
Abstract
Background:
Relatively little is known about where foreign-born individuals die in Sweden and how birth region might influence place of death. Thus, there is a need for population-based studies investigating place of death and associated factors among foreign-born individuals.
Objectives:
The aim of this study was to identify variations in place of death among foreign-born individuals residing in Sweden and to compare place of death between the foreign- and domestic-born population. We also examine the association between place of death, underlying cause of death and sociodemographic characteristics among the foreign-born population.
Design:
A population-based register study.
Methods:
All deceased individuals ⩾18 years of age in Sweden with a registered place of death between 2012 and 2019 (n = 682,697). Among these, 78,466 individuals were foreign-born. Univariable multinomial logistic regression modelling and multivariable multinomial logistic regression analyses were performed.
Results:
Overall, hospital was the most common place of death among the foreign-born population. However, there were variations in place of death related to region of birth. Compared to domestic-born, a higher proportion of foreign-born individuals dies at home, the majority of whom were born on the African continent.
Conclusion:
Region of birth is one of the several factors associated with place of death among foreign-born individuals. Further research is needed to explore both preferences and barriers to place of death among foreign-born individuals.
Keywords
Introduction
The trend worldwide is for deaths to predominantly occur in hospitals,1–6 although common preferences among patients in high-income countries are to die at home.7–9 Increased attention is given to improving care at the end of life, including developing a better understanding of where individuals die, and factors related to place of death. All individuals with similar needs should have the same access to place of death and palliative care, given that equal access to healthcare is one of the fundamental principles of the human right to health. Patients in need of palliative care may be cared for in their own homes, special housing (such as nursing homes) and in hospitals. 10 An expected death does not necessarily equate to palliative care needs, although research suggests that between 69% and 83% of all deaths in high-income countries were caused by conditions indicative of palliative care needs.2,11 The integration and provision of palliative care – and the population’s awareness of such matters – varies greatly between high-income countries, with Sweden being at the forefront of palliative care integration. 12
Social inequality regarding health – including palliative care provision – is a global reality. Socioeconomic and sociodemographic factors – such as education, age, ethnicity and language – have an impact on health, and they also affect palliative care provision, including access to 13 and actual place of death.2,14–17 Studies in high-income countries point towards an overall trend of people with higher socioeconomic status being more likely to die in their homes 14 and less likely to die in hospital than those with lower socioeconomic status.13,14,18 Research from Great Britain also points towards ethnicity (with country of birth often used as a proxy for ethnicity) as a factor influencing place of death, with certain immigrant or minority groups, such as Black, Asian and minority ethnic groups being more likely to die in hospital and less likely to die at home.19,20 However, it is unclear how transferable these results are to the Swedish context, who has its own specific migration pattern.
Sweden has been a country of immigration since the 1930s. After the Second World War and up until the 1970s, migration mainly consisted of labour immigrants, foremost from the other Nordic countries but also from southern Europe and Turkey. Latin American dictatorships and the Islamic revolution in Iran attracted immigrants in the 1970s–1980s. In the 1990s and the first years of the 2000s, immigration was foremost from Yugoslavia and the Soviet Union, and from civil war-torn Iraq and Somalia. 21 Immigration peaked in 2016, with newcomers mainly originating from Syria, Afghanistan and Northern Africa, 22 even though large parts of immigration during the 2000s were re-immigrated persons born in Sweden. The public health in Sweden is affected by immigration in many ways. Foreign-born individuals uniformly report having poorer health than those who are domestic-born, where those born outside of Europe reported having the worst health. 21 Previous studies have shown higher mortality and morbidity in foreign-born compared to domestic-born people.23,24
To date, relatively little is known about where foreign-born individuals die and their use of palliative care services at the end of life. Studies in the United Kingdom of cancer deaths show that place of death varies according to the individuals’ birth region but also between ethnic groups. Individuals born in Asia, Africa and the Caribbean were more likely to die in hospital than domestic-born 19 and minority ethnic groups were more likely than White patients to die at hospital. 20 Similarly, a recent study from the United States found Black and Hispanic people with dementia (PWD) more likely to die in hospital compared to White PWD. 25 A German study shows that immigrants are underrepresented in Hospice and Palliative Care (HPC), foremost Turkish immigrants 19 and a study conducted in Sweden shows that foreign-born individuals are less likely of being cared for in specialized palliative care units. 26 Thus, there is a need for population-based studies to ensure that palliative care needs are met in whole populations, including people who have immigrated. Investigating place of death and associated factors in a population is a way of learning about and understanding patterns and inequalities regarding access to and utilization of healthcare services. It can also help with retrieving information on where and how palliative care is provided, prioritized and integrated. To our knowledge, there are no international studies focusing on the association between place of death and migration (in terms of region of birth) among the country’s full adult population. There is a knowledge gap regarding how migration (region of birth) influences the place of death and palliative care provision in populations. Thus, the primary objective for this study is to identify variations in place of death between foreign- and domestic-born adults (⩾18 years of age) residing in Sweden. Furthermore, this study examines associations between place of death, underlying cause of death, and sociodemographic variables among the foreign-born population.
Methods
Setting
The Swedish healthcare system provides universal healthcare coverage for all residents and is publicly financed along with a minimal patient fee. 27 It is divided into three levels: the state, regions and municipalities. The extent and management of palliative care is chiefly organized by regions, but also municipalities, at the local level. Care for older people, including end-of-life care, is mainly provided by the municipalities and their share of the costs for end-of-life care increases with the patient’s age. 10 There are large local differences regarding the degree to which palliative care is organized and implemented depending on geography (rural versus urban), local traditions and competency.
Study population
This population-based register study includes all deceased individuals ⩾18 years of age in Sweden with a registered place of death between 2012 and 2019 (n = 682,697). Of these, 78,466 individuals were foreign-born. Death certificate data (sex, age, underlying cause of death and place of death) were obtained from the Swedish National Board of Health and Welfare. Information was obtained from the longitudinal integrated database for health insurance and labour market studies register (LISA) and the multigeneration register accessed from Statistics Sweden (SCB) about the following sociodemographic factors: geographical area, region of birth, single-person household, children below 18 years of age in the household, marital status and educational background. The data were retrieved during November 2020, and all retrieved data were coded so that no individuals could be identified.
Variables
The primary outcome variable for all analyses was place of death, categorized into three categories, that is, hospital (unspecified speciality within hospital), nursing home 28 (long- or short-term care facilities, primarily for older people) and own home. The underlying cause of death was grouped into 11 disease categories according to International Classification of Diseases, 10th Revision (ICD-10; Supplementary Table 1). The following individual and sociodemographic variables known to affect place of death were included in the analyses: sex (male/female), age, geographical area (urban/rural), marital status (married/unmarried/widowed/divorced), single-person household (yes/no), children below 18 years of age in the household (yes/no), educational background (operationalized according to the Swedish classification system SUN2000 into the following categories: no formal or elementary education, lower secondary education, higher secondary education, higher education) and region of birth (based on SCBs classification into the following categories: Sweden, Nordic countries except Sweden, EU28 except Nordic countries, Europe except EU28 and Nordic countries, Africa, North America, South America, The former Soviet Union, Asia and Oceania) (Supplementary Table 2). In addition, the variable potential palliative care needs (according to Murtagh et al. 29 – assigned as yes/no) was added (Supplementary Table 1).
Statistical analysis
Numbers and percentages were calculated for demographics and distribution of place of death among the foreign- and domestic-born population. For investigating variations in place of death and associated factors among foreign-born individuals, we started with performing univariable binary logistic regression modelling (Supplementary Table 3) to examine each variable by itself and see how much it contributes to the output. Then we continued with performing multivariable multinomial logistic regression analyses (Supplementary Tables 4–5, Table 3). Associations were evaluated using omnibus F-test. All statistical analyses were performed on all available data without imputation. Place of death was the dependent variable, and for multivariable analyses, complementary models were used controlling for different combinations of covariates and the known fundamental influencing factors were selected; while for each model, we stepwise added more uncertain variables (model 1 = sex, age; model 2 = sex, age, cause of death, potential palliative care needs and model 3 = sex, age, cause of death, children in the household, single-person household, palliative care needs, marital status, educational background, residing in urban area, and region of birth) to gain more insight into the respective role of these individual characteristics. Given the size of the studied population, a p-value of less than 0.001 was considered statistically significant. Area under the receiver operating characteristic (ROC) curve (AUC-statistics) was used for the goodness-of-fit. SPSS v28.01.0 (SPSS IBM Statistics) was used for the preparations of the variables. All analyses were performed using SAS® v9.4 (SAS Institute, Cary, North Carolina, USA).
Results
Demographic data
Of all adults dying in Sweden between 2012 and 2019, 11.5% were born abroad. The largest immigrant group was that of people who had migrated from other Nordic countries (46.9%) (Table 1). The mean age at death among foreign-born individuals was 76.6 (range, 18–115) years and, in the case of domestic-born individuals, this figure was 80.4 (range, 18–111) years. A lower percentage of foreign-born people died at an age greater than 90 years than domestic-born people (15.8% versus 25.7%). Of the foreign-born individuals, 93.5% resided in an urban area versus 88.2% of the domestic-born individuals. Diseases of the circulatory system were the most common underlying cause of death category among both foreign- and domestic-born people (33.8% and 35.7%, respectively). Overall, 78.7% and 78.5% of all foreign- and domestic-born people, respectively, died from conditions indicative of potential palliative care needs. Among these, 44% of the foreign-born individuals died in hospital versus 38.1% of the domestic-born individuals (Table 2).
Demographic characteristics of the population.

Percentages in parentheses are column percentages.
Total number of deaths ⩾18 years of age with a registered place of death in Sweden 2012–2019, n = 682,697.
Distribution of place of death. a
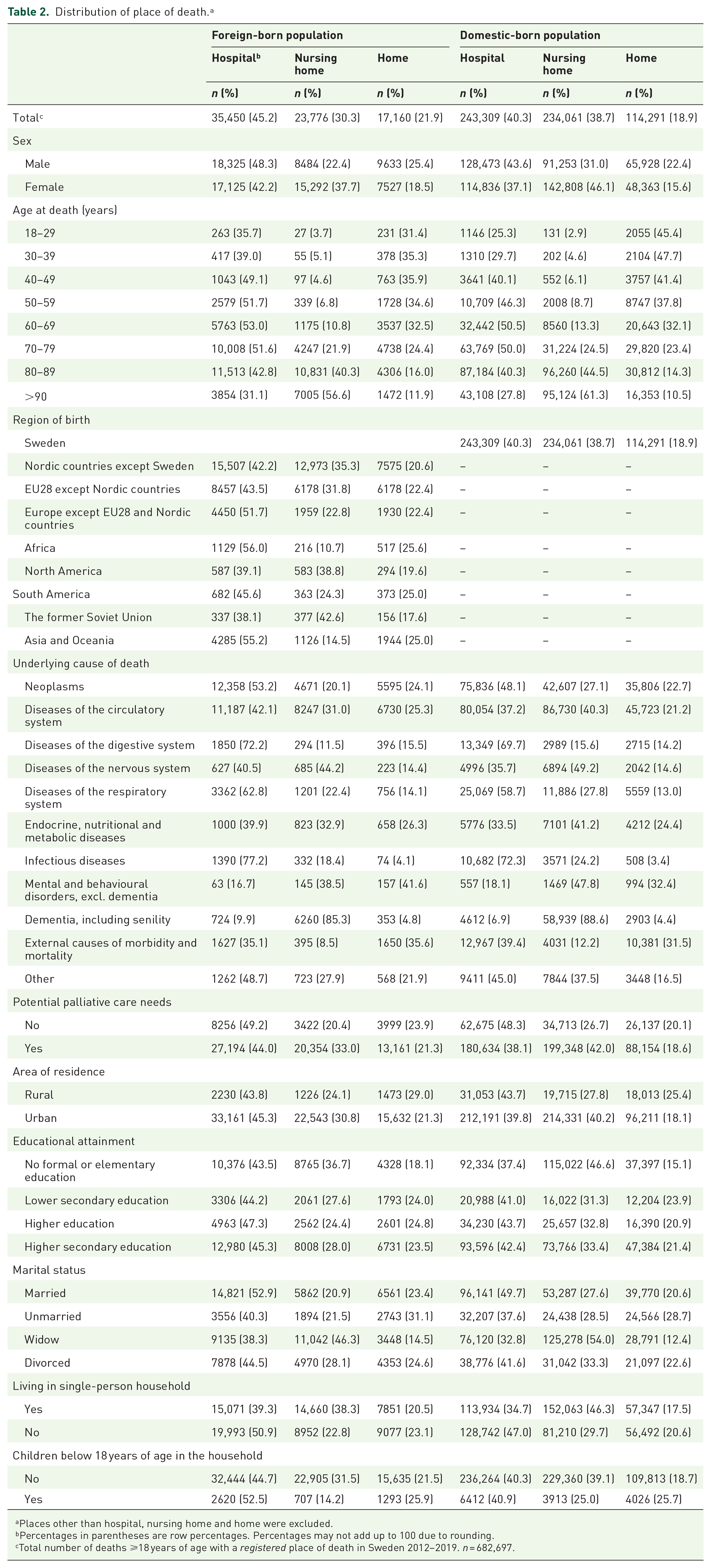
Places other than hospital, nursing home and home were excluded.
Percentages in parentheses are row percentages. Percentages may not add up to 100 due to rounding.
Total number of deaths ⩾18 years of age with a registered place of death in Sweden 2012–2019. n = 682,697.
Distribution of place of death by region of birth
Of all deaths among foreign-born individuals, 45.2% occurred in hospital, 30.3% in nursing home and 21.9% at home (Table 2). Among domestic-born individuals, 40.3% occurred in hospital, 38.7% in nursing home and 18.9% at home. People born on the African continent had the highest percentage of deaths in hospital (56.0%), followed by Asia and Oceania (55.2%). Individuals from the African continent had the lowest percentage of deaths in nursing home (10.7%), while individuals from North America had the highest (38.8%). Home deaths were more common among individuals born on the African continent (25.6%), followed by South America (25.0%), and Asia and Oceania (25.0%). Those born in the former Soviet Union had the lowest percentages of hospital (38.1%) and home deaths (17.6%).
Association between region of birth and place of death among foreign-born individuals
In the final model (compared to people born in Nordic countries other than Sweden), people from all regions of birth [except North America and the former Soviet Union (NS)] were less likely to die in nursing home than at hospital [odds ratio (OR) = 0.59–0.85; Table 3]. People born in EU28 except Nordic countries [OR = 1.07, 95% confidence interval (CI): 1.02–1.12] were the only group associated with a higher likelihood of dying at home than in hospital. By contrast, individuals from Europe (excluding EU28 and Nordic countries; OR = 0.84, 95% CI: 0.79–0.90), Africa (OR = 0.75, 95% CI: 0.66–0.85), and Asia and Oceania (OR = 0.77, 95% CI: 0.72–0.84) were less likely to die at home.
Multivariable multinomial logistic regression analyses of factors associated with the likelihood of dying in hospital versus dying in nursing home or at home, among foreign-born individuals. Final model 3.

CI, confidence interval; OR, odds ratio; ROC, receiver operating characteristic.
Odds ratio.
Confidence interval.
Factors associated with the likelihood of dying in hospital among foreign-born individuals
Foreign-born people dying from diseases of the digestive system (OR = 0.35, 95% CI: 0.30–0.41), respiratory system (OR = 0.59, 95% CI: 0.54–0.64), infectious diseases (OR = 0.49, 95% CI: 0.41–0.57) and external causes of morbidity and mortality (OR = 0.53, 95% CI: 0.45–0.62) as compared to people dying from neoplasms were more likely to die at hospital than nursing home (Table 3). Moreover, those dying from diseases of the digestive system (OR = 0.50, 95% CI: 0.44–0.57), nervous system (OR = 0.83, 95% CI: 0.70–0.98) and respiratory system (OR = 0.59, 95% CI: 0.53–0.64) were associated with less likelihood of dying at home than in hospital. Potential palliative care needs were associated with higher likelihood of dying both at nursing home (OR = 1.27, 95% CI: 1.16–1.38) and home (OR = 1.11, 95% CI: 1.02–1.21) than in hospital.
Among the foreign-born population, being female, as compared to male, was associated with a higher likelihood of dying in nursing home than in hospital (OR = 1.27, 95% CI: 1.22–1.33) and a lower likelihood of dying at home versus hospital (OR = 0.91, 95% CI: 0.87–0.95) (Table 3). All marital statuses, compared to Married, were associated with a higher likelihood of dying in nursing home versus hospital (OR = 1.35–1.58). Individuals who were unmarried at the time of death were associated with a higher likelihood (OR = 1.23, 95% CI: 1.14–1.32) of dying at home than in hospital, while this likelihood was lower in the case of widowed individuals (OR = 0.85, 95% CI: 0.79–0.91). Residing in an urban area, as compared to rural, was associated with less likelihood of dying at home versus hospital (OR = 0.75, 95% CI: 0.70–0.81).
Discussion
Main findings
The main result of this population-based study is variations in place of death in relation to region of birth. Foreign-born individuals from all regions of birth have higher percentages of home deaths (except the former Soviet Union) and hospital deaths (except North America and the former Soviet Union) than domestic-born individuals. This study also shows that compared to people born in Nordic countries other than Sweden, people from all regions of birth [except North America and the former Soviet Union (NS)] were less likely to die in nursing home than at hospital. The only group associated with a higher likelihood of dying at home than in hospital was people born in EU28 except Nordic countries.
Notably, individuals born in Africa, followed by Asia and Oceania, have the highest percentages of both home and hospital deaths and the lowest percentages of deaths in nursing home. Immigrants from the African continent, and Asia and Oceania differ the most from people born in the Nordic countries except Sweden.
What this study adds
Most studies investigating place of death focus on specific disease groups, geographic area or sociodemographic factors2,3,14,17,19,20,25,30–34 Our study focuses on all foreign-born adult individuals in the population and gives us a unique opportunity to map the place of death among foreign-born individuals and compare these results with place of death among domestic-born individuals.
In high-income countries, home death is often considered a desired or ‘good’ death, while in low-income countries, a home death might reflect lack of access to – and utilization of – modern healthcare services.35,36 This study shows that one-fourth of all deaths in Sweden, among individuals born in Africa, Asia and Oceania, and South America, are home deaths, compared with almost one-fifth among domestic-born individuals. At the same time, individuals from Africa, and Asia and Oceania are less likely to die at home than in a hospital, which agrees with the findings by Koffman et al. 19 and Coupland et al. 20 who found that individuals born in Asia and Africa, and ethnic minorities were more likely to die at hospital in the United Kingdom. A higher share of foreign-born individuals dies at home than domestic-born individuals – a result that we cannot account for without more research investigating preferences in place of death among these individuals to draw conclusions.
In accordance with previous research,1,2,37 this study confirms that hospital is the most common place of death in the overall population, although we did find variations in place of death in relation to region of birth. This study shows that depending on birth region, the proportion of hospital deaths ranges from 38.1% (individuals born in the former Soviet Union) to 56.0% (individuals born in Africa). Furthermore, among both foreign- and domestic-born individuals, nursing home was the second most common place of death (30.3% and 38.7%, respectively). The percentages of deaths in nursing homes range from 10.7% among those born in Africa to 42.6% among those born in the former Soviet Union. Foreign-born individuals had lower percentages of deaths at nursing homes and immigrants from all region-of-birth groups, except North America and the former Soviet Union (OR = NS), showed less likelihood of dying in nursing homes. As a group, foreign-born individuals die at a younger age than domestic-born individuals (76.6 versus 80.4 years of age, respectively), which might explain why foreign-born individuals are less likely to die in a nursing home. Most people being cared for in nursing homes are elderly and the mean age of individuals moving to nursing homes in Sweden in 2015 was 86.2 years among women and 83.7 years among men. 38 The utilization of nursing home beds among foreign-born individuals might also reflect a different care context in their home country. The culture surrounding nursing home beds might differ between the home country and host country, as might access to and knowledge of the nursing home setting. Sweden has a tradition of providing special care for elderly 39 and the numbers of nursing home beds (as a proportion of the population) are among the highest in the world. 40 Moreover, the mortality of a population is regarded as a measure of the population’s health and the difference in mean age at death might indicate and agree with previous research stating that foreign-born individuals in Sweden overall have worse health status. 41
Potential palliative care needs did not seem to affect the general patterns of place of death among the foreign-born population, although potential palliative care needs were associated with a higher likelihood of hospital deaths. Studies show that the degree of urbanization of the area of residence has an impact on place of death2,14,42 and this study supports previous research 14 stating that areas with a high level of urbanization were associated with a lower probability of dying at home than is the case for rural areas. In high-income countries, such as Sweden, there is a general trend of migration from rural/remote areas to cities, with new immigrants also settling in cities. 43 Of the foreign-born population included in this study, 93.5% were residing in urban areas and among them, residing in an urban area was associated with less likelihood of dying at home versus hospital.
Strengths and limitations
The main strength of this study is that the death certificate data include all individuals with a registered death from all areas in Sweden, including those individuals who were outside of Sweden at the time of death. The registers used in this study are considered to be very reliable, with a high degree of coverage. Using death certificate on population-level studies also provides limitations, one being inaccuracies in the registering of the underlying cause of death. The number of missing individuals in the death certificate is between 1% and 2%. Further limitations are that the data do not distinguish between (1) different types of immigration – a factor that we know can have implications for health – or (2) how long the individuals have lived in their host country, which may also affect health status. Hence, we cannot discuss migration experiences, which is important when discussing migrants’ health status. The categorization of region of birth is very broad and does not consider cultural and ethnic variations within each regional category. Moreover, the domestic national registers do not contain data that distinguish general (i.e. non-specialized) and specialized palliative care services on a population level. The findings from this study might reflect barriers (including infrastructure and competency) or different preferences regarding place of death – or even differences in terms of access to specialist palliative care since both Swedish and international studies indicate that foreign-born individuals and ethnic minorities are less likely to be cared for within specialized palliative care.19,26,44,45
Conclusion
To our knowledge, this is the first international population-based study using death certificate data to examine variations in place of death among the entire adult foreign-born population. We found considerable differences between regions of birth and place of death – in hospital, at home or in a nursing home. Overall, hospital was the most common place of death, followed by nursing home and home. Foreign-born individuals from all regions of birth had higher percentages of home deaths (except the former Soviet Union) and hospital deaths (except North America and the former Soviet Union) than domestic-born individuals. Of these, individuals born in Africa, Asia and Oceania, and Europe except EU28 and Nordic countries were found significantly less likely to die at home than in a hospital. Further research is needed to explore personal preferences regarding place of death, barriers and facilitators that influence access to preferred place of death and patterns of care at the end of life among foreign-born individuals.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524231185157 – Supplemental material for Place of death among foreign-born individuals: a national population-based register study
Supplemental material, sj-docx-1-pcr-10.1177_26323524231185157 for Place of death among foreign-born individuals: a national population-based register study by Emma Lundberg, Anneli Ozanne, Cecilia Larsdotter, Susanna Böling, Lisen Dellenborg, Daniel Enstedt and Joakim Öhlén in Palliative Care and Social Practice
Footnotes
Acknowledgements
The authors thank the ‘Place of death’ research group for valuable comments and discussions regarding the article. They also thank Statistiska Konsultgruppen and Hussein Hamoodi for conducting the statistical analyses.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.