
Abstract
For apparently healthy pregnant women, regular physical activity is recommended. The American College of Obstetricians and Gynecologists (ACOG) created recommendations for physical activity and exercise during pregnancy in 1985. At that time, pregnant women were advised to not exceed a heart rate of 140 beats per minute with physical activity. The heart rate recommendation was subsequently removed with the recommendations published in 1994, 2002, and 2015. In 2020, the ACOG updated its recommendations on physical activity for pregnant and postpartum women. The recommendation included exercising at a “fairly light to somewhat hard” perceived intensity and at less than 60–80% of age-predicted maximum heart rate, usually not exceeding a heart rate of 140 beats per minute. Women often seek advice from healthcare providers on physical activity during pregnancy, yet providers report concern about giving appropriate physical activity guidance. This paper summarizes the key scientific literature on monitoring absolute and relative exercise intensity in relation to the current ACOG recommendations, providing background on intensity-related concepts used in the recommendation. This paper also provides practical guidance to assist healthcare providers in relaying this information to pregnant women.
“...monitoring intensity during regular exercise consistently can help pregnant women identify when a change happens...”
During pregnancy, women who are physically active can derive numerous benefits, such as prevention of excessive gestational weight gain and gestational diabetes mellitus; decreased risk of preeclampsia; and reduced length of labor and incidence of lower back pain.1,2 Uncommon acute risks of physical activity during pregnancy include hyperthermia, musculoskeletal injury, and reduced uteroplacental blood flow that could injure the fetus or cause fetal growth restriction.2,3 Yet, despite the supportive evidence for physical activity, pregnant women from the United States are insufficiently physically active during pregnancy.4,5
Women often seek guidance about physical activity during pregnancy from their healthcare providers6,7,8; those who seek advice are more likely to report exercising during pregnancy, particularly in the later stages.9,10 However, some pregnant women characterize provider advice about physical activity as overly conservative, vague, and confusing.6,7,11,12,13,14,15,16,17,18 This is not surprising, given that providers report concern about giving appropriate physical activity guidance.19,20
Exercise Intensity Recommendations from ACOG, 1985 to 2020.
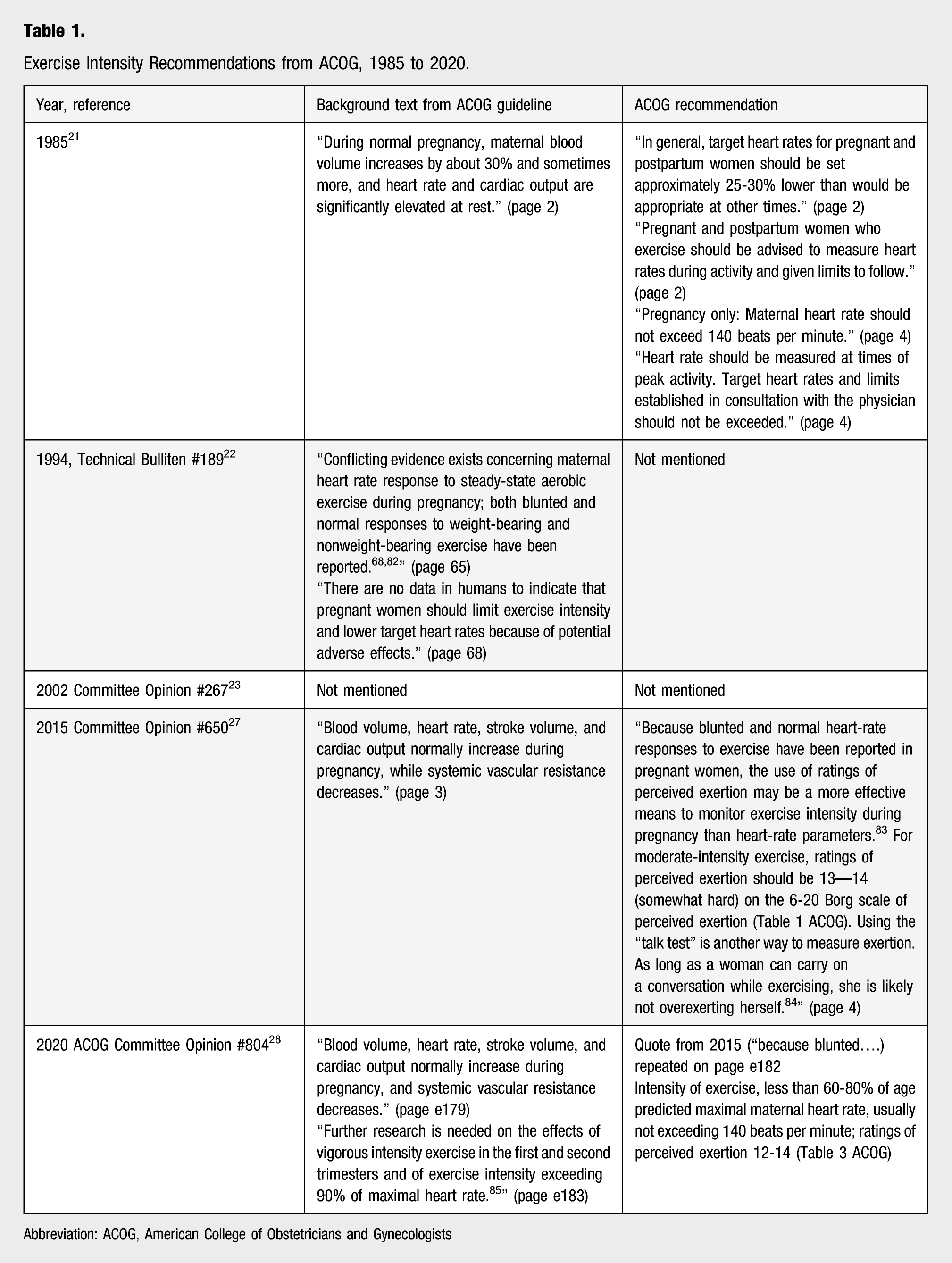
Abbreviation: ACOG, American College of Obstetricians and Gynecologists
The heart rate recommendation was removed in the next update from ACOG in 1994 22 and in 2002. 23 Despite the removal of heart rate recommendations, healthcare providers continued giving advice from the 1985 ACOG guidelines using the heart rate restriction of 140 bpm.7,8,11,19,24,25,26 For example, in a small study, 67% of physicians self-reported that heart rate should stay below 140 bpm several years after the restriction was removed. 25 In the 2015 updated guidance, the use of perceived exertion was supported with moderate intensity physical activity allowed. 27
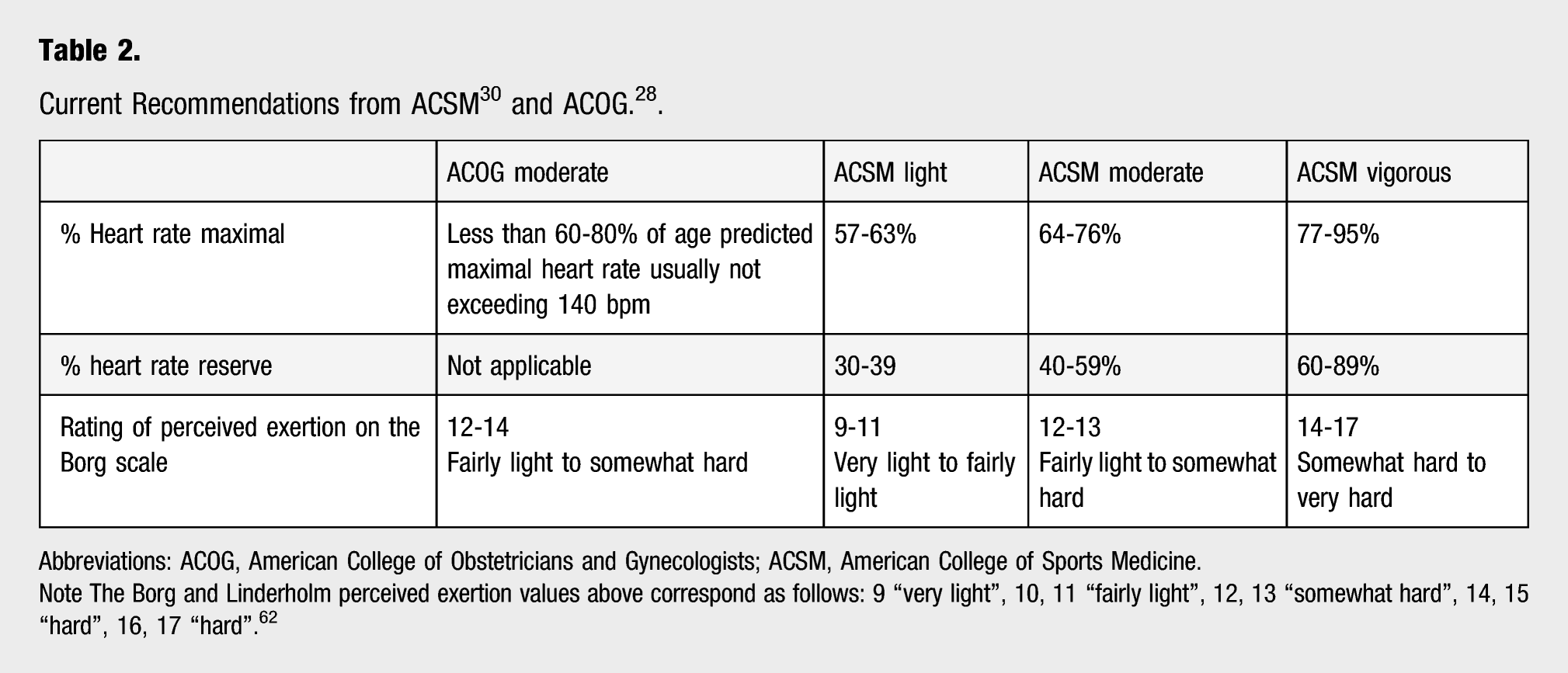
Abbreviations: ACOG, American College of Obstetricians and Gynecologists; ACSM, American College of Sports Medicine.
Note The Borg and Linderholm perceived exertion values above correspond as follows: 9 “very light”, 10, 11 “fairly light”, 12, 13 “somewhat hard”, 14, 15 “hard”, 16, 17 “hard”. 62
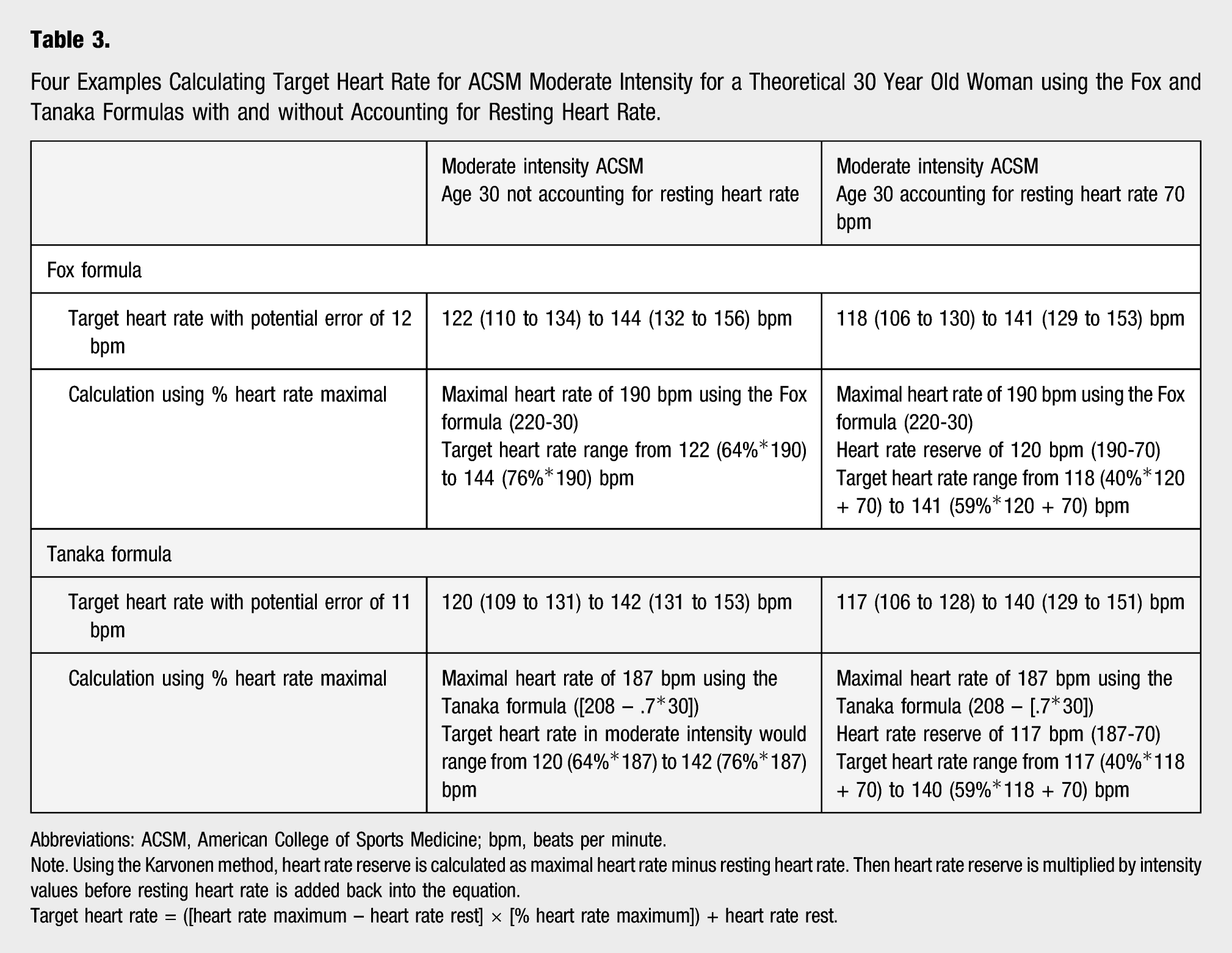
Four Examples Calculating Target Heart Rate for ACSM Moderate Intensity for a Theoretical 30 Year Old Woman using the Fox and Tanaka Formulas with and without Accounting for Resting Heart Rate.
Abbreviations: ACSM, American College of Sports Medicine; bpm, beats per minute.
Note. Using the Karvonen method, heart rate reserve is calculated as maximal heart rate minus resting heart rate. Then heart rate reserve is multiplied by intensity values before resting heart rate is added back into the equation.
Target heart rate = ([heart rate maximum – heart rate rest] × [% heart rate maximum]) + heart rate rest.
Differences between guidelines can cause confusion for both healthcare providers and pregnant women. For example, the 2018 Physical Activity Guidelines for Americans 31 and the 2020 World Health Organization Guidelines on Physical Activity and Sedentary Behavior 32 do not include target heart rates for pregnant women. Moreover, the 2019 Canadian guidelines for pregnancy provide heart rate recommendations during physical activity, but they differ from those of ACOG by taking account of age and intensity. 33 This paper addresses the 2020 ACOG intensity recommendation 28 by summarizing the key scientific literature on the use of heart rate and perceived exertion to monitor exercise intensity during pregnancy. The overarching goal is to try to assist healthcare providers as they counsel women on their physical activity and exercise intensity during pregnancy.
Physical Activity Intensity
Physical activity is any bodily movement produced by skeletal muscles that results in energy expenditure.30,31 Exercise is not synonymous with physical activity, but rather is a component of physical activity that is planned, repetitive, and structured. As stated, key components of physical activity include frequency, duration, time, type, and intensity. This paper focuses on intensity or the magnitude of effort required to perform a given physical activity, which can be expressed in either absolute or relative terms. 31 Absolute intensity is based on the work that is being performed, expressed as a metabolic equivalent (MET). It does not consider an individual’s cardiorespiratory fitness, which may be higher or lower than the assigned MET value of an activity. In contrast, relative intensity, expressed as a percent of maximum aerobic capacity, accounts for cardiorespiratory fitness and is assessed based on measured oxygen uptake, heart rate, or perceived exertion. The ACSM recommends that exercise intensity is prescribed using either absolute (MET values) or relative (oxygen uptake, heart rate, and perceived exertion) values. 30 Absolute intensity can be imprecise and oxygen uptake is often not available or unfeasible to measure, which is likely why the ACOG suggests monitoring intensity based on heart rate and perceived exertion, 28 which we review here.
Relative Intensity Estimation Using Heart Rate
As background, heart rate increases linearly with oxygen uptake until near maximal effort, making it a reasonable indicator of exercise intensity. 34 In the absence of a recent maximal exercise test to provide maximal heart rate, a number of formulas can be used to estimate maximal heart rate. Several formulas are predicated on maximal heart rate declining with age in a linear fashion.35,36 Derived in 1971, the first equation is the widely used Fox formula based on (220-age). 37 In 2001, Tanaka et al. 38 performed a meta-analysis of 351 studies and derived an alternative predictive formula for maximal heart rate: (208 – [.7 * age]). When the Fox and Tanaka formulas were rigorously evaluated among 762 sedentary adults with maximal bicycle exercise tests, maximal predicted heart rate from both the Fox and Tanaka formulas correlated ∼.60 with measured heart rate at maximal effort. 35 There was a larger error among Blacks and those with older age, lower cardiorespiratory fitness, and higher body mass indices. The ACOG recommendations indicate the use of “age-predicted maximum maternal heart rate” which can be derived using either the Fox or Tanaka formulas.
Calculation of exercise intensity can be performed with or without accounting for resting heart rate. The estimation formula accounting for resting heart rate before the intensity values are assigned is the Karvonen formula or heart rate reserve method.39,40 There is discrepancy in the literature as to whether accounting for resting heart rate more closely corresponds to submaximal aerobic capacity than not accounting for it. Based on a review of studies conducted from 1966 to 2010, the Karvonen formula was recommended over other alternatives. 41 In a large study of adults, exercise intensity based on estimated heart rate reserve (i.e., difference between resting and maximal values) was compared to the use of measured heart rate at maximum effort. 42 Not surprisingly, given the prior findings on the evaluation of the Fox and Tanaka formulas, 35 large inter-individual variability was found. Based on this variability, the authors indicated that “using a standard and unique formula to predict aerobic exercise intensity can yield relatively high error in a single subject… and should raise the question of whether relying on the currently recommended equivalence between heart rate reserve and percent of oxygen uptake reserve to prescribe and monitor aerobic exercise intensity is still acceptable.” 42 Nevertheless, when accounting for resting heart rate (e.g., heart rate reserve) while using the Fox or Tanaka formulas for maximal heart rate, the recommended heart rate ranges should be calculated at a lower percent range (Table 2).
The ACSM defines intensity differently depending on the use of percent of maximal heart rate or heart rate reserve (e.g., Karvonen formula) (Table 2). 30 The ACSM recommends the use of heart rate reserve over percent of maximal heart rate to calculate exercise intensity, 30 assuming that maximal heart rate was obtained from a maximal exercise test. While a maximal test is the best method for assessing maximal heart rate, this is not recommended in pregnant women. 43 Using alternative regression formulas to estimate maximal heart rate (examples provided in Ref. [30]) instead of a maximal exercise test can provide greater accuracy than relying on the Fox or Tanaka formulas. Examples of the formulas applied to a theoretical woman 30 years of age are provided in Table 3. Based on our examples, target heart rates vary slightly depending on the method used with a higher range for percent of maximal heart rate (122–144 bpm) compared to percent of heart rate reserve (118–141 bpm).
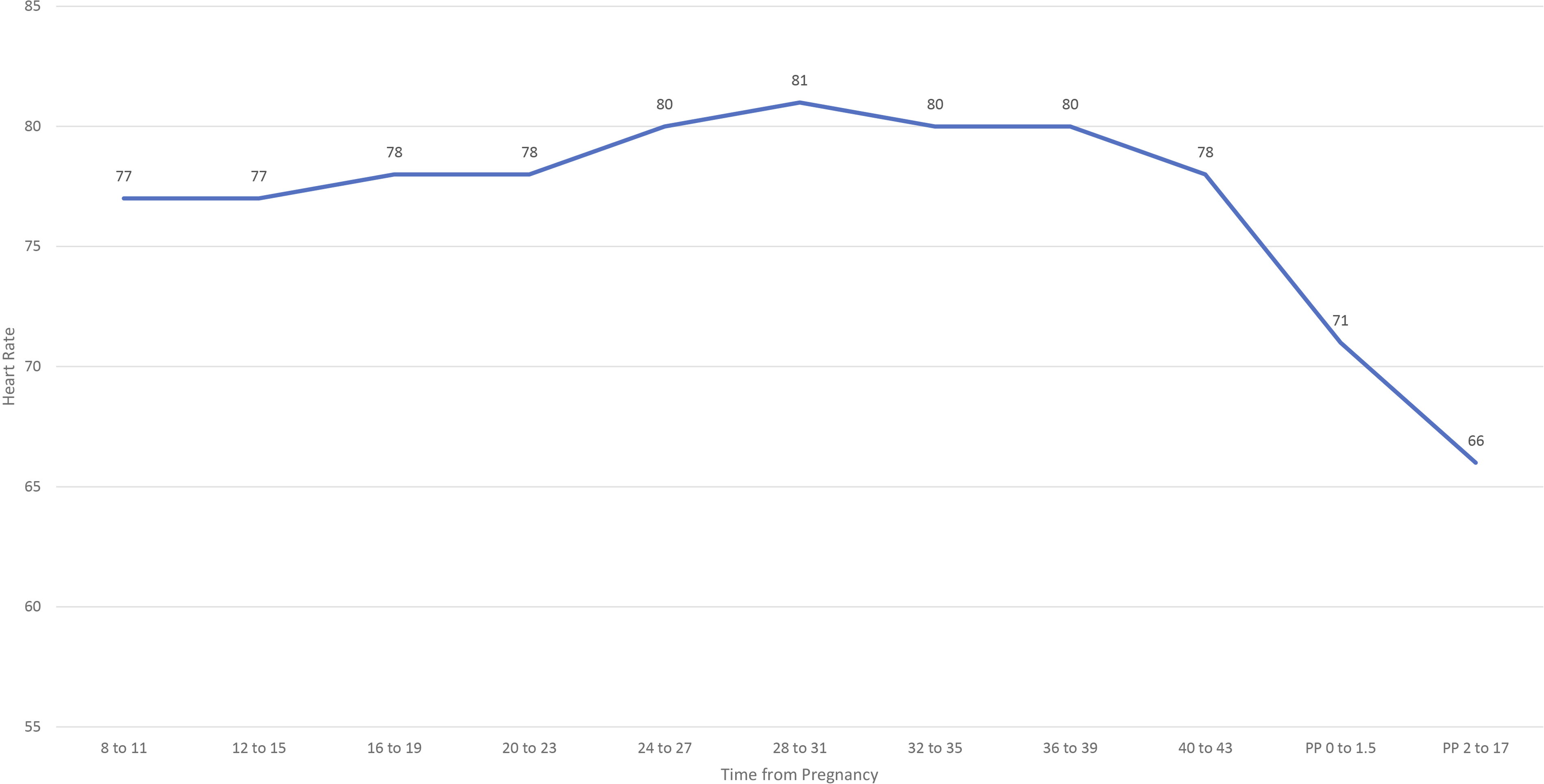
In pregnancy, studies conducted as early as 1938 found resting cardiac output (stroke volume multiplied by heart rate) to be higher in pregnant women than when not pregnant.44,45 In 1966, a prospective study reported on cardiac output and heart rate measured up to 9 times for 30 women from 8 weeks’ gestation to 17 weeks’ postpartum.
45
Average resting heart rate rose from early pregnancy to delivery by 10 to 20 bpm and, following delivery, dropped to a level lower than during early in pregnancy (Figure 1). In 1985, Clapp
46
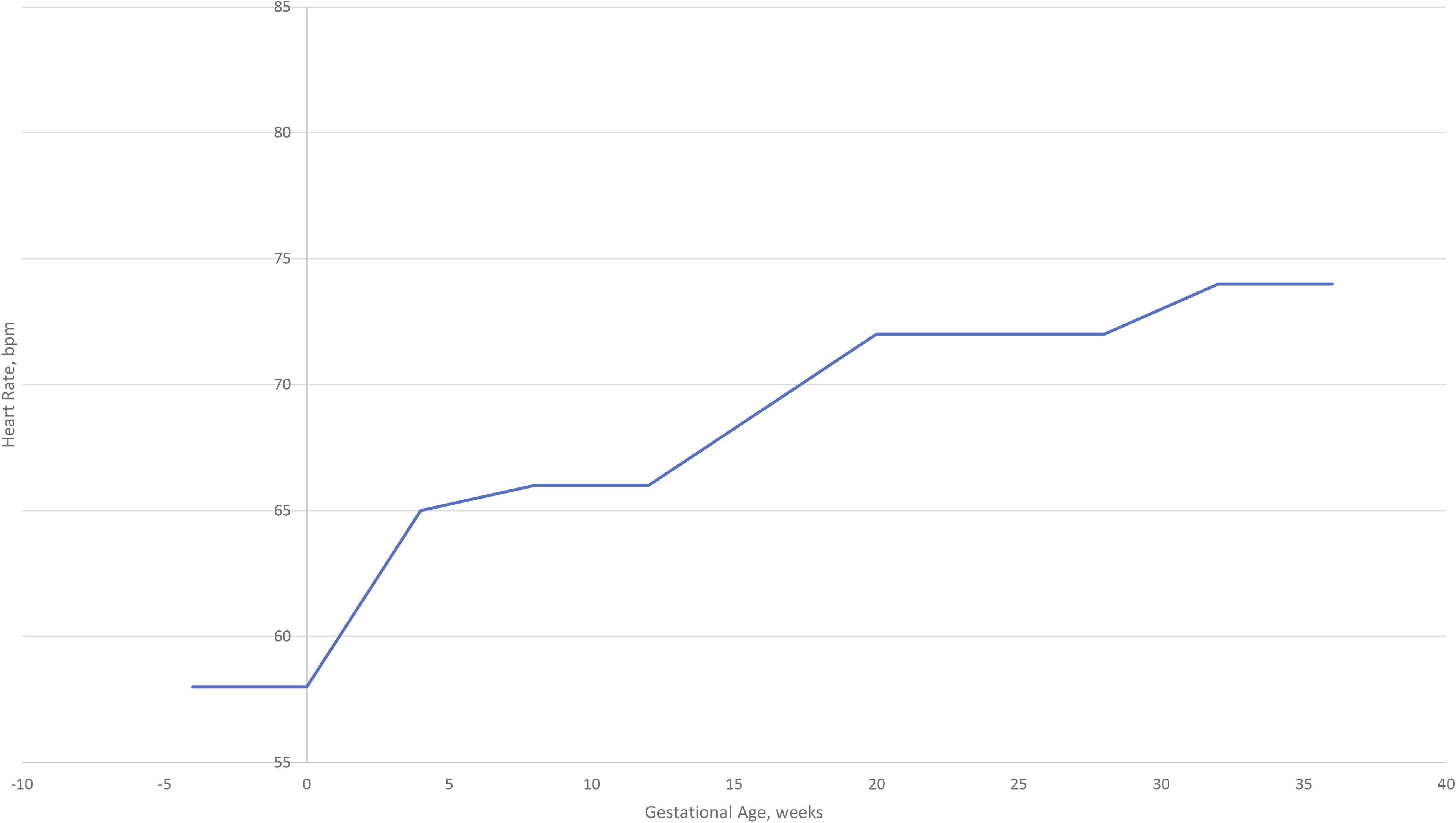
documented resting heart rate upon awakening for 10 pregnant women who ran prior to and during pregnancy. Mean resting heart rate was 7 bpm higher at 4 weeks’ gestation compared to pre-pregnancy. Resting heart rate gradually increased to 32 weeks’ gestation and then plateaued for the remainder of pregnancy. Overall, on average, women’s resting heart rate increased 16 bpm from pre-pregnancy to delivery (Figure 2). This finding has been substantiated in other studies.47,48 Plot of mean heart rate (bpm) among women serially measured throughout pregnancy and postpartum (n = 18)*; Abbreviation: bpm, beats per minute; PP, postpartum. *The data were plotted using mean heart rate provided in Table 1 of the study.
45
Plot of mean resting heart rate (bpm) among women runners serially measured before and during pregnancy (n = 10)*; Abbreviation: bpm, beats per minute. *The data were plotted using mean heart rate provided in Table 1 of the study.
46
These early study findings are supported by more recent work indicating early hemodynamic changes with pregnancy, starting around 2–5 weeks’ gestation. 49 During submaximal weight-bearing and non–weight-bearing exercise, measures of oxygen uptake, stroke volume, and heart rate are higher during pregnancy compared to non-pregnant states.47,50 In a small study of active women, heart rate during the same level of submaximal exercise was on average ∼8 bpm higher in third trimester pregnant women compared to non-pregnant controls, but was similar at maximal effort. 48 Others have reported that maximal effort heart rate may be reduced due to the blunted sympathetic nervous system response to exercise late in pregnancy. 51 A target heart rate range appropriate before pregnancy could meaningfully differ with the autonomic balance shift toward increased sympathetic control and away from parasympathetic control.47,50,52
Due to a higher resting heart rate, functional heart rate reserve at rest and submaximal exercise are reduced during pregnancy. 43 Heart rate reserve will be lower due to the higher resting heart rate and lower maximal heart rate. This results in heart rate becoming a less precise tool for monitoring intensity since it may underestimate intensity at higher work rates and overestimate intensity at lower work rates. 43 Based on the variation found in adults,35,42 the implications for pregnant women are that exercise intensity based on heart rate estimated from age alone, or age and resting heart, is likely to have substantial error.
To demonstrate the challenges specifically with the heart rate recommendations, Figure 3 plots target hearts rates for pregnant women 20 to 40 years of age from ACOG 2020
28
and from ACSM using heart rate maximum and heart rate reserve,
30
with resting heart rates of 60, 70, and 80 bpm. Several observations regarding target heart rate can be made. There is variation in both moderate and vigorous target heart rates across the 5 examples. Considering percent of heart rate using the Fox formula, ACOG recommends 60% while ACSM recommends 64% for the lower bound of moderate intensity. Moreover, the 140 bpm restricts heart rate moreso for younger women who generally have higher maximal heart rates than older women. The heart rate cap also restricts women with higher resting heart rate compared to a lower resting heart rate. For a younger woman with a resting heart rate of 80 bpm, she would be most limited by the ACOG heart rate cap, only reaching to around the median of the heart rate range. At 140 bpm, most pregnant women would not reach vigorous intensity unless deconditioned. In addition to these observations, it seems prudent to highlight that the heart rate recommendations should be reconsidered among women taking beta-blockers or other medication that alters heart rate. In this case, the maximal heart rate will be lower, and inappropriately calculated using the Fox or Tanaka formulas. Heart rate recommendations during moderate and vigorous exercise by age from ACSM
30
for adults and ACOG
28
for pregnant women; Abbreviations: ACOG, American College of Obstetricians and Gynecologists; ACSM, American College of Sports Medicine; BPM, beats per minute; HRR, heart rate reserve using Karvonen formula; HRmax, heart rate using Fox formula (220-age).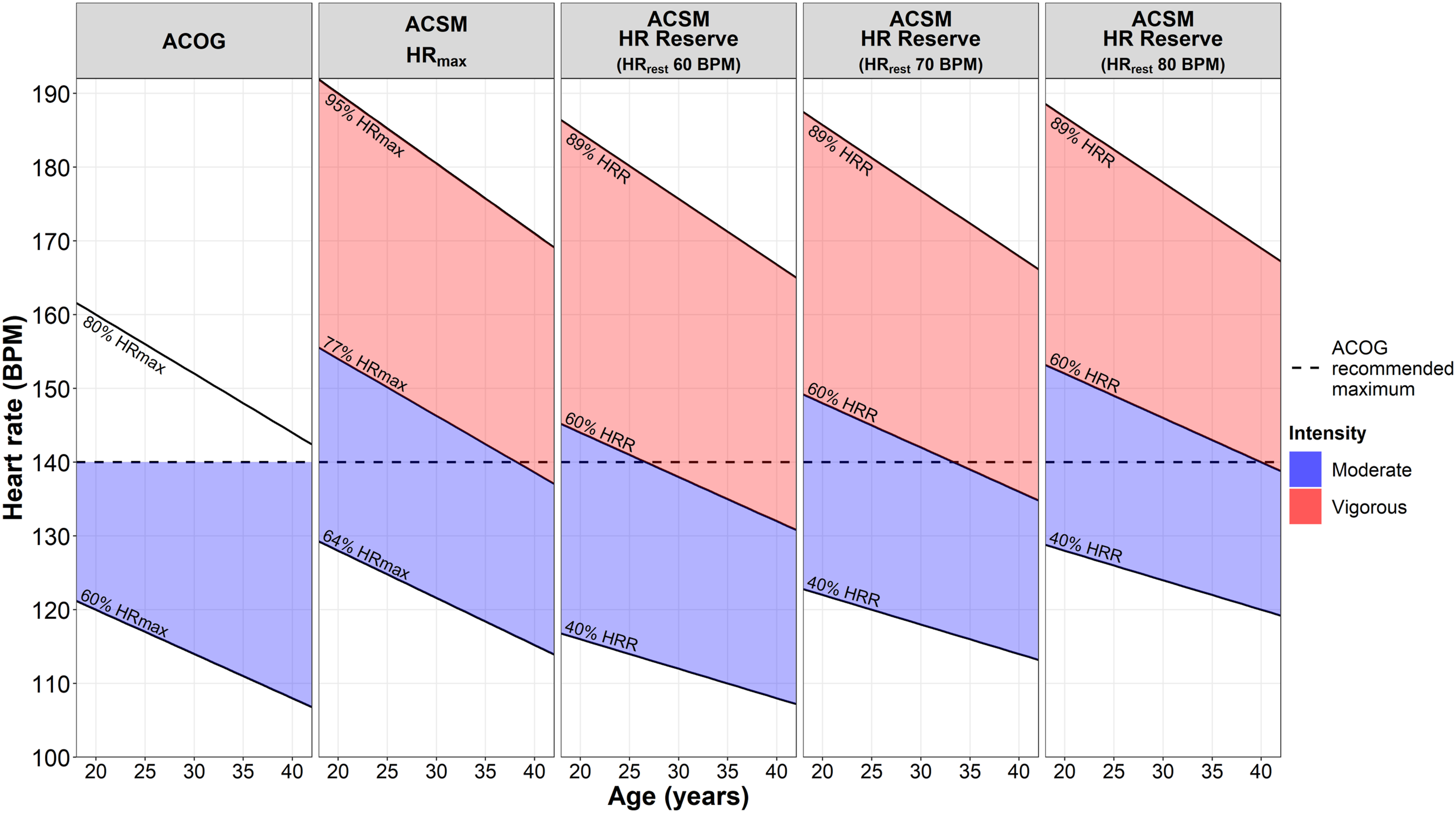
Measuring Heart Rate
Self-assessment of heart rate is an important consideration with the ACOG heart rate recommendation. 28 The most common options a pregnant woman have for measuring heart rate include (i) palpitation, (ii) wearing a device (e.g., activity tracker, smartwatch, and pulse oximeter), or (iii) using a device (e.g., smartphone). First, palpitation is a method usually conducted at the radial artery on the wrist, rather than the carotid artery at the neck, to avoid possible syncope particularly during exercise. It can be difficult to palpitate and count heart rate for at least 10 seconds while exercising.
Second, wearing a device offers the option to collect and usually store heart rate over an extended period of time, both at rest and exercise. For many years, chest straps were the best option for measurement. The advantages to a chest strap included their accuracy and lower cost, but the disadvantages include slipping, discomfort over longer periods of time, and not providing a reading when not in direct contact to the body. The strap often needed water between its surface and the skin to read correctly.
An alternative to the chest strap is the wrist band. It has gained popularity in recent years since heart rate assessment is integrated into activity trackers and smartwatches. 53 The wrist bands use contact photoplethysmography (PPG) to estimate heart rate by utilizing differential reflection of light-emitting diodes in response to the pulsatile changes in blood volume near the skin surface with each heart contraction.54,55 In a review of 5 studies documenting the validity of heart rate assessment on Garmin activity trackers, agreement with the gold standard measure was not optimal; the Garmin performed better at rest compared to higher intensity activities. 56 Other wrist-worn brands indicate similar variability when using PPG for heart rate estimation.57,58 Emerging options for heart rate assessment creatively utilize headphones, rings, clothing, or pulse oximetry.
Third, consumers can use smartphone apps that measure heart rate, also assessed with PPG. In this case, the process utilizes the phone’s camera and flash to detect changes in blood volume near the skin’s surface. Apps that required contact (such as touching your fingers) to the phone’s camera tend to be more accurate than noncontact apps that request holding the camera to your face. 59 Apps are also more accurate when the individual is in normal sinus rhythm compared to rhythms with irregular rate or tachycardia. 60 Limitations of this method include variation in heart rate assessment due to skin tone, ambient light, user movement, finger pressure, and lower than optimal sampling rate of the phone. 53 Other smartphone options include (i) mobile phone apps combined with accelerometry using the seismocardiogram and the ballistocardiogram signals 61 and (ii) mobile phones with an electrocardiogram sensor and app to assess heart rate through the handheld electrocardiogram recorder. 53
Relative Intensity Estimation Using Perceived Exertion
The original ratings of perceived exertion scale approximates exercise heart rate from 6 (i.e., 60 bpm) to 20 (i.e., 200 bpm) 62 ; predicted heart rate is in essence based on the numeric rating of perceived exertion multiplied by 10. The ACSM provides recommendations for ratings of perceived exertion using the Borg scale, summarized in Table 2. 30 Although describing exercise based on perceived exertion can be useful since it allows an approximately equivalent work-rate in individuals who have differing baseline fitness or exercise capabilities, 63 it is not without challenges.
Studies in non-pregnant populations suggest that perceived exertion may be both under- and over-estimated based on intensity level. For example, among 343 women aged 40–91 years, estimates of perceived intensity were higher for light and vigorous physical activity, but lower for moderate physical activity compared to absolute intensity based on MET values from a compendium of physical activities. 64 The mismatch was largest with vigorous physical activity. A similar mismatch was observed at higher intensities, where women and men correctly estimated light intensity effort during a treadmill walk, but underestimated walking at moderate and vigorous effort. 65 When participants were asked to walk at a pace to benefit health, about half (52%) walked at light intensity, with fewer walking at moderate or vigorous intensity. Results did not differ by sex, ethnicity, or body mass index, but younger adults (<30 years old) underestimated moderate and vigorous intensity to a greater extent than middle-aged adults (≥30 years old). Another study indicated that mismatches between perceived and measured intensities may differ by level of training; at 50–80% of maximal oxygen consumption, trained runners on average exhibited a lower level of perceived exertion compared to untrained runners. 66
Perceived exertion is one way in which pregnant women are now recommended to monitor their physical activity intensity during pregnancy. However, the range of intensity that ACOG 28 recommends for moderate intensity (RPE 12 to 14) spans moderate (RPE 12–13) to vigorous (14–17) intensity activity using the Borg scale 62 according to the ACSM guidance (Table 2). 30 The Borg scale 62 defines a RPE of 11 as “fairly light,” 13 as “somewhat hard,” and 15 as “hard.” Changes to a woman’s physiology during pregnancy, her baseline pre-pregnancy cardiorespiratory fitness, and the type of activity performed may all make it difficult for women to accurately predict both perceived and actual exertion during pregnancy.
As with resting heart rate, the energy costs for any given physical activity are higher during later pregnancy compared to earlier in pregnancy 67 or compared to 12 weeks’ postpartum. 68 This may imply that women perceive physical activity to become more difficult as pregnancy progresses, but study findings vary as to whether this is the case. On an incremental step-test, perceived exertion for pregnant exercisers was higher compared to non-pregnant controls, 69 and another study found women perceived physical activity to be more difficult at 32 weeks’ compared to 20 weeks’ gestation relative to the energy cost. 70 In contrast, no differences in perceived exertion at either 20 or 32 weeks’ gestation were found at either moderate or vigorous intensity treadmill exercise when exercisers and sedentary women performed 5 minutes at self-selected speeds. 70 Other studies also show that perceived exertion remains unchanged during pregnancy for moderate intensity cycling,69,71 and in response to a fixed load on a treadmill and cycle ergometer. 72
It is possible that while perceptions may not change during pregnancy, women alter their physical activity intensity as pregnancy progresses either consciously or otherwise as shown by Marshall and Pivarnik. 70 In their study, women who were told to exercise at a vigorous intensity on a treadmill task did so at 20 weeks’ gestation but did not at 32 weeks’, with energy expenditure measurement accounting for their treadmill speed and grade. This is similar to a small sample of pregnant women who reported a change in self-paced walking over the course of pregnancy, 73 and another study showing slower walking paces in obese women combined with reductions in the metabolic cost of walking from 15 to 30 weeks’ gestation. 74 Women who were 32 weeks pregnant also had lower activity energy expenditure, performed less total physical activity, and walked at a slower pace compared with non-pregnant controls. 75 It may, therefore, be inferred that earlier in pregnancy, a woman’s perception of what constitutes moderate and vigorous intensity does not differ, but this changes as pregnancy progresses; pregnant women may compensate for physiological changes during gestation by decreasing walking and running speeds. More research is required to determine whether this mis-match between “perception and reality” has important physiological implications. It may however be something for providers to bear in mind when recommending activity in later gestations; women who remain active will do so at an intensity comfortable to them, with the decreased effort potentially being a natural and important mechanism for engaging in safe physical activity during pregnancy.
Maternal heart rate increases during exercise as pregnancy progresses at a given workload, regardless of perceived exertion. 76 However, no significant correlation between heart rate and perceived exertion in 20 pregnant women was found, where perceived exertion was higher at 15 and 30 minutes during resistance vs aerobic exercise. 77 It is likely that in those who exercise prior to pregnancy, perceived exertion is less than those who were previously sedentary. 70 Moreover, women who performed exercise training throughout gestation had a blunted perception of effort at given cycle power outputs as pregnancy progressed. 78 In trained women, perceived exertion, therefore, tends to underestimate actual heart rate during pregnancy (except for walking in the third trimester), with large underestimations in some cases putting women in higher heart rate zones than recommended by ACOG in 2020. 28 This may support findings that prior exercisers self-select exercise at intensities that are higher compared to previously sedentary women. Indeed, caloric expenditure, alveolar ventilation, and cardiac output responses appear proportionately higher in trained compared to sedentary pregnant women. 79 Trained pregnant women may therefore be at a greater risk of under estimating exercise intensity when using perceived exertion than untrained pregnant women. Others have concluded that pregnant women should not rely solely on perceived exertion when training to maintain an exercise intensity below 140 bpm, 76 the maximal heart rate recommendation from ACOG in 1985 21 and now in 2020. 28
It is suggested that the correlation between perceived exertion and heart rate is less linear during pregnancy compared to the non-pregnant state, 76 and that this relationship may differ by activity type. One study of 124 pregnant women who were trained or sedentary in the second or third trimester showed that heart rate was not correlated with perceived exertion during walking, cycling, circuits, or aerobics. 76 Another found no significant correlation between heart rate and perceived exertion in 20 pregnant women, but that perceived exertion was higher during resistance training compared to aerobic exercise. 77 Ohtake and Wolfe 78 observed perceived exertion to be higher for pregnant women conducting step-testing at the same target heart rate compared to cycling, with women more likely to underestimate their heart rate in the cycling condition. Conversely, pregnant women were shown to work harder, both in terms of perceived exertion and heart rate, when cycling compared to walking. 80 Overall, healthy participants worked at (mean/standard deviation) 65 ± 8% and 76 ± 9% of individual age predicted heart rate maximum during treadmill tasks and static cycling, respectively, indicating the treadmill walking was perceived as “somewhat hard” and stationary cycling “hard.” While no pattern is evident for which activities are likely to result in higher perceived exertion for pregnant women, it may in part depend on what women are used to and also how her body adapts to each specific pregnancy. Nevertheless, it is recommended that providers (a) use perceived exertion as a way of counseling women on how they can be safely active during pregnancy; (b) be aware that activities performed at a given perceived exertion may change depending on trimester; and (c) query how active a woman was, and what types of activity she engaged in, prior to pregnancy.
Practical Application and Conclusion
The earliest United States recommendations on physical activity during pregnancy date from the middle of the 20th century. 81 At that time, the guidelines had little scientific basis and encouraged housework, gardening, occasional swimming, and daily walks, while discouraging sports participation. In 1985, the ACOG provided their first prenatal exercise recommendations based on a consensus panel of obstetricians. 21 This guideline was updated in 1994, 22 2002, 23 2015, 27 and 2020. 28 Healthcare providers should be prepared for some confusion around the 2020 ACOG exercise intensity recommendations 28 since the heart rate restriction was included in the 1985 recommendation 21 but subsequently removed since 1994. 22
Practical Guidance for Monitoring Physical Activity Intensity During Pregnancy.
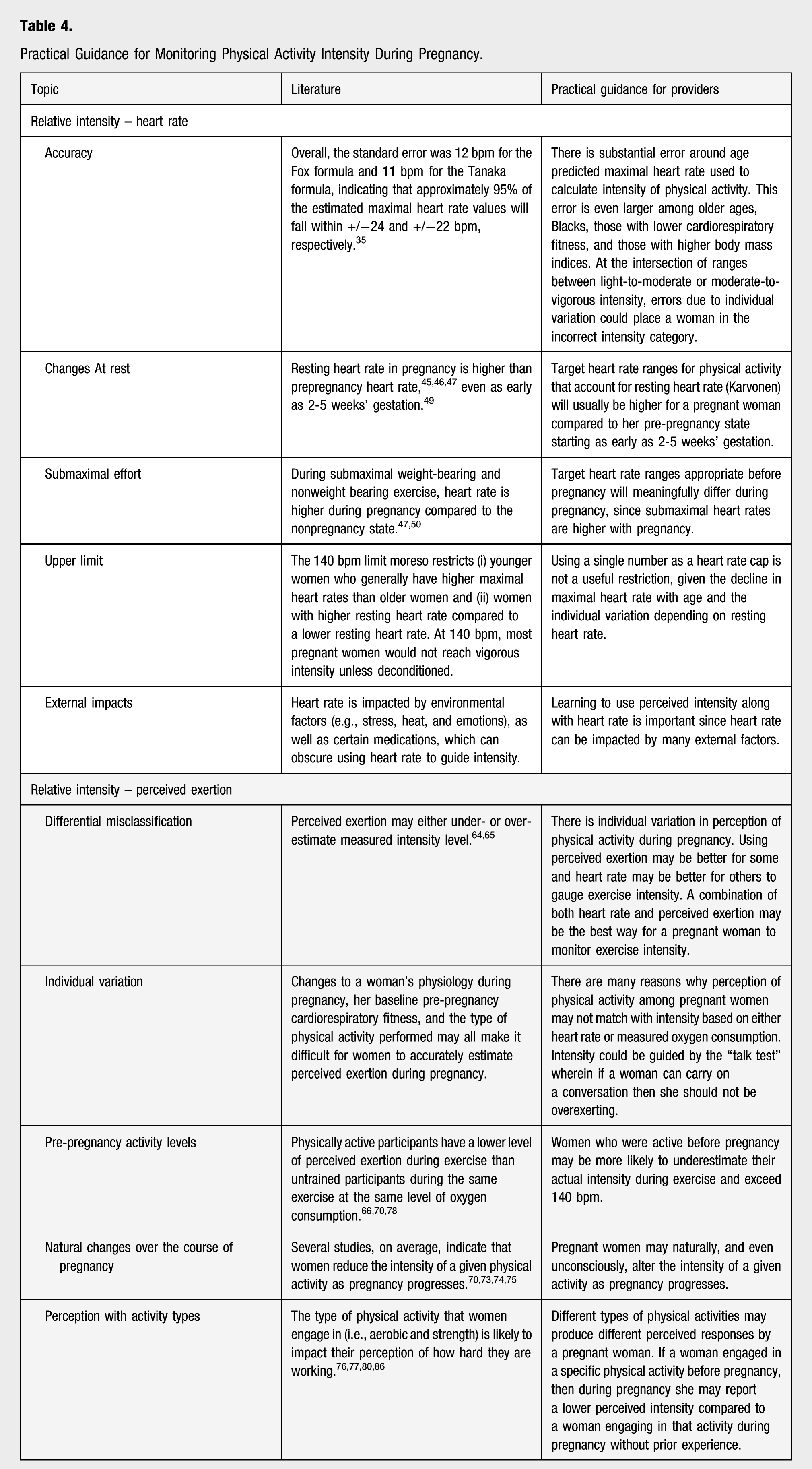
For pregnant women, a combination of both heart rate and perceived exertion may be the current best way to monitor exercise intensity to account for their prior level of training. There are several options for women to self-monitor their heart rate during exercise. Each method has advantages and disadvantages that should be taken into consideration. However, monitoring intensity during regular exercise consistently can help pregnant women identify when a change happens and if there might be a reason to lower their intensity. More research is required to better specify guidance on physical activity intensity throughout pregnancy, considering a range of intensities, ages, cardiorespiratory fitness levels, and body sizes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Evenson acknowledges support by the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health (NIH, #UL1TR000083). Dr Hesketh was supported by the Wellcome Trust (107337/Z/15/Z). The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.