
Abstract
This study aims at exploring the trends and socioeconomic inequalities in the use of maternal healthcare utilization between 1997 and 2014. Data were analyzed using descriptive and multivariate regression methods. Women in the higher wealth quintiles (Q4 and Q5) generally had higher prevalence of using health facility delivery and postnatal care services compared with those in the lower wealth quintiles (Q1 and Q2), whereas the prevalence of timely and adequate antenatal care visit was comparatively higher among those in the lower wealth quintiles. Findings indicated important sociodemographic inequalities in using maternal healthcare services, addressing which may help promote the utilization of these services.
Firstly, Promoting the use of basic maternal healthcare services such as antenatal care, health facility delivery and postnatal care constitute the key strategies to curb maternal and child mortality in low-income settings. Secondly, a large number of countries in Africa, including Zambia, are struggling to improve the coverage and utilization of these affordable and life-saving services. Thirdly, more research evidence is necessary to understand the trend and socioeconomic disparities in the use of maternal healthcare services.
This study is the first to report the pattern of using basic maternal healthcare services in nationally representative sample in Zambia covering the period between 1997 and 2014. Findings suggested an overall progress in usage of maternal healthcare utilization since 1997, expect for the adequate ANC visits that has been declining since 2002. Important sociodemographic disparities were observed in the odds of using the services, among which the most notable were women’s education, ethnic background, wealth status of the household, parity, education of the husband and exposure to family planning communication through mass media.
Improving maternal healthcare uptake in Zambia should focus on addressing the sociodemographic inequalities that prevent women from accessing the available services.
Introduction
Zambia is a land-locked country in Southern Africa with around two-third of the total population living below international poverty line. 1 Despite being one of the fastest growing economies in Africa, a large proportion of the Zambian population is still facing significant challenges in meeting the basic amenities such as proper housing, access to clean water, and sanitation and healthcare. The demography is characterized by widespread poverty, food insecurity and malnutrition, and a fragile healthcare system which are contributing to high burden of maternal and child mortality in the country. Historically, Zambia has a high maternal mortality ratio2,3 which, even after an appreciable progress during last two decades, 4 remains one of the highest in the world (398 in 2014 vs 577 in 1990).5,6 Zambia’s situation of poor healthcare condition is not unique in the continent as most of the African countries failed to meet the maternal and child health related Millennium Development Goals such as reducing maternal mortality ratio between 1990 and 2015 by the 75%.7,8
A large number of studies have highlighted the importance of socioeconomic factors in maternal health and healthcare service utilization related outcomes.4,8-10 Although healthcare seeking as a behavior is considered to be driven to a great extent by perceived need of care and health literacy, the critical role one’s financial capacity to medical services cannot be overestimated especially in the low-income countries like Zambia where there is not universal healthcare system to safeguard the health needs of the disadvantaged communities. This growing popularity of social cash transfer programs to promote maternal health provides a strong evidence on the role of socioeconomic determinants as well. In Zambia, the social cash transfer program to address maternal mortality has proven to be a success story. Strong commitments by the government and partnership with international collaborators such as World Health Organization have opened avenues for lager success as well. In 2007, the Zambian Ministry of Health implemented a new WHO-recommended roadmap for reproductive health including the maternal death review (MDR) system in line with World Health Organization recommendations which was able to reduce maternal mortality rates to a great extent in the country. 9 Another mention-worthy example of private-private partnership the Saving Mothers, Giving Life (SMGL) program that is target to reduce maternal mortality through a systems approach and healthcare capacity building. 4
The causes of low maternal healthcare services uptake are numerous and multifaceted, and broadly classified into behavioral, cultural, economic, and sociodemographic factors at individual level and remoteness of health facility, inadequate infrastructure and skilled human resource for healthcare at community level.10-14 A large number of studies has been conducted on Demographic and Health Survey data that adopted the Andersen and Newman Behavioral Model to identify the factors associated with poor use of ANC, facility delivery, and postnatal services.15,16 To date, there is no such study or report available for Zambia, and thus the factors behind the low utilization of maternal healthcare services are not yet fully understood. Although a few subnational studies have been conducted,14,17,18 there remains a lack of comprehensive research data showing the full spectrum of maternal healthcare services use such as timing and adequacy of antenatal care, health facility delivery, and postnatal care. Therefore, the present study was conducted to explore the factors associated with these four components of maternal healthcare using nationally representative data from Zambia Demographic and Health Surveys (DHS) conducted since 1996-1997. DHS provides information on a wide range of demographic and socioeconomic factors which were selected systematically to fit within the scope of the Andersen and Newman Behavioral Model. Findings of the present study are expected to enhance the understanding of the enabling and predisposing factors associated with the uptake of maternal healthcare services in Zambia as well as in the neighboring countries with similar economic and sociocultural environment.
Materials and Methods
Setting
Data for this study were collected from the last four rounds of Zambia Demographic and health survey (ZDHS 1997, 2002, 2007, 2014). These surveys are conducted by Central Statistical Office (CSO) in partnership with the Ministry of Health. Financial assistance was provided by the Ministry of Health and United States Agency for International Development (USAID) along with technical assistance by ICF international. The main purpose of these surveys is to provide quality information for monitoring and evaluation of population health programs and assist in evidence-based health policy making. DHS surveys employ multistage cluster design for sample selection and are conducted by face-to-face interviews on eligible men (15–59 years), women (15–49 years), couples, and households. 19
Details of the Zambia Demographic and Health Surveys.

List of provinces: Central, Copperbelt, Eastern, Lusaka, Luapula, Muchinga*, Northern, North-Western, Southern, and Western (*newest province).
Central Statistical Office (CSO) [Zambia], Ministry of Health (MOH) [Zambia], and ICF International. 2014. Zambia Demographic and Health Survey 2013-2014. Rockville, Maryland, USA: Central Statistical Office, Ministry of Health, and ICF International. *
Outcome Measures
The outcome variables of interest were: (1) timing of first antenatal care, (2) frequency of antenatal care, (3) facility delivery, and (4) postnatal care for the latest childbirth occurring within the last five years from the survey. All of these items are assessed based on the self-report of the participant. Timing of first antenatal care was classified as timely (if within the first trimester) and late (if beyond the first trimester).
20
Frequency of antenatal care visits was defined as adequate and inadequate as per World Health Organization recommendation.
21
Facility delivery was defined as childbirths occurring at any healthcare institution, and home delivery if otherwise.
22
Use of postnatal care (Yes/No) was assessed by asking whether or not the respondent underwent any health check-up by a health professional after delivery. This study considered a postnatal check-up within 48 hours after birth as a potential maternal healthcare indicator as per the WHO. (Figures 1-4) Maternal healthcare utilization by type. Figure 1 shows that prevalence of women making the first ANC visit within the first trimester has increased from 11.8% in 1996-1997 to 23.9% to 2013-2014, whereas that of making at least 4 ANC visit has decreased from 72.3 to 55.3% in 2013-2014. The prevalence of health facility delivery (44.2% in 1996-1997 vs 73.4% in 2013-2014) and postnatal care (43.8% in 2002 vs 73% in 2013-2014) has also increased substantially during the same period. Maternal healthcare utilization by age groups. Figure 2 shows the prevalence of maternal healthcare services across age groups. The prevalence of timely ANC visit, health facility delivery, and postnatal care were higher among those aged between 20 and 34 years than the adolescent and those aged above 34 years. Maternal healthcare utilization by educational level. Figure 3 shows the prevalence of maternal healthcare services according to educational level. The prevalence of timely ANC visit, health facility delivery, and postnatal care were higher among those aged between 20 and 34 years than the adolescent and those aged above 34 years. Women who had no education had the lowest prevalence of making timely and adequate ANC visits, facility delivery, and postnatal care, while those had primary level education had the highest prevalence of using these services. Maternal healthcare utilization by household wealth quintile. Figure 4 shows the prevalence of maternal healthcare services according to household wealth status. Women in the higher wealth quintiles (Q4 and Q5) generally had higher prevalence of using health facility delivery and postnatal care services compared with those in the lower wealth quintiles (Q1 and Q2), whereas the prevalence of timely and adequate ANC visit was comparatively higher among those in the lower wealth quintiles.



Explanatory Variables
Selection of explanatory variables was guided by Andersen’s behavioral model of health service utilization which postulates that healthcare utilization is a function of three major factors: (1) predisposing factors, (2) enabling factors, and (3) need factors. 16 For this study, the data were secondary and hence the selection of the explanatory variables in line with the behavioral model was not possible. To this effect, the three sets of factors were met by using proxy indicators. Predisposing factors were indicated by the sociodemographic variables including: age (15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49 years), residency (urban, rural), religion (Christian, other), ethnicity (Bemba, Tonga, Chewa, Other), parity (1–2, >2 children), and sex of household head (male, female). 23 Enabling factors were indicated by women’s education (none, primary, secondary/higher), employment (none, professional, eg, sales/services, agriculture/other manual), household wealth quintile (Q1/richest, Q2/richer, Q3/middle, Q4/richer, Q5/poorest) and husband’s education (none, primary, secondary/higher). 16 Wealth quintile refers to household wealth quintile scores which is performed by principal components analysis, based on a selected range of household assets, for example, number of household members, floor, wall and roof material; type of cooking fuel; access to potable water and sanitation, ownership of radio, TV, refrigerator, motorcycle, and others. Based on their wealth scores, households fall into five wealth quintiles ranging from poorest to richest (poorest, poorer, middle, richer, richest). 25 Need factors were proxied by encountering family planning (FP) related message in newspaper (Yes/No), radio (Yes/No), and TV (Yes/No). 23 Measurement technique for wealth quintile was published elsewhere. 24 The assumption was that women access mass media channels for information related family planning and childbirth related services. Making ANC visits was also regarded as a need factor for facility delivery and postnatal care. 12
Statistics Analysis
Data were analyzed with Stata version 14. Datasets were merged and cleaned by applying the inclusion criteria: experience of at least 1 childbirth in the preceding 5 years. As the surveys used cluster sampling techniques, all analyses were adjusted for this by using the svy command. 26 This command uses the information on sampling weight, strata, and primary sampling unit provided with the datasets. Following that, the dataset was accounted for the cluster sampling design, sampling strata and weight by using complex survey mode. Sample characteristics were described as percentages. Prevalence of antenatal care, facility delivery, and postnatal care was presented as bar charts. Following that, multinomial logistic regression models were used to estimate variations in the odds of receiving the maternal healthcare services. Results of four outcome variables were presented in four separate tables, each divided into three subsamples: overall, urban, and rural.
Results
In total, 22,605 women were included in the study from the four surveys: DHS 1996-1997 (4615), DHS 2002 (4491), DHS 2007 (4148), and DHS 2013-2014 (9351). Sample characteristics were provided in the appendix (Table A). In short, majority of the women were aged between 20 and 24 years, rural residents, followers of Christianity, of Bemba ethnicity, had more than two children, lived in male-headed households, had primary level education, and had outdoor employment.
Descriptive Analyses
Multivariate Analyses
Predictors of Timely Initiation of First Antenatal Check in Zambia. (n = 22 591) ZDHS 1997–2014.

Exponentiated coefficients; 95% confidence intervals in brackets.
cP < .05.
aP < .01.
bP < .001.
Predictors of Making at Least one Antenatal Check in Zambia. (n = 22 591) ZDHS 1997–2014.

Exponentiated coefficients; 95% confidence intervals in brackets.
aP < .05.
cP < .01.
bP < .001.
Predictors of Adequate Antenatal Checks in Zambia (n = 22 591) ZDHS 1997–2014.

Exponentiated coefficients; 95% confidence intervals in brackets.
cP < .05.
bP < .01.
aP < .001.
Predictors of Using Health Facility Delivery Services in Zambia. (n = 22 591) ZDHS 1997–2014.
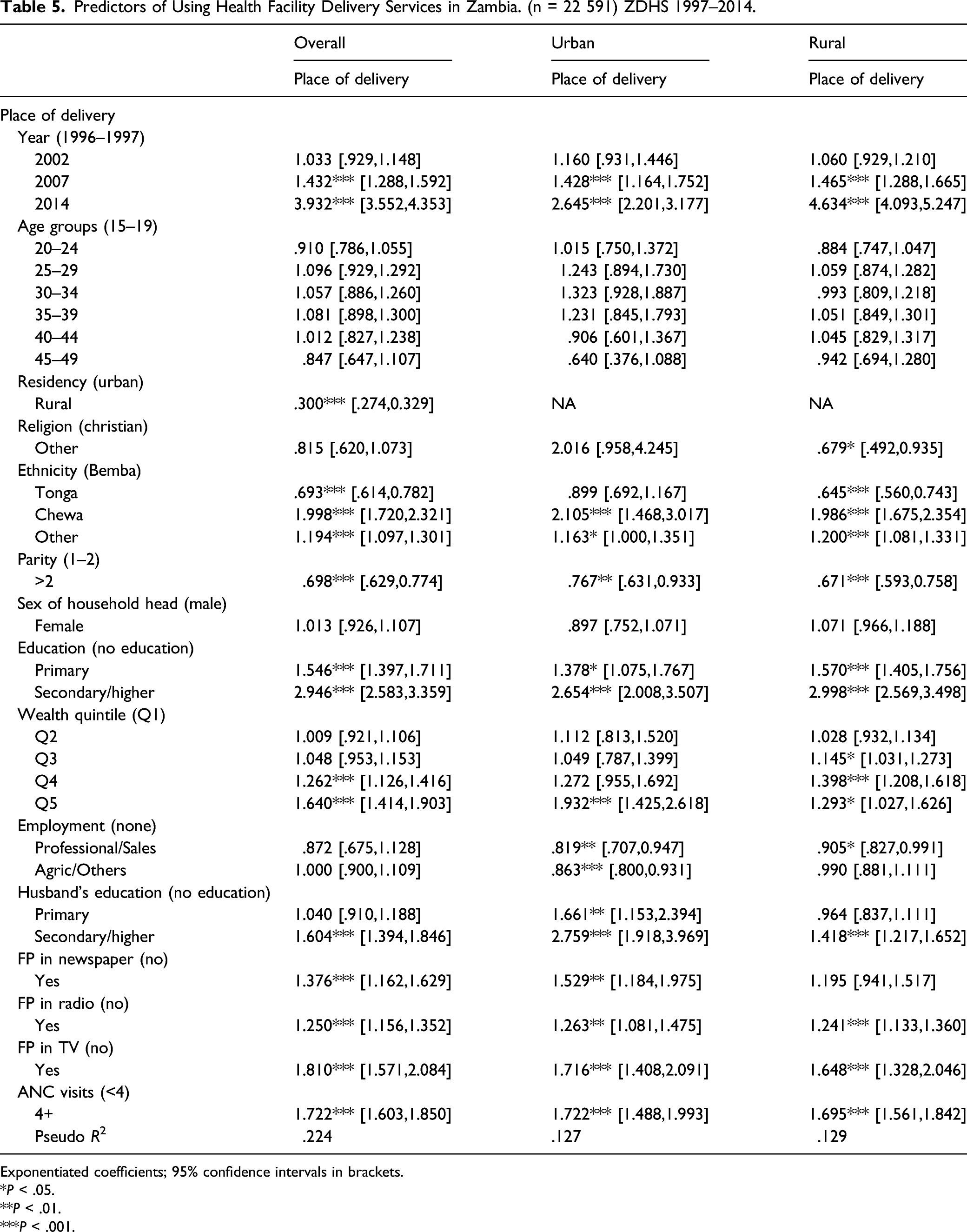
Exponentiated coefficients; 95% confidence intervals in brackets.
*P < .05.
**P < .01.
***P < .001.
Predictors of Taking Postnatal Care in Zambia. (n = 16 472) ZDHS 1997–2014.

Exponentiated coefficients; 95% confidence intervals in brackets
*P < .05.
**P < .01.
***P < .001.
Compared with women who had no formal education, those who had primary and higher education generally had significantly higher odds of having adequate ANC visits, health facility delivery, and postnatal care. Women from the highest wealth quintile households have higher odds of timely initiation of ANC [OR = 1.178, 95%CI = 1.013,1.369], adequate ANC [OR = 1.424, 95%CI = 1.059,1.913], health facility delivery [OR = 1.640, 95%CI = 1.414,1.903], and postnatal care [OR = 1.228, 95%CI = 1.048,1.439]. Regarding ANC visits, the association was significant only for those in the second wealth quintile and in the urban areas [OR = 2.54, 95%CI = 1.042,6.216]. For health facility delivery, wealth quintile didn’t show any significant association; however, for PNC the odds were found to be noticeably higher for higher wealth quintiles especially in the urban areas. Non-Christian women in general had lower odds of using most of the maternal healthcare services. Compared with Bemba, belonging Chewa ethnicity showed a positive effect on all the outcome measures except for timely initiation of ANC visits. Having more than 2 children were inversely associated with adequate ANC, health facility delivery, and postnatal care services. Regarding media use, encountering FP related message on newspaper, radio, and TV showed a positive association with all types of the maternal healthcare services. Women with husband’s having secondary/higher education showed a protective effect on using ANC, health facility delivery, and postnatal care services. Women who made at least four ANC visits had significantly higher odds of using facility delivery [OR = 1.722, 95%CI = 1.603,1.850] and postnatal care [OR = 1.378, 95%CI = 1.262,1.504] as well, and this association was significant for both urban and rural areas.
Discussions
Optimal utilization of maternal healthcare services is essential for ensuring better pregnancy outcome and consequently the health of future generations. A healthy pregnancy determines not only the health of the newborn but also has a major impact on adult health with broader and long-lasting implications for national human development efforts. Data-based evidence is therefore necessary to inform the ongoing programs working to meet the maternal health related targets such as Sustainable Development Goals. The current study provides an insight on the prevalence and predictors of the three crucial components of maternal healthcare including antenatal, skilled birth attendant, and postnatal care services. The findings indicate that the proportion of women making their first ANC visit within the first trimester has been increasingly albeit slowly since 1997. The prevalence of women of making at least one ANC visits has also increased during the same period, however, that of making four or more ANC visits has been decreasing since 2002. This finding is potentially alarming one and the cause behind this negative trend requires further investigation. A possible explanation might be that women who received care once didn’t seek further assistance owing to unsatisfactory service quality. Patience dissatisfaction in maternal healthcare service such as ANC is common in African settings,27,28 and has been shown have negative effects on subsequent healthcare visits including low level of institutional delivery. 29
Despite the lower prevalence of adequate ANC visits, the average prevalence of facility delivery has been increasing since 1997. The prevalence of women delivering at health facility for the four surveys were 57.7% and has improved from 44.16% in 1996–1997 to 73.37% in 2013–2014, which is higher than the sub-Saharan African average of about 50%. 30 As expected, the prevalence of receiving PNC has also increased from over two-fifth (43.7%) in 1997 to around three-quarter (73%) in 2013-2014. The positive effect of using skilled birth assistance on taking PNC was reported in Ethiopia 31 and Tanzania. 32 Also worthy of note is the age and educational difference in the uptake of all type maternal healthcare services. For instance, the prevalence of timely ANC visit, health facility delivery, and postnatal care were generally higher among women aged between 20 and 34 years and lower among the adolescent and those aged above 34 years. In a recent study on Demographic Health Survey data from seven countries (Bangladesh, Cambodia, Cameroon, Nepal, Peru, Senegal, and Uganda), similar patterns of using ANC and facility delivery were reported. 33 Non- and inadequate use of healthcare among the adolescent women is common issue that needs to be addressed to promote the prevalence of maternal health service utilization.
In addition to age, the descriptive analyses also revealed noticeable disparities in the use of the four types of services among different education subgroups. Women with no education had lower prevalence of taking ANC, facility delivery and PNC services than those who had primary and higher education. The positive effect of education on healthcare service utilization in general can be interpreted through its enabling mechanism. Educated individuals are more likely to be health aware, that is, concerned of their health status and need for timely medical services 34 and have better capacity to afford the services compared with those without education. 35 A multicountry study (DR Congo, Egypt, Ghana, Nigeria, and Zimbabwe) based on Demographic and Health Surveys data reported that women’s education had significantly positive effect on taking professional ANC, timing and frequency of ANC visits, facility delivery. 36 These finding is well in line with those from the present study; women having primary and higher education had significantly higher odds of taking adequate ANC, facility delivery and PNC services. However, it is important to note that primary education showed a positive association with early ANC contact in urban sample only, but not on rural sample. In a similar context, having leant about family planning from newspaper, TV, and radio showed a positive association with the utilization of all type of maternal healthcare services. Interestingly, husband’s educational status also appeared to be an important predictor adequate ANC, facility delivery, and PNC services. These findings imply the need for continued effort to improve women’s education status and health communication through mass media channels to promote the use of maternal healthcare services in the country.
Significant economic (wealth quintile), geographic (urban/rural), and cultural differences (religion/ethnicity) were also observed in the odds of utilizing the maternal healthcare services. Those in the highest wealth quintile (Q5) had significantly higher odds of timely initiation of ANC visits. We didn’t find any significant association with facility delivery. In contrast, the odds were remarkably higher for higher wealth quintiles, especially in the urban areas. This urban-rural difference in wealth quintile might be indicative of the influence urban poverty, and the absence of significantly wealth inequality in the rural areas. The varying degrees of sensitivity of the outcomes variables to household wealth status are interesting findings and provide the impetus for further analysis to explore the underlying mechanisms. Women in the rural areas had higher odds of making early ANC contact, but lower odds of using facility delivery and PNC services. Having an employment did not show any strong impact in particular; however, higher parity showed a negative association with taking the services. Interestingly, the odds of wealth quintile were not as pronounced as educational status, despite the fact that these 2 indicators usually show similar effect in terms of healthcare utilization. The present findings showed that women from higher wealth status households generally had higher odds of having used adequate ANC, facility delivery and PNC services. For PNC, the effects are particularly higher among urban women. The underlying mechanisms behind these differential effects of the different predictors are hard to pinpoint by quantitative methods, and therefore calls for more comprehensive and qualitative studies. Nonetheless, the findings offer plenty of insight into the diverse sociodemographic factors that influence the use of maternal healthcare services in Zambia. Policy efforts to improve maternal healthcare service utilization should therefore focus on developing innovative interventions strategies to address the sociocultural barriers to accessing care. Evidence-driven social determinants based approach by incorporating the specific needs of subpopulations may facilitate a more equitable provision of these essential and life-saving healthcare services to the vulnerable communities.
Findings of the present study fill an important gap in the literature. Main strengths were the use of nationally representative data from four rounds of survey that allows making a generalizable conclusion about the prevalence and associations. The use of Andersen and Newman Behavioral Model and methodological rigor in the analyses add further strengths to the findings. Nonetheless, this study has several limitations to report. First of all, the data were cross-sectional and hence no causality can be inferred from the associations. The data were secondary and authors have to influence over the selection and measurement of the variables. As the data were self-reported, the chances of recall and reporting bias cannot be ignored.
Conclusions
The finding of this study reveals an overall progress in usage of maternal healthcare utilization in Zambia. The prevalence of women making the first ANC visit within the first trimester has more than doubled between 1996–1997 and 2013–2014, while that of having adequate ANC visits have decreased by a considerable margin. Important sociodemographic disparities were observed in the odds of using the services, among which the most notable were women’s education, ethnic background, wealth status of the household, parity, education of the husband, and exposure to family planning communication through mass media. Barriers to maternal healthcare utilization highlighted by the socioeconomic and cultural inequalities should be given special attention in designing intervention programs.
Footnotes
Acknowledgments
We are appreciate the author of Southwest University of Political Science and Law (Zhifei He), who contributed to initial drafting and writing, as well as the data analysis. We appreciate the authors of Ottawa University (Ghose Bishwajit), who contributed a lot in data collection and analysis. Meanwhile, we appreciate the authors of Southwest University of Political Science and Law (Caihua Zhang, Shiming Wang, Xinglong Yang) who contributed to the revisions in the final manuscript.
Authors’ Contributions
ZFH contributed to the conception and design of the study and data analysis. ZFH, GB performed data collection and analysis. GB, ZHC, XLY contributed to the final review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article we are appreciated the National Social Science Foundation of China (No.20XGL027), Chongqing Education Commission Base Project of Humanities and Social Sciences (No.21SKJD012), and 2019 Southwest University of Political Science and Law Project (No.2019XZQN-30), which provides the funding support.
Ethical Approval
Dataset is available from the DHS website to registered users; therefore, no additional approval was necessary.