 15 to 20 minutes, as in the pilot study.
The questionnaire consisted of 3 sections. Section 1 (social demographic data) included gender, age, educational level, years of experience in the ED, years of experience as a nurse/physician, sepsis training and continual education, whether the participant follows a specific protocol/guideline for sepsis management, and the percentage of shifts dealing with sepsis patients at the ED.
Section 2 included questions on knowledge, attitudes and practices (KAP variables) related to sepsis management. The survey consisted of multiple-choice questions (MCQ) and closed-ended questions based on the Likert scale of strongly agree (1), always agree (2), frequently natural (3), occasionally disagree (4), rarely and strongly disagree or (5), never (6), with the results being reported using the percentage, mean and frequency, and analyzed using correlation analysis and the independent t-test. The level of the participants’ knowledge was categorized using 3 components based on their percentage scores 17 as: good (80-100%), moderate (50-79%), and poor (less than 50%). To assess the participants’ attitude and practice levels, the category was divided into higher or lower levels based on the mean (M) score results.
Section 3 included closed-ended questions on barriers related to sepsis management based on the Likert scale. The biggest barriers towards sepsis and sepsis management were identified based on the highest mean score for each group.
Pilot Study
A pilot study was conducted with 10 emergency nurses and 10 emergency physicians in order to identify any weaknesses in question wording and predicted response rates, in addition to determining the time needed to fill the questionnaire. It also identified areas of vagueness and tested the validity and suitability of the questionnaire. The questionnaires were evaluated by 2 internal medicine specialists, with their comments and modifications being applied as needed.
Validity
The construction of the questionnaire was reviewed by experts, who judge its face and content validity, and provided feedback and comments.
Reliability
The reliability test was calculated for 3 domains (knowledge, attitude, and practices). Once the data was collected from all participants and analyzed using SPSS, analysis showed that Cronbach’s alpha equaled 0.5 for the knowledge questions and 0.7 for the total attitude and practice questions. Due to the limited number of available participants, the pilot participants were also added to the study sample.
Data collection
Self-developed, validated, closed-ended questions, and an MCQ survey were used. Surveys were distributed by hand to the identified participants for the main study. The researcher waited for the participants to complete the surveys when they were off work during a break period. These meeting times were coordinated beforehand and were conducted towards the end of morning or evening shifts, which improved the response rate. In total, 243 surveys were distributed, all of which were returned. The response rate was 66.67% for emergency nurses and 55.46% for physicians, when considering the entire target population.
Ethical Considerations
Ethical approval was granted by the XX and the administrators of the hospital where the study was conducted. The study was also approved by the X committee, under number PHRC/HC/805/21.
Analysis
In this study, statistical analysis, data manipulation, and generation of tables and graphs of the collected data were conducted using the statistical package for the social sciences (SPSS) version 23. Descriptive statistical analysis in the form of frequencies and percentages were presented in tables and figures. Means and standard deviations were used to summarize the data. Additionally, t-tests and ANOVA were used to test correlations between variables. Furthermore, multivariate linear regression was used to identify for predictors, with the statistical significance threshold being set at P < .05.
Results
Regarding the personal characteristics of the participants in the study, as seen in Table 1, the majority (78.6%) were males between the ages of 21 and 30 (58.8%), and 179 (73.7%) held a university bachelor’s degree. Regarding the participants’ experience, the majority (139, 57.2%) of nurses and physicians (58.7% and 53.5%, respectively) had less than 3 years of experience, half of them had less than 5 years of experience, and a few of them (7%) had more than 10 years of experience in the emergency department. As for continual education and training on dealing with sepsis cases, the results showed that up to 60% of nurses and physicians had not received any such training, and few of them had received information either through workshops in the emergency department (25.5%), courses (10.3%), or through online electronic sources (7%).
Demographic and Characteristics of the Study Participants.

ED = emergency department.
Regarding the existence of international protocols or guidelines adopted in emergency departments, the results reflect the absence of such protocols or guidelines adopted to deal with sepsis cases. Very few physicians (2.8%) answered that they use such protocols or guidelines received from international institutions such as the CDC, despite the fact that a relatively high number of physicians and nurses indicated that the rate of dealing with these cases reaches more than 30%.
The Level of Knowledge About Sepsis and Sepsis Management Among Nurses and Physicians
Figure 1 reflects that the majority of both nurses and physicians had poor (47.7%) to moderate (51.0%) levels of knowledge about sepsis, while just 1.2% had a good level of knowledge. The average knowledge level (poor, moderate and good) for nurses (48.8%, 50.0%, and 1.2%) was slightly lower than the average knowledge level of physicians (45.1%, 53.5%, and 1.4%), but this difference was not statistically significant (P = .86).

The level of knowledge about sepsis and sepsis management among nurses and physicians.
Knowledge Related to the Definition and Cause of Sepsis Among Nurses and Physicians
When the participants were asked about the most common routes of infection, 41.6% (40.1% of nurses and 45.1% of physicians) answered, correctly, that the respiratory system is the most common route of infection. In total, 60.9% (58.7% of nurses and 66.2% of physicians) knew the definition of the systemic inflammatory response and 67.9% (65.7% of nurses and 73.2% of physicians) knew the correct definition of sepsis, which is the presence of infection with 2 SIRS criteria, as shown in Figure 2.
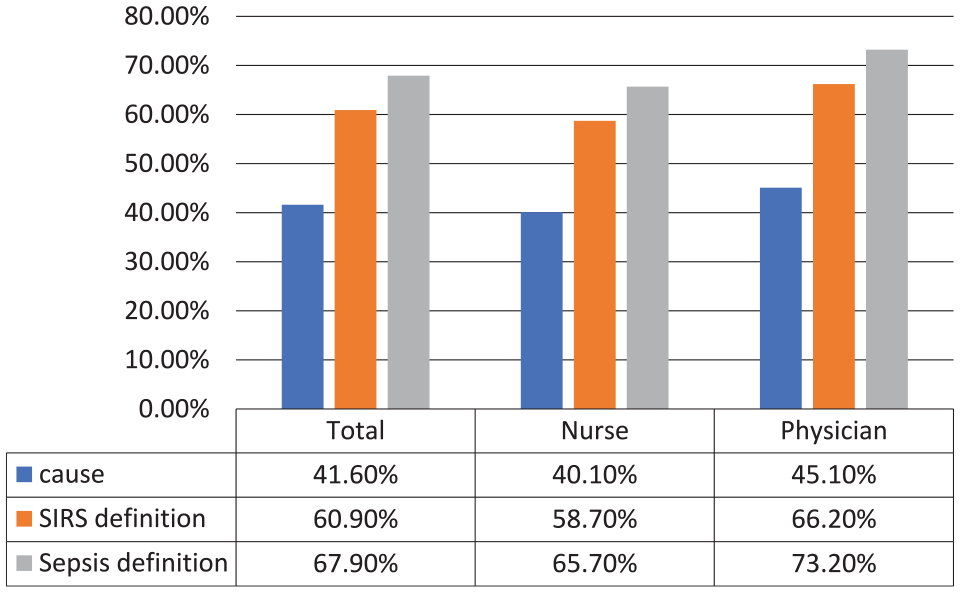
Knowledge related to definition and cause of sepsis among nurses and physicians.
Nurses and Physicians’ Knowledge Level Related to Monitoring Lactate, Scoring, and Hemodynamic Parameters for Sepsis
When the participants were asked about the monitoring of sepsis, 33.3% (34.9% of nurses and 29.6% of physicians) answered correctly that the elapsed time before the performance of a lactate test is 30 to 60 minutes for patients with symptoms suggesting sepsis, and 39.1% (39.0% of nurses and 39.4% of physicians) knew that a lactate threshold of 4 indicates that a patient is in sepsis. Overall, 51.0% (47.1% of nurses and 60.6% of physicians) knew that the mental status, BP, RR, SPO2, and JVP of a septic patient should be measured at least once every 30 minutes in the ED. This low level of knowledge is to be expected, given that 41% of participants (48.8% of nurses and 23.9% of physicians) stated that the scoring assessment system for sepsis is not used in daily practice in their workplace, as shown in Table 2.
Knowledge Related to Monitoring Lactate, Scoring, and Hemodynamic Parameters of Sepsis Among Nurses and Physicians.

The highest Percentage
Knowledge Related to Sepsis and Sepsis Management
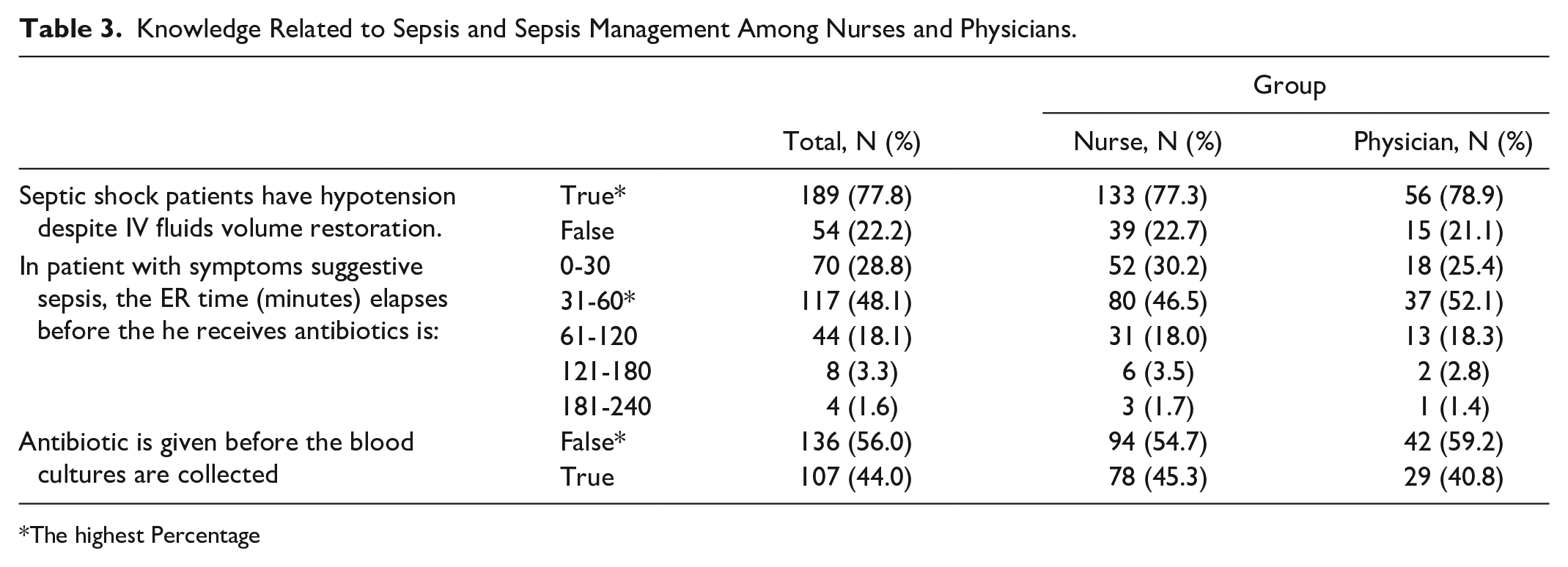
Of the total participants, 77.8% (77.3% of nurses and 78.9% of physicians) answered correctly that patients in septic shock may have hypotension despite IV volume restoration with fluids, and 48.1% (46.5% of nurses and 52.1% of physicians) knew that the patient should receive antibiotics within 31 to 60 minutes if they have symptoms of sepsis in the ER. Furthermore, 56.0% (54.7% of nurses and 59.2% of physicians) knew that blood cultures should be collected before antibiotics are given, as shown in Table 3.
Knowledge Related to Sepsis and Sepsis Management Among Nurses and Physicians.
The highest Percentage
Knowledge Related to Early Detection and Diagnosis of Sepsis and Sepsis Management Among Nurses and Physicians
Regarding the knowledge related to early detection and diagnosis of sepsis among nurses and physicians, 43.2% (39.0% of nurses and 53.5% of physicians) answered correctly that a fall in MAP < 70 mmHg increases the suspicion of sepsis, and 62.1% (59.9% of nurses and 67.6% of physicians) knew that vomiting, diarrhea, gastroparesis, and ileum may be early signs of organ dysfunction. Furthermore, both nurses and physicians considered that a patient may have septic syndrome when the patient develops LOC alterations (58.8%; 59.9% of nurses and 56.3% of physicians) or hyperglycemia (>7.7 mmol/L) in the absence of diabetes (46.5%; 42.9% of nurses and 52.1% of physicians).
Additionally, 48.6% (47.7% of nurses and 50.7% of physicians) of participants thought a WBC count of 4 × 109/L does not meet the diagnostic criteria for sepsis, and 67.9% (70.3% of nurses and 62.0% of physicians) expected that the level of SPO2 in sepsis patients is less than 90%, as shown in Table 4.
Knowledge related to early detection and diagnosis of sepsis among nurses and physicians.

WBC = white cell count; ED = emergency department.
True answer.
Participants’ Demographics Variables and Their Level of Knowledge Related to Sepsis and Sepsis Management
Except for the practical emergency experience of nurses and physicians (P = .046), linear regression analysis revealed that neither demographic variable nor attitudes or practices of the nurse and physician participants were able predict their level of knowledge about sepsis and sepsis management, as shown in Table 5.
Linear Regression for Predictors’ Variables of Emergency Participants’ Demographics Variables and Their Level of Knowledge Related to Sepsis and Sepsis Management.

Attitudes Regarding Sepsis and Sepsis Management Among Emergency Nurses and Physicians
Although the attitudes of both nurses and physicians were high, the physicians had relatively higher attitudes towards early screening and intervention (4.03/5), IVF as a positive factor (3.97/5), laboratory tests (blood cultures) and drugs (3.93/5), and educational training about sepsis (3.9/5), as shown in Table 6.
Level of Attitudes Regarding Sepsis and Sepsis Management Among Emergency Nurses and Physicians.

Participants’ Demographic Variables and Their Attitudes Related to Sepsis and Sepsis Management
Through linear regression analysis, age (P = .040), occupation (P = .016), the percentage of septic cases dealt with (P = .009), and practice level with septic cases (P < .001), were found to be predictors of the attitudes of the participants towards sepsis and sepsis management, as shown in Table 7.
Linear Regression for Predictors’ Variables of Attitudes Regarding Sepsis and Sepsis Management Among Emergency Nurses and Physicians.

Practices Regarding Sepsis and Sepsis Management Among Emergency Nurses and Physicians
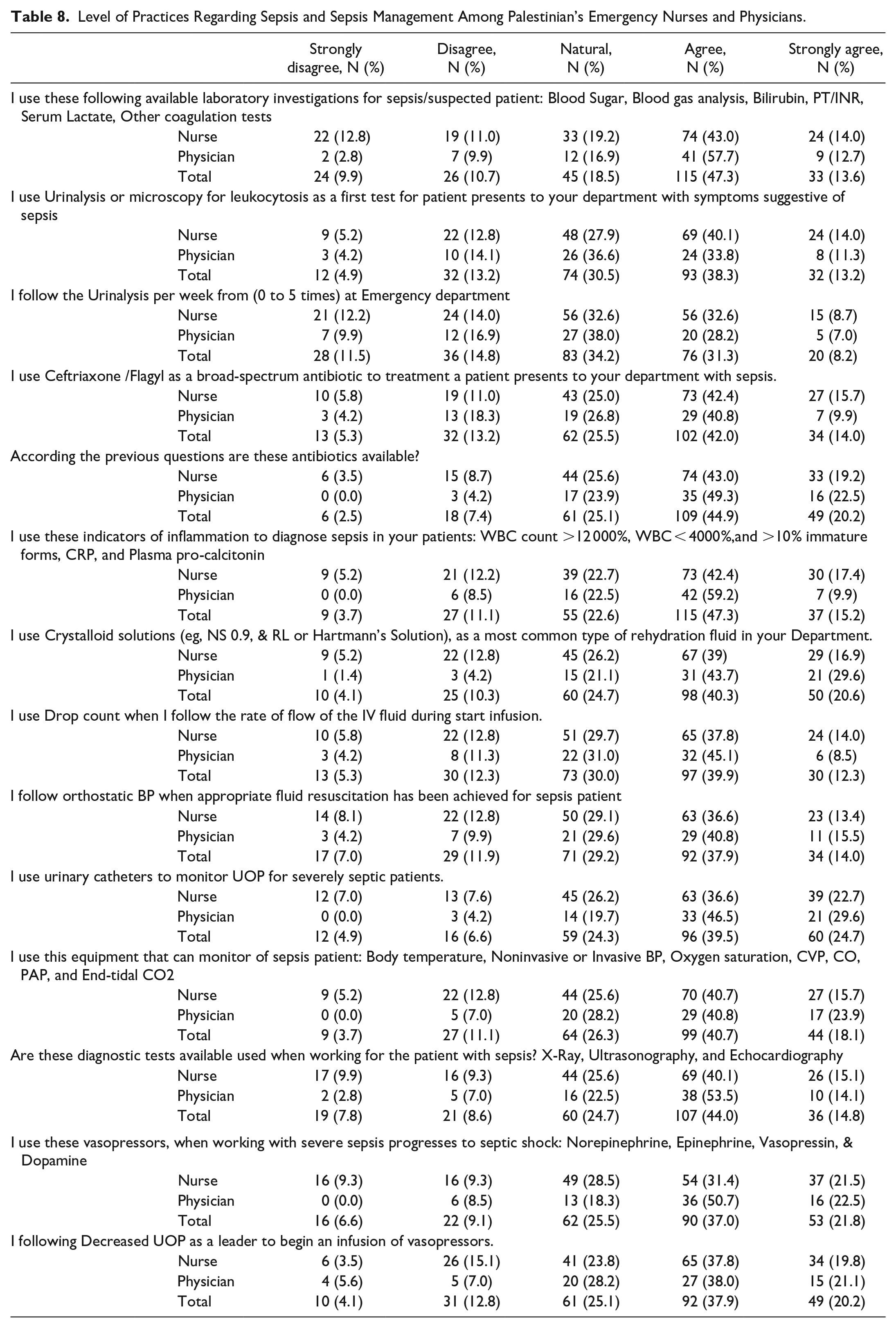
The rate of performance of practices related to patients with sepsis and sepsis management among nurses and physicians was moderate, at 48.3 out of 70 among the nurses and 51 out of 70 among the physicians. Figure 3 shows that the rate of performance of practices for patients with sepsis and sepsis management among nurses and physicians working in emergency departments was between 3 and 4 out of 5, meaning that it was moderate to the extent that it was between 60% and 70%. Physicians had higher rates than nurses, except for the questions related to the use of urinalysis or microscopy for leukocytosis, as shown in Table 8.
Level of Practices Regarding Sepsis and Sepsis Management Among Palestinian’s Emergency Nurses and Physicians.

Barriers Level regarding sepsis and sepsis management among Palestinian’s emergency Nurses and physicians.
Participants’ Demographic Variables and Their Level of Practices Related to Sepsis and Sepsis Management
Post hoc multiple comparison revealed that ED participants with 3 to 5 years’ experience had a higher mean practice (51.1) compared to other participants and this difference was statistically significant (P = .021). Participants with work experience of 15 years or more had the lowest mean practice (36.5) compared to other participants, also showing a statistically significant difference (P < .001). Participants who were untrained had the highest mean (51.8) practice compared with other participants (P < .001).
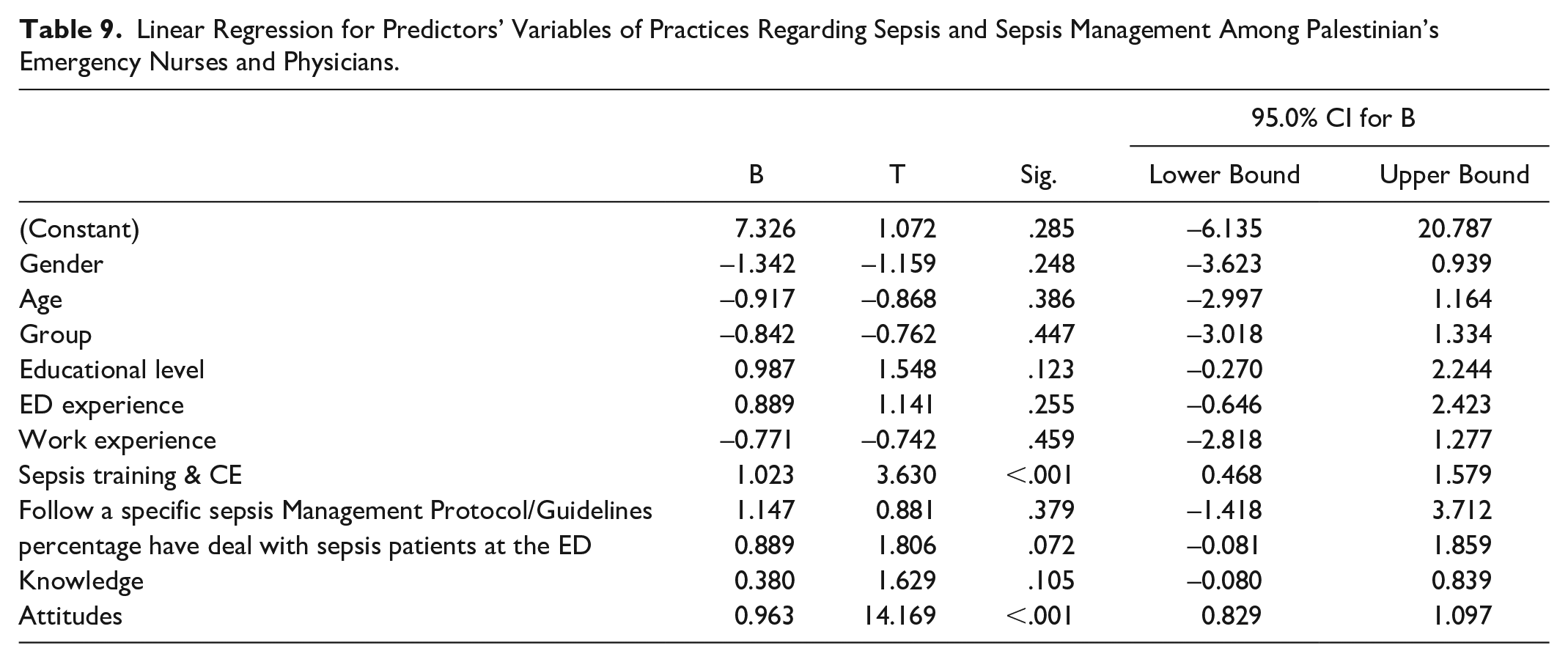
The linear regression analysis showed that training, continual education, and attitude have the ability to predict the practice of nurses and physicians working in emergency departments. There was a statistically significant relationship between these variables and the percentage of practice of sepsis and sepsis management among nurses and physicians working in emergency departments, as shown in Table 9.
Linear Regression for Predictors’ Variables of Practices Regarding Sepsis and Sepsis Management Among Palestinian’s Emergency Nurses and Physicians.
Barriers Regarding Sepsis and Sepsis Management Among Emergency Nurses and Physicians
According to workers in the emergency department, including the nurses and physicians participating in this study, the lack of monitoring equipment was the biggest obstacle preventing proper practice when dealing with septic cases (2.49 and 2.44 out of 5, respectively). According to the physicians, lack of antibiotics and lack of staff were the second and third biggest barriers. Lack of staff and lack of lectures on the subject were the second and third biggest barriers according to the nurses (2.37 and 2.37 vs 2.41 and 2.40, respectively).
According to the nurses, the last 3 barriers were lack of antibiotics (2.37), lack of information (2.34), and work pressure (2.33). For the physicians, they were work pressure (2.25), lack of lectures (2.21) and lack of information (2.11), as shown in Figure 3.
Discussion
Based on the current study, the majority of both nurses and physicians had poor (47.7%) to moderate (51.0%) levels of knowledge regarding sepsis, while only (1.2%) of them had a good level of knowledge. This is inconsistent with a study published by Hasan et al (2020), who found that the majority of nurses (70%) had a good level of knowledge regarding sepsis prevention at a neonatal care unit. 18 Another study published by Nucera et al 14 in Northern Italy, showed that >75% of nurses and physicians had an excellent awareness of procedures that raised the risk of sepsis, 50% to 70% had fairly good knowledge of blood culture technique, and 50% had a poor understanding of early detection, methods, and scores for the diagnosis and management of sepsis, which is consistent with the current study.
In our study, urinary tract infection was the most common cause of infection. This was inconsistent with a previous study, which found that respiratory tract infection was the most common cause of infection. 19
When the participants were asked about the elapsed time before a lactate test should be performed, 33.3% of them gave the correct answer of 30 to 60 minutes. This is consistent with the results of Levy et al 20 When the participants were asked about the lactate threshold used for septic patients, 39.1% of them gave the correct answer of 4 mmol/L, which is consistent with the results of Belsky et al 21 On the other hand, when participants were asked whether a WBC count of 4 × 109/L meets diagnostic criteria for sepsis, 51.4% of them answered incorrectly, which was inconsistent with the results of Singer et al. 13
According to the current study, none of the demographic and characteristic variables showed any statistically significant relationship with their level of knowledge about sepsis and sepsis management. This is similar to the results of a study published in Malaysia in 2019, which showed no significant relationship between the participants’ characteristics and their knowledge score on sepsis and systemic inflammatory response syndrome. 10 A study published by Hasan et al’s study, 18 in Hilla city showed that education levels and training courses about septicemia had a statistical significant effect on nurses’ knowledge regarding the prevention of sepsis at a neonatal care unit.
According to the current study, only experience in the ED was able to predict the knowledge level of sepsis and sepsis management. A study published in Western China (2021) showed that the scores of attitudes and practices can predict the knowledge level regarding the prevention of medical device-related pressure injury (P < .005). 22
In our sample, physicians had a higher attitude than nurses. A study published in the Gaza Strip (2017) showed that nurses expressed more positive attitudes towards collaboration than physicians, which is inconsistent with the current study. 23 Although physicians had a relatively higher attitude regarding early screening and intervention to improve outcomes for sepsis patients, IVF as a positive factor, laboratory tests (blood culture), drugs, and educational training about sepsis should be implemented in hospitals. A study published in Northern Italy (2018) found that physicians have the highest attitudes towards early screening, intervention and blood culture lab tests. 14 Another study published in Iran (2012) showed that high attitudes of ICU nurses regarding sepsis were due to educational programs, which is consistent with the current study. 12 A study published in India (2019) showed that nurses had poor attitudes regarding antibiotic use for viral infection. 24 This is inconsistent with the current study, which shows that antibiotics are considered the most important treatment by emergency nurses dealing with sepsis and sepsis management.
This study showed that group categories, ED experience, work experience, and sepsis training had a statistically significant correlation with the attitudes regarding sepsis and sepsis management. A study published in the Gaza Strip (2017) showed significant differences in the attitude towards collaboration between physicians and nurses. Moreover, the nurses’ mean scores was higher than the those of the physicians. This indicates that the nurses’ attitudes towards nurse-physician collaboration were higher than those of the physicians. 23 This is inconsistent with the current study, which showed a group category that had a statistically significant relationship with their level of attitude about sepsis and sepsis management and emergency physicians.
Post hoc test results of another study published in Western China (2021) showed a significant relationship between attitudes of ICU nurses and length of work experience (11-15 years, 16-20 years, and >25 years). Attitude scores were highest in subjects with 16 to 20 years of work experience. 22 This is inconsistent with the current study, where work experience had a significant impact on the level of attitude regarding sepsis and sepsis management, but those with 15 years or more had the lowest mean attitudes compared to other participants. Another study published in Indonesia (2016) showed that positive attitudes in nurses and physicians were critical in emergency practice, as they have a direct impact on the quality, safety, accountability, and responsibility of care. 25 This is inconsistent with the current study, as sepsis training had a significant correlation with the attitude levels regarding sepsis and sepsis management, but the participants who acquired information online had the lowest mean attitudes compared to participants who had workshop emergency or no training. A study published in Turkey (2018) showed no significant relationship between emergency nurses’ attitude and the ED experience regarding patient safety. 26 This is inconsistent with the current study, which showed that ED experience for emergency nurses and physicians had a significant correlation with their attitude towards sepsis and sepsis management.
According to the current findings, the predictors of attitude levels among nurses and physicians towards sepsis and sepsis management were age, occupation, percentage of dealing with septic cases, and practice levels with septic cases. A study published by Zhang et al’s, 22 in Western China (2021) showed that the knowledge score and practice had a statistically significant effect according to the linear regression analysis to investigate the effects of demographic characteristics on ICU nurses’ attitudes about the prevention of medical device-related pressure injury. This is consistent with the current study, as practice levels with septic cases had a significant correlation with the attitude to sepsis and sepsis management among the emergency nurses and physicians. This, however, is inconsistent with the current study in the sense that knowledge had no statistically significant relationship with the level of attitude regarding sepsis and sepsis management among the emergency nurses and physicians.
According to the current findings, the most highly regarded practice by emergency nurses is the use of antibiotics (ceftriaxone/flagyl). The current study also shows that the most highly regarded practice among emergency physicians is the use of urinary catheters to monitor UOP in severely septic patients. A study published in Kenya (2015) showed that crystalloid fluids were the most common resuscitation fluids for sepsis management, with 80% of healthcare providers utilizing the drop count method, and 50% in the ICU using IVF pumps for most antibiotic treatments with ceftriaxone/flagyl. 5
The study showed that ED experience, work experience, and sepsis training had a significant relationship with the level of practice regarding sepsis and sepsis management. A study published in Indonesia (2019) showed that training had a significant impact on the emergency nurses’ practice. 27 Another study published by Gruda and Sopjani’s, 28 in Kosovo (2017) showed that the work experience regarding the management of hospital-acquired infections had a significant relationship with the emergency nurses’ practices. Moreover, a study published in Saudi Arabia showed that over 5 years of ED experience had a more significant impact on emergency nurse and physician knowledge than practices and attitudes did. 29
The linear regression analysis showed that training, continual education, and attitudes can predict the practices of nurses and physicians working in emergency departments. A study published in Western China (2021) showed that attitude plays a key role in the ability to predict the practices of nurses in the ICU regarding preventing medical device-related pressure injury. 22
The biggest barriers for emergency nurses regarding sepsis and sepsis management in Palestinian hospitals, were lack of monitoring equipment, shortage of staff, inadequate lectures/workshops/conferences/seminars about sepsis, lack of information about sepsis, and workload in the ED. A study published in South Korea (2013) showed that the high crowding in the ED had adverse effects. This led to a low compliance rate with the resuscitation bundle in managing severe sepsis and septic shock. 30 Another study showed that staff scarcity was the most prevalent obstacle in compliance with the sepsis bundle, followed by delayed patient presentation and overcrowding. 31
However, a study by Seok et al’s, 32 showed that a combination of insufficient diagnostic criteria for sepsis and time constraints to provide broad-spectrum antimicrobial therapy continues to be an impediment to antimicrobial stewardship. Efforts such as selecting appropriate empirical antibiotics and deciding whether to discontinue antibiotics may help to improve a sepsis patient’s prognosis. 32 Furthermore, a study by Mathenge, 5 showed that the most common barriers regarding sepsis management are advanced patient presentation, lack of antibiotics, and lack of sufficient staff.
Conclusion
We can conclude that both emergency nurses and physicians have a poor to moderate level of knowledge, while emergency physicians had higher attitudes towards sepsis and sepsis management than emergency nurses. However, the practices of sepsis and sepsis management showed moderate levels among both emergency nurses and physicians.
Most of the participants reported that lack of monitoring equipment is the largest barrier to providing quality care to patients who present with sepsis. The study further revealed that most of the emergency nurses and physicians did not attend sepsis training or continual education concerning sepsis and sepsis management. Most of the emergency nurses and physicians did not receive any specific protocols/guidelines. These findings can be used by educators, hospital administrators and policymakers to plan future measures to improve sepsis management and reduce sepsis-related mortality.
Recommendations:
We recommend: (1) Dissemination of the current recommendations about sepsis and sepsis management among emergency nurses and physicians to avoid mistakes and, at times, risky attitudes, practices, common therapeutic errors and the lack of emergency department resources. (2) Implementation of training and continual educational programs for emergency nurses and physicians by using the latest guidelines regarding the proper management of sepsis. This may be an effective method to change the emergency nurses’ and physicians’ knowledge and practices towards the management of sepsis. (3) Consider emergency room training and continual education to improve sepsis and sepsis management situations. (4) Consider providing monitoring equipment, staff and laboratories with diagnostic resources to emergency departments to improve the management of sepsis patients. (5) Recommend decision-makers to formulate unique protocols/guidelines for dealing with sepsis patients in Palestinian hospitals.
Footnotes
Authorship Statement
All authors listed meet the authorship criteria and all authors are in agreement with the content of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.