
Abstract
Introduction
Ankle pump exercise (APE) is an effective method to prevent deep vein thrombosis (DVT) in the lower extremities. However, traditional APE at a frequency of 3 times/min applied in the clinic lacked high compliance, and individuals were found to prefer an APE of 30 times/min. This study aimed to compare the effects of APEs with the above two different frequencies on the venous hemodynamics and fatigue of lower extremities.
Methods
The study applied a randomized cross-over design, and 307 healthy adults were randomly assigned into two groups, whose left feet performed 5 minutes of traditional APE (3 times/min, after 10 minutes of rest) and 5 minutes of selected APE (30 times/min, after 10 minutes of rest) in different orders. The diameters and blood flow velocities of the external iliac vein, femoral vein, and popliteal vein of the left extremities were recorded with the color doppler ultrasound when participants were at rest and after 5 minutes of traditional or selected APE. The fatigue of lower extremities was assessed with the Rating of Perceived Exertion (RPE) after the participants performed 5 minutes of different APEs.
Results
After both traditional APE and selected APE, the diameters and blood flow (peak systolic) velocities of the external iliac vein, femoral vein, and popliteal vein increased significantly in the participants (P<.01), and the effects of the two APEs on venous hemodynamics of the lower extremities had no significant difference (P>.05). However, participants reported that traditional APE caused higher fatigue, and 252 (82.1%) participants preferred APE at 30 times/min.
Conclusion
Both traditional and selected APE could increase venous blood flow in the lower extremity. Despite the equivalent effects, the selected APE of 30 times/min may cause less fatigue than the traditional one of 3 times/min.
Keywords
• Ankle pump exercise (APE) could effectively prevent deep vein thrombosis in the lower extremities. • Despite the equivalent effects, the selected APE at 30 times/min may cause less fatigue than the traditional one of 3 times/min. • This study provides healthcare professionals evidence that the APE performed at 30 times/min would result in more patient adherence and should be further explored in patients.
Introduction
Deep vein thrombosis (DVT), the formation of blood clots in deep veins, 1 continues to be a significant health problem that causes morbidity, mortality, and economic burden on the healthcare system globally.2,3 Lower extremity DVT had an incidence of about .1% in the general population, and DVT led to 600 000 hospitalizations and 80 000 deaths in the USA annually. 3 In China, although there was a lack of multicenter epidemiological data, the prevalence of DVT among patients in intensive care units was reported to be between 10% and 100%, and 2.1% to 4.7% of patients died because of DVT. 4 Therefore, the prevention of DVT is of particular importance, and nurses are assumed to play a pivotal role in DVT prevention. 5
Ankle pump exercise (APE) has always been recommended as the most common mechanical prevention method.6,7 Through the movement of the ankle joint, APE drives the calf muscle to contract and relax rhythmically to increase the venous reflux of the lower extremities. 8 Normally, each calf muscle contraction can discharge 60 mL to 90 mL of blood, effectively squeezing the blood from the veins of the lower limbs to the proximal. 9 And reduced calf muscle pump function is a risk factor for DVT. 10 APE has been proven to effectively relieve limb edema and reduce DVT, widely used in daily life and clinical practice. 11 However, in practice, standardized APE has not been established yet.
Previous studies had discussed the optimal position, 12 exercise mode (active or passive), 13 and ankle range of motion; 14 and had drawn similar conclusions which were in accordance with the clinical practice. APE in the supine position was found to be more effective in facilitating the blood flow than in the leg-up and head-up positions. 12 Both passive and active APE could increase the blood flow velocity of the femoral vein, while active APE was more effective. 13 Moreover, a large ankle range of motion was more efficient, 14 and plantarflexion (hook the foot up at the maximum possible angle) and dorsiflexion (stretch the foot and step down the toes as far as possible) were recommended for APE.
As for the frequency of performing APE, traditional APE proposed keeping plantar flexion and dorsiflexion for 10 seconds, resulting in a slow frequency of 3 times/min. However, in the clinic, we found that the patients lack high compliance when performing traditional APE, and the results of recent studies did not support the traditional frequency. According to Li et al.‘s study, 15 fast-frequency APE was more effective in promoting venous blood by comparing four different frequencies of 6 times/min, 10 times/min, 30 times/min, and 60 times/min. Based on a study of 29 patients after total hip arthroplasty, Nakayama et al 16 reported that APE at 60 times/min was more effective than that at 40 or 80 times/min. However, when performing APE at 60 times/min, participants reported that they were tired after exercising for 2 to 3 minutes.15,16
To our knowledge, there was no study on the exercise duration and interval of APE. It was recommended that each exercise time for APE was 5 minutes. Under the current background, we would like to find a more appropriate frequency to exercise for 5 minutes. As the staff of the Department of Vascular Surgery, the authors pre-investigated 30 healthy adults, finding that they could not continue performing APE at 60 times/min for more than 2 or 3 minutes because of limb fatigue (the participants stated that they were exhausted); and the majority preferred an APE at about 30 times/min (plantarflexion and dorsiflexion stayed for 1 second respectively). Patient preferences become a fully-fledged part of nursing decision-making in evidence-based practice when in practice. 17 However, there was a lack of comparison between selected APE (30 times/min) preferred by the individuals and traditional APE (3 times/min) applied in practice.
Therefore, the purpose of this study was to compare the impact of APEs at the above two frequencies (adopted a supine position, and an ankle range of plantarflexion and dorsiflexion) on the venous hemodynamics and fatigue of lower extremities, to provide nurses a theoretical basis for the guidance of APE.
Methods
Participants
The participants were recruited from the nursing interns of XXX Hospital between December 2020 to February 2021. To be included in the study, people were healthy adults without taking medicine in recent 2 weeks and were willing to follow the experimental procedure. People were excluded if they: (1) had skin damage in the lower extremity, (2) with a history of trauma or vascular disease in the lower extremity (eg, atherosclerosis, varicose veins, venous thrombosis), or (3) dropped out of the experiment or could not cooperate with the researchers to do APE under the instructions. Written consent was obtained from all the participants.
Experimental Design
The study applied a randomized cross-over design, followed by the CONSORT checklist. The study protocol was approved by the Ethics Committee of the Shanghai Changhai Hospital Ethics Committee (CHEC2019-080). This study had been registered in the Chinese Clinical Trial Registry (No. ChiCTR2100042776). Participants were randomly divided into group A and group B. Simple randomization was applied with the random number table of SPSS statistical software, and the random numbers were generated according to the UNIFORM function. All the participants lay in the supine position throughout the experimentation, keeping their emotions calm, limbs relaxed, and breath as steady as possible, since the blood flow velocity might be influenced by their breath. 18 Both group A and group B performed 5 minutes of traditional APE and 5 minutes of selected APE in different orders. In group A, the participants’ left lower limbs performed 5 minutes of traditional APE, 10 minutes of rest, and then 5 minutes of selected APE. While in group B, they performed 5 minutes of selected APE, 10 minutes of rest, and then 5 minutes of traditional APE. A researcher counted according to the stopwatch to ensure that the participants' performance met the requirements.
The study took the internal diameters and the blood flow velocities of the external iliac vein, femoral vein, and popliteal vein as the main index. According to the pre-test results, the mean velocity of the popliteal vein was 13 cm/s at rest and increased to 15 cm/s after selected APE; and the pooled standard deviation was 5 cm/s. Based on a test level of .05 and test efficiency of .90, the sample size was calculated to be above 68 with PASS software. The sample size could be guaranteed as 324 volunteers registered for the study.
A fully digital colored Doppler ultrasonic diagnostic system (Model Apogee 1100, 180W Power), produced in August 2017 by Shantou Ultrasonic Instrument Research Institute Co, Ltd, was applied to measure the main index. The internal diameters and the peak systolic velocities of the external iliac vein, femoral vein, and popliteal vein were measured at various time points (at rest, after 5minutes of traditional APE, and after 5 minutes of selected APE). All the measurements were carried out by one staff of the Ultrasonography Department. Besides, the Rating of Perceived Exertion (RPE), 19 which had been widely used to subjectively quantify an individual’s perception of the physical demands of an activity, 20 was applied to assess the lower extremity fatigue after 5 minutes of APE. After all the procedures, the participants were asked to choose their preferred frequency of APE.
Statistical Analysis
Descriptive statistics such as number, percentage, mean (M) and standard deviation (SD) were used to describe the demographic characteristics of the participants. χ2 test and independent sample t-test were applied to compare the participants’ characteristics between the two groups. Paired-t comparison and analysis of variance (ANOVA) were conducted to compare the differences in the diameters and the velocities of the external iliac vein, femoral vein, and popliteal vein at various time points. Wilcoxon rank sum test was applied to compare RPE values rated on the two frequencies APE, which were abnormal distribution data. The analyses were performed using SPSS version 20.1, and the two-tailed significance level was P < .05.
Results
Participants’ Characteristics
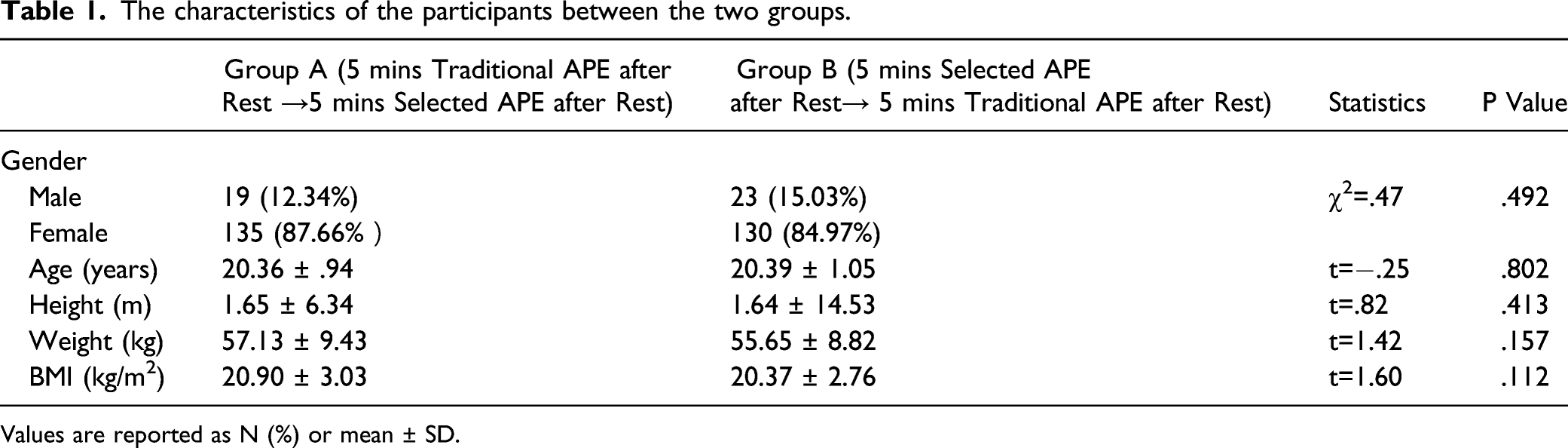
A convenient sample of 307 participants completed the research (see Figure 1). The participants reported no vascular risk factors or diseases. Most of them (n=265, 86.3%) were female, and their average age was20 (SD=1) years. There were no differences in gender, age, and body mass index (BMI) between group A and group B (Table 1). Flow chart of the enrollment process. The characteristics of the participants between the two groups. Values are reported as N (%) or mean ± SD.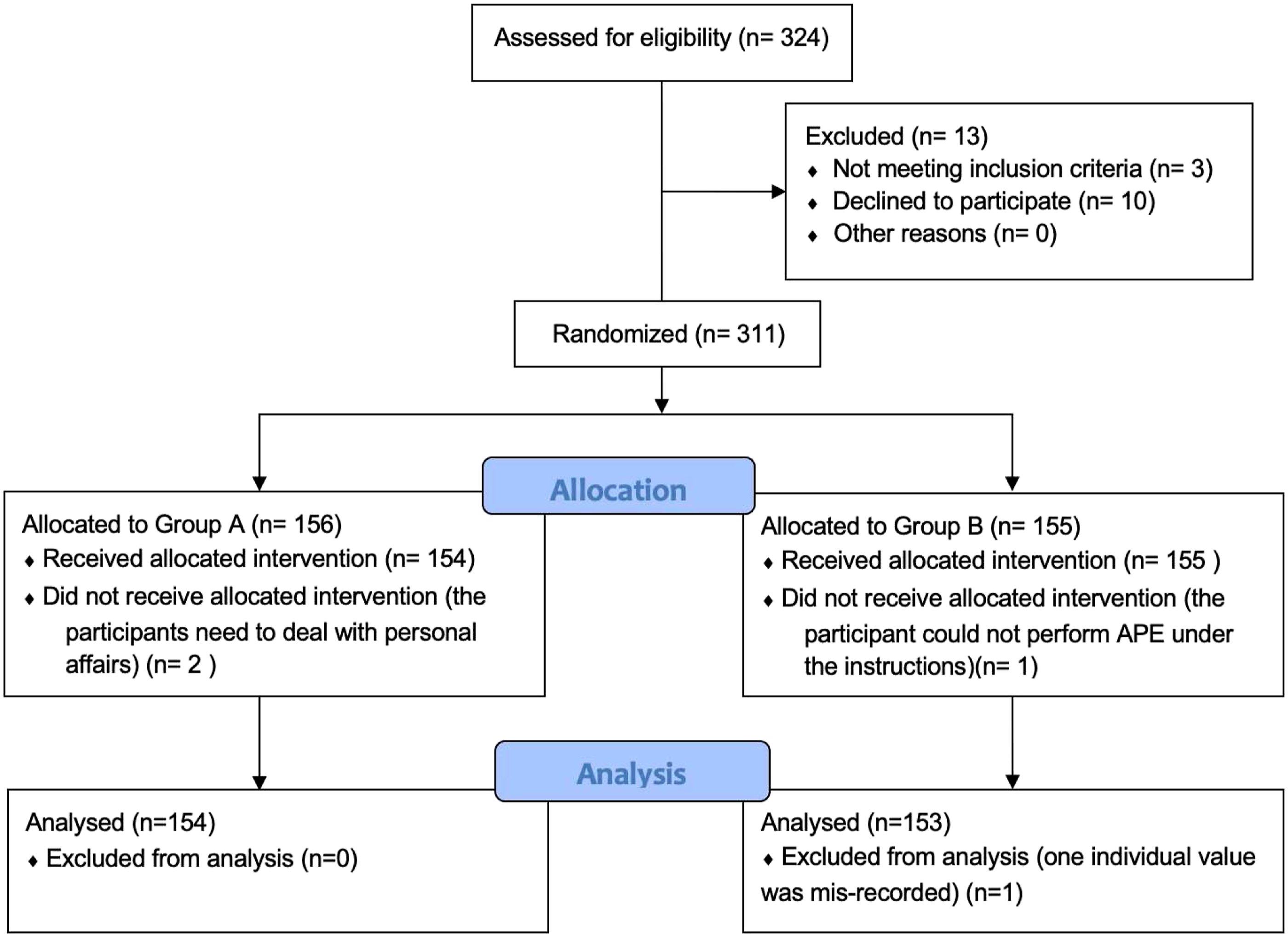
Effects of APEs on Venous Hemodynamics of Lower Extremities
At rest, the mean internal diameters of the external iliac vein, femoral vein, and popliteal vein were .83 (SD=.14), .74 (SD=.12), and .70 (SD=.11) cm. The mean peak systolic velocities of the external iliac vein, femoral vein and popliteal vein were 21.36 (SD=8.13), 16.21 (SD=6.56) and 16.21 (SD=6.56) cm/s. No matter after 5 minutes of traditional APE or after 5 minutes of selected APE, the mean diameters and the mean velocities of the external iliac vein, femoral vein, and popliteal vein were larger than those at rest (see Figure 2, Table 2). Paired-t test showed that the increases in the diameters and velocities were significant (P<.01, see Table 2). The internal diameters and the peak systolic velocities of the external iliac vein, femoral vein and popliteal vein at various time points. The diameters and the velocities of the external iliac vein, femoral vein, and popliteal vein before and after APEs. Values are reported as mean ± SD. aCompared with the index when the participants were at rest.

Comparisons of the Effects of the Two APEs on Venous Hemodynamics
Changes in the internal diameters and the blood flow velocities of the external iliac vein, femoral vein, and popliteal vein after APE at different frequencies.

Values are reported as mean ± SD.
Effects of Two APEs on the Lower Extremity Fatigue
Comparison of RPE scores rated on different frequencies APE.

Values are reported as median (Q1, Q3).
Discussion
Evaluation of the APE frequency could help nurses standardize performing APE in practice. As expected, this study found that no matter performing APE at a slow frequency of 3 times/min or a fast frequency of 30 times/min, the diameters and the velocities of the external iliac vein, femoral vein, and popliteal vein were all larger than those at rest. These findings supported that APE could prevent DVT by increasing venous blood flow velocities and raising the quantity of reflux.
Traditional APE was required to maintain the plantarflexion and dorsiflexion for 10 seconds, since it was believed that slowing down exercise frequency could increase the contractile force of the calf muscle and facilitate the venous blood return more effectively. 15 However, this study found that after 5 minutes of selected APE at 30 times/min, both the diameters and the velocities of the three veins had no significant differences from those after 5 minutes of traditional APE at 3 times/min. The results indicated that both slow-frequency and fast-frequency APE had no difference in promoting venous blood return. The authors inferred that although slow frequency increased the contractile force, the long-term contraction of the calf muscle maintained the veins in a continuous clamping state, 21 which was not conducive to venous reflux. The above two effects might offset each other.
However, this finding was not consistent with previous studies,13,15,16 which that found the frequency of APE could impact the venous hemodynamics of lower extremities. In Li et al.‘s study, 15 fast-frequency APE could yield faster blood flow velocity in the femoral vein. Similarly, Shimizu et al 13 reported that with a novel leg exercise apparatus, passive APE at 60 times/min was more effective in increasing venous reflux than that at 30 times/min. While in Nakayama et al.‘s study, 16 compared with a frequency of 40 or 80 times/min, APE at 60 times/min was more effective. The inconsistency among the existing studies might come from the different research subjects, different ways of measuring the venous hemodynamic, and different sample sizes, further indicating the necessity of future research in this field.
In our study, all the participants performed both traditional APE and selected APE in different orders. Most of the participants (82.1%) reported that they preferred APE at 30 times/min. After 5 minutes of traditional APE, they rated the scores of RPE representing their fatigue as 12 (10, 13), while after 5 minutes of selected APE the scores of RPE were 10 (8, 11). However, in Li et al.‘s study, 15 when performing the APE at 30 times/min and the score of RPE reached 16 (the corresponding fatigue was tired), the exercise duration among patients with upper limbs damaged was 3 minutes and that among patients with lower limb fracture was 2 minutes. The differences might be due to our study’s sample of healthy young adults. In this study, participants felt less fatigue when performing selected APE than traditional APE, indicating that they were prone to fatigue when keeping the plantarflexion and dorsiflexion for 10 seconds than performing continuous ankle movements.
Since it was argued that APE did not require anything other than patients’ willingness to perform exercises at a regular pace, 6 combined with the recommended time of 5 minutes and the investigation of the participants’ preferences, from the evidence by now, we would like to recommend a frequency of 30 times/min. However, there are many unsolved problems such as the exercise internal; more studies focused on this area would be helpful for the nurses to give optimized APE instruction. Moreover, randomized trials to test the utility of APE as well as combined pharmacological and/or mechanical prophylaxis in patients would be valuable for the DVT prevention. 22
Strengths and Limitations
Our study has several strengths. First, the study applied a randomized cross-over design, which could reduce the influence of individual differences on intervention factors. Second, to evaluate the effects of APE comprehensively, the study measured both the diameters and blood flow velocities of the external iliac vein, femoral vein, and popliteal vein as the physical index, also the subjective feelings of the participants (fatigue of the lower extremity). Third, a sample size of 307 with good compliance could improve the accuracy of the results.
However, there are also some limitations in this study. First, the study was applied to healthy female adults with an average age of 20 (SD=1) years, limiting its generalization to the elderly and patients. Second, in this study we only explored the impact of APE on the venous hemodynamics; there might be other effects on biochemistry factors such as plasminogen activation and factor-VIII increase 23 caused by APE, more studies are needed to explore the mechanism of APE in preventing thrombosis. Third, because of the difficulty in accurately measuring the diameters and velocities of veins during exercise, the study only measured the peak systolic velocities and the internal diameters of the veins immediately after exercise. Future studies should enroll participants in the patients, especially those with orthopedic surgery and apply new methods measuring the venous hemodynamics of lower extremities.
Conclusion
Nurses are assumed to take the responsibility to instruct the patients and the public to perform APE to prevent DVT. Based on our study, both traditional APE at 3 times/min and selected APE at 30 times/min could increase venous blood flow in lower extremities, and no difference was found between the effects of the two APEs. However, participants reported less fatigue when performing APE at 30 times/min, which might promote the patients’ compliance. Therefore, this study provides healthcare professionals evidence that the APE performed at 30 times/min would result in more patient adherence. Additional studies on the patients would help to confirm these findings.
Footnotes
Acknowledgments
The authors gratefully thank the participants enrolled in this study and the staff of the Ultrasonography Department for their assistance in measuring the statistics of the venous hemodynamics.
Author Contributions
All authors had made substantial contributions to conception and design. HYL, QSL, JPW and YRZ collected the data and conducted statistical analyses. WZ drafted the manuscript. HYL, LJZ and LSZ critically revised the manuscript. All authors have given final approval of the version to be published. Each author has participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Shanghai Nursing Peak Discipline, 18QPBJ07, Shanghai Nursing Association, 2019MS-B18 and Changhai Hospital Affiliated to Naval Medical University, 2019YXK040.
Ethical Approval
The study protocol was approved by the Shanghai Changhai Hospital Ethics Committee (CHEC2019-080). The potential participants were given the details of the study and it was made clear that their participation or non-participation was voluntary and would have no impact on them. Informed consent was obtained from all the participants.
Data Availability
The datasets used during the current study are available from the corresponding author on reasonable request.
Trial Registration
Chinese Clinical Trial Registry No. ChiCTR2100042776.