
Abstract
Background
Patients with chronic low back pain can contribute to a global socioeconomic burden. Current international recommendations emphasize that low back pain management should occur at the primary-care level. However, there is a lack of essential services for low back pain management at the primary-care level in Saudi Arabia. We explored the current state of low back pain management in Saudi Arabia from the perspective of spine surgeons and physiotherapists.
Methods
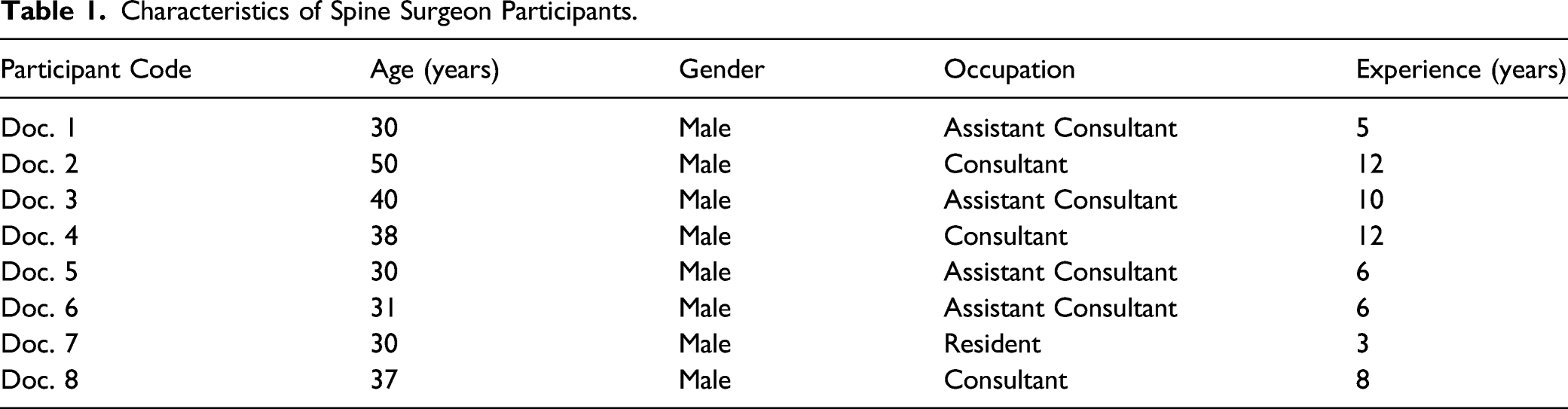
A qualitative study with semi-structured interviews was conducted on spine surgeons and physiotherapists. A total of 17 healthcare workers, 8 spine surgeons (age range 28–49 years) and 9 physiotherapists (age range 30–49 years) participated in the study. Data were recorded and analyzed thematically.
Results
Three main themes were identified from the interview data that outlined current low back pain management in Saudi Arabia: clinical guideline availability and pathways of care, utilization of primary care services, and overutilization of secondary care resources.
Conclusions
This study suggests underutilization of primary care services and overutilization of secondary care services in Saudi Arabia. Therefore, the implementation of local clinical guidelines could improve patient care as well as reduce the cost of low back pain management.
Background
Low back pain (LBP) is the number one cause of disability globally, affecting 540 million people at any one time, and the global burden of LBP is projected to increase. 1 Most of the LBP cannot be linked to specific detectable abnormality in the spine, and therefore, clinical practice guidelines are against the routine use of diagnostic imaging. 2 There is a call for action to address the widespread misconceptions especially among health professionals, about the LBP causes, prognosis, and effective treatments and to get rid of the outdated models of care. 3
The Ministry of Health (MOH) is the primary healthcare provider in Saudi Arabia. There are 3 hierarchical levels of care within the MOH—primary, secondary, and tertiary, 4 that provide preventive, curative, and rehabilitative healthcare for Saudi citizens. 5 There are 2325 primary healthcare centers (PHCs) in Saudi Arabia, providing curative and preventative services, as well as referrals to secondary healthcare centers. 6 Additionally, the number of private healthcare facilities is increasing; recent MOH statistics show that there are 152 private hospitals across the country. 7 According to the World Health Organization, the secondary level of healthcare is defined as one provided at the hospitals having 5 to 10 clinical specialties and size ranging from 200 to 800 beds. 4 Tertiary level of healthcare is one step ahead of the secondary level and is defined as one in which highly specialized personnel and electromedical equipment are available and the bed strength of the hospital has a range of 300 to 1500 beds. 8
Currently, there are no established pathways of care or clinical guidelines for patients with low back pain (LBP) in Saudi Arabia. Patients may visit a general practitioner (GP) at a PHC or pay out-of-pocket to see a spine consultant at a private hospital without a GP referral. GPs in PHCs can refer patients to a consultant at a higher-level center for services that are unavailable at the primary-care level, such as physiotherapy, advanced imaging, and laboratory tests. This process extends the time patients have to wait to see a physiotherapist (PT) up to 4 months, which for some patients may adversely impact recovery
42
(see Figure 1). Illustrated process for receiving physiotherapy services in Saudi Arabia. Reprinted with permission from “Psychosocial Factors Associated with an MRI Diagnosis of Chronic Non-specific Low Back Pain in Saudi Arabia” by A. Alhowimel, 2019, Doctoral dissertation, University of Nottingham.
As evident in Figure 1, patients with lower back pain in Saudi Arabia have 2 options. They can either visit the governmental primary healthcare centers or pay for private healthcare for themselves. LBP patients presenting to the private hospitals are directly seen by specialist (orthopedic, spine, or neurosurgeon) who might refer them to physiotherapy within 2 weeks from the start of the complaint. Alternatively, if they chose to visit governmental primary care, they are required to present to the primary care general practitioners who refer them to secondary care level facilities where they are seen by specialist. Afterward, specialists can refer the patients to physiotherapy service which might take 8–12 weeks from the start of the complaint.12,42 The role of general practitioners and family physicians at the primary care level, therefore, is restricted only to referral in case of lower back pain, majority patients of which ultimately require physiotherapy. 12
Current international guidelines emphasize that LBP patients should receive treatment at the primary-care level, since only some cases will require a specialist referral. 9 However, there are notably no clinical guidelines or pathways of care for LBP in Saudi Arabia.
Al-Ahmadi and Roland and Alzaied and Alshammari focused on PHC accessibility and found that accessibility was more satisfactory in urban areas than in rural areas.6,10 However, neither LBP management at PHCs nor the pathways of care have ever been investigated, due to the provision of rehabilitation services being restricted to secondary and tertiary healthcare centers in Saudi Arabia.
In a cross-sectional study conducted among 80 GPs from Riyadh, Saudi Arabia, Alsaleh et al 11 sought to determine the GPs’ levels of awareness regarding the use of the “red flag tool” to screen for LBP. In total, 68% of the GPs reported they were aware of this tool. Consequently, this lack of awareness reflected in the practice of refereeing LBP to attend unnecessary management. In a separate study, Alsaleh et al 12 reported that, in cases where disc prolapse was diagnosed based on an MRI, 61% of 80 GPs referred patients to higher levels of care. This was possibly due to the absence of consistent guidelines and care pathways for LBP management. These studies suggest that primary care management of LBP patients is suboptimal, and their referral to higher levels of care may place undue pressure on secondary- and tertiary-level services.
While there are a few studies that focus on LBP management in Saudi Arabia, these studies were all cross-sectional, conducted at PHCs, and only included GPs.10–12 Thus, the current state of LBP management in Saudi Arabia has not been studied in higher-level centers or with multiple direct care providers. Qualitative studies can provide insight into the process of patient care and allow for a wide range of views from different practitioners, in order to develop a proper interventional study. 13 Therefore, this study aimed to collect qualitative interview data to explore current LBP management in the tertiary care facilities in the central region of Saudi Arabia from the perspectives of 2 groups of healthcare practitioners: physiotherapists and spine surgeons who are ultimately involved in caring for nearly all the cases of chronic lower back pain.
Methods
Design
A qualitative one-to-one in depth interview was used in the study
Participants
A non-probability convenience sampling method, which is advisable for the qualitative exploration of a complex phenomenon, 14 was adopted in this study. Spine surgeons in the tertiary care facility in the central region of Saudi Arabia who were in direct contact with LBP patients and with the authority to refer patients for an MRI were recruited as clinician participants. Outpatient PTs with a primary interest in LBP management were also included. Healthcare professional (spine surgeon or PT) who have no contact to LBP patient, in internship, or recently graduated were excluded from the study.
Recruitment
The original intention was to begin recruiting from both a government and private hospital that has spine clinic. The private hospital’s ethics committee, however, refused to participate. As a result, the research was limited to one location: King Fahad Medical City in Riyadh. The center is a tertiary-care hospital in Saudi Arabia that accepts referrals from secondary and primary care centers across the country.
PTs and spine surgeons who met the inclusion criteria were identified by their team leaders then a list of potential participants along with their emails was supplied to the main author. The main author invited all of the identified participants by email, attached to the e-mail was an information sheet detailing the objectives and methods of the study, including how information from participants would be used, and ensuring confidentiality for participants. The majority of the candidates agreed to participate (n = 22, 85%) and replied to the email with written informed consent.
Procedure
We used one-on-one, semi-structured interviews for data collection (Appendix A). Semi-structured interviews generally provide a degree of flexibility in allowing interviewers to follow and explore content elicited in the interview situation. Furthermore, semi-structured interviews present a chance to consider new information that may not have been identified at the beginning of the study. 15 The semi-structured interview schedule used in this study was informed by previous literature and agreed upon by all the authors. Additionally, the schedule was piloted in 2 healthcare practitioners before conducted the data collection. The semi-structured interview included some prompts to ensure the participants do not deviate from the study aim (ie, to explore current LBP management in tertiary care facilities). However, it was only provided when the participants started discussing irrelevant issues to the study aims. The interviewer tried to use the prompts when appropriate without leading the answers of the interviewees.
Interviews lasted approximately 25 to 45 minutes. The number of participants included in the study was limited to data saturation, at which no new data could be identified, and recruitment was closed. 16 The point of data saturation occurs when the semi-structured interview schedule becomes counterproductive and do not elucidate new “emerging” data.
The male interviewer (A.A) was not known to the participants and was introduced to them as a postgraduate researcher. The interviewer received training in qualitative research methods as part of his postgraduate education and has experience in qualitative research and interviewing.
Ethical approval for the study was obtained from King Fahad Medical City in November 2016 (IRB: H-01-R-R-012). All interviews were audio recorded digitally and transcribed verbatim by the first author.
The transparency and rigor of the collected data were further enhanced by adopting a framework analysis method. 17 After becoming familiar with the data by checking transcripts against the recorded interviews, emerging and existing themes were identified. The transcripts were subsequently indexed or coded, coding was conducted by 2 independent authors (AH and MA) and a periodic conference meeting with all authors to discuss the analysis progress and resolve any conflict. Afterward, the codes were sorted into the identified themes. Finally, codes and themes were examined independently by all the authors, which further enhanced data validity. 18 Respondent validation was assured by discussing the analysis results with 20% of the participants from both groups. NVivo (version 10) software was used to arrange and code the transcripts and examine the data and their interactions.
Results
Characteristics of Spine Surgeon Participants.
Characteristics of PT Participants.

Clinical Guideline Availability and Pathways of Care
In this theme, the participants deliberated how clinical guidelines could be used in the management of LBP and the need for the adoption of international clinical guidelines to match the current healthcare system of Saudi Arabia
More than half of PTs and spine surgeons were in agreement regarding the convenience of international clinical guidelines for managing LBP.
“Guidelines are great to assure a good quality outcome, but I honestly do not use them,” PT 4.
“Unfortunately, we do not have any (clinical guidelines),” Spine surgeon 3.
Moreover, clinical guidelines do not currently exist in Saudi Arabia, nor is there an internationally adapted version available.
“We do not have clinical guidelines for low back pain, and we are thinking of adapting international clinical guidelines,” Spine surgeon 5.
However, less than 20% of the PT participants acknowledged that they would sometimes refer to the international guidelines when uncertain.
“I use them (international clinical guidelines) as a reference when I am not sure about something,” PT 1.
Utilization of Primary Care Services
Unfortunately, it appeared that the lack of coordination among healthcare services might have influenced patients’ lower levels of trust in primary care services. However, both spine surgeon and PT participants related that mistrust to a general deficiency in healthcare resources, including spine surgeons and available services (rehabilitative and diagnostic), identified as a primary obstacle to delivering adequate primary healthcare services.
“People have more trust in secondary-level hospitals. For a period, primary care had a lack of resources; therefore, people have this idea they should distrust them,” Spine surgeon 3.
“We have a lack of PHCs and staff. We need time to build community trust in these centers,” PT 4.
Both PTs and spine surgeons also highlighted that early physiotherapy intervention through primary care services is critical for patients.
“Physical therapy and primary healthcare providers are very important cornerstones in the treatment of low back pain,” Spine surgeon 4.
More than half of the PT participants added that early physiotherapy intervention could be beneficial in reducing the need for running further tests on patients with LBP.
“If physiotherapy was used as a first point of contact in these cases, we would not need to use an MRI.” PT 7.
Overutilization of Secondary Care Resources
As a consequence of the poor implementation of primary care treatment for LBP, secondary-level healthcare is over utilized with cases that could be managed earlier through primary care services.
“70% of the LBP cases we see here (in secondary care) could be treated through primary care and physiotherapy,” Spine surgeon 4
Spine surgeons voiced concerns regarding the cases referred to secondary-level services and questioned the validity of the referrals.
“The way patients get referred, the type of patients to be referred, and the validity of their medical reports are obstacles to improving patient care in secondary hospitals,” Spine surgeon 4.
These referrals might be the result of the lack of services at the primary-care level.
“They (the patients) have an excuse, because primary-level hospitals usually lack spinal surgeons,” Spine surgeon 3.
In the participants’ view, this problem is due to mismatched priorities, with too much emphasis placed on secondary hospital care and too little on primary care.
“Coordination between services is not satisfactory. If we could reach a good level of coordination between healthcare providers, we would decrease costs and time,” Spine surgeon 2.
The consequences of this imbalance are an unnecessarily increased burden on secondary care staff and services and longer patient waiting times.
“Patients may wait for two months to have an MRI, then book a follow-up appointment, then be referred to physiotherapy, which might take a year,” PT 5.
Healthcare practitioners reported high demand for MRI scanning by patients with NS-LBP, who are keen to identify any changes in their condition over time, compared with their original scans. However, the healthcare practitioners claimed they rarely change their original clinical opinion, despite further scans.
“Very rarely, the MRI will affect the treatment decision,” Spine surgeon 5.
“Patients insist we do an MRI or request a follow-up MRI to see how quickly the condition is progressing or what the extent of the problem is,” Spine surgeon 6.
Discussion
This study aimed to explore the current healthcare services being provided to LBP patients in Saudi Arabia from the perspective of PTs and spine surgeons. Our findings shed light on the importance of having more organized clinical pathways of care and emphasized the importance of early patient management at the primary-care level to reduce the costs of care and waiting times for patients
Data from this study showed local, specific clinical guidelines for LBP management seems to be unavailable in Saudi Arabia, and that healthcare providers, consequently, either consult international guidelines or do not refer to any clinical guidelines when managing patients with LBP. Compared with other health problems observed in primary care, the lack of clinical guidelines for LBP management also poses a particular challenge for healthcare practitioners. For instance, international guidelines recommend that healthcare providers should not immediately resort to laboratory and imaging tests, but instead focus on functional recovery.8,19-21 However, the lack of local clinical standards for LBP management may place healthcare providers at a disadvantage regarding access to the tools and evidence-based guidance necessary to offer appropriate primary care services.
The lack of coordination in the delivery of healthcare services in this study indicates that secondary healthcare services seem to be over utilized in cases that could be managed at the primary-care level. The healthcare practitioners we interviewed recommended early treatment at the primary-care level to reduce the load on medical practitioners and the cost of care. Ideally, patients with LBP should seek care through their GP. However, these doctors might not have the resources available to properly diagnose and treat such chronic conditions. 12
Physiotherapy is the standard conservative treatment recommended by clinical guidelines for people with LBP.20,22 However, this service is not available through primary healthcare services in Saudi Arabia and is considered a referral-based service at the secondary level. In this study, most participants agreed on the importance of initiating physiotherapy treatment at an early stage for LBP patients. Empirical evidence has shown that PTs are proficient in the efficient management of musculoskeletal complaints within a general practice/primary care environment in various countries.23-25 Further, physiotherapy has been shown to result in a high level of patient satisfaction.23,26 These findings correspond with the global strategy of integrating physiotherapy into primary care services.27-29
This study’s findings suggest that early initiation of physiotherapy services could lead to early recovery and subsequent decreases in medication, consultation, and imaging costs. This is consistent with previous research that suggested reduced cost of care was associated with integrated physiotherapy services at the primary-care level.27,28,30
Secondary care is readily available in Saudi Arabia; however, identifying the proper specialist and coordinating care may be challenging. As a result, care for patients with LBP often ends up being fragmented among several providers. Again, this relates to the lack of clinical guidelines for LBP management tailored explicitly to the Saudi Arabian healthcare system. Care coordination measures should focus primarily on ensuring that healthcare teams can provide patients with excellent communication, smooth transition, and timely care. 31
The lack of local guidelines and pathways of care suggest poor coordination between healthcare services, overutilization of secondary healthcare services, and underutilization of primary healthcare services. According to the spine surgeon participants in this study, the current overutilization of secondary-level services may be associated with patients waiting longer to receive treatment. Increased waiting time has been associated with the increased chronicity of LBP.32,33 Consequently, LBP patients may need to take more time off work, thus negatively affecting their productivity. 32 The impact of reduced utilization of the healthcare system might have more considerable negative socioeconomic consequences that could be reflected at both the individual and societal levels.
Multiple research implications can be identified from this study. The findings suggest that including rehabilitation services at the primary-care level could reduce the cost of care in Saudi Arabia. Similar findings have also been supported in other countries.27,28,30 Our study also highlighted that additional costs for the care of LBP may be overly spent at the secondary-care level (ie, cost associated with imaging, consultation, medication, and surgery). Therefore, the application of a healthcare model with an established cost of care, such as the Saskatchewan Spine Pathway of Canada, 34 is worth exploring further. Future research is needed to estimate the costs spent in the secondary-care level in such services.
Multiple publications suggest that having clinical guidelines is ineffective unless implementation strategies are also developed for them.35‐37 Some countries have focused on and implemented effective guidelines in LBP management. In Denmark,37,38 Canada, 34 and the UK, 39 clinical practice has been improved through the implementation of guidelines that assist practitioners by providing criteria for making informed decisions. For example, the implementation strategy in Denmark was cost effective when compared with the usual strategy for implementing LBP clinical practice guidelines in general practice. It was also significantly reducing the referral from primary care to secondary healthcare, without decreasing the quality of patient care.33,34 As such, adapting of successful and previously applied clinical pathways of care in Saudi Arabia could be beneficial in many ways (eg, patient’s care and cost-effectiveness). It is also evident that replicating policies over time increases their efficacy in the diagnosis and management of LBP.9,41
Despite being the first study to qualitatively explore LBP management in Saudi Arabia, a likely limitation of this study was that the geographical transferability of the findings might be challenged by the inclusion of a single, prominent governmental center. However, the selected center receives patients from across Saudi Arabia. Furthermore, subjectivity may have been an issue during data analysis, because a single individual conducted the interviews and performed the transcription and preliminary coding. Nevertheless, sharing the transcript with 20% of the participants could potentially enhance the accuracy and trustworthiness of the data. 40
The result of this qualitative study elucidates the effects of a deficient functioning pathway of LBP management locally in Saudi Arabia. However, the incapability of managing LBP in PHC level might be associated with similar results internationally. Therefore, as it has been highlighted, 19 guidelines should aim to manage LBP conservatively at an early level of care. In particular, future studies should seek to adapt and implement a local clinical standard for LBP management in Saudi Arabia to obtain the optimal results.
Conclusion
In conclusion, the findings of this study may indicate a lack of essential services for low back pain management at the primary-care level as reported by PTs and spine surgeons practicing in central region of Saudi Arabia. It may also suggest the need of early patient management at the primary-care level and the need of having a clinical pathway of care in Saudi Arabia. As such, adapting of successful and previously applied clinical pathways of care in Saudi Arabia could be beneficial.
Footnotes
Acknowledgment
We are also immensely grateful to King Fahad Medical City for their contribution in facilitating the data collection process. We also would like to express my deepest appreciation to the Deanship of Scientific Research at Prince Sattam Bin Abdalaziz University.
Author contributions
A.H and M.A were responsible for the study design.
A.H and F.A were responsible for the data collection and analysis.
D.M and M.A were responsible for drafting and critical revision of the manuscript.
All authors have approved the submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Deanship of Scientific Research at Prince Sattam Bin Abdalaziz University under the research project No: 2019/01/13195. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript
Ethics approval and consent to participate
Ethical approval for the study was obtained from King Fahad Medical City in November 2016 (IRB: H-01-R-R-012). All participants gave written informed consent before data collection began.
Consent for publication
Not applicable.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.