
Abstract
The main component of error minimization in operating rooms (ORs) is to maintain high reliability of surgical teams. The analysis of adverse events in the OR reveals deficiencies in cognitive and interpersonal skills as the main factors influencing surgeons’ errors. Therefore, research of these additional factors is necessary, besides factors related to surgeons’ clinical knowledge and technical skills. In this paper, the key factors for evaluating activities in surgical operating rooms are identified. Fuzzy analytic hierarchy process is used for identification of key factors. Fifteen key factors are identified for evaluating activities in surgical operating rooms to improve the efficiency of surgical operations. For each group of activities (surgical “capabilities,” operating room characteristics, and non-technical skills), five factors are identified. As the most important, the following factors are obtained: communication, indoor environment standardization, and tool handle design. The aim of the analysis of these key factors is surgeons’ work capability enhancement, rational design of operating rooms, and advancement of operators’ cognitive and interpersonal skills.
Keywords
The analysis of adverse events in healthcare leads to the conclusion that most of them are not the consequence of inadequate use of technical skills or insufficient clinical knowledge of surgeons but not applying an ergonomic approach in designing space, devices, conditions, and interrelationships in the ORs.
The research defined in this paper opens new research field related to the improvement of cognitive and social skills of surgeons, as well as the improvement of their coordination, communication, and leadership during teamwork.
The contribution of this research is the formation of new methodological approach that leads to increased efficiency of operators in the OR and new quantitative method for research, the efficiency of teamwork in the OR, as well as possibility of applying the results of this research in a large number of medical institutions.
Introduction
The extent of ergonomic research on practical surgical activity in operating rooms (ORs) has improved significantly over the years, but the results of these studies are still insufficiently used. 1 The OR design requires multidisciplinary collaboration of experts, who use their expertise to achieve a common goal, which is designing a more efficient and more functional OR. 2 The OR environment consists of physical space, which has significant deficiencies,3,4 as well as equipment and people (medical staff and patients).
Surgical procedures are different types of interventions performed in operating rooms using instruments (tools). Various adverse events may occur during surgery. The causes of these events are various, and the hints are not predictable in advance. The analysis of risk events in healthcare leads to the conclusion that many causes of these events are of non-technical nature,5,6 such as communication,7,8 cooperation, coordination, and leadership. 9
Communication problems can affect safety and lead to injury of surgical patients. 10 In complex surgical procedures, teamwork, and coordination and communication skills are the essence of successful work.11,12 Greenberg et al. point out that the most common problems occur in the simplest communication pattern, verbal communication between the two people in the OR. 13 Burgener emphasize the importance of effective communication and teamwork in patient care, which is even more important during surgical interventions. 14 Communication problems can cause different types of adverse effects. Ineffective communication is the cause of numerous problems during surgical operations. 15
Stress can also affect surgeon’s performance. Certain level of improvement in performance under stress has been detected.16,17 The causes of stress may be technical flaws in the OR, time pressure, distractions, interruptions, or increased workload.18,19 In order to ensure the safety of patients undergoing surgical procedures, it is important that surgeons possess high mental judgment ability in the OR.20,21
Some operations are performed manually, using special tools that allow cutting and extraction, retraction, and sealing (closing the wound). Therefore, hand tool ergonomics is very important when considering activities in the operating room. Studies have shown that there are no significant differences in hand dexterity between medical students and other people, despite their commitment to surgery. 22 Others reveal decrease in hand dexterity over time.22,23
Standardization in the field of operating environment and equipment is a significant factor that affects quality of team work in the OR. Poor ventilation and increased temperature can lead to work-related errors, and the risk of infection increases.24-26 Inadequate noise, illumination, humidity, and temperature levels can negatively affect surgeons’ activity in the OR and patient’s safety. 27 Survey of surgical checklists and analysis after their application show that their introduction reduces mortality and morbidity in surgery.28-32
The analysis of literature showed that there is a lot of research on operative approaches of surgeons, their expert knowledge and abilities (sensory-motor capabilities and situational awareness), their workload (mental and physical) and workload-caused vulnerability (musculoskeletal disorders and hand dexterity).
However, research attention has not been focused on the ergonomic aspects in the design of ORs and working equipment (operating table and hand tools), the impact of working environment conditions on the work of surgeons (microclimate and noise), and importance of surgeons’ non-technical skills (group work, communication, cooperation, coordination and leadership, stress, and use of checklists).
Therefore, a new research procedure with the goal to improve surgeons’ working capacity, achieve more humane and rational design of ORs and devices, and improve surgeons’ cognitive and interpersonal skills is needed. It consists of systematic sequence of logically connected research activities, as shown in the following text.
Method
The analysis of factors affecting work efficiency in complex working environments and activities in such environments does not give a complete picture of the problem itself. An integrated and synergistic approach, taking into consideration a number of factors, leads to a more complete analysis of the problem. This approach is applied during the research presented in this paper.
For the purpose of ranking the key factors for activity assessment in surgical operating rooms, it is necessary to determine the most important factors and classify them into appropriate groups. Based on the analysis of the existing literature and previous analyses of different impacts of a working environment,33,34 fifteen key factors are identified and grouped into three major categories: surgeons’ capabilities, operating room properties, and non-technical skills.
The following methods were used for the analysis of selected factors: • Surgeons’ capabilities: Motor-sensor - response matrices; Mental workload - SWAT (Subjective Workload Assessment Technique); Situational awareness - CARS (Crew Awareness Rating Scale); Musculoskeletal disorders - OWAS (Ovako Working Posture Assessment System); and Hand dexterity - Manual dexterity aptitude test. • Operating room: Operating room design - ISO 11064 standard for control room ergonomics and simulation of Digital Human Models (DHM); Indoor environmental quality - standards defining measurement methods and application procedures for specific measurements, as well as ISO 14000 for environmental management and ISO 45000 for occupational safety; Visualization - Illuminance recommendations for ORs; Noise levels - Serbian national standard SRPS ISO 1996-1: 2019; and Tool handle design - scale for Local Perceived Discomfort (LPD). • Non-technical skills: Teamwork - Observational Teamwork Assessment for Surgery (OTAS); Leadership - The Oxford NOTECHS System; Communication efficiency - graphs and matrices (scope of communication, team connection, workload balance, and workplace isolation); Stress - Workplace stress scale (WSS); and Surgical safety checklist - WHO surgical safety checklist.
The main drawback of using a lot of factors is that all groups of factors and all factors do not have equal impact on the problem under consideration. The effect of certain factors has a more significant impact on surgeons' activities. That is the reason for the application of the group and factor ranking method, and the involvement of more experts in decision-making.
It is recommended to use the multi-criteria analysis method to determine the key factors of a complex problem. Based on the method presented in the aforementioned research, 33 for simpler understanding of the decision-making process and more accurate ranking results, the following factors are used: fuzzy numbers, analytic hierarchy process, and group decision-making.
The applied group fuzzy analytic hierarchy process consists of the following steps: (1) identifying the experts and assigning significance describing their influence on the final decision based on the level of experience; (2) creation of hierarchical structure of factors and groups of factors; (3) pairwise comparison groups and individual factors based on the proposed hierarchical structure using fuzzy numbers; (4) determining the aggregate patterns based on the comparison of individual experts and their roles describing their influence on the final decision; (5) determining fuzzy significance for groups of factors and individual factors based on obtained aggregate fuzzy patterns; (6) defuzzification (determination of crisp numbers based on fuzzy numbers), and ranking based on the obtained results.
Ranking determines the significance of individual factors and groups of factors for the purpose of using them in further analyses. The weights of individual experts are defined by gamma coefficient. 33 Based on the experience of an individual expert in the analysis of activity in the operating rooms (denoted by b k ) and experience in the analysis of activities in operating rooms adapted to certain types of operations (denoted by c k ), the value of γ k is determined. The scale for describing experience is 1 to 5. Based on Eq. (5), 33 a weight vector of experts Γ is obtained: Γ={0.09,0.13,0.09,0.19,0.13,0.13,0.09,0.06,0.06,0.04}.
On the basis of row geometric mean method (RGMM), aggregated matrices are determined. The consistency of individual expert comparison is verified using consistency index (CI), while the consistency of group decision-making is determined by centric consistency index (CCI). 35 Defuzzification is obtained using the mean aggregated weight method.
Results
During the analysis of surgical room activities at the Vascular Surgery Clinic, Clinical Center in Nis, hierarchy of factors is created (Figure 1). This hierarchy is used in the group ranking, involving 10 experts from different fields (ergonomics, medicine, information processing, and safety) by means of fuzzy AHP. Hierarchical structure of factors. Note: There are three groups of factors. The first group describes surgeons’ capabilities: mental and physical workload (S1), sensory-motor capabilities (S2), situational awareness (S3), musculoskeletal disorders (S4), and hand dexterity (S5). The second group describes operating room properties affecting the work efficiency: operating room design (O1), indoor environment standardization (O2), visualization (O3), noise (O4), and tool handle design (O5). The third group describes non-technical skills: teamwork (N1), leadership (N2), communication (N3), surgical safety checklist (N4), and stress (N5).
The expert group was composed of six surgeons from the Clinical Center Nis (endocrine surgeon, two orthopedic surgeons, two vascular surgeons, and neurosurgeon), one ergonomics expert, one safety expert, one mathematician, and one computer scientist. At the panel discussion, experts analyzed research goals, relevant literature data on this topic, and expectations of the authors. Based on the panel discussion, the authors formed a questionnaire with thirty potential factors, of which experts identified fifteen key factors. The analysis of completed questionnaires, with the consent of all experts, identified fifteen key factors.
Experts estimate activities using triangular fuzzy numbers and the following values of the fuzzified Saaty’s scale: identical (1,1,1), equally significant (1,1,3), more significant (1,3,5), much more significant (3,5,7), markedly more significant (5,7,9), and dominant (7,9,9). The factors are compared in groups, and pairwise comparison matrices are formed.
The Aggregated Matrix for Groups of Factors.

The Aggregated Matrix for Factors in Relation to Surgeons’ Capabilities (Group S), Operating Room Properties (Group O), as well as Non-technical Skills (Group N).

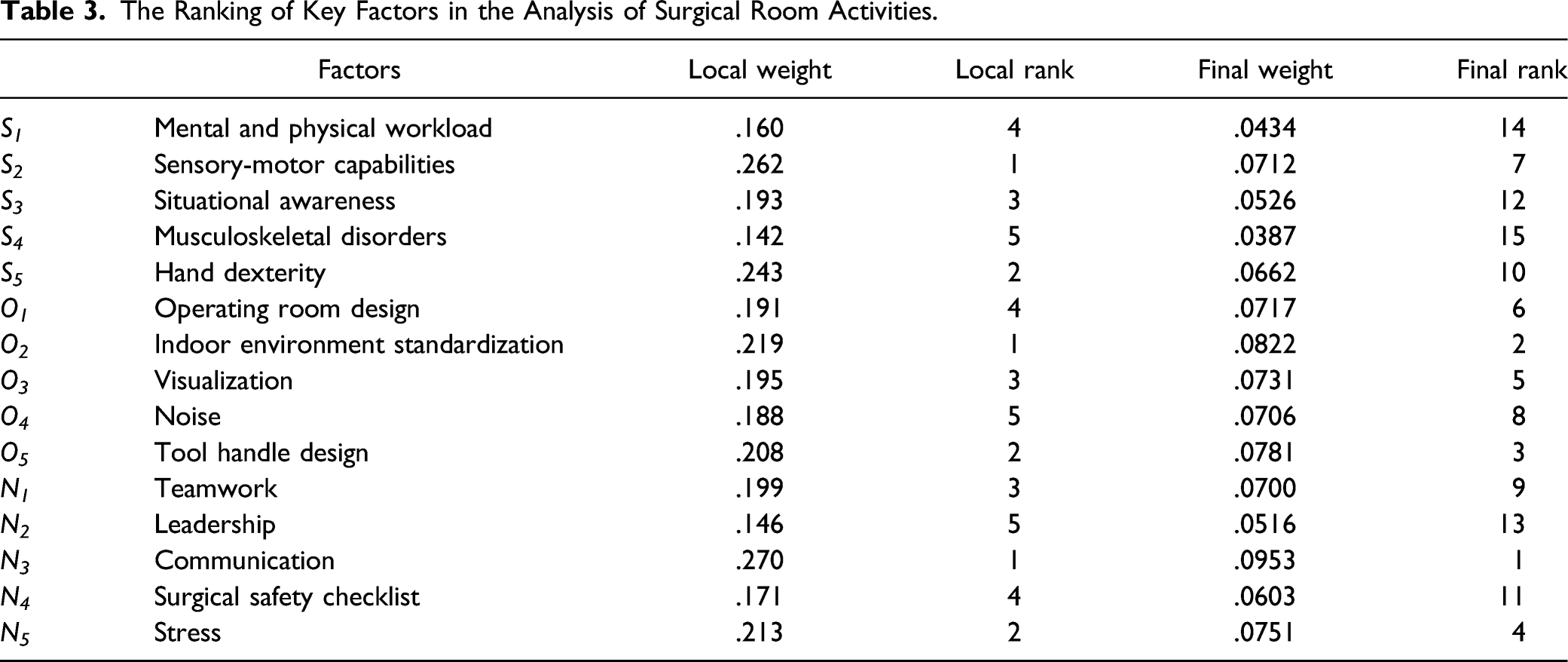
The Ranking of Key Factors in the Analysis of Surgical Room Activities.
At the Vascular Surgery Clinic, Clinical Center in Nis, Serbia (Figure 2), a communication efficiency investigation was conducted for groups of three and four surgeons (Figure 3), using graphs and forms. Evaluations of these investigations are presented in quantitative form.
34
Operating room in the vascular surgery clinic, clinical center in Nis. Communication scheme between three (a) and four (b) surgeons in operating room.

Discussion
The expert team applied this new synergistic methodological approach to ergonomic research in surgery during the analysis of surgeons’ activities from vascular, orthopedic, and neurosurgical clinics of the Clinical Center in Nis, in cooperation with experts in ergonomics, computer engineering, and safety.
Experts from different fields of research compare factors for activity analysis with more precision when using linguistic variables. Fuzzy numbers allow describing particular linguistic variables using a set of values from a certain range. Group decision-making reduces the subjectivity of the decisions of individual experts. A selection of appropriate experts (information processing, ergonomics, safety, and medicine) allows better problem assessment.
Based on the results of final ranking, shown in Table 3, the following can be concluded: the highest ranked group of factors is “Operating room properties” (O), followed by “Non-technical skills” (N), and “Surgeons’ capabilities” (S). Among the factors, the highest ranked factors belong to groups Operating room properties (O) and Non-technical skills (N). Among them, the most important is Communication.
Failures in the transmission of information and communication are common in surgical practice. Therefore, a review of published literature data is performed using Medline, Embase, PsycINFO, ScienceDirect, and interviews with surgical team members.
Different communication patterns are identified in surgical teams.36,37 Information transfer can be different in manner and tension level among team members. The way of information transfer is defined by the number of team members, communication channels, team members and their roles, and events during surgical operations (normal or emergency activities). Communication before operation can be very helpful in avoiding errors during operations. Many authors emphasize that the lack of communication before operation and ineffective communication during operation are the most important causes of errors during surgical operations. Therefore, the research on efficient communication patterns during surgical operations is important because these patterns enable the formation of standardized communication, through checklists, forms, and technological innovation, which improves the quality of transmission and communication in surgical operating rooms.
Lingard et al. identified the following key factors causing problems during communication in the OR: problems with timing; insufficient or inadequate information; unidentified goals; inadequate group composition causing decreased collaboration; and communication tension. 15
Team performance in surgery is increasingly seen as crucial for safety. Through the analysis of data, three themes are created that illustrate communication culture of team work in surgery: “building shared understandings through open communication,” “managing contextual stressors in a hierarchical environment,” and “intermittent membership influences team performance.” 38 In creating a security culture in a health organization, the optimal results of the team rely on open discussion on team work and team expectations, and significantly depend on how organizational culture promotes such discussion.
Inadequate communication and team factors are the main causes of errors during surgical operations.15,39,40 The development of different methodological approaches in recent years has significantly improved research on communication in teamwork in healthcare. These studies are supported by studies that investigate causes of adverse events and impact of better communication of team work on the prevention of these events, quality of communication by health service providers, and various forms of communication, coordination, and leadership that support effective teamwork. 41
The experts emphasized the importance of effective communication and coordination of activities during the surgical operations, helping surgeons during effective performing of tasks, activity coordination, and performing activities during adverse events in the OR.
The significance of the research of ergonomic aspects in surgical activities consists of the definition of approach describing the improvement of surgeons’ capabilities. It also leads to improvement of surgeons’ non-technical skills, more humane OR design, quantification of communication efficiency, and overall OR team work efficiency. However, there are some limitations for this study. First, the anthropometric research methods determining the dimensions of the surgeon’s body and body parts were not applied. The anthropometric dimensions significantly affect ergonomic design of the equipment in the OR. Second, the research should be additionally supported by biomechanical-kinesiological research methods to analyze movements of the surgeon’s hands during surgical procedures and determine maximum force. The reliability of the surgeon’s should be also analyzed, that is, errors during the work, to reduce their number, and the consequences. Future research should be based on the development of new valid research tools that quantify research results to support descriptive explanations.
Conclusion
Significant numbers of adverse events in surgical practice occur due to non-application of research approaches related to surgeons’ capabilities, operating room properties, and non-technical skills, and not due to essential requirements in surgery related to application of clinical knowledge and surgeon’s technical skills. Therefore, it is necessary to supplement knowledge with research and identify other causes of adverse events in ORs.
In this paper, the expert team ranked 15 factors representing the causes that affect surgeons’ efficiency in operating rooms. The analysis is based on multidisciplinary ergonomic approach. The application of results is necessary for further improvement of surgeons’ efficiency, and better and more humane design of ORs. The results of this research are the basis for further research of the efficiency of professional medical staff.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.