
Abstract
Introduction
This study aimed to determine if applying International Classification of Diseases (ICD) disease codes directly as the cause of death (COD) on death certificates (DCs) instead of writing or typing the COD could reduce the use of garbage codes.
Methods
Beginning in April of 2016, a documentation process change was made, retiring the process of hand-writing or typing the COD onto DCs to directly applying ICD disease codes that were registered during the patient’s course of treatment. The DCs issued at the emergency department (ED) 1 year before (Pre-code group) and after (Code group) applying ICD disease codes directly on DCs was instituted were retrospectively analyzed. The occurrence of garbage codes along with other major and minor errors was compared between the two groups. The investigation and judgment of errors were performed by four emergency physicians.
Results
The overall garbage code occurrence in the Code group (25%) was significantly lower than that in the Pre-code group (49%). Fewer garbage codes were used in the Code group with an average of .5 in the Pre-code group and .3 in the Code group. No significant difference was identified in major error occurrences except for in the garbage codes. Minor errors were more common in the Pre-code group than in the Code group.
Conclusion
The overall use of garbage codes on DCs could be reduced by changing the process by which physicians complete DCs, that is, the application of documenting ICD disease codes directly as the COD on DCs.
It is known that there were many errors in death certificates, including the use of garbage codes, which could not be used as an underlying cause of death. Reducing garbage codes is important to improving the quality of mortality statistics. Garbage codes can be reduced by applying disease codes as the cause of death, which can improve the quality of death certificate statistics. To improve the quality of death statistics, the quality of death certificates should be improved. As one of the methods, if disease codes are applied to death certificates as the cause of death, the quality of death certificates can be improved by reducing the use of garbage codes.What Do We Already Know About This Topic?
How Does Your Research Contribute to the Field?
What Are Your Research’s Implications Toward Theory, Practice, or Policy?
Introduction
A death certificate (DC) is a legal record of a person’s cause of death (COD). The information from a DC is collected for COD statistics, which is essential in determining the direction of healthcare policies.1-4 Since the 1990s, researchers in the Global Burden of Diseases (GBD) study have tried to analyze the COD data derived from DCs. Despite the researchers’ efforts, the validity and quality of COD data remain questionable in many countries. 5
In 1996, Murray et al introduced the term “garbage codes” to describe diagnoses that could not be used as an underlying COD. Various studies are being conducted to classify and reduce these garbage codes to improve the quality of COD statistics.5,6 Although there have been studies such as educational interventions and online learning programs on how to complete a DC, and the development of algorithms to redistribute these garbage codes to improve COD data,3,6-10 garbage codes are still found in about 30% of all DCs. 11 Since garbage codes impact healthcare policy establishment, attempts should be made to reduce these errors.
Establishing a well-functioning COD registration system is challenging for a number of reasons. Physicians occasionally document CODs outside of accordance with the standardized rules of the International Classification of Diseases (ICD) proposed by the World Health Organization (WHO). These physicians utilize non-standardized terms in the COD section on a DC, often because they are handwritten or typed in by the attending physician. This informal documentation of the COD on DCs then goes through a process called coding, which converts the descriptive terms into diagnoses that suit the ICD standard. Lu et al 12 identified that the most frequent type of disagreement between the reviewers and coders involved COD nomenclature. Physicians tend to complete DCs with diagnoses familiar to them in clinical practice, without fully understanding how the coding system works. Due to these challenges, garbage codes occur frequently, making the COD statistics less reliable. To the best of our knowledge, there is a lack of studies focusing on changing ways to complete DCs to overcome these challenges.
This study aimed to reduce garbage codes by suggesting alternative methods to complete DCs. In this study, we compared DCs that were completed by typing in the COD with those completed by selecting the COD directly from an ICD coding system and evaluated the occurrence of garbage codes.
Methods
This was a retrospective analysis study, which included DCs issued in the emergency department of Ulsan University Hospital, a university training hospital in Korea. It was reviewed by an institutional review board.
The CODs on the DCs were handwritten or typed by the attending physicians until March of 2016 in Ulsan University Hospital, where this study was conducted. Beginning in April of 2016, a documentation process change was made, retiring the process of hand-writing or typing the COD onto DCs to directly applying ICD disease codes that were registered during the patient’s course of treatment (Figure 1). The disease codes that were registered during the treatment of the deceased were based on the ICD-10 published by the WHO. It was made possible that if the physician disagreed with the selected disease code or simply wanted to type in the cause, it could be deleted and typed in. However, typing in the COD was possible only after deleting the COD that was selected from the registered disease codes, so the attending physicians could not type in the COD from the beginning. Electronic record input for the COD section in DCs in the Pre-code group (A). The initial COD section in the Code group (B) was the same as in the Pre-code group. In the Pre-code group, a physician typed in the COD after clicking (a). In the Code group, upon clicking (a), a popup window containing ICD-10 codes appeared (b), and a physician could search for and select the suitable COD code.
In this study, we analyzed DCs that were issued in the emergency department at Ulsan University Hospital in the years 2015 and 2017, one year before and after the 2016 documentation process change for disease codes used for the COD on DCs was applied. The DCs issued in the emergency department of the university hospital in 2015 (Pre-code group), when the COD was typed in directly, were compared with the ones issued in 2017 (Code group), when the COD was selected from the registered disease codes. This study included the DCs of the patients that died during treatment at the hospital with relatively clear CODs. Autopsy certificates issued after death and DCs of patients who died of unknown causes were excluded from the study. DCs of patients who were dead on arrival were also excluded. Among the total of 192 DCs in 2015 (Pre-code group) and 152 DCs in 2017 (Code group), 50 cases and 26 cases, respectively, were excluded from the study (Figure 2). The power for the sample sizes of 142 of in the Pre-codes group and 126 in the Code group was .99. Study subjects.
The garbage codes, introduced by Murray and Lopez, and further classified by Naghavi et al into four categories, were as follows.
11
1. Type 1: Causes that cannot or should not be considered as an underlying cause of death (UCOD). 2. Type 2: Intermediate causes of death without an underlying cause such as septicemia or pulmonary hypertension. 3. Type 3: Immediate causes of death such as cardiac arrest or respiratory failure. 4. Type 4: Insufficiently specified causes of death.
The definition of errors on death certificates.
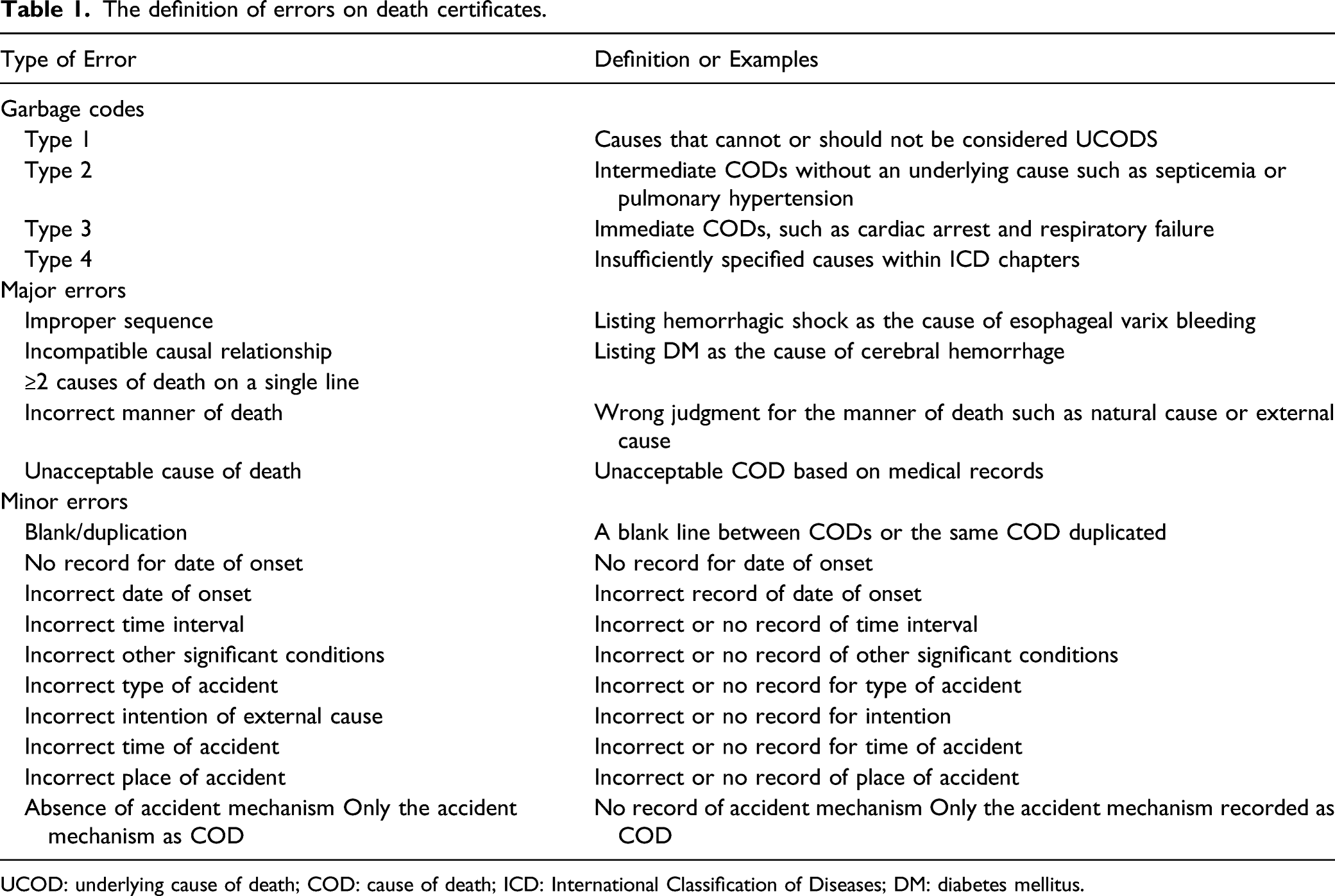
UCOD: underlying cause of death; COD: cause of death; ICD: International Classification of Diseases; DM: diabetes mellitus.
The number and type of garbage codes were investigated along with the number of CODs recorded on the DC, the number of major and minor errors, and the total number of errors. The judgment of errors was first conducted by three individual resident-physicians who had received education on certifying death and ICD-10 coding, and were currently practicing in the ED. Then, a senior emergency physician who had research experience on DCs performed a secondary review process. The senior emergency physician and the residents then performed a final consensus process together for CODs that needed further determinations. CODs that were hard to determine even after the final consensus process were to be excluded from the study, but no cases were excluded from this study. The independent variables in this study were Pre-code group and Code group, and the rest of the variables were dependent.
Statistical Analyses
Frequency analysis, the chi-squared test, Fisher’s exact test, and the Student’s t-test were used to compare the errors including garbage codes in the Pre-code group and the Code group. IBM SPSS 24.0 (IBM, Armonk, NY, USA) was used for the statistical analyses, and statistical significance was defined as P < .05.
Results
A total of 142 cases in the Pre-code group and 129 cases in the Code group met the inclusion criteria for the study. The average age was 63 years in the Pre-code group, and 62 in the Code group. Among the deaths, 57% were male in the Pre-code group and 68% in the Code group. Of the deaths, 76% in the Pre-code group and 73% in the Code group were disease-related, with no significant difference between the two groups. Of all the CODs, 60% of the CODs in the Pre-code group had a single COD, whereas 52% of the Code group had a single COD. There were 2 or more CODs in 40% and 48% of the Pre-Code and Code groups, respectively.
Characteristics of death certificates according to the application of disease codes for the cause of death.

Garbage codes on death certificates according to the application of disease codes for the cause of death.

Errors other than garbage codes as the underlying cause of death on death certificates according to the application of disease codes for the cause of death.

UCOD: underlying cause of death; COD: cause of death.
Discussion
Garbage codes were found in 48.6% of the Pre-code group, which was similar to previous studies where errors related to the cause of death were found in about 48–64% of all DCs.4,18,19 In contrast, garbage codes in the Codes group were decreased to 24.6%.
Causes that cannot or should not be considered a UCOD, classified as a type 1 garbage code, usually occur mainly in elderly patients, where the definitive cause of death is difficult to identify, and were found on up to 10% of all DCs in previous studies.6,13 In this study, type 1 garbage codes decreased from 12% in the Pre-code group to 1.6% in the Code group. Senility was the most frequent cause of death accounting for type 1 garbage codes. According to Lee et al, 20 senility accounted for 5% of all causes of death in Korea. A diagnosis such as senility, which is not a valid cause of death, is of no use from the point of view of the cause of death statistics. There were two cases in which type 1 garbage codes were used as the cause of death in the Code group, both of which had been typed in and not selected from the ICD disease code list. It is not impossible to select senility as the cause of death from the ICD disease codes list, but it seems plausible that the process of looking up the ICD disease code list might have helped in selecting a valid disease code during the documentation process.
Intermediate CODs without an underlying cause such as septicemia or pulmonary hypertension, classified as type 2 garbage codes, ranged from 22% to 30% of all DCs in previous studies.3,10,21 There was no difference in the incidence of type 2 garbage codes between the Pre-code group and the Code group, as they were found in 12.7% and 14.3%, respectively. The application of disease codes alone did not reduce the occurrence of type 2 garbage codes since intermediate CODs usually occurred due to reasons such as poor training on death certification or limited diagnostic equipment.6,11 In settings that do not lack diagnostic equipment, like in this study, educational interventions could be helpful in reducing the use of type 2 garbage codes as shown in the studies of Myers et al, 7 Lakkireddy et al, 8 and Wood et al. 10
The immediate causes of death such as cardiac arrest or respiratory failure, classified as type 3 garbage codes, ranged from 5.8% to 34% on all DCs in previous studies.1,4,18,22 The incidence of type 3 garbage codes decreased from 25.4% in the Pre-code group to 11.1% in the Code group. Cardiac arrest was the most frequent reason for type 3 garbage codes, which occurred when the time to conduct diagnostic tests to accurately determine the patient’s condition was limited. There were cases in both groups where the immediate cause of death had to be used because the UCOD could not be determined. However, as Schuppener et al 3 proposed, the majority of the errors on DCs were due to the omission of known conditions or illogical sequencing of known events leading to death. Making an effort to determine the UCOD through sufficient review of the patient’s medical history and test results remains crucial.
Insufficiently specified causes of death, classified as type 4 garbage codes, ranged from 4.5% to 19% in previous studies.1,3,18 In this study, type 4 garbage codes were not found in the Pre-code group, and there was only one case of a type 4 garbage code in the Code group. The rate of type 4 garbage codes in this study was significantly lower than in previous studies. This is because, unlike other studies, we did not consider the lack of a specific cancer site (eg, not specifying which lobe of the lung or which part of the colon) or not specifying the occluded artery in a stroke, problematic. According to Naghavi et al, 9 these diagnoses are likely to be confined to a single disease category, having much less impact on healthcare policy implications. Listing lung cancer as the COD without specifying its specific location would still be assigned as death by lung cancer, similar to stroke death reporting.
In this study, a type 4 garbage code was found in the death of a lung cancer patient with brain metastasis. The diagnosis of secondary cancer, not lung cancer, was used as the COD. When receiving outpatient and inpatient treatment, the secondary cancer code, not lung cancer, was continuously selected, and even when the patient died, the most recently registered secondary cancer code was selected as the COD on the DC. If applying disease codes as the COD becomes common, physicians should always give careful consideration when selecting the COD to avoid making this kind of mistake.
As identified in previous studies,14,15 in this study, the greater the number of CODs listed, the more errors were found. Major and minor errors were found in 3.3% and 92.1% in DCs with a single COD, 20.5% and 93.2% in DCs with two CODs, and 55.2% and 100% in DCs with three or more CODs, respectively. The number of GCs and the number of CODs written did not show a statistically significant relationship. Major errors were found in 17.6% and 11.1% of the Pre-code and Code groups, respectively (P = .132). Although the results failed to show statistical significance, the number of major errors tended to decrease in the Code group. The most common type of major error was listing more than two CODs on a single line. It would be challenging to choose the correct cause of death when two or more causes of death are recorded in a single line, which could lead to a decrease in the quality of the COD data.
As interest in COD statistics increases, research on garbage codes is being conducted. In many cases, methods to improve the quality of COD statistics by analyzing garbage codes that have already occurred are being studied. Reclassification methods, where a physician evaluates the medical records and test results to define the COD along with redistribution, which is a process of defining the UCOD of the DCs containing garbage codes based on statistical methods or analyses, have been conducted.6,20,23 In addition, as electronic coding systems for the causes of death have been introduced in many countries, studies that use automated coding systems such as IRIS to analyze the COD are showing promising results.24,25 However, since these attempts rely on the data of the DCs that have already been completed, it is necessary to increase the accuracy of DCs in advance. In addition to educational interventions on completing a DC, which were shown to be effective in several previous studies, the change in the documentation method of completing DCs attempted in this study is expected to enable physicians to certify death more accurately.
In Korea, medical doctors, dentists, and oriental medicine doctors have the authority to complete death certificates. If a death certificate is issued with a cause of death that does not require an autopsy and has no legal problems, the death certificate is registered at the administrative office based on the death certificate, and after a final review by the National Statistical Office, it is finally registered in the national death statistics. If the cause of death is an external cause or an autopsy is required, the death certificate is issued after an investigation by the police and prosecutors, and the subsequent process is the same. Despite the researchers’ efforts, the validity and quality of COD data remain questionable in many countries including Korea. Chang et al and Park et al reported disappointing results regarding the validity of DCs issued in Korea.14,15 Although many types of errors in DCs are made by physicians every day, there is no official education or feedback program in Korea concerning how to write a death certificate.
This study analyzed DCs issued by a single training hospital’s emergency department and there is a limitation on generalizing the results of this study since DC forms vary from institution to institution and the pattern of errors may be different. Furthermore, this study did not include the degree of education related to the issuer of the DC, which could have a significant impact on errors on the DC. However, even though no education related to issuing DCs was provided before and after the application of disease codes as the COD, the incidence of garbage codes decreased. It is possible that applying disease codes for the COD, aroused physicians’ attention on certifying death, which led to the decreased use of garbage codes.
Conclusions
In this study, we found that the overall garbage code usage could be reduced by a relatively simple method of changing the process by which physicians complete DCs, that is, the application of documenting ICD disease codes directly as the COD on DCs. If the effectiveness is proven through continuous research related to the application of disease codes for the COD in an environment that can register the disease code according to the ICD classification, this method could be worth referencing as a model for reducing garbage codes, and the overall positive impact this could have on healthcare policies. With this result, it is important to select the correct ICD disease codes before writing the DC. If incorrect ICD disease codes are selected, the expected positive effect of reducing errors in the DC by applying ICD disease codes will be reduced. Therefore, education on selecting the correct ICD disease codes should also be carried out.
Footnotes
Acknowledgments
The author(s) thanks to Dr Byeong Ju Park and Dr Sangyeop Jung, resident of emergency medicine in Ulsan University Hospital for their contribution of data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.