
Abstract
Background
The aim of this study was to construct a system dynamics (SD) model to estimate the future medical care expenditure and to address the dynamic issues of health care that should be resolved. In particular, the measures for promoting the spread of generic drug (GE drug) usage in Japan and reducing cancer-related medical expenses were investigated regarding their future impact on medical finances.
Methods
The SD model was constructed from FY 2018 to FY 2050. The change in the future GE drug quantity share was analyzed by using a regression equation. The impact of the increase in medical expense for cancer and the change in the future national medical care expenditure were also estimated.
Results
The annual total medical care expenditure in FY 2050 would arrive at 58.9–64.2 trillion JPY (US$ 535.1–584.0 billion) (1.3–1.5 times higher than that in FY 2018) with different trends in age groups. The cumulative total medical care expenditure was expected to decrease by about 787.0–989.4 billion JPY (US$ 7.2–9.0 billion) if the impact of the spread of GE drug usage was considered. On the other hand, due to the continuous increase in the cancer-related medical expense, the cumulative total medical care expenditure was estimated to increase about 7554.3–11715.0 billion JPY (US$ 68.7–106.5 billion).
Conclusions
If the cancer-related medical expense continues to increase in the future, an increase of 686.4–1104.2 billion JPY (US$ 6.2–10.0 billion) in FY 2050 is expected which suggests that this disease field should be prioritized regarding the measures to maintain medical finances.
Keywords
Highlights:
What do we already know about this topic?
Japanese society is facing marked changes due to the aging population and the concomitant rapid increase in the national medical care expenditure, resulting in tight medical finances.
How does your research contribute to the field?
This research quantified the magnitude of the impact of the measures for promoting the spread of GE drug usage and reducing cancer-related medical expenses in future medical finances under the national health insurance (NHI) system in Japan by using a constructed system dynamic model.
What are your research’s implications toward theory, practice, or policy?
The decrease expected by taking the measures for the spread of GE drug usage was exceeded by the increase of the cancer-related medical expense by more than 10-times which suggests that this disease field should be prioritized regarding the measures to maintain medical finances.
Background
Japan introduced a national health insurance (NHI) system in 1961. The entire nation is guaranteed the right to receive equal medical care if a copayment specified by the national regulations 1 is paid. Technical fees for medical technology and practice are established publicly. Drug prices are determined according to the NHI drug price scheme that was enacted in September 1950. 2
Circumstances surrounding the NHI system are changing. Japanese society is facing marked changes due to the aging population 3 and the concomitant rapid increase in the national medical care expenditure, resulting in tight medical finances. 4 The population aged 65 years or older accounted for 28.14% of the total population in Japan in 2018, being the highest among the Organization for Economic Co-operation and Development (OECD) member countries, and this is 1.6 times higher than the mean (17.20%) of the OECD member countries. In addition, the Gross Domestic Product (GDP) ratio vs national medical care expenditure was ranked 14th among the OECD member countries in 2010, but it became sixth in 2018 (10.9%), reflecting a rapid rate of increase in the national medical care expenditure compared with those in other countries. 5 Based on the above, the national medical care expenditure will continue to increase if the current state continues. Moreover, regarding the condition of Japan’s national finances, the financial deficit is increasing continuously. Indeed, the total expenditure in fiscal (FY) 2014 surpassed the total tax revenue by 46 trillion JPY and more than 40 trillion JPY of the national bond is floated. 6 In response to this situation, the necessity of the reform of the medical care system for the efficient use of limited medical care resources has been indicated.
As a policy aiming at a sustainable NHI system, the full-scale introduction of cost-effectiveness evaluations (termed Japanese Health Technology Assessment [HTA]) started in April 2019 under an initiative by the Ministry of Health, Labour and Welfare (MHLW). 7 The Japanese HTA enables us to evaluate innovations and price them logically in order to promote the efficient usage of limited medical resources.
In order to maintain a sustainable NHI system, it is also important to pursue the efficient allocation of limited medical care resources. Yan et al stated that it is important in decision-making in health care to show information on how to promote patient outcomes while minimizing the burden on health system resources. 8 Australian governments are increasingly mandating the use of cost-benefit analysis considering in monetary terms to ensure efficient use of limited government resource. 9 To design efficient measures to achieve this, it is essential to predict and verify changes in the national medical care expenditure in the future brought by those measures.
The system dynamics (SD) theory was developed in 1956 at the Massachusetts Institute of Technology (MIT), and SD simulation is used in a variety of business settings. SD modeling is suitable to predict the future medical care expenditure because there are many factors10-12 that influence future medical care expenditure. In addition, future medical care expenditure will be influenced by the change in related variables over time. The SD model is simple to analyze for all scenarios by finding patterns of behavior, and evidence-based scenario analysis is highly important to discuss the efficient allocation of medical care resources.
The aim of this study was to forecast the future medical care expenditure in Japan using the SD model and to address the dynamic issues of health care that should be resolved. In particular, the measures for promoting the spread of generic drug usage (i.e., GE drug usage) and reducing the cancer-related medical expenses (i.e., part of the medical treatment expenditure and dispensing pharmacy expenditure), for which an increase in impact on national medical care expenditure is of concern from the viewpoint of the disease field, were investigated regarding their future impact on medical finances. In Japan, “A roadmap for promotion of the use of generic drugs” was formulated by the MHLW in April 2013 as a policy to help improve medical insurance finances and relevant activities are underway.
13
But to our knowledge, there has been no report on quantitative verification of its medical expense-reducing effects in the future. According to the changes of the composition ratio in the medical expense for diseases from FY 2010 to FY 2017 (JPY per capita) (Figure 1),
14
the impact of the cancer-related medical treatment expenditure on the health care finance in Japan is increasing. Also a similar trend was noted in the composition ratio of anticancer drugs in the dispensing pharmacy expenditure.
15
Therefore, in order to contribute to the discussion on how to implement the efficient allocation of medical resources is expected, the extent of the increase in the future was simulated. Medical treatment expense by disease (% per capita).
Method
Model Construction
There are a number of previous studies on future estimates of total medical care expenditure, and it is common to use a forecasting method which breaks the expenses down into population number, medical care expenditure per capita and increase rate of medical care expenditure per year under the Japanese health care system. 16 (Additional file 1). Total medical care expenditure was calculated in each age group; 0–14 years, 15–44 years, 45–64 years and ≥65 years group, and summed as the total medical expenditure. The simulation term was set from FY 2018 (index year) to FY 2050. The population number in each year was expressed as “stock” connected to the “flows,” the number increased (flow-in) and the number decreased (flow-out), controlled by the TIME function set in “converter.” The future population in Japan referred to the 2017 estimation (medium-fertility) from the National Institute of Population and Social Security Research. 17 This is the most reliable data of the future population estimates in Japan, which is used for preliminary calculation to examine various policies. Medical care expenditure per capita in each year (expressed by “stock”) fluctuated according to the increase rate per year (expressed by “converter”). For the increase rate per year, the mean of the increase rates from FY 2010 to FY 2017 (0–14 years group; 2.6%/year, 15–44 years group; 2.2%/year, 45–64 years group; 1.0%/year, and ≥65 years group; .9%/year) was used. 18
Parameter List for the System Dynamics Model Construction.

Scenario 1: Impact of the Spread of GE Drug Usage
According to the “Basic Policy on Economic and Fiscal Management and Reform 2017” (cabinet decision on June 9, 2017), 24 the target ratio of GE drug usage to be achieved by September 2020 is 80%.
The calculation logic of the impact of the spread of GE drug usage on the future medical care expenditure in Japan was expressed using a contributing factor diagram (Additional file 2). The impact of the spread of GE drug usage was incorporated in the “Medical care expenditure per capita.” The parameters that affect the “Medical care expenditure per capita” were “Drug cost rate; proportion of total drug costs in total medical care expenditure,” “GE drug cost ratio; ratio of GE drug prices to the original drug prices,” and “GE drug cost rate; proportion of GE drug costs in total drug costs” expressed by “converter.”
The proportion of total drug costs in total medical care expenditure (i.e., Drug cost rate) was calculated as 13.329% using the data in 2017, 25 and it was assumed to be consistent through the simulation term.
When the original drugs are changed to GE drugs, it was assumed to be reduced to 50% of the costs of the original drugs (i.e., GE drug cost ratio). “GE drug cost rate” was estimated from “GE drug quantity share” using the following equation derived from changes in the GE drug quantity share and GE drug cost rate in the past from FY 2013 to FY 2018;
GE drug cost rate = .2647x–.0151
x; GE drug quantity share
The GE drug cost rate in FY 2018 was estimated as 18.451%.
The GE drug quantity share in FY 2018 (75.9%) 15 was calculated by the following equation; GE drug quantity share = (Number of GE drugs)/((number of original drugs which are substitutable by GE drug) + (number of GE drugs))
The GE drug quantity share in other countries in FY 2018 26 was 92% in the US and 87% in Germany, demonstrating that a spread rate higher than the target value in Japan has been realized in other developed countries. Thus, in this estimation, the GE drug quantity share after FY 2018 was estimated using an estimate equation derived from the past GE quantity share from FY 2013 to FY 2018:
GE drug quantity share = −.0027t2 + .0402t + .7541
(Polynomial approximation, R2 = .9914)
Year 2018 is defined as t = 0
Parameter List for the Scenario 1. (Impact of the Spread of Generic Drug Usage).

GE, generic.
Scenario 2: Impact of the Increase in the Medical Treatment Expenditure and Dispensing Pharmacy Expenditure for Cancer
The changes in the national medical care expenditure were estimated assuming that the current increasing tendency in the medical expense for cancer will continue in the future, and its financial impact was determined.
The calculation logic of the impact of the increase in the medical expense for cancer in Japan was expressed using a contributing factor diagram (Additional file 3). The parameters that affect the “Medical care expenditure per capita” were “rate of the medical treatment expenditure and dispensing pharmacy expenditure,” “rate of cancer-related cost,” and “Year-to-year growth rate of cancer-related cost” expressed by “converter.”
The rates of the medical treatment expenditure and dispensing pharmacy expenditure in the national medical care expenditure in FY 2017 by the age groups were set as follows: 0–14 age group, 69.3 and 19.0%, respectively; 15–44 age group, 64.7 and 19.1%, respectively; 45–64 age group, 69.0 and 19.0%, respectively; ≥ 65 age group, 74.2 and 17.5%, respectively. 18 The rates of cancer-related cost in FY 2017 by age group were as follows: Medical treatment expenditure, 2.9, 9.9, 17.9, and 14.7%, respectively 18 ; dispensing pharmacy expenditure was uniformed to 4.2%. 18 The year-to-year growth rate of cancer-related cost was calculated based on changes from FY 2014 to FY 2017. 18 For the medical treatment expenditure, +.09%, 0% (i.e., flat), +.18% and +.28% were set for the age groups, respectively, and +.26% was uniformly set for the dispensing pharmacy expenditure. Assuming that this growth rate was retained during the simulation period, it was incorporated into the variable for medical care expenditure per capita.
Parameter List for the Scenario 2. (Impact of the Increase in the Medical Treatment Expenditure and Dispensing Pharmacy Expenditure for Cancer).


Simplified model structure. Boxes signify “stocks,” arrows in/out stocks represent “flows” and boxes free represent “converters.”
Sensitivity Analysis
In Scenario 1, GE drug quantity share is set based on the assumption. Also the estimation equation of GE drug quantity share can be affected by the approximation method of a curve. Therefore, we conducted a sensitivity analysis of Scenario 1 based on the following 2 conditions; (condition 1) if the latest reported value of GE drug quantity share (%) (Year 2018: .759) is continued in 2019 and beyond (that is, assuming that GE drug usage does not spread after 2019), and (condition 2) if the estimation equation of GE drug quantity share uses a linear approximation (GE drug quantity share = .0537t + .7632, R2 = .9861).
Results
Model Validation
Our SD model was validated by confirming that population changes in the future are reproduced by SD model simulation based on existing reports. The population estimate in 2050 in Japan published as 101,923,107 (2017 estimation). 17 The population estimate in 2050 in the SD model was 101,923,093 and the difference from the reported population estimate in each year during the estimation period was within ±10−5%, confirming that changes in population in the future can be reproduced by the SD model.
Estimation of Future Medical Care Expenditure
Annual total medical care expenditure in FY 2050 was estimated as 58.9 trillion JPY (US$ 535.1 billion, 1US$ = 110 JPY), being estimated to increase by 1.3 times over 32 years from FY 2018 (43.8 trillion JPY (US$ 398.2 billion)) (Figure 3). The annual total medical care expenditure in FY 2050 was estimated using 2 analysis settings with regard to the increase rate per year (%), i.e., the nominal GDP formula and OECD formula, and the estimates were 59.2 trillion JPY (US$ 537.8 billion) and 64.2 trillion JPY (US$ 584.0 billion), respectively, being estimated to increase by 1.4 and 1.5 times, respectively, over 32 years from FY 2018. At either setting of the increase rates, the annual total medical care expenditure in FY 2050 was 58.9–64.2 trillion JPY (US$ 535.1–584.0 billion) (1.3–1.5 times that in FY 2018). Trend of annual total medical care expenditure. GDP, Gross Domestic Product; MHLW, Ministry of Health, Labour and Welfare; OECD, Organisation for Economic Co-operation and Development.
The trend of total medical care expenditure was different in each age group (Additional file 4). The total medical care expenditure in the ≥65 years group accounted for the highest rate in all FY. The trend in total medical care expenditure in FY 2018–FY 2050 was flat or a slightly increasing in the other 3 age groups, but it continuously increased in the ≥65 years group, reaching the peak in FY 2050, exhibiting an increase by 1.4 times from 26.4 trillion JPY (US$ 240.0 billion) in FY 2018 to 38.1 trillion JPY (US$ 346.4 billion) in FY 2049 in the base case (MHLW formula).
Impact of the Spread of GE Drug Usage
Annual total medical care expenditure in FY 2050 was estimated as 58.8 trillion JPY (US$ 534.6 billion) to 64.2 trillion JPY (US$ 583.4 billion). Compared with the estimated value in FY 2050 without the impact of the spread of GE drug usage, total medical care expenditure was expected to be reduced 53.7 billion JPY (US$ .488 billion) to 70.6 billion JPY (US$ .642 billion) (Figure 4). Impact on the total medical expenditure (MHLW formula). GE, generic; MHLW, Ministry of Health, Labour and Welfare.
The cumulative total medical care expenditure from FY 2018 to FY 2050 was estimated as 1760.9 trillion JPY (US$ 16 007.8 billion) to 1839.9 trillion JPY (US$ 16 726.3 billion). Compared with the estimated value without the impact of the spread of GE drug usage, the cumulative total medical care expenditure was expected to be reduced 787.0 billion JPY (US$7.2 billion) to 989.4 billion JPY (US$ 9.0 billion) (Figure 5). Impact on the cumulative medical expenditure (MHLW formula). GE, generic; MHLW, Ministry of Health, Labour and Welfare.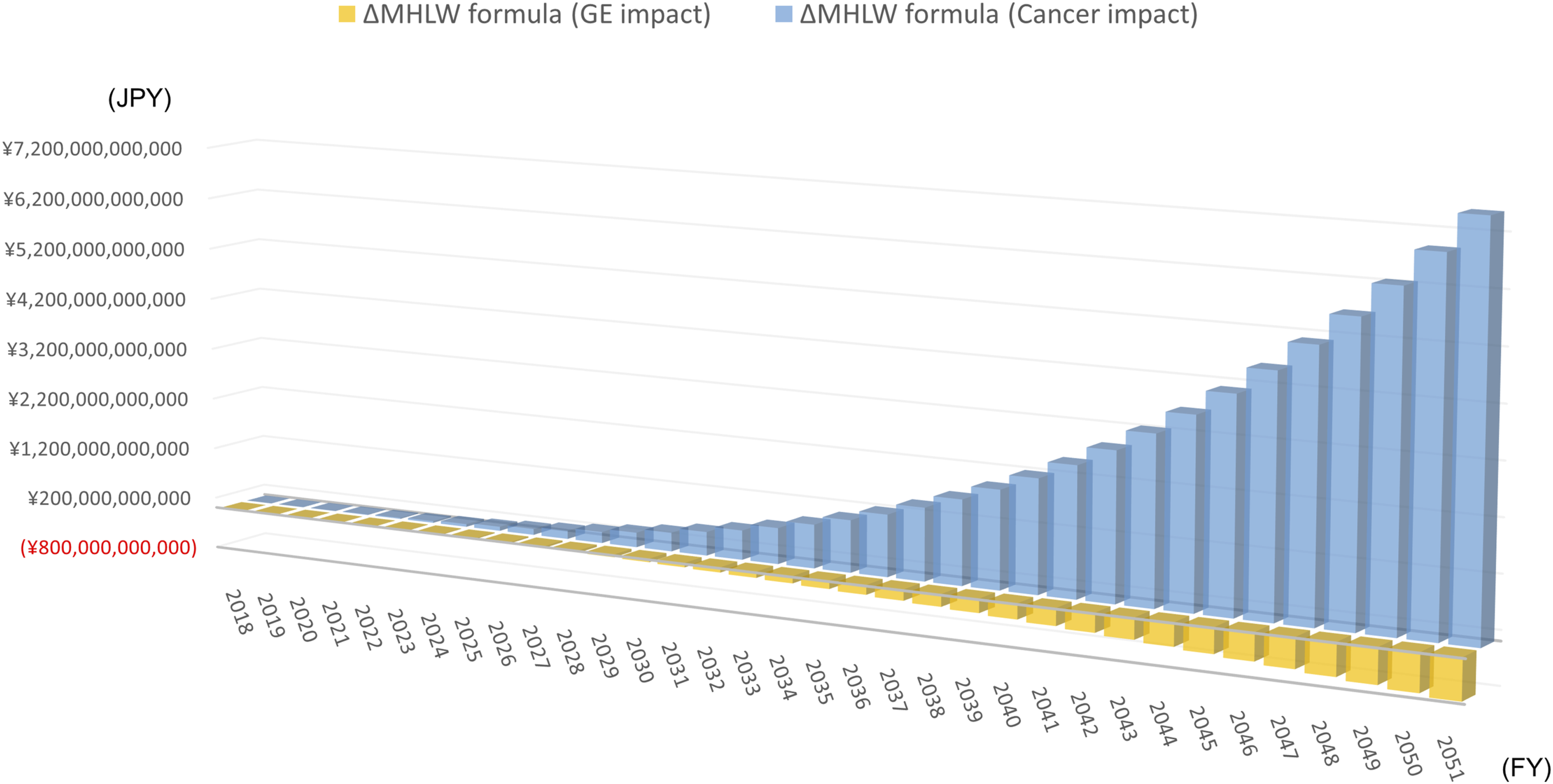
As a result of the sensitivity analysis, in condition 1, compared with the estimated value in FY 2050 without the impact of the spread of GE drug usage, total medical care expenditure and the cumulative total medical care expenditure were expected to be reduced 2.0 billion JPY (US$ 18 million) and 30.8 billion JPY (US$ .28 billion), respectively. In the same way, the saving amount of the medical care expenditure in condition 2 was expected to be 64.6 billion JPY (US$ .59 billion) and 958.8 billion JPY (US$ 8.7 billion), respectively.
The annual total medical care expenditure in FY 2050 was estimated as 59.5 trillion JPY (US$ 541.3 billion) to 65.3 trillion JPY (US$ 594.0 billion). Compared with the estimated value in FY 2050 without the impact of the increase in the medical expense for cancer, the total medical care expenditure was estimated to be increased 686.4 billion JPY (US$ 6.2 billion) to 1104.2 billion JPY (US$ 10.0 billion) (Figure 4).
The cumulative total medical care expenditure from FY 2018 to FY 2050 was estimated to be 1769.2 trillion JPY (US$ 16 083.7 billion) to 1852.6 trillion JPY (US$ 16 841.8 billion). Compared with the estimated value without the impact of the increase in the medical expense for cancer, the cumulative total medical care expenditure was estimated to increase 7554.3 billion JPY (US$ 68.7 billion) to 11 715.0 billion JPY (US$ 106.5 billion) (Figure 5).
Regarding changes in each age group, the annual total medical care expenditure in FY 2050 in the ≥65 years group was estimated as 38.6 trillion JPY (US$ 350.9 billion) to 46.0 trillion JPY (US$ 417.8 billion), and the increase compared with the estimated value without the impact of the increase in the medical expense for cancer was estimated as 485.9 billion JPY (US$ 4.4 billion) to 908.5 billion JPY (US$ 8.3 billion).
Discussion
The main result from the SD model, built for forecasting the future medical care expenditure, shows the nation-wide medical care expenditure in FY 2050 to be 58.9-64.2 trillion JPY (US$ 535.1-584.0 billion), which represents an increase of 1.3–1.5 times from that in FY 2018. Considering that Japan’s nominal GDP growth over the 26 years from 1994 to 2020 was about 1.05 times, 27 the impact of this increase cannot necessarily be overlooked. As the increase rate used in this estimation was based on the baseline case published by the Cabinet Office, the estimation may be conservative. We tried estimation using the increase rates based on the 3 representative methods (MHLW formula, nominal GDP formula, and OECD formula) and there was no major difference in the estimation among their use in the analysis.
Multiple studies on future estimations of the national medical care expenditure in Japan have been reported. The estimation in 2050 was 38.7 trillion JPY (US$ 351.8 billion) in a report from Fukawa published in 2013. 30 In reports from the Cabinet Secretariat, Cabinet Office, Ministry of Economy and Finance, and MHLW in May 2018, the estimate in 2040 was 78.1 trillion JPY (US$ 710.0 billion). 31 General comparison is not favorable because the estimation varies depending on the economic indices expected at the time of executing estimation and changes in demographics. Moreover, it is important to periodically update and verify the forecasts. However, the values estimated by us were within the range of these reported values, demonstrating our estimates are generally reasonable.
The time-course on GE drug quantity share has been periodically reported, aiming at achieving the goal laid out for “the roadmap for promotion of the use of generic drugs” by the Japanese government. Under the assumption that a 90.32% GE drug quantity share is achieved based on the spreading speed of GE drug in Japan in the past and the usage conditions of GE drug in foreign countries, we performed the simulation in which the measures for promoting the spread of GE drug usage were added. The cumulative decrease over the 33-year period to FY 2050 was estimated to be 787.0 billion JPY (US$ 7.2 billion) to 989.4 billion JPY (US$ 9.0 billion).
The medical care expenditure in FY 2050 was estimated under the assumption that the increase rate of the cancer-related medical expense in the last 4 years will continue thereafter, the medical care expenditure in FY 2050 was estimated to be 59.5 trillion to 65.3 trillion JPY (US$ 541.3–594.0 billion) and an increase by 686.4 billion to 1104.2 billion JPY (US$ 6.2–10.0 billion) and cumulative increase by 7554.3 billion to 11 715.0 billion JPY (US$ 68.7–106.5 billion) over the 33-year period to FY 2050 were expected. This estimation exceeded the cumulative decrease expected by the measures for promoting the spread of GE drug by more than 10-times, implying cancer-related measures are one of policy issues to be focused on. Preparing a policy to increase the efficiency of treatment, such as development of innovative medical technology, financial investment for a policy promoting prevention and early discovery, and development of innovative testing techniques, may be important.
There are reports evaluating a policy that may contribute to reduce the cancer-related medical care expenditure in other countries. For example, Kuipers et al investigated the relationship between mass media campaigns for smoking cessation and the success rate of quit attempts, and found that an increase in mass media expenditure of 10% of the monthly average was associated with a .51% increase in success rates of quit attempts (95% CI .10%–.91%). 32 Holleman et al evaluated the impact of alternative risk-sharing arrangements (RSAs) for non-small cell lung cancer therapies based on real-world data and concluded that RSAs can mitigate uncertainty around the incremental cost-effectiveness or budget impact of drugs. 33 Modi et al reported that stronger engagement of urologists in accountable care organizations was associated with a lower likelihood of potential overtreatment (odds ratio: .29; 95% confidence interval: .10-.86) in the US. 34 Shi et al compared the cost-effectiveness of 6 common cancers from a priority setting perspective. Their preliminary analysis suggested that stomach cancer and colorectal cancer were the most cost-effective target cancers, and they concluded that they can be prioritized in future scaled-up screening in the general population. 35
If an efficient allocation of limited resources is considered as a national policy, it has to be considered based on 2 axes: not only reducing expenditure, but also pursuing improvement of the people’s quality of life. Both the efficiency of treatment selection based on evaluation of cost-effectiveness and the efficient use of limited national financial resources must be investigated with a long-term vision. To investigate the efficient allocation of resources, it is essential to discuss about the prioritization of a nation’s need and equity, and development of suitable indicator of social worth is also necessary. 36 The Global Burden of Disease (GBD) study has provided a conceptual and methodological framework to quantify and compare the health of populations using a summary measure of both mortality and disability, the disability-adjusted life year (DALY). 37 Park et al investigated whether the Ministry of Health and Welfare (MOHW)’s research and development (R&D) budget has responded to the burden of diseases evaluated using disability adjusted life years (DALYs) in Korea. As a result, a mismatch was observed between the R&D budget and the burden of disease in terms of DALYs, and they concluded that a novel approach for allocating government R&D funding based on the goal of minimizing the disease burden in the Korean population should be considered. 38 Grépin et al reported a survey that elicited preferences of different stakeholders for criteria guiding the allocation of external financing for health across countries using an online discrete choice experiment (DCE), and found that stakeholders assign a great deal of importance to health inequalities and the burden of disease. 39
Multiple studies that analyzed the impact on national healthcare costs with the SD method have been reported. Wang et al simulated the relationships between the total health expenditure financial resource and its key constraining factors in one Chinese province from 2002 to 2012 and put forward suggestions for the improvement of equity of health financial sources. 40 Nishi et al simulated the health care costs in Japan consisted of medical and long-term care expenditure from 2020 to 2040 and concluded that the increase will be attenuated if the proportion of dependent people decreases. 41
This study forecasted the future medical care expenditure in Japan from FY 2018 to FY 2050 using the SD model and estimated the future financial impact of the spread of GE drug usage and the increase of cancer-related medical expenses. Based on these, the need to introduce policies for attenuating the increase of the cancer-related medical expense was suggested. By using the SD model developed in this study, it will be possible to analyze the relationship between several possible policies and cancer-related medical care expenditure, and to identify more effective policies and their key success factors in the future. This study also serves as a reference for designing a policy in countries that will enter a super-aging society in the future such as that in Japan.
To consider efficient long-term allocation of resources, it is necessary to investigate not only changes in the expenditure, but also changes in the national revenue influenced by the national economic state and working population at the same time. To increase the accuracy of simulation, investigation considering the concept of fiscal health modeling42,43 enabling political decision-making based on age-specific transfer cost (i.e., health care costs and disability) and changes in tax receipts may be necessary in the future.
Last but not least, it should be kept in mind that the technological progress in healthcare and demographic trends, mostly structure of the population, are only part of a much wider set of influences on future health expenditure. Notably, technological advances in the healthcare interventions available and in the methods for delivering them will probably speed up in the coming decades. This means that attention should be paid on supply side drivers of the healthcare as an effective strategy to provide high quality care at an acceptable cost. The impact of the COVID-19 pandemic on public health may also be an important factor in forecasting future health expenditures. Hueso et al reported that expenditure related to COVID-19 accounted for 12.3% of the total Spanish public health budget and was greater than cancer and diabetes costs. 44 There have been reports that prevention and management of the COVID-19 pandemic is associated with high financial expenditure for hospitals 45 and a substantial deterioration in mental health. 46 In Japan, the expansion of the COVID-19 has led to a significant change in the consultation behavior of the population and the national health care expenditure itself is decreasing, but the government has a separate reserve fund of about 5 trillion JPY for COVID-19 countermeasures. 47 Based on the above, the COVID-19 pandemic might be an important factor that will affect the future healthcare system. Therefore, validation of the prediction of future health expenditure based on further data accumulation will be required in the future. Moreover, the future needs for long-term care cannot be projected in the same way as healthcare. Hence, the need for more specific indicators on healthcare needs as well as evidenced-based healthcare decision making will remain high on the agenda.
As a result of the estimation of medical care expenditure by our SD model, it became clear that the trend of medical care expenditure and its scale differed by each age group. This implies the importance of understanding the difference in impact on each age group and recommending an efficient allocation of limited medical care expenditure considering the age distribution in policy making. This study may serve as a reference for designing a policy in countries that will enter a super-aging society in the future such as that in Japan.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580221091397 – Supplemental Material for Forecasting of Future Medical Care Expenditure in Japan Using a System Dynamics Model
Supplemental Material, sj-pdf-1-inq-10.1177_00469580221091397 for Forecasting of Future Medical Care Expenditure in Japan Using a System Dynamics Model by Sachie Inoue, Hua Xu, Jean-Claude Maswana and Makoto Kobayashi in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Sachie Inoue. The first draft of the manuscript was written by Sachie Inoue and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Supplementary Material
Supplementary material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.