
Abstract
“What is already known on this subject?” and “What does this study add?”
Previous studies that examined children under age 5 mortality in Ethiopia found that socio-demographic characteristics (educational status of mother, marital status, occupation of mother/caregiver), age at first marriage, Antenatal Care Visit (ANC) visit, skilled birth attendant, pregnancy termination, types of fuel used, and housing conditions were linked with under 5 child mortalities.1,3,7,9,10,14,15 However, these studies were institutional-based cross-sectional and used small and limited data. Due to this, the inference associated with the estimated parameters may be different from the actual value, resulting in wrong generalization.
In addition, some articles emphasized specific diseases related to child mortality and used simple statistical analysis to show the trend and factors associated with mortality. Additionally, studies’ aggregate analysis of the first 59 months of life is very limited in Ethiopia, especially since most studies focus on Neonatal. Furthermore, much work remains to be done in order to obtain an accurate figure of childhood deaths in the country. This study aimed to show the trend of under-five child mortality and common factors associated with mortality using community-based longitudinal data.
Background
Child mortality is an important demographic, health, and development issue for a number of reasons. Mortality is one of the 3 measures (along with fertility and migration) that determine population size and growth rate, the age-sex distribution, and the spatial spread of the population.1,2 It is an essential indicator of development and crucial evidence of a country’s value and priorities.2,3 According to the World Health Organization (WHO) report of 2018, under-five deaths accounted for 5.3 million of the estimated deaths of 6.2 million children and adolescents under the age of 15 years. The risk of a child dying before completing 5 years of age is still highest in the WHO African regions (76 per 1000 live births), around 8 times higher than that in the European region (9 per 1000 live births). 3 However, there was a decline in the trend, which was 39 deaths per 1000 live births in 2018 compared to 93 deaths in 1990 and 76 per 1000 live births in 2000, a 59% and 49% decline, respectively. The total number of under-five deaths dropped to 5.3 million in 2018 from 12.5 million in 1990. On average, 15 000 children died before age 5 every day in 2018, compared to 34 000 in 1990 and 27 000 in 2000. Sub-Saharan African countries remain the region with the highest under-five mortality in the world. In 2018, the region had an average under-five mortality rate of 78 deaths per 1000 live births. These indicate that 1 in 13 children died before they celebrated their fifth birthday. 4
In Ethiopia, there has been a tremendous effort to reduce child mortality that has brought remarkable progress in the past 2 decades. However, under-five mortality is still high, with 67 deaths per 1000 live births, meaning that 1 in 15 children in Ethiopia die before reaching age 5.4-11 According to various studies under 5, mortality is influenced and/or determined by various social, economic, demographic, environmental, cultural, or behavioral factors. Some of these factors influence under-five mortality directly, while others affect it indirectly.9-11
A cross-sectional study found that mothers’ education, wealth status, place of residence, religion, immunization, type of birth, breastfeeding, housing, sanitation, and source of drinking water were all linked to under-five child mortality.10-12 In particular to Ethiopia, few of the studies conducted examine factors associated with under-five mortality in the country’s base health facilities which are not representative of the under-five population of children aged under 5 years in the country. In addition, there is a limited study, particularly in the Eastern part of the country, that assesses the trends and risk factors associated with under-five mortality based on the data of longitudinal. There are previous studies that were conducted on the same surveillance site with various years of data analysis.13,31,32,41 But they focused on neonatal mortality and the cause of death. In addition, they did not indicate the trend of under-five mortalities in the area. Few of them presented a trend of neonate death with data that appeared to indicate an upward or downward trend over time, which was frequently presented without a statistical analysis, making it difficult for decision-makers to determine whether these apparent trends were due to chance variation.13,31,41 Therefore, population-based longitudinal study is the method of choice to discover factors associated with death in Ethiopia. Therefore, this study aimed to assess the trends in under-five childhood mortality and identify factors associated with under-five mortality (U5M).
Materials and Methods
Study Area and Period
Kersa Health and Demographic Surveillance Site (KHDSS) is one of the districts in the eastern Hararghe zone that was established in 2007. It is 44 km west of Harar and 531 km from the capital, Addis Ababa. Kersa Health and Demographic Surveillance Site (KHDSS) is located in Kersa district, East Hararghe Zone, Oromia region. It is located between 41 0 40′ 0′ and 41 0 57′ 30’ (longitude) and 09 0 15′ 15′ and 09 0 29′ 15’ (latitude). In 2007, the Central Bureau of Statistics estimated that the total population of the region was 170 816. Of which 86 134 were males (50.4%) and 84 682 were females (49.4%); 11 384 (6.67%) of its population were rural residents. The district has 7 health centers, 7 health stations, and 8 private pharmacies in different locations in the district (CSA, 2012). The study was conducted from February 20th to February 30th, 2020.
Study Design
Kersa HDSS uses an open cohort population-based longitudinal surveillance design. It follows individuals in selected sites longitudinally every 3 months up to 2012 and every 6 months since 2013. Death registration and verbal autopsy for cause of death are taken for newborns ≤28 days, children’s 4 weeks to 15 years, and adults ≥15 years, adopted from the 2007 standardized World Health Organization (WHO) questionnaires. It covers all socio-economic, demographic, and environmental conditions of subjects longitudinally followed (individuals and household units).
The source population is all children under the age of 5 recorded in the KHDSS database from 2008 to 2016. The study population was children under 5 years of age, selected from the Kersa Health and Demographic Surveillance System database.
All children under the age of 5 years recorded in the KHDSS database were included in the study. Children under 5 years of age with incomplete socio-demographic data were excluded from the study sample size determination.
Data Extraction Method and Tools
First of all, the available data on the Kersa health and demographic surveillance system database was observed, and appropriate data was extracted from the KHDSS database and Open Data Kit (ODK) by trained data collectors who have enough knowledge and experience in operating computers using the prepared data collection format from the already existing record.
Data Collection Procedure in the Surveillance Site
KHDSS covers 24 kebeles in Kersa District (the smallest administrative unit in the country) and 12 kebeles in Harar Town. The baseline information was assessed in 2007. There are permanently employed data collectors in each kebele who update the list of individuals living in the house during the 6-monthly field visits. The data collected includes births, deaths, and moving in or out every 6 months. Immunization, human waste disposal, solid waste disposal, water supply, housing conditions, reproductive health, nutrition, HIV/AIDS, and health care seeking and use are assessed and updated every year, and economic status is updated every 2 years. The death registration for the deceased, which includes verbal autopsies for the cause of death, was taken from close relatives, typically after the mourning period of 45 days. The verbal autopsy questionnaire is based on the World Health Organization (WHO) verbal autopsy form for neonates (less than 28 days of age), children (4 weeks to 15 years of age), and adults (15+ years of age). The verbal autopsies are done by data collectors separately from the regular surveillance data collection. 6 At the end of each data extraction day, the principal researcher checks the completeness, clarity, and consistency of the data extracted from each record.
Variables
Outcome Variables: Under-Five Child Mortality
Independent variables
Socio-economic characteristics such as gender, mother’s education, religion, marital status, occupation, antenatal care (ANC), vaccination, birth outcome, breastfeeding, birth interval, parity, birth attendant, place of delivery, environmental factors, such as the source of drinking water and the distance between the water source and the house, whether the household has a separate kitchen and window, the type of toilet, and whether it is shared, and the materials the house is made of.
Operational definition
Under-five mortality—The death of children before reaching the age of 5 years in the study area.
Under 5 mortality rate(U5MR)—is the rate calculated as equal to the number of deaths of children under 5 in calendar years between 2008 and 2016 divided by the number of under-five children in the same years and multiplied by 1000.
Water source—water utilized for drinking and for domestic purposes such as preparing food, whether it is from a protected or unprotected source.
Sanitation facilities—presence and utilization of facilities such as latrines and types of latrines.
Normal birth weight—birth weight of equal to 2,500g
Big birth weight—birth weight of greater than 2,500g.
Low birth weight—birth weight of less than 2,500g
Data quality control
Data quality was ensured during data extraction, recoding, and analysis. During the data extraction period, adequate training and follow-up were provided for all data extraction personnel. The principal investigator worked closely with the data manager during data extraction. At the end of each day, the extracted data was reviewed and checked for completeness, accuracy, and consistency by the investigator, and corrective discussions were undertaken with all research team members. During the data extraction, the principal researcher worked closely with the data manager. At the end of each day, the investigator reviewed and checked the completeness, accuracy, and consistency of the data extraction form and had a corrective discussion with members of the research team. Prior to further analysis, data were checked for incompleteness and cleaned using statistical software (SPSS version 26 and/or STATA version 15). The data was further cleaned by visualizing and calculating frequencies and sorting in STATA and/or SPSS. A correction was made according to the original data.
Data Processing and Analysis
STATA version 15 (for analysis of associated factors) and/or SPSS version 26 (for trend analysis) software were used to edit, clean, and analyze the data. To look for outliers, consistency, and missing values, a frequency distribution was performed. The descriptive analyses used were proportion, mean, and median. The mortality rate was calculated for the entire study period. The Box–Jenkins method was used to analyze the trend of under 5 deaths, which is a time series. The method follows iterative application of the model; (i) identification (using plots of the data, autocorrelations, and partial autocorrelations) to select a simple model; (ii) estimation (using maximum likelihood estimation (MLE) to maximize the probability of obtaining the data that we have observed); (iii) model diagnostic checking (the fitted model is checked for inadequacies by scatter plot of residuals on the y axis and fitted values on the x axis to detect non-linearity, unequal error variances, and outliers). Based on the Box–Jenkins method, the ARIMA model is used to predict the mortality trend of children under 5 years of age. Autoregressive Integrated Moving Average (ARIMA) is a time series method that fits specific statistical equations to past data. The model is expressed as ARIMA (p, d, q) s, where p means the order of auto-regression, d means the degree of trend difference, and q means the order of moving average. It requires a stable time series data set, which means that the time series has no fluctuations or periodicity over time. This means the ARIMA model is applied to stationary data only (a dataset is stationary if it has a constant mean, variance, and covariance over time). If the data is not stationary, then it is made so by the process of differencing (the process of subtracting an observation from the previous time step observation until the data is stationary by the Augmented Dickey–Fuller test). Parameters of the ARIMA model (p, d, q) were estimated by the ACF (autocorrelation function) graph and the PACF (partial autocorrelation) graph. A simple line graph was used to show the trend in under-five mortality. A Mann–Kendall trend test was also employed to check the trend significance as well as at what rate the trend changed over the period. The factors associated with under-five mortality were analyzed using multi-level modeling by considering the nesting of the outcome variables (child mortality) with the survey years. Individual-level covariates and survey years were modeled to examine variations and predict under-five child mortality.
For multi-level modeling in stata, 2 steps were followed. First, an empty model was built by fitting without factors to test the random variability in the intercept by survey year. This is to check whether multi-level logistic regression is an appropriate statistical model for the data. Then, a full model was built to evaluate the impact of the survey and the variables of interest simultaneously. In the full model, the variables included were antenatal care utilization, radio, television, type of drinking water source (improved or unimproved), toilet type (improved or unimproved), maternal age, maternal education, family size, place of delivery, birth attendant, mother’s occupation, sex of a child, pregnancy duration, and the presence of a window in the house and residence. By extracting variables with a P-value of <.25 from the binary logistic regression model, the variables are included in the multivariate regression. Variables with a P-value of .05 or lower in the multivariable logistic regression model were considered significantly and independently associated with under-five mortality.
Result’s
Socio-Demographic and Economic Characteristics of Children and Households
The total number of live births at the surveillance sites from 2008 to 2016 was 18 759, of which males accounted for 9574. Of the total number of births, 1602 children under the age of 5 died during this period.
Background characteristics of children and mothers/caregivers in Kersa health and demographic surveillance, 2008–2016, Ethiopia, 2020.

Causes of death in children under the age of 5 in Kersa health and demographic surveillance data analysis from 2008 to 2016, Ethiopia, 2020.

According to the data, infant mortality accounted for more than 62% of the 9 consecutive years of surveillance, with neonatal mortality accounting for 38%.
Under-Five Child Mortality Trends in a Surveillance Site.
Mortality rates in neonates, infants, and under-five age children in Kersa health and demographic surveillance 2008–2016, Ethiopia, 2020.
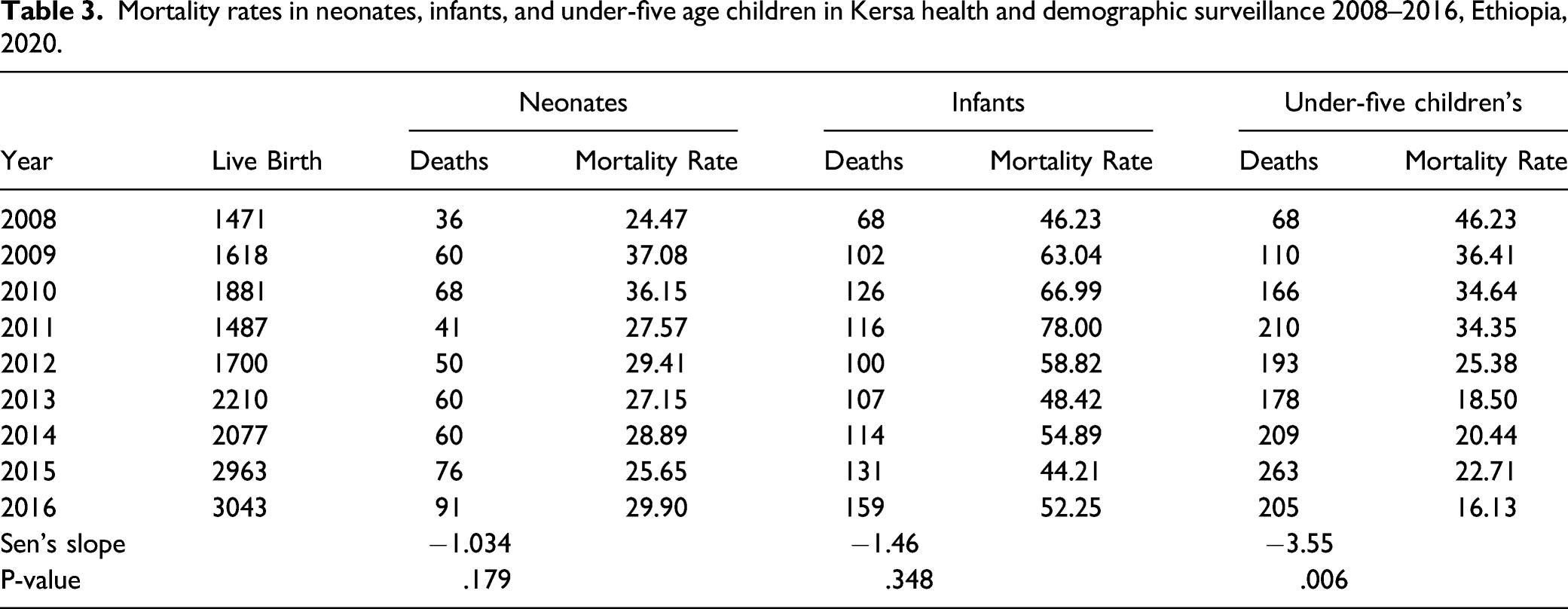
In the surveillance site, the overall rate of under-five child deaths is 85 per 1000 live births. Regarding the age distribution of deaths in the surveillance sites during 9 consecutive years, infant mortality was 55 deaths per 1000 live births and neonatal mortality was 29 deaths per 1000 live births (Supplementary, Figure 1).
Regarding sex-specific under-five mortality rates over a 9-year period, a decreasing pattern was observed in both sexes. A wide gap of mortality was observed in 2008 with a higher male under-five mortality rate (Figure 1). Distribution of sex-specific under-five mortality rates in Kersa HDSS, 2008-2016, Ethiopia, 2020.
Model for Predicting Under-five Child Mortality in a Surveillance Site
Estimated parameters of selected tentative models fit to the ARIMA model to predict under-five mortality rate in Kersa health and demographic surveillance site 2008–2016, Ethiopia, 2020.
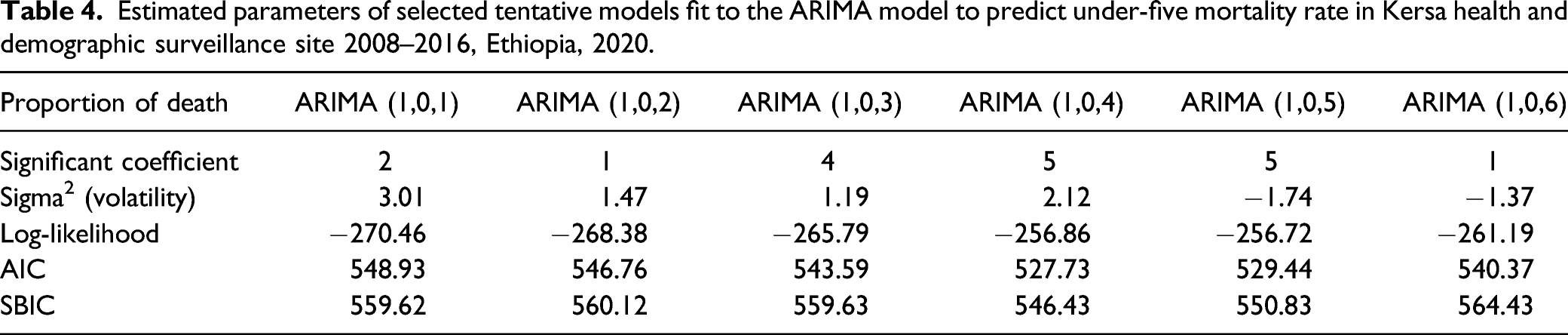
Based on the fitted model, the mortality rate is expected to decline ahead of the surveillance year of 2016 with fewer fluctuations in the trend. The prediction interval for the times is wider, with a 95% confidence interval. This wide range of predictions indicates the high uncertainty of the prediction (Figure 2). The observed, expected, and predicted values of the ARIMA (1, 0, 4) model of under-five mortality with 95% confidence limits in Kersa health and demographic surveillance, Ethiopia, 2020.
Factors Associated With Under-five Mortalities in Surveillance Site
Multi-level logistic regression on under-five mortality and associated factors in Kersa health and demographic surveillance site; 2008–2016, Ethiopia, 2020.

Discussion
From 2008 to 2016, the under-five mortality rate at the Kersa Health and Demographic Surveillance Site dropped significantly, despite a slight decrease in neonatal and infant mortality. The current finding is consistent with prior studies conducted in similar areas (Kersa HDSS)13,31,32 and other previous studies conducted at national and community-based levels that reported a similar trend of under-five children’s deaths. 13 However, these findings revealed lower infant and neonate death rates than the study conducted in Uganda. 14 The decreasing trend in the mortality rate of U5C (under 5 children) during the study period agrees with the national and international decrement of under-five children dying. The decreasing trend of under-five deaths during the study period may be a consequence of an essential improvement in health services, such as education on health problems and how to prevent and control them, maternal and child health care, including family planning, immunization against major infectious diseases and current government policy priority areas of child health (improvement in resource mobilization, scale-up of high-impact interventions coordination and partnership).
The forecast for the next 5 years from 2016 shows that there is a certain downward trend in the mortality rate of children under 5, but there is a certain degree of uncertainty. Uncertainty in the prediction could be due to the inaccuracy of data. Therefore, using recent and accurate data, such predictions can be used for forecasting progress toward sustainable development goals.
The finding shows the socio-demographic characteristics of the mother’s association with under-five mortality in the surveillance site. After controlling for other variables, the mother’s educational status emerges as a strong predictor of under-five mortality, which is consistent with other studies conducted in southwest Ethiopia 15 and the latest Ethiopian demographic and health survey of 2016 analysis 30 and elsewhere.33,34,36 The reason may be that educated mothers are more capable of gaining health care access and receiving antenatal care services because of their better income, higher health literacy, and power to make healthier decisions on the health for themselves and their children. Furthermore, education can contribute to child survival by suspending early marriage and motherhood as a result of the decreased total number of children a woman has. 16
A strong association was shown between maternal working and under-five deaths. Children of mothers working were found to be significantly increasing odds of under-five mortality. This is higher than the 2011 analysis of Ethiopian demographic and health survey. 17 This could be because of increased family income, which enables parents to provide their children with higher quality health care services and improve mothers' and thus child wellbeing. 18
In addition, this study revealed a significant relationship between the mother’s gestational age and the under-five mortality rate. Mothers who had a preterm pregnancy experienced much higher child deaths than those mothers who had given birth at term. This finding is consistent with the EDHS analyses of 2000, 2005, and 2011. 19 It is also consistent with previous research that has found a high risk of mortality among children under the age of 5 whose mothers gave birth prematurely.38-40 This could be due to babies born prematurely having more health problems at birth and later in life than babies born later. 20 This may also be due to the following reasons: increased mortality from sudden infant death syndrome, prolonged impairment of pulmonary function, infections and respiratory conditions, early birth itself, and increased susceptibility to various health conditions, including behavioral disorders, neurological conditions, impaired vision and hearing, and chronic illness.38-40
The findings of the study confirmed that mothers who had more than 5 total births experienced significantly higher child mortality than those who had less than 2 total births. This variable is, in 1 way or another, related to family planning that affects family size. Family size is positively associated with child mortality. This is comparable with the study conducted in Nigeria. 21 Different reasons are given for the rise in mortality for mothers who have had many children. This may be because of insufficient support and care for the child. 29 However, the findings of this study are not in line with the study conducted in the Afar region, which has shown family sizes have a significant reduction in child mortality. 35
The risk of under-five deaths was higher among children who lived in houses built with inadequate materials than in those with standard and moderate housing materials (a house built in the absence of windows and inadequate materials from which the roof was built). The house built with moderate housing materials (windows installed) reduced the risk of dying more than a child in a house built with inadequate materials. These finding gave credential to other studies conducted in northern Ethiopia22,23 Nigeria, 36 and Pakistan 37 that established an association between ill health and poor housing conditions because of inadequate building materials. The standard quality of the materials with which the house is built is entirely related to the durability of the materials the house is built with and the health of the family living in it. 22
Poor housing conditions could lead to the formation of damp in the house, which can result in the formation of molds and different kinds of fungal pathogens that can cause different types of respiratory health problems such as asthma. 24 In addition, there are cracked buildings (walls); this provides a favorable environment for the reproduction of various insects such as cockroaches, mites, and arthropods, all of which promote the pathogenesis of respiratory health problems.25,26
The current study also revealed that house those who did not have windows and shared latrine facilities had experienced higher under-five deaths than those who had windows and not shared latrine facilities, respectively. This may be due to poor ventilation and poor sanitation which led to the death of children from respiratory diseases and diarrheal diseases respectively. 27 However, the finding is slightly different from the studies conducted in some else.27,28
Strength and Limitations of the Study
This study had several strengths. First, it is representative surveillance that uses a standardized method that yields a high response rate. Second, the pooled method (large sample size) maximized the study power and permitted valid generalization of the results to a population of similar characteristics. Third, advanced statistical analysis was used to estimate the outcome and factors associated with it. However, it faces a number of limitations: First, some important predictors of under-five deaths were not included in the analysis because of imprecise measurement due to incomplete or mislabeled variables, restricted variable data, inconsistent values, and missing records of the predictors. Second, the analysis considers under-five children who had vital information, which might lead to an underestimation of mortality rates. The effects of some associated factors may also be underestimated.
Conclusion
During the study period, the mortality rate of children under 5 at the surveillance site dropped significantly. Mother’s education, pregnancy duration, safe sanitation, birth weight, total number of children born, and house material were all significantly associated with under-five deaths in the surveillance site. As a result, an intensified effort is required to address the issue. In realization of this fact, we recommend that efforts toward access to prenatal care and quality care service throughout the pregnancy, childbirth, and postnatal period should be ensured to reduce the incidence of low birth weight and other pregnancy related complications. Improving the literacy status of women is essential so that they can care for their children for better health. Broad-scale public health and educational efforts in various areas, especially on sanitation and family planning, will have a strong impact on child health and survival. Strategies aimed at socio-economic development may also impact child survival.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580221090394 – Supplemental Material for Trends and Associated Factors of Under-five Mortality Based on 2008–2016 Data in Kersa Health and Demographic Surveillance Site, Eastern Ethiopia
Supplement Material, sj-pdf-1-inq-10.1177_00469580221090394 for Trends and Associated Factors of Under-five Mortality Based on 2008–2016 Data in Kersa Health and Demographic Surveillance Site, Eastern Ethiopia by Gebisa Dirirsa Gutema, Abraham Geremew, Dechasa Adare Megistu, Yohannes Mulugeta Dammu and Kefelegn Bayu in The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgments
We would like to express our special thanks and gratitude to the Kersa Demographic and Health Surveillance site workers who gave us golden assistance to do this wonderful research on this topic. We are grateful to our staff colleagues, especially Dr Tariku Dingeta, who has read and commented on several parts of our research document.
Authors’ Contributions
GD and AG conceived and designed the study, analyzed the data, interpreted them and drafted the manuscript. DA, YM, and KB have contributed to data analysis and interpretation. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Kersa HDSS is one of the INDEPTH members supported by the Centers for Disease Control and Prevention (CDC) in collaboration with the Ethiopian Public Health Association (EPHA) through project agreement GH001039-01 with Haramaya University. The funder had no role in the design, data collection, analysis, interpretation, and writing of this manuscript.
Data Availability
The data set used and/or analyzed in the current study belongs to Kersa
HDSS. The data set is accessible upon filling out an agreement form based on the data sharing policy online with the link ![]() . The author confirmed that they did not collect or do not own the data and that other researchers can access the same data in the same manner as the authors through a formal request. According to the application, the Kersa HDSS team conducts an evaluation, and the applicant can analyze the raw data. If the application is granted open access, sensitive information like names, identification numbers, and house numbers is removed before providing the data set to the applicant through generating new identification numbers to enable them to link it back to the original data. The derived data supporting the results of this study will be available from the corresponding author upon reasonable request.
. The author confirmed that they did not collect or do not own the data and that other researchers can access the same data in the same manner as the authors through a formal request. According to the application, the Kersa HDSS team conducts an evaluation, and the applicant can analyze the raw data. If the application is granted open access, sensitive information like names, identification numbers, and house numbers is removed before providing the data set to the applicant through generating new identification numbers to enable them to link it back to the original data. The derived data supporting the results of this study will be available from the corresponding author upon reasonable request.
Ethical Approval and Consent to Participate
The Kersa HDSS site was established after ethical approval from various agencies. The site has received ethical approval from the Centers for Disease Control and Prevention (CDC), the Ethiopian Public Health Association (EPHA), the Ethiopian Science and Technology Agency, and the Haramaya University Health Research Ethical Review Committee (HRERC). Similarly, for these studies, secondary data for analysis was obtained after getting an approval letter from the Institutional Health Research Ethics Review Committee of Haramaya University College of Health and Medical Sciences. The letter was written from Haramaya University to the College of Health and Medical Sciences, Kersa HDSS office. Full permission was obtained from these offices, and identifying information for the study was obtained upon request. The data was fully anonymized in order to protect the privacy of those prior to accessing it. The name or any other identifying information was not used, and the information taken from the database was kept strictly confidential. The information retrieved was used for the study’s purposes only.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.